
Abstract
Background:
Community pharmacy professionals play a vital role in health care, have a greater impact on public health programs, and play a critical role in patient counseling for both non-pharmacological and pharmacological management. This study aimed to evaluate the knowledge, attitude, and practice of community pharmacy professionals toward nutrition and lifestyle counseling in Gondar City, Ethiopia.
Methods:
A cross-sectional survey was undertaken in Northwestern Ethiopia from May to June 2021. Face-to-face structured interviews were performed to collect data using a specially created questionnaire. Descriptive, independent t-test, and one-way ANOVA analyses were used. A significant difference was defined as a p-value of less than 0.05.
Results:
This survey drew 100 community pharmacy professional from a pool of 105 participants, with a 95.2% response rate. More than a third of the participants (n = 43, 43%) defined medical nutrition therapy as the use of food to prevent disease, and almost half of the participants (n = 51, 51%) viewed therapeutic nutrition to be part of their job responsibilities. More than half (64%) believe that patients should be provided a combination of nutritional and pharmacological treatments in the majority of cases. The majority of participants (75%) gave patients counseling on drug-food interactions.
Conclusion:
The majority of community pharmacy professionals said they knew a lot about medical nutrition therapy and were enthusiastic about nutrition evaluation and medical nutrition therapy, they see these tasks as part of their job, and they practiced dietary counseling that was limited to pregnancy and chronic diseases.
Background
Health promotion, according to the World Health Organization (WHO), is the act of assisting individuals in taking control of and improving their health by focusing on individual behavior in response to a variety of social and environmental interventions. 1 Alcohol and smoking abstinence, as well as encouraging obese patients to lose weight, healthy eating, and physical activity, are among the most important health promotion measures for improving the overall quality of life and reducing the personal and societal implications of poor nutrition. 2
Community pharmacy professionals (CPPs) play an important role in the healthcare system, have a greater impact on public health programs, and play a critical role in patient education. 3 Because of their ease of accessibility, lack of need for an appointment to interact with patients, and widespread geographical distribution, CPPs seem to be ideally positioned to implement health prevention and health promotion strategies, according to the joint International Pharmaceutical Federation and WHO guidelines for good pharmaceutical practice.4,5 Community pharmacies, in general, play an important role in optimizing pharmaceutical care and patient outcomes, as well as preventing drug misuse and lowering costs. 3
One of the most significant services provided by pharmacists is patient counseling. It helps patients reduce medication-related problems and improve their overall health by providing a variety of services. 6 In general, pharmacists inform their patients about the correct use, potential side effects, safety, warnings, and storage conditions of prescribed pharmaceuticals and dietary supplements, as well as public awareness of non-pharmacologic treatments and dietary, lifestyle, and physical activity changes.7–9
Nowadays, the professional image of pharmacy shows the evolution from a product-oriented to a patient-centered one, called a clinical pharmacy. 10 This enhances the role of clinical pharmacists who can focus on patient-oriented services 11 and the development of pharmaceutical care, which is a new form of pharmaceutical practice, has imposed a new responsibility on pharmacists.
Professional organizations such as the American College of Clinical Pharmacy (ACCP), the American Society of Health-System Pharmacists, as well as the Canadian Society of Hospital Pharmacists, have all recommended that nutritional supplements (natural medicine products, nutrients, and micronutrients) be actively included in the pharmacy profession’s area of practice. 12 In addition, pharmacists’ nutritional counseling needs to be improved to improve patient quality of life. 13
For patients seeking nutritional and vitamin counseling, as well as in cases of nutritional and vitamin deficiency, the success of complementary medicine is dependent on the patient’s understanding of proper therapy, which varies from person to person, and pharmacists can assist patients in obtaining nutritional supplements or provide information based on their interactions with conventional drugs.14,15 This shows that to effectively counsel consumers about vitamins and the treatment of nutritional deficiencies, community pharmacists must have the necessary knowledge, attitude, and counseling abilities regarding vitamin and dietary supplement products. 16
Policymakers need to collect data on pharmacists’ level of involvement in nutrition and lifestyle counseling, as well as their attitudes, perceived skills, and potential hurdles, to maximize pharmacists’ untapped potential cost-effectively. Educational institutions would also benefit from identifying gaps to improve pharmacists’ ability to perform desired functions. As a result, we plan to bridge this knowledge gap and assist Ethiopia in allocating evidence-based resources and prioritizing key components of nutritional supplements and lifestyle counseling. To the best of the author’s knowledge, few studies have looked into pharmacists’ knowledge, attitudes, and practices when it comes to nutrition and lifestyle advice in Ethiopia. In Gondar, Ethiopia, this study looked into the role of pharmacists in nutrition counseling, particularly nutrition counseling for obesity and other chronic and medical illnesses. It also sought to learn more about pharmacists’ roles in delivering dietary supplement information, drug-food interactions, and directions and cautions for certain foods and dietary supplements. This study also looked at challenges to pharmacist-led nutrition counseling, as well as potential ways to overcome them. Therefore, the goal of this research was to determine CPPs’ knowledge, attitudes, and practices about nutrition and lifestyle counseling, as well as to identify impediments and strategies for improving nutrition and lifestyle counseling in Gondar, Ethiopia.
