
Abstract
Background:
While the World Health Organization recommends exclusive breastfeeding (EBF) for the first 6 months, evidence on EBF practices among HIV-positive mothers in Ethiopia remains limited. This study aimed to assess the prevalence and determinants of EBF among HIV-positive mothers in the Gurage Zone and Yem Special Woreda, Central Ethiopia.
Methods:
A cross-sectional study was conducted from June 1 to 30, 2023, among mothers attending antiretroviral therapy (ART) and prevention of mother-to-child transmission (PMTCT) services. Data were collected using interviewer-administered questionnaires and analyzed with Statistical Package for the Social Sciences version 26. Logistic regression identified determinants of EBF, with significance at P < .05.
Results:
Of 311 participants, 72.6% practiced EBF. Awareness of complementary feeding time, early breastfeeding initiation, family support, and HIV-status disclosure were determinants of EBF.
Conclusion:
The overall EBF among HIV-positive mothers was 72.6%. Interventions targeting the identified determinant factors could help improve mothers’ adherence to EBF practices.
Introduction
Breastfeeding is critical for achieving global goals on nutrition, health and survival, economic growth, and environmental sustainability breastfed. 1 Globally, a minority of infants and children meet World Health Organization (WHO) recommended breastfeeding practices; only 44% of infants initiate breastfeeding within the first hour after birth, and 40% of all infants, fewer than 6 months of age, are exclusively breastfed. 1 Improving breastfeeding practices could save over 820 000 lives a year. 2 Exclusive breastfeeding provides the greatest benefits for both mothers and infants; even any breastfeeding is associated with improved survival and other health outcomes compared with no breastfeeding. 3
Breastfeeding is the ideal food source for all newborns globally. However, in the era of the Human Immune Deficiency Virus (HIV), infection in breastfeeding is a challenge due to mother-to-child HIV transmission. 4 According to 2019 United Nations (UN) AIDS data, currently at a global level, 1.7 million children under 15 years live with HIV. Even though new infections and Acquired Immunodeficiency Syndrome (AIDS) related deaths are continuously decreasing in the general population, there is still a high number of new infections and AIDS-related deaths of 160 000 and 100 000, respectively, occurring in children less than 15 years of age per year globally. 5
Despite the overall decrease in mother-to-child transmission of HIV, new pediatric infections continue to occur, and transmission dynamics have now shifted toward a proportional increase in transmission during the postnatal period. 6 Safe breastfeeding practice is one of the major preventive strategies for mother-to-child HIV transmission. 1 According to the evidence, exclusive breastfeeding combined with efficient antiretroviral therapy is an important method for preventing mother-to-child HIV transmission since ART decreases maternal viral load while exclusive breastfeeding reduces newborn gut susceptibility. Therefore, WHO promotes exclusive breastfeeding for 6 months with continued breastfeeding under ART support.7,8
Countries, including Ethiopia, largely implemented the recommended practices starting in 2010 based on WHO guidelines. These recommendations emphasize that mothers living with HIV who are receiving effective lifelong antiretroviral therapy (ART) should exclusively breastfeed for the first 6 months of their child’s life, introduce appropriate complementary foods thereafter, and continue breastfeeding for at least 12 months, and up to 24 months or longer if supported and virally suppressed.9 -11 However, different studies indicate that there is a significant gap between what the WHO recommended and the actual breastfeeding practice for HIV-exposed children. 1 The infants receiving mixed feeding were 42 times at risk of acquiring HIV infection compared to those receiving exclusive breastfeeding. 12 In another study conducted in Addis Ababa, 23% mixed feeding practices were observed in infants less than 6 months old, which still increased the risk of mother-to-child transmission of HIV. 13 The 2019 Ethiopia Mini DHS revealed that only 59% of infants under 6 months were exclusively breastfed, which is below the WHO target of 60% to 70% by 2030 for children under 6 months of age.14,15 The current evidence shows that the prevalence of exclusive breastfeeding practice among HIV-positive mothers is from 80.8% to 94%.16 -18 The determinants of exclusive breastfeeding practice among HIV-positive mothers are antenatal care follow-up, disclosure of their HIV serostatus, family income, mother’s awareness, having breast problems, and mother’s breastfeeding initiation time after delivery.19 -21
In the study area, a limited study was done on this issue, besides the national goal of zero HIV transmission from mother to child by 2030. The evidence for exclusive breastfeeding practices among HIV-positive mothers in Ethiopia is limited and primarily derived from single-facility-based research conducted outside Central Ethiopia, limiting its generalizability. Because Central Ethiopia has different sociocultural contexts, geographical variation, and HIV treatment delivery patterns, there is a lack of multicenter data indicating current infant-feeding practices among HIV-positive mothers. This study addresses these geographic, methodological, and population-specific gaps by assessing the prevalence and determinants of exclusive breastfeeding practices in Central Ethiopia. Thus, this study aimed to assess the prevalence of Exclusive Breastfeeding Practice and determinants factors among HIV-positive mothers in Central Ethiopia.
