
Abstract
Introduction. Breastfeeding practices fall short of optimal levels globally, despite its known health benefits and World Health Organization endorsements. We aimed through this study to firstly estimate the global prevalence of principal indicators of breastfeeding practice in Tunisia. Secondly, we aimed to identify their associated factors and to assess the temporal trend of breastfeeding practice in Tunsia from 2000 to 2018. Methods. We extracted data from all available reports of Multiple Indicator Cluster Surveys (MICS) surveys conducted in Tunisia (MICS2000, 2006, 2012 and 2018) that were publicly available on the MICS UNICEF website prior to 2024. Results. Never breastfeeding prevalence was 4% (95% CI [3%-7%]) with a significant increase (P < 10−3) from 2000 (2.4%) to 2018(7.8%). The prevalence of early breastfeeding initiation was 56% (95% CI [20%-87%]) with a significant decrease(P < 10−3) from 2006(87.4%) to 2018(31.5%). The prevalence of exclusive breastfeeding was 15% (95% CI [5%-35%]) with a significant decrease(P < 10−3) from 2000(46.4%) to 2018(13.4%). The prevalence of predominant breastfeeding was 41% (95% CI [31%-51%]) with a significant decrease(P < 10−3) from 2000(50.5%) to 2018(30.4%). The prevalence of continued breastfeeding up to the age of 2 years was 19% (95% CI [16%-22%]) with no significant decrease from 2000 to 2018(P = .09). The mother educational level was significantly associated with early breastfeeding initiation, exclusive and predominant breastfeeding. A higher prevalence of exclusive breastfeeding was found among mothers from rural areas. Conclusions. Tunisia has been experiencing low rates of breastfeeding practice, with a concerning decline observed over the years. Addressing this issue effectively necessitates a comprehensive, multi-faceted approach that encompasses various aspects of society, healthcare, and policymaking.
Introduction
Breastfeeding is an ideal, safe, and ecological source of nutrients and immune factors promoting optimal growth and development while reducing the risk of infections and chronic diseases such as obesity and diabetes.1,2 It provides many health benefits for both infant and mother health.3,4 It has been demonstrated that breastfeeding can have long-term repercussions on health even in adulthood.5,6 Not breastfeeding increased infant mortality, especially in low and middle-income countries, due to infections and illness such as pneumonia and diarrhea. 7
The United Nations International Children’s Emergency Fund (UNICEF) and The World Health Organization (WHO) advocates for early initiation of breastfeeding within 1 hour after birth, for exclusive breastfeeding during the first 6 months of life, and for continued breastfeeding until 2 years and beyond. 8
Breastfeeding practices fall short of optimal levels recommended by the WHO, despite its known health benefits. According to the WHO, fewer than half (44%) of infants aged 0 to 6 months worldwide are exclusively breastfed which falls below the global WHO target of 50% by 2025 and at least 70% by 2030. 8 Many children do not start breastfeeding early enough, are not exclusively breastfed for the recommended 6 months, or stop breastfeeding too early. Breastfeeding frequency tends to decline rapidly a few months after birth with early introduction of foods and reliance on breast-milk substitutes as an easy alternative which may contribute to the early cessation of breastfeeding.9,10
In Tunisia, there is a lack of recent studies on breastfeeding prevalence, and the few existing ones are not updated and conducted on small, non-representative samples, among diverse settings in various regions of the country, with no standardized study designs and outcomes definitions.11-13 According to these studies, the practice of exclusive breastfeeding for 6 months appears to be low and varies widely from 1.9% to 41.5%.11,12
While few studies have assessed the prevalence and determinants of breastfeeding in various regions of Tunisia, there is a need to consolidate existing data and provide a comprehensive understanding of breastfeeding practices nationwide.
Multiple Indicator Cluster Surveys (MICS) are national surveys conducted in Tunisia regularly from 2000 and the last one dates from 2018. These surveys essentially estimate prevalence of standard breastfeeding indicators.
Aggregating all the breastfeeding relating data available from MICS surveys, will enable us to enhance our understanding of breastfeeding behaviors from national standardized surveys, visualizing temporal trends and understanding the factors influencing breastfeeding practices across the country from a large representative sample size.
We aimed through this study to firstly estimate the pooled prevalence of principal indicators of breastfeeding practice (never breastfeeding, early initiation of breastfeeding within the first hour following birth, exclusive and predominant breastfeeding during the first 6 months, continued breastfeeding up to the age of 2 years), in Tunisia. Secondly, we aimed to identify the associated factors of practicing breastfeeding and to assess the temporal trend of principal indicators of breastfeeding practice in Tunsia from 2000 to 2018.
Methodology
Study Design, Data Source and Study Population
This was a review study of all MICS surveys conducted in Tunisia, utilizing information solely available from the official UNICEF MICS website.