Methods
Study design, settings, and period
A cross-sectional study was conducted using self-report in Gondar City and neighboring rural community drug retail outlets (CDROs) in Tseda and Azezo which are two rural CDROs that have comparable services to Gondar City community drug retail outlets. The population of Gondar was predicted to be 323,875 in 2015, according to the Central Statistics Agency’s (CSA) population projection (2013). This study data was collected from May 10 to June 15, 2021 GC.
Study populations, inclusion, and exclusion criteria
The study included all pharmacy professionals working in CDROs in Gondar and nearby towns who volunteered to participate at the time of data collection. Those who were unavailable at CDROs during the data collection period and declined to participate in the study were, on the other hand, excluded.
Sample size determination and sampling technique
In the city of Gondar, there are 76 pharmacies with 128 CPPs working in them (Gondar Health Authority Bureau). All of the participants were from Gondar City, Tseda, and Azezo. The city of Gondar was chosen on purpose, but the rural localities were chosen by lottery from among the other rural localities. These rural locations have pharmaceutical services that are comparable to those in Gondar. Out of 128 pharmacy professionals, 105 were available during data collection in the selected facilities, and out of 105 pharmacy professionals who received questionaries, 100 pharmacy professionals completed and returned their questionnaires (Figure 1).
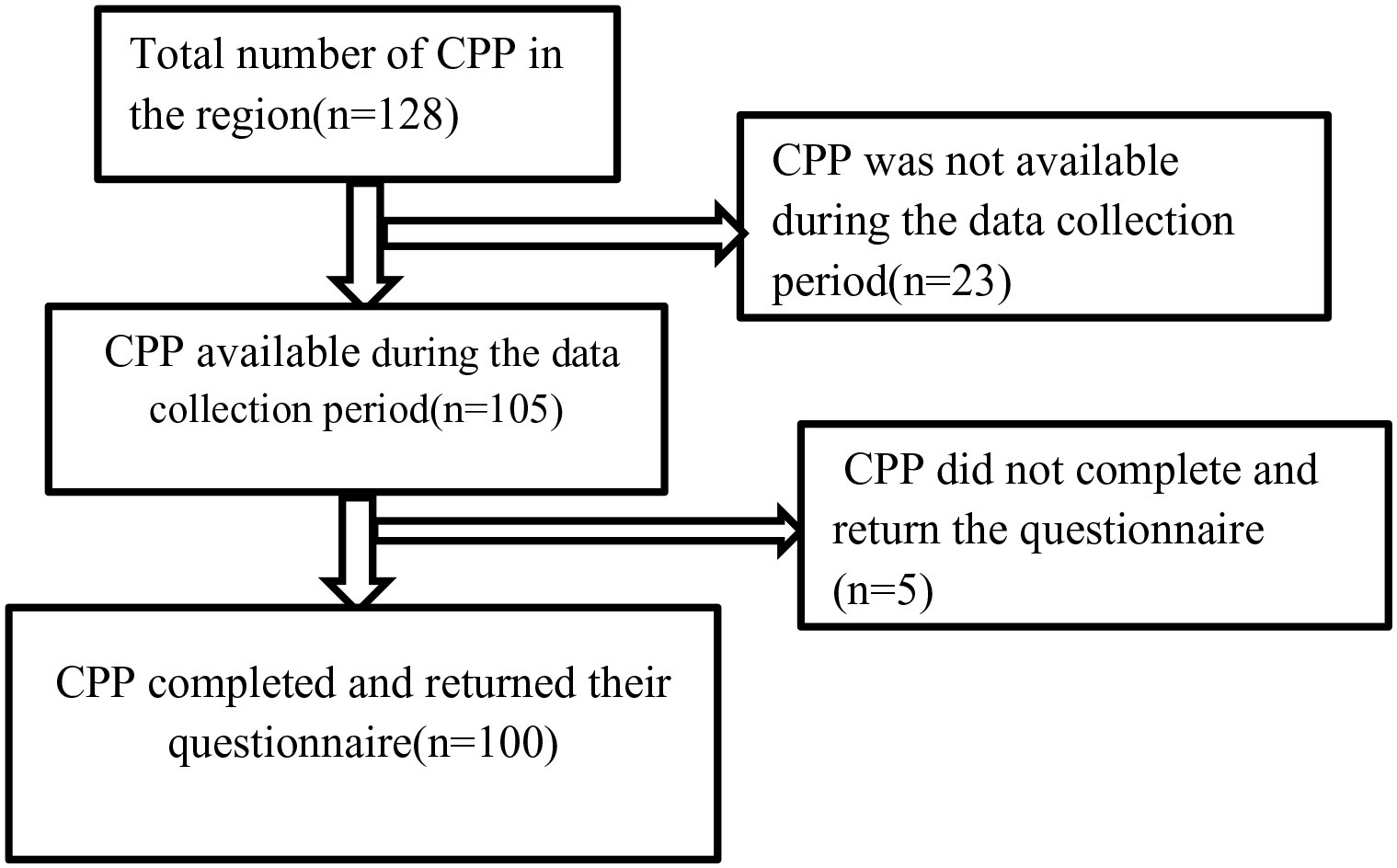
Sampling procedure of community pharmacy professionals’ knowledge, attitude, and practice toward nutrition and lifestyle counseling in Gondar City (n = 100).
Data collection instruments and procedures
A structured self-administered questionnaire was adapted from a previous similar study 17 with minor adjustments made to account for the community settings. A set of questions was created to gather data on community pharmacists’ nutrition and lifestyle counseling knowledge, attitudes, and practice. Because the questionnaire was written in English, the final version was translated into Amharic and then back into English to ensure uniformity. There were two components to the data collection tool. The first section of the questionnaire included demographics and other distinguishing characteristics, such as gender, age, basic graduate qualifications, nutrition information sources, and the nutritional supplements offered in the pharmacy. The second section has 18 questions divided into four groups. Section I consisted of five closed-ended, perception-based