Methods and Materials
Study Settings and Period
The study was conducted in the Gurage Zone and Yem Special Woreda in Central Ethiopia from June 1 to June 30, 2023. The total population of the Gurage Zone was 1 727 522 dwellings in 16 rural woredas and 8 urban administrations, of which 52% comprises the female population according to the 2019 Zonal government’s report, and Yem special woreda has a total population of 100 800 with 52% of the female population. Among 7 hospitals and 75 health centers, 22 health facilities were implementing the ART/PMTCT program. Across the 22 ART/PMTCT service-providing health facilities, a total of 4000 patients were enrolled in the ART program. During the study period, 61% (2440) of these patients were women aged 15 years or older, of whom 359 had children under 2 years of age.
Study Design and Population
An institution-based cross-sectional study was conducted to assess exclusive breastfeeding practices and their determinants among HIV-positive mothers of children aged 6 to 23 months attending ART/PMTCT clinics. The source population comprised all HIV-positive mothers with children aged 6 to 23 months attending health institutions for ART/PMTCT services in the Gurage Zone and Yem Special Woreda. The study population included all HIV-positive mothers with children aged 6 to 23 months who attended these institutions during the data collection period. Mothers who were ill, not enrolled in ART services, unable to respond at the time of the interview, or whose children did not receive infant antiretroviral prophylaxis were excluded.
Sample Size Determination and Sampling Technique
The sample size was calculated using the single population proportion formula with the following assumptions: the prevalence of exclusive breastfeeding practice among HIV-positive mothers was taken from a previous study conducted in West Oromia (72%), 22 with a 95% confidence level, and a desired precision of 5%. After adding a 10% non-response rate, the final sample size was 341. All health facilities providing ART/PMTCT services in the Gurage Zone and Yem Special Woreda were included. All HIV-positive mothers with children aged 6 to 23 months who attended the ART/PMTCT clinics for their monthly ARV refill during the study period were recruited until the required sample size was reached.
Operational Definition
HIV-Exposed Infant
An infant or child born to a mother living with HIV until the infant or child is reliably confirmed to be HIV-negative.
Antiretroviral Therapy (ART)
The use of a combination of 3 or more antiretroviral (ARV) drugs to treat HIV infection. ART is a lifelong treatment.
Exclusive Breastfeeding
The infant receives only breast milk, without any other liquids or solids, not even water, except for oral rehydration solutions, drops, or syrups containing vitamins, minerals, or medicines.
WHO-Recommended Breastfeeding
Initiation of breastfeeding within the first hour of life; exclusive breastfeeding for the first 6 months; continued breastfeeding up to 2 years of age or beyond; and breastfeeding on demand, regardless of the mother’s HIV status 23.
Mixed Feeding
Giving an infant younger than 6 months other liquids and/or foods in addition to breast milk. This may include water, other types of milk, or any type of solid food 23.
In this study, knowledge of exclusive breastfeeding was assessed using 10 questions. Mothers who answered 6 or more correctly were classified as having good knowledge, while those who answered fewer than 6 were classified as having poor knowledge.21,24
Data Collection, Quality Control, and Measurements
A standardized questionnaire was adapted from related published literature, taking into account the local context of the study area.13,20,21,23,24 It was initially prepared in English, translated into the local language, and then back-translated into English to ensure consistency. The questionnaire included socio-demographic characteristics, disclosure of HIV status, knowledge and information on exclusive breastfeeding, healthcare and obstetric-related factors, and exclusive breastfeeding practices. The content and face validity of the questionnaire were checked by a panel of experts, and internal consistency was confirmed using the Cronbach’s alpha test. When HIV-positive mothers arrived at the health institution for their monthly ART appointment, data were collected by trained and experienced data collectors using a structured interviewer-administered questionnaire. Interviews were conducted in a private setting where mothers felt free to express their responses and ideas. Continuous supervision of the data collectors was maintained. To ensure data quality, the data collectors and supervisors received 2 days of training. Two weeks before the actual data collection period, 5% of the sample size was used to pretest the questionnaire among HIV-positive mothers attending the ART/PMTCT site at Halaba Kulito Hospital in Halaba Zone, and all necessary modifications were made.