MICSs are population-based cross-sectional household surveys using similar sampling strategies and standardized questionnaires carried out at approximately 6-year intervals in Tunisia since 2000. We extracted data from all available reports of MICS surveys conducted in Tunisia (MICS 2000, 2006, 2012 and 2018) that were publicly available on the MICS UNICEF website 14 prior to 2024.
MICS data were collected in standardized face-to- face interviews with respondents, using the method of Computer-Assisted Personal Interviewing (CAPI) and based on a set of globally recommended standardized questionnaires. The questionnaires are tested on a small sample of households before starting the data collection.
The study sample of all MICS surveys comprised all mothers who had a live birth in the 24 months preceding the survey.
Measurement of Outcomes
the main outcomes of interest for this study were the pooled prevalence of 5 principal indicators of breastfeeding practice:
-
Number of children who were never breastfed/ Number of last-born children born alive in the last 2 years.
-
-
Number of infants who were exclusively breastfed during the first 6 months/Number of infants aged between 0 and 5 months.
*
-
Number of infants who receive breastfeeding as the predominant source of food / Number of infants aged between 0 and 5 months
*
-
Number of children aged 20 to 23 months who continue to receive breastmilk/ Number of infants aged between 20 and 23 months
Data Collection
Data for our study was extracted from the included MICS studies reports and the following information were reported for each study whenever it was available: the year of conduction; the prevalence of breastfeeding indicators (never breastfeeding, early breastfeeding initiation, exclusive breastfeeding, predominant breastfeeding and continued breastfeeding up to the age of 2 years) for each MICS study; the stratified prevalence of each breastfeeding indicator, by infant sex, region, environment of residence, place of birth, mother educational level and economic well-being index.
Data Analysis
The prevalence of each of the of the 5 breastfeeding indicators was combined by applying a random-effects model meta-analysis using the inverse variance method with implementation of logit transformations of proportions. 15
Breastfeeding indicators were assessed with the following risk factors (binary variables) whenever it was possible, and information was available from included MICS reports:
-Infant sex: Male or female.
-Region of the country: Noth or center/south.
Environment of residence: Urban or rural.
Place of birth: Public or private healthcare structure.
Mother educational level: Illiterate /primary or secondary/Higher.
Economic well-being index: The poorest or other status (Second/medium/fourth/the richest).
Associations between these risk factors and each breastfeeding indicator were assessed using pooled odds ratios (OR) as outcome measures using random-effects models. A P-value ≤.05 was considered as significant.
Between-studies heterogeneity was assessed using Higgins’s I-Squared statistic (I2) and Cochran’s Q-statistics (Q test). 16 Statistical significance for Q test is set at P < .05. 17
Pearson’s Chi-squared Test was used to assess if there is a significant difference for each breastfeeding indicator between the latest and the oldest MICS study.
All analyses were performed with the statistical R-Soflware (version 4.2.3; R Core Team, 2020), using package meta.
Ethical Approval and Informed Consent
The ethical approval was not needed because all data utilized are published, openly accessible and thoroughly anonymized.
Results
Breastfeeding Indicators and Their Associated Factors
Never breastfeeding indicator
Pooled prevalence of children who were never breastfed
The pooled prevalence of children who were never breastfed was 4% (95% CI [3%-7%]), among an overall sample size of 5594 (from MICS 2000, 2006, 2012 and 2018). The results were heterogenous (I2=93%; 95% CI [85% -97%]; P < .01), (Figure 1).

Forest plot of pooled prevalence of children who were never breastfed according to the MICS Tunisian surveys (2000-2006-2012-2018).
The stratified pooled prevalence of never breastfeeding is represented in Table 1. The pooled prevalence of never breastfeeding was higher in urban then rural environment (5% [4%-7%] and 3% [1%-6%] respectively). At regional level, results were comparable with prevalence variation from 4% to 5%. A higher prevalence of 36% was reported among illiterate mothers compared to other mother educational levels. When considering place of birth, this prevalence was 5% in both public and private structures. This prevalence varied between 4% and 6% within the different levels of economic well-being index.
Stratified Pooled Prevalence of Never Breastfeeding by Socioeconomic and Demographic Characteristics of Mothers (Data From Tunisian MICS 2000-2006-2012-2018).

Associated factors to never breastfeeding
1.
Two MICS studies (2012-2018) were included in the analysis with a total of 2371 mothers. The place of birth (Public structure compared private structure) was not significantly associated with never breastfeeding (pooled OR = 0.85; 95% CI [0.53-1.37]; P = .5; Table 2). According to the Q-test, the result was homogenous (P = .29) and I2= 9%. The Forest plot is illustrated in Figure 2A.
Associated Factors to Never Breastfeeding (Combined Results From Tunisian MICS Surveys).