knowledge questions about pharmacists’ nutrition counseling competence. A Likert scale from 1 to 5 was used to assess knowledge perception. One pharmacist’s average knowledge score ranged from 1 to 5. The second section of the survey included four closed-ended questions about pharmacists’ perspectives on therapeutic nutrition, dietary supplements, and providing nutritional advice. Section III included four closed-ended questions about pharmacists’ techniques in taking patient histories and providing nutrition counseling for various health conditions and life stages, nutritional support for various sports and physical activities, medical nutrition therapy, and the principles of nutrition supplement use in a variety of clinical situations. Section IV consisted of five multiple-choice questions about the obstacles that pharmacists face in providing counseling and how to overcome them. Previous research on barriers to counseling patients and offering health promotion services at community pharmacies was used to develop the hurdles questions.17–19
Data quality management, entry, and statistical analysis
After a half-day of instruction on components of the data collection tool and ethical considerations, two clinical pharmacists gathered data. The researchers made the goal of the study and the data abstraction tool available throughout data collecting periods very clear to the study participants. To confirm the completeness of the data abstraction format, pretests for the survey were done on the five CDROs in the study area. The format was then changed suitably. The pretest responders were not included in the final analyses. This allowed us to spot any flaws in the approach and data collection instrument (algorithm). The goal of the pretest, the technique, and the time frame were all communicated to all five CDROs.
All five CDROs were informed about the objective of the pretest, the methodology, and the time in which the sudden visits occurred. The authors conducted routine on-site surveillance and checked the surveys for completeness, accuracy, clarity, and consistency daily. The data were then imported into SPSS version 26 and analyzed after being double-checked for cleanliness, completeness, and consistency. To characterize the characteristics of the study participants and display the study results, descriptive statistics, means, proportions, and tables were employed. A histogram and Q-Q plot displaying a normally distributed continuous variable were used to verify the data’s normality. The independent samples T-test and one-way ANOVA were used to examine the mean differences between the groups.