Data Processing and Analysis
The data were entered into EPI Data 3.1 and exported to SPSS version 26 for analysis. Descriptive analysis was used to summarize the study variables, including frequency, percentage, mean, and standard deviation. Bivariate logistic regression was conducted to assess the association between each independent variable and the outcome variable. Variables with P-values less than .25 in the bivariate analysis were entered into the multivariate logistic regression model. An attempt was made to verify whether the necessary assumptions for using multivariable logistic regression were met. To check for goodness of fit, the Hosmer and Lemeshow test was used, with a P-value of .473 indicating good fit. The effects of multicollinearity and confounding were investigated, and variance inflation factors (VIF) and tolerance tests indicated no multicollinearity. Finally, a P-value less than .05 was considered statistically significant, and the adjusted odds ratio, along with 95% confidence intervals (CI), was used to measure the strength of the association between dependent and independent variables. The results were presented in narration, tables, and figures.
Ethical Approval and Informed Consent
Ethical approval of the study was obtained from the Institutional Ethical Review Board (IERB) of Wolkite University with reference number IERB/0339/23. A permission letter was obtained from the Gurage Zone and Yem special Woreda. The study was conducted based on the ethical standards of the Declaration of Helsinki. The ethical letter was given to Gurage Zone and Yem Special Woreda to initiate the permission process to collect data. The purpose of the study, participants’ right to refuse, confidentiality, and voluntary participation were explained in detail to the study participants, and informed written consent was obtained. Moreover, consent from participants with no formal education was obtained after the information sheet was read aloud in the local language and documented by thumb impression with a witness. Additionally, written informed consent was obtained from the legally authorized representatives of the minor groups of less than 18 years before enrollment. Confidentiality and anonymity of information were maintained during data collection procedures.
Results
Socio-Demographic Characteristics of Study Participants
Of the expected 341 samples, 311 of them participated in the study with a response rate of 91.2%. The mean age of mothers and children was (28.9 ± 4.9) years and (11.74 ± 6.33) months, respectively. More than half of the study respondents (67.2%) were rural residents. Mothers who had a male child were 176 (56.6%), and most of the mothers, 253 (81.3%), were married. Concerning educational status, 216 (40.5%) mothers cannot read or write. In the case of religion, 156 (50.6%) respondents were Orthodox Christians. Regarding ethnicity and occupation of the mother majority, 216 (69.5%) were Gurage and 219 (70.4%) were housewives, respectively. Two hundred forty-nine (80.1%) of respondents belonged to a family size of less or equal to 5. About 250 (80.4%) of the mothers have support from their families (Table 1).
Socio-Demographic Characteristics of HIV Positive Mothers Who Attended for ART/PMTCT Service in Health Facilities in Gurage Zone and Yem Special Woreda, 2023.

Healthcare and Obstetrics-Related Factors of HIV-Positive Mothers
Among 311 mothers, the majority of respondents, 283 (91%), had ANC follow-up during their last pregnancy. More than two-thirds (68.8%) of the study participants were multiparous. All mothers had postpartum follow-up. Of the respondents who delivered in health institutions, 255 (82%) had spontaneous vaginal deliveries (Table 2).
Healthcare and Obstetrics-Related Factors of HIV-Positive Mothers Attending ART/ PMTCT Services Providing Health Institution in Gurage Zone and Yem Special Woreda, 2023.

Abbreviations: ANC, antenatal care; SVD, spontaneous vaginal delivery; C/S, cesarean section; ART, antiretroviral therapy; NGO, non-governmental organization.
Disclosure Status of HIV-Positive Mothers
Among the study participants, 261 (83.9%) had disclosed their HIV status to relatives, with 155 (59.0%) disclosing to their husbands. The primary reason for disclosure was advice received from health professionals during counseling sessions (64.0%). Whereas, the reason for non-disclosure was mainly attributed to fear of stigma and discrimination (67.9%), fear of partner reaction (19.6%), and lack of social support or absence of a trusted person to disclose to (12.5%; Figure 1).
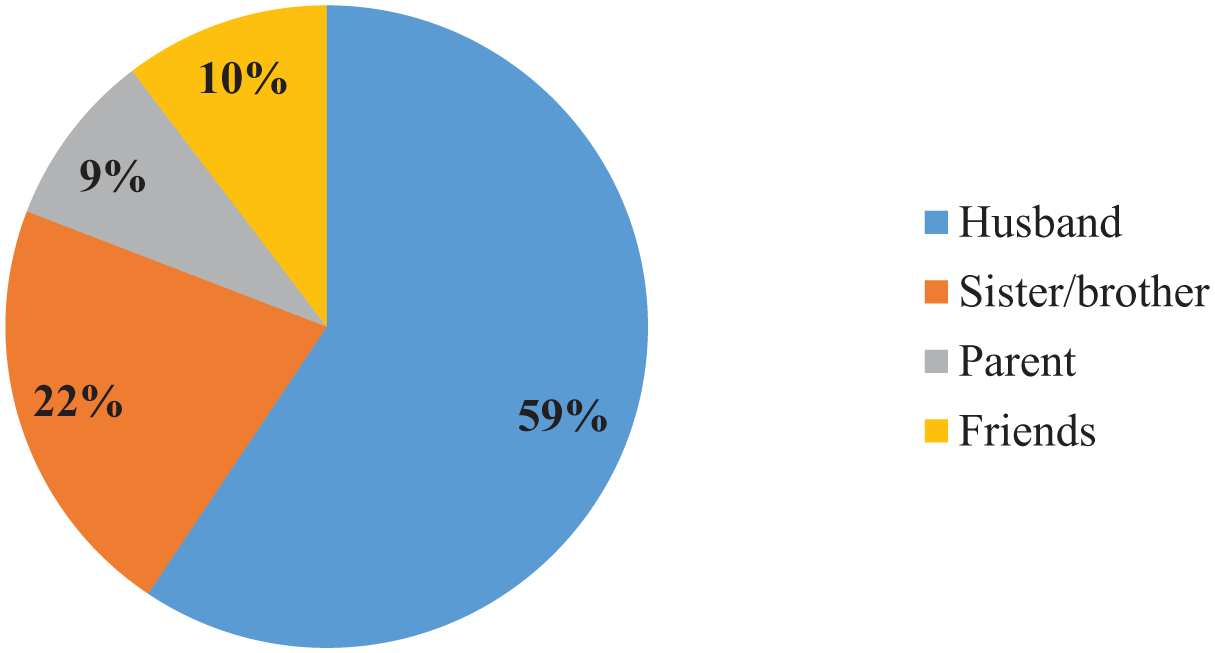
Percentage of relative HIV positive mothers who disclosed their HIV status in Gurage Zone and Yem special Woreda, Central Ethiopia, 2023.
HIV-Positive Mothers’ Knowledge and Information About Exclusive Breastfeeding
The majority of mothers, 280 (90%), heard about exclusive breastfeeding, and among these, 245 (78.8%) received the information from the health care personnel. 219 (70.4%) mothers were counseled on exclusive breastfeeding. During the counseling session, the health care provider counseled on feeding options, the advantages, and disadvantages of the feeding option, and husband support for feeding options were 271 (96.7%), 256 (91%), and 70 (25%), respectively. Mothers who were aware of the recommended time of initiation of breastfeeding within 1 hour after delivery, mother’s awarenes regarding the time to start complementary food at 6 months, and HIV-positive mothers who started breastfeeding before 6 months were 261 (83.9%), 131 (42.1%), and 49 (15.8%), respectively. Regarding mother-to-child (MTCT) transmission of HIV, 61% of respondents reported transmission during childbirth, 19% during pregnancy, and 20% during breastfeeding. In this study, 206 (66.2%) of mothers have good knowledge of exclusive breastfeeding.
The Prevalence of Exclusive Breastfeeding Practice Among HIV-Positive Mothers
Of all mothers, 311 (100%) had breastfed their children. Among these, 261 (83.9%) started breastfeeding within the first hour after delivery. The prevalence of exclusive breastfeeding (EBF) practice among HIV-positive mothers of children less than 2 years of age was 229 (72.6%; 95% CI: 68.7, 77.6), while the remaining mothers (27.4%) practiced mixed feeding. More than one-fourth of the mothers (42.1%) were aware of starting complementary feeding at the recommended time, at 6 months of age.