Operational definition
❖ Knowledge: If stands for the level of one’s understanding of something
❖ Good knowledge: Participants who scored greater than or equal to the mean knowledge score
❖ Poor knowledge: Participants who scored less than the mean knowledge score
Results
Socio-demographic characteristics of the participants
A total of 105 community pharmacists were approached for an interview due to incompleteness, five respondents were excluded from the study, resulting in a 95.2% response rate. Among the study participants, more than half participants (55%) were females. The mean (±SD) age of the respondent was 33.9 (±9.6) years with most of the belonging to the 30–39 years range. Nearly half of the participants (48%) had a degree in pharmacy. More than two-thirds of participants (69%) had worked in a pharmacy setting for up to 5 years (65%). The frequent source of nutritional information was undergraduate study followed by internet 11 (11%) and training 9 (9%) (Table 1).
Socio-demographic characteristics of the participants (n = 100).

Methods of nutritional assessment used by CPP
More than one-third of participants (38%) nutritional status through laboratory method and 8%, 13%, 15%, and 26% of participants assessed the nutritional status of patients through clinical, anthropometric, dietary, and a combination of these methods (Figure 2).

Methods of nutritional assessment used by CPP, UOG, 2021.
CPPs’ self-perceived knowledge about nutrition counseling
More than half 55 (55%) of the participants had a good level of knowledge about therapeutic nutrition. Half of the participants 50 (50%) have excellent knowledge about taking medicine with food. Participants also have good knowledge of the indication of drugs 39 (39%), efficacy 44 (44%), and food interaction/herbal drug interaction 39 (39%). One-quarter of the participants 25 (25%), on the other hand, had average knowledge of nutrigenetics (Table 2).