The Determinants of Exclusive Breastfeeding Practice of HIV-Positive Mothers
In the bivariate analysis, the occupation of the mother, family support, the time of initiation of breastfeeding after delivery, women’s awareness regarding the time to start complementary food, mothers’ knowledge of exclusive breastfeeding, and maternal disclosure of HIV status were selected for the final model based on the P-value (<.25). However, in the multiple logistic regressions, women’s awareness regarding the time to start complementary food, family support, maternal disclosure of HIV status, and the time of initiation of breastfeeding after delivery were determinants of exclusive breastfeeding practice. HIV-positive mothers who were not aware of the time to start complementary food were 98% less likely to practice exclusive breastfeeding compared with those who started complementary food after 6 months (AOR = 0.02; 95% CI: 0.01, 0.060). HIV-positive mothers who initiated breastfeeding within the first hour of delivery were 2.2 times more likely to practice exclusive breastfeeding (AOR = 2.2; 95% CI: 2.0, 3.67) compared with those who initiated breastfeeding within 8 hours. HIV-positive mothers who had family support for breastfeeding their infants were 2.91 times more likely to practice exclusive breastfeeding (AOR = 2.91; 95% CI: 1.74, 9.12) compared with those who were not supported. Mothers who disclosed their HIV status were 2.6 times more likely to practice exclusive breastfeeding (AOR = 2.6; 95% CI: 1.92, 8.53) compared with their counterparts (Table 3).
Bivariate and Multivariable Logistic Regression Analysis of Factors Associated with Exclusive Breastfeeding Practice of HIV Positive Mothers in Gurage Zone and Yem Special Woreda, Central Ethiopia, 2023.
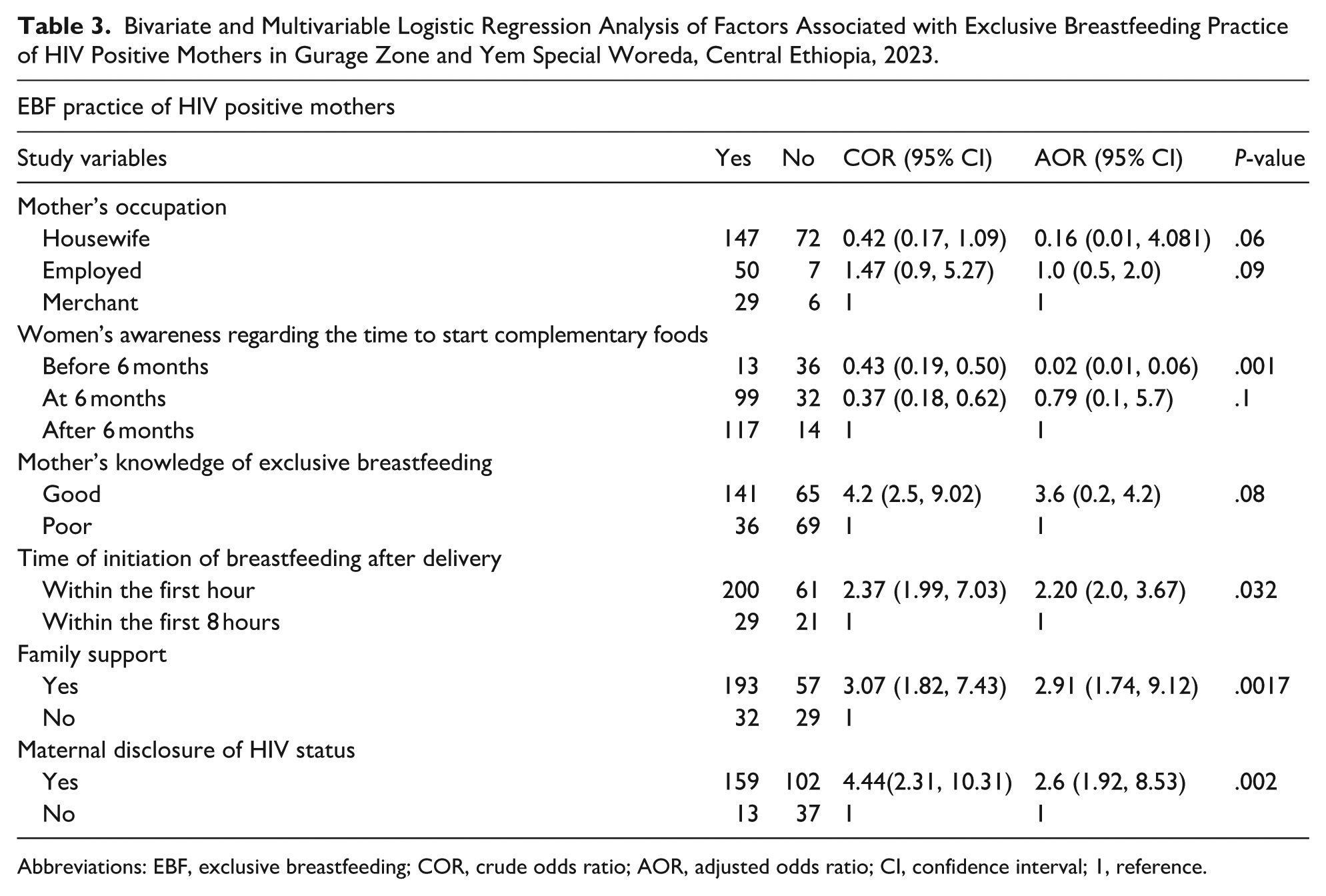
Abbreviations: EBF, exclusive breastfeeding; COR, crude odds ratio; AOR, adjusted odds ratio; CI, confidence interval; 1, reference.