Community pharmacy professionals’ self-perceived knowledge about different nutrition counseling topics, UOG 2021.

The knowledge scores of the CPPs in different nutrition counseling
The mean (±SD) knowledge score of pharmacy professionals was 3.7 ± 0.59. The independent sample T-test showed that there was no mean knowledge score difference between males and females (p = 0.203). Similarly, there was no mean knowledge score difference among qualification, clinical pharmacy study years, work experience, income, available products, and source of nutritional information. In the one-way ANOVA, most variables do not have meaningful mean knowledge score differences. However, there were significant knowledge score differences among CPPs’ age (p = 0.007) and type of medication retail outlet (p = 0.045). Following this, the Tukey post hoc test disclosed professionals aged 20–29 had a good knowledge score of 3.9 (±0.42) compared to those greater than 40 years of 3.4 (±0.80), and professionals who had worked in pharmacy had a higher knowledge score 3.9 (±0.48) than worked RDV 3.2 (±0.33) (Table 3).
Mean knowledge scores of the community pharmacy professional at Gondar City 2021.

Nutritional counseling of special populations
Based on nutritional counseling for different populations, one-fifth of the participants (20%) offered advice to pregnant women. Twelve percent of participants provided advice to childhoods. Nearly two-thirds of the participants (61%) provided advice to different population groups including infancy, childhood, adolescence, adulthood, pregnancy, and lactation (Figure 3).
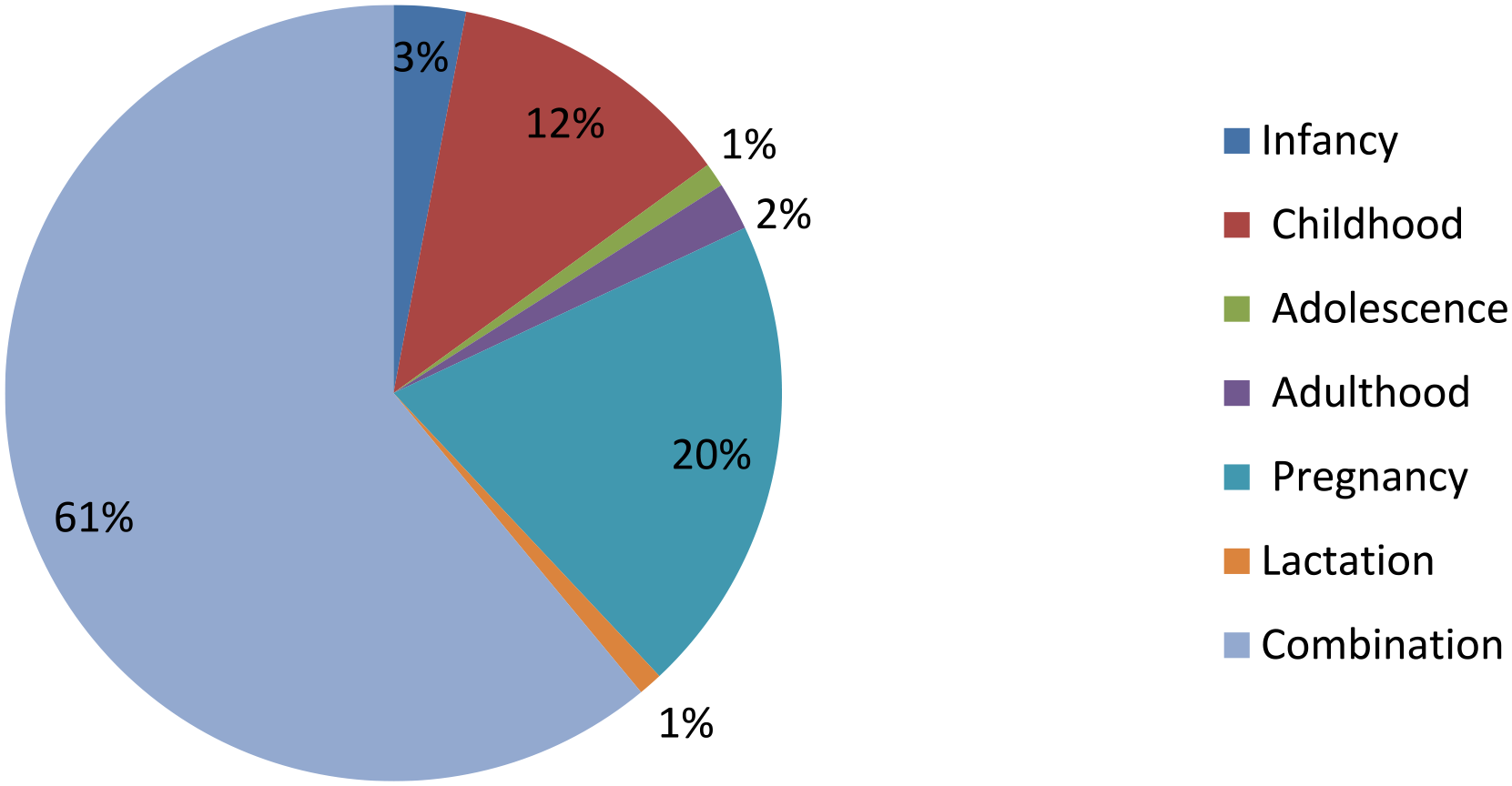
The percentage of participants who counseled individuals in different life stages or with different lifestyles on their nutrition requirements, UOG, 2021.