Discussion
An institution-based cross-sectional study was conducted to assess the prevalence and determinants of exclusive breastfeeding practices among HIV-positive mothers with children aged 6 months to 2 years who attended ART/PMTCT clinics in the Gurage Zone and Yem Special Woreda, Central Ethiopia. In the present study, women’s awareness regarding the time to start complementary food, family support, maternal disclosure of HIV status, and the time of initiation of breastfeeding after delivery were determinants of exclusive breastfeeding practices. The overall prevalence of EBF practice in HIV-positive mothers of children aged 6 months to 2 years was 72.6% (95% CI: 68.7, 77.6). This finding is consistent with studies conducted in Debre Markos 77.1%, 16 West Oromia 72%, 22 and Bahir Dar, North Ethiopia 75.2%. 25 However, it is lower than studies conducted in Mekele (90.3%), 26 Gonder 94%, 18 and Northern Ethiopia 88.8%, 21 respectively. This disparity might be explained by socio-demographic differences among the study participants, such as educational level and living standards, as well as the characteristics of the study area, cultural practices, maternal knowledge, and access to healthcare, information, and health education from healthcare personnel.
On the other hand, this study finding was lower than those reported in Addis Ababa 37%, 13 Southern Ethiopia 48.2%, 24 and SNNPR 56.3%. 27 The discrepancy might be due to regional variability and differing socio-cultural backgrounds, which can create barriers to exclusive breastfeeding practices. Moreover, the higher prevalence might be attributed to differences in the time period, as improvements in access to healthcare and awareness of available services may have occurred over time.
In this study, 27.4% of mothers practiced mixed feeding. This was higher compared with studies conducted in Debre Markos, North Ethiopia 14.2%, 16 SNNPR, Ethiopia 10.9%, 25 and Bahir Dar, Ethiopia 8.1%. 27 However, the proportion of mothers who practiced mixed feeding in this study was almost similar to that reported in West Oromia 24.6%. 22
Regarding the determinants of exclusive breastfeeding practices, HIV-positive mothers who were not aware of the time to start complementary food were 98% less likely to practice exclusive breastfeeding compared with those who started complementary food after 6 months. This finding was supported by the study conducted in Nigeria.24,25,28 The evidence showed that, as women’s awareness increases, their knowledge of exclusive breastfeeding practices increases.20,25,28,29
HIV-positive mothers who initiated breastfeeding within the first hour of delivery were 2.2 times more likely to practice exclusive breastfeeding. The possible justifications are that early initiation of breastfeeding within the first hour strengthens milk production, promotes mother-infant bonding, reduces breastfeeding difficulties, and enhances breastfeeding self-efficacy, which leads to increased exclusive breastfeeding among HIV-positive mothers.30,31 This finding is supported by studies conducted in Bahir Dar Town and SNNPR, Ethiopia,17,25 respectively. In this study, HIV-positive mothers who have family support for breastfeeding their infant were 2.91 times more likely to practice exclusive breastfeeding. This finding is supported by studies conducted in Gondar Town 18 and Tanzania. 32 The evidence revealed that family support has an impact on exclusive breastfeeding practices. 33
This study also revealed that mothers who disclosed their HIV status were 2.6 times more likely to practice exclusive breastfeeding. The finding of this study is consistent with a study conducted in Southern Ethiopia. 34 The evidence indicated that mothers who disclosed their HIV status were more likely to practice exclusive breastfeeding, which allows for better access to counseling, partner and family support, and adherence to recommended infant feeding guidelines. 35 These supportive situations lower fear and stigma, allowing for consistent exclusive breastfeeding practices.34,36 In this study, the prevalence of exclusive breastfeeding practices and their determinants in central Ethiopia were assessed, which gives a hint to further investigate ways to enhance exclusive breastfeeding practices.