The three biggest health issues of patients counseled by pharmacists were obesity/overweight (6%), diabetes (15%), and food allergy (16%) (Figure 4).
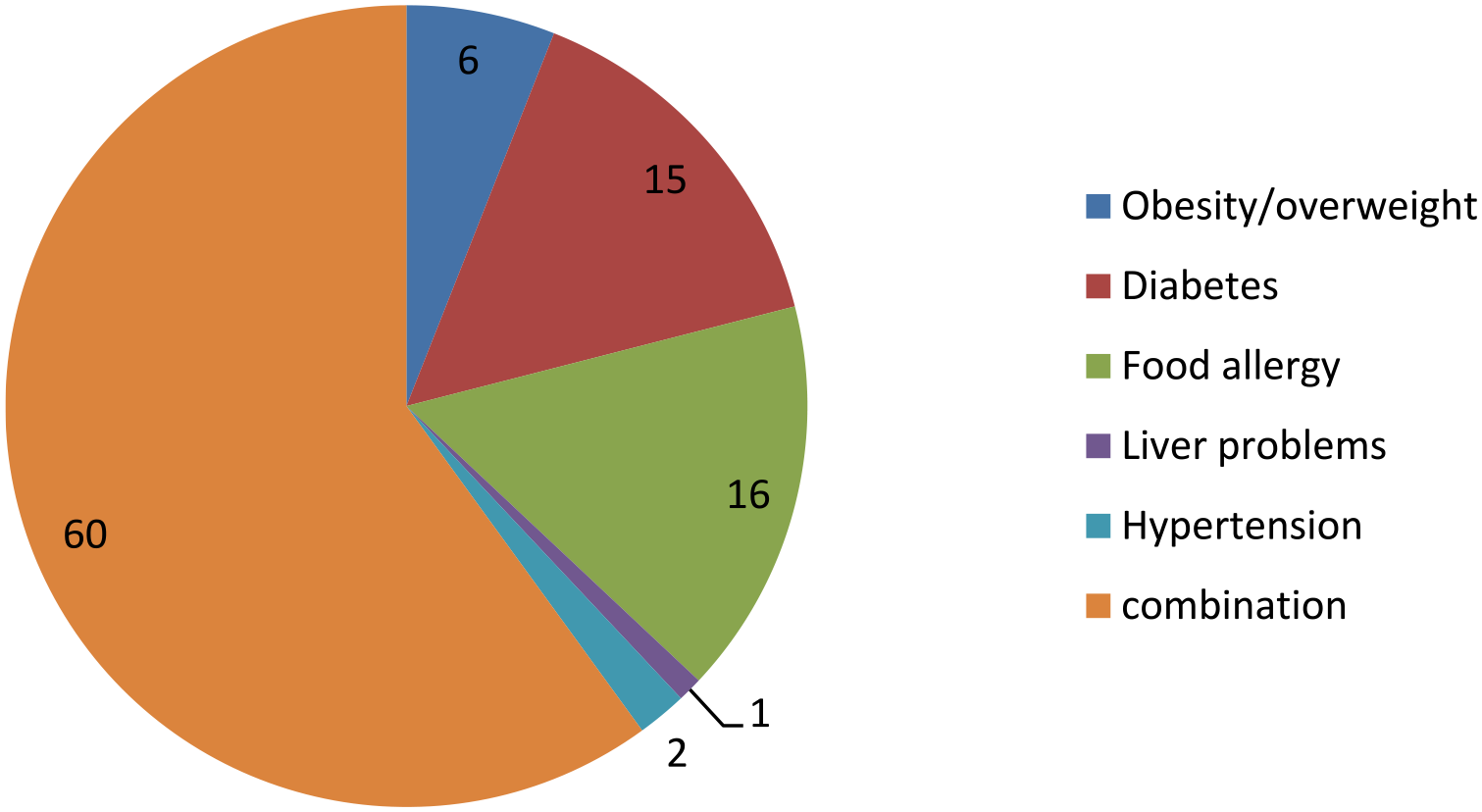
The percentage of participants who counseled patients with different medical conditions at UOG 2021.
More than one-third (41%) of participants provided counseling for customers most of the time about food or meal supplement or replacement safety. More than one-third (44%) of participants gave counseling for patients most of the time to take medicine with food or on an empty stomach. More than one-third (39%) of participants gave counseling to patients most of the time about food-drug interactions. More than one-quarter (29%) of participants gave counseling to patients most of the time about herbal-drug interactions. Nearly one-third (30%) of participants gave counseling to patients most of the time about the safety of using over-the-counter supplements (Table 4).
A detailed breakdown of nutrition-related counseling frequency in Gondar City community pharmacy professionals.

Barriers and strategies for improvement for counseling to nutrition and lifestyle
Lack of patient awareness about pharmacy professionals’ expertise in nutritional counseling 14 (14%), lack of pharmacy professionals, who are expertise nutritional counseling 8 (8%), lack of acceptance 11 (11%), lack of repayment to the pharmacist for counseling by pharmacy professionals’ management 11 (11%) were the most frequent barriers to nutrition counseling. Improvement of pharmacist knowledge about therapeutic medical nutrition 9 (9%), establishing private consultation areas in the pharmacy 8 (8%) and increased public awareness about pharmacists’ abilities for nutritional counseling 7 (7%) were the frequent strategies to overcome barriers (Table 5).
The main barriers to nutrition counseling and appropriate strategies to overcome barriers to nutritional counseling Gondar 2021.