Strengths and Limitations of the Study
In this study, to improve the sample size, all health institutions that provide ART/PMTCT services for HIV-infected patients were included. The study incorporated all health facilities that provide ART/PMTCT services in Gurage Zone and Yem special Woreda, which is ideal to represent Central Ethiopia.
Even though the necessary efforts were made to minimize or avoid the possible limitations of this study, the results should be interpreted in light of the following limitations. The study was health facility-based, and the findings may not be generalizable to all HIV-positive mothers with HIV-exposed infants. A relatively small sample size was used. This was because very small numbers of HIV-positive mothers with HIV-exposed infants attend health facilities, and it is difficult to trace them at the community level. Furthermore, this study employed only a quantitative approach; it would have been better if it had included a qualitative approach to investigate factors in greater detail. This study was based on self-reported survey data, which may be influenced by recall bias and potential bias from social desirability since women may report more acceptable responses. Since a cross-sectional design was used, the cause-and-effect relationship could not be established.
Conclusion
In the present study, the prevalence of exclusive breastfeeding (EBF) among HIV-positive mothers was 73.6%. Women’s awareness regarding the appropriate time to start complementary feeding, family support, maternal disclosure of HIV status, and the timing of breastfeeding initiation after delivery were identified as determinants of EBF practices. Therefore, interventions targeting these modifiable factors could help increase HIV-positive mothers’ awareness and adherence to exclusive breastfeeding practices.
Recommendations
To achieve zero new HIV infections by 2030, improving exclusive breastfeeding practices among HIV-positive mothers is essential. The regional health bureau, zonal health department, and Woreda health offices are encouraged to provide basic training for healthcare personnel, particularly ART/PMTCT service providers, on awareness creation, and counseling HIV-positive mothers about exclusive breastfeeding practices.
Healthcare providers are encouraged to provide detailed, individualized counseling to mothers on the appropriate time to start complementary feeding, the timing of breastfeeding initiation after delivery, and maternal disclosure of their HIV status to enhance recommended exclusive breastfeeding practices. Additionally, encouraging and facilitating family support for exclusive breastfeeding is crucial to promote adherence and improve outcomes.
Footnotes
Acknowledgements
The authors would like to thank Wolkite University for allowing us to conduct the research and for granting ethical approval. The authors also extend their gratitude to the Gurage zone health department and Yem special Woreda for their valuable support, study participants, data collectors, and the supervisor for their unreserved efforts and willingness to participate in this research study.
Ethical Considerations
Ethical approval of the study was obtained from the Institutional Ethical Review Board (IERB) of Wolkite University with ref.no. IERB/0339/23. A permission letter was obtained from the Gurage Zone and Yem special Woreda. The study was conducted based on the ethical standards of the Declaration of Helsinki. The ethical approval letter was submitted to the Gurage Zone and Yem Special Woreda to to facilitate the data collection process.
Consent to Participate
The purpose of the study, participants’ right to refuse, confidentiality, and voluntary participation were explained in detail to the study participants, and informed written consent was obtained. Moreover, consent from participants with no formal education was obtained after the information sheet was read aloud in the local language and documented by thumb impression with a witness. Additionally, written informed consent was obtained from the legally authorized representatives of the minor groups of less than 18 years before enrollment. Confidentiality and anonymity of information were maintained during data collection procedures.
Consent for Publication
Not applicable.
Author Contributions
MA, SJ, and ABD participated in conception and design, acquisition of data, analysis and interpretation of data, and took part in drafting the article. HZ, YF, KA, TM, MP, AS, and MAY participated in the sequence alignment and design of the study and performed the statistical analysis. MA and SJ conceived the study and participated in its design and coordination, and helped with editing the English language. ABD, SJ, and MA reviewed the draft manuscript for intellectual content and participated in the revision. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data that support the findings are available from the corresponding author upon a reasonable request.