Discussion
This is the primary study used to look at CPPs’ knowledge, attitudes, and practice toward dietary and lifestyle counseling in Ethiopia. Pharmacy professionals have an ethical and professional responsibility to consider the needs and situations of the patients. 20 Pharmaceutical care is the contribution of pharmacy professionals to care for individuals to optimize medicine use and improve health outcomes. 21 Pharmaceutical care services have been expanding simultaneously with the increasing role of pharmacists and the number of prescriptions dispensed. 22 Advancement in pharmacy service demands competent professionals and patient-centered communications. 23 Patient-centered communication is the understanding of patient perspectives, patient psychological and cultural context, and reaching a shared understanding of patient problems concordantly. 20
According to the findings, medical nutrition therapy is characterized by almost one-third of pharmacists as a nutrition treatment to prevent disease and 14% as a nutrition therapy to treat a pre-existing ailment. These findings contrast with those found in Egypt, where more than half of the participants characterized medical nutrition treatment as using nutrition to prevent disease and 40.8% defined it as using nutrition to treat a pre-existing problem. 17
Regarding the role of pharmacists in nutritional assessment, around 88% of the current survey believed that CPPs play a role. The percentage of people who believe CPPs play a role in nutritional assessment is slightly higher than in an Egyptian survey. 17 More than half of our participants believed that therapeutic nutrition is a component of their role and that a physician or dietitian was accountable for this, which is supported by other studies. 17 CPPs believed that patients should receive a combination of diet and pharmacological treatment in most circumstances, which was a significant difference from the Cairo study. 17
Pharmacist knowledge level about contraindications, adverse effects, and efficacy was not up to their knowledge level about dietary supplement interaction, indication, dosage, and rate of administration. These findings are comparable with an Australian study that found that only around 15% of community pharmacists were confident in addressing questions concerning the safety, interactions, side effects, and advantages of complementary and alternative medications. 24 Using high-quality literature sources, a study conducted in Jordan found that pharmacists were less knowledgeable of exact dosages, drug interactions, adverse effects, and expert advice on vitamin supplements. 25
To avoid misuse, around half of the participants thought that dietary supplements considered therapeutic nutrition to be part of their duties and that they must be provided according to a dietician’s or physician’s prescription. These views are similar to those of pharmacists in the United States and Canada, who are evenly divided on the safety and efficacy of dietary supplements. Due to a lack of appropriate or consistent information about these items, almost 50% of American and Canadian pharmacists believe that dietary supplements are unsafe.17,26
Instead of counseling people in other life stages, the majority of participants counseled adults and pregnant women. This result is similar to one obtained in Egypt, 17 but it differs from one obtained in the United Kingdom (UK), in which pharmacy staff were able to provide suitable healthy eating recommendations to consumers of various ages, sexes, and lifestyles. They also used the Eat Well guide to promote healthy eating messaging and to assist customers in understanding food labels, choosing healthier options, and avoiding allergens. 27 This research highlights the need for pharmacy professionals to gain a better understanding of nutritional needs at various periods of life. Similarly, a Nigerian study found that CPPs should be promoted as promoters, facilitators, and implementers of maternal, newborn, and child health. 28 Diabetes mellitus, food allergies, and obesity were the three leading medical disorders of patients who were counseled by pharmacists, which supported our findings. An Egyptian study backs up this conclusion. 17
Participants seldom conducted any counseling on herbal–drug combinations, contraindications, or warnings on particular meals, supplements, or food substitutes, or signs of hypovitaminosis or hypervitaminosis, as a mirror reflection of their lack of expertise. Similarly, according to a study conducted in Jordan and Egypt, pharmacists are less likely to offer information on potential interactions between vitamin supplements and concurrent drugs.17,25 Furthermore, according to a comprehensive analysis conducted in the United States and Canada, the majority of pharmacists wanted more training on dietary supplements, particularly on interactions, adverse effects, patient counseling points, therapeutic uses, and dose. 26
The current study reported that lack of patient awareness about pharmacist expertise in nutritional counseling, lack of pharmacists who are experts in nutritional counseling, and lack of patient demands to counsel were major limitations of nutrition counseling. Other studies have found that pharmacists’ lack of understanding, experience in nutrition counseling, lack of knowledge, inadequate training, and lack of practice guidelines are impediments to public health promotion services.17,18,28 However, the study conducted in Sudan indicated that the main barriers to counseling patients about positive lifestyle changes, nutrition, and dietary supplements were lack of knowledge, lack of time for counseling, lack of expertise in counseling, lack of patient demand, lack of patient demand for counseling. 29
Evidence-based nutrition training is needed to create the capacity and expertise that healthcare workers require to treat patients, according to the Forgotten Medicine Conference in London. 30 Several healthcare professionals, including pharmacists, lack the basic knowledge to advise patients on nutritional regimens.31–33 The Association for Nutrition in the United Kingdom, which is responsible for defining and advancing evidence-based nutrition practice standards, was prompted to develop core competencies in nutrition after pharmacists’ increased role in providing dietary advice and a lack of diet and health training.34,35 Understanding these barriers, as well as pharmacists’ extensive interactions with patients, their high accessibility, the positive impact of pharmacists’ public healthcare services, the insufficient number of dieticians, 34 and the insufficient information of nurses and physicians31–33 may be driving interest in including nutritional science in pharmacists’ undergraduate curricula, continuing education programs, post-graduate studies, and training.
Regarding the community pharmacists’ belief that nutritional counseling should be provided based on their observations (malnutrition, obesity, symptoms of vitamin deficiency, etc.) our findings are similar to Egypt’s study. 17 In contrast to the Egyptian study nutritional counseling based on patients’ diagnoses (diabetes, hypertension, gout, etc.) was higher in this study.
In comparison to the Egyptian study, where nearly all participants said they didn't have any flyers or educational materials to help them provide nutrition counseling, our findings revealed that a smaller percentage of respondents said they didn’t have any flyers or educational materials to help them provide nutrition counseling. However, our findings revealed that the majority of our participants rely on leaflets and internet sources for information provided by medical representatives of manufacturing businesses, as reported by health authorities in our study (FMHACA, Zone Health Bureau). 17 Therefore, the knowledge of CPPs about nutrition and lifestyle counseling is extremely important to improve society’s overall health. The federal minister of health and other concerned bodies would cooperate to increase the knowledge, attitude, and practice of CPPs.
Implication of the study
Improving CPPs’ knowledge about nutritional requirements could expand their ability to provide nutrition counseling services and healthy eating advice for the needs of different populations, including infants, children, pregnant women, lactating women, geriatrics, and patients with different chronic disorders. The confidence in dispensing dietary supplements and the frequency of counseling may be improved by increasing professionals’ knowledge about dietary supplements such as their efficacy, indications, dosage, frequency of administration, adverse effects of drug interaction, and contraindications. Pharmacy professional’s positive attitude toward nutritional assessments and medical nutrition therapy could predict a promising role of community pharmacists in nutrition counseling as a health promotion service that needs to be supported to reach its maximum benefit
Limitations
The study was a single center with a smaller number of participants. In addition, the study looked at dietary supplements as a whole. Power analysis for sample size calculation was not done and we have used purposive sampling which might be exposed to a certain bias. If vitamins, herbal supplements, and complementary foods were tested separately, different results might have been found. We suggest the future prospective multicenter study with a larger sample size to assess vitamins, herbal supplements, and complementary foods separately using a systematic random sampling technique to reduce the chance of bias. We also suggest that future prospective multicenter studies with larger sample sizes assess the impact of health outcomes through nutrition and lifestyle counseling.
Conclusion
The majority of CPPs rated their medical nutrition therapy knowledge as near-excellent. They knew more about therapeutic nutrition and taking medicine with food or on an empty stomach than they did about the dose, a dietary supplement’s indication, efficacy, contraindications, precautions, adverse effects, and drug–supplement interactions. CPPs have a good attitude toward nutritional assessment and medical nutrition therapy, and these tasks are considered part of their job responsibilities. The majority of CPPs on nutrition counseling services were restricted to pregnant women and patients with certain medical issues (i.e., obesity, diabetes, and food allergy). The main hurdles to nutrition counseling were a lack of patient awareness of pharmacist expertise in nutritional counseling and a lack of patient demand for therapy. As a result, curricular requirements and required nutrition and physical activity competencies in pharmacists’ education, training, and continuing education are needed to increase their nutrition education and knowledge.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241256569 – Supplemental material for Community pharmacy professionals’ knowledge, attitude, and practice toward nutrition and lifestyle counseling in Gondar City, Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121241256569 for Community pharmacy professionals’ knowledge, attitude, and practice toward nutrition and lifestyle counseling in Gondar City, Ethiopia by Eyayaw Ashete Belachew, Biniam Siyum Shibe, Aschalew Mulatu Tefera and Samuel Agegnew Wondm in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to acknowledge the study participants, data collectors, and supervisors in conducting this study.
Authors’ contributions
All authors contributed significantly to the work reported, whether in the conception, study design, execution, data acquisition, analysis, and interpretation, or all of these areas; participated in the drafting, revising, or critical evaluation of the article; gave agreement of the version to be published; agreed on the journal to which the article was submitted.
Availability of data and material
The materials and data of this study are available from the corresponding author upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study was ethically approved by the University of Gondar Institutional Review Committee with reference number (UOG-SOP 262/2021). Before the study, the study participants were given written and verbally informed permission to discuss the study’s purpose and objectives. Respondents were told of the study’s goal, why they were chosen, and what was expected of them during the consent process. They were also told that they could withdraw from the study at any point during it. Participants were also informed that any information gathered during the research would be kept private. Personal identifiers were not used throughout data collection to maintain respondents’ anonymity.
Consent for publication
All authors consent to this manuscript’s publication.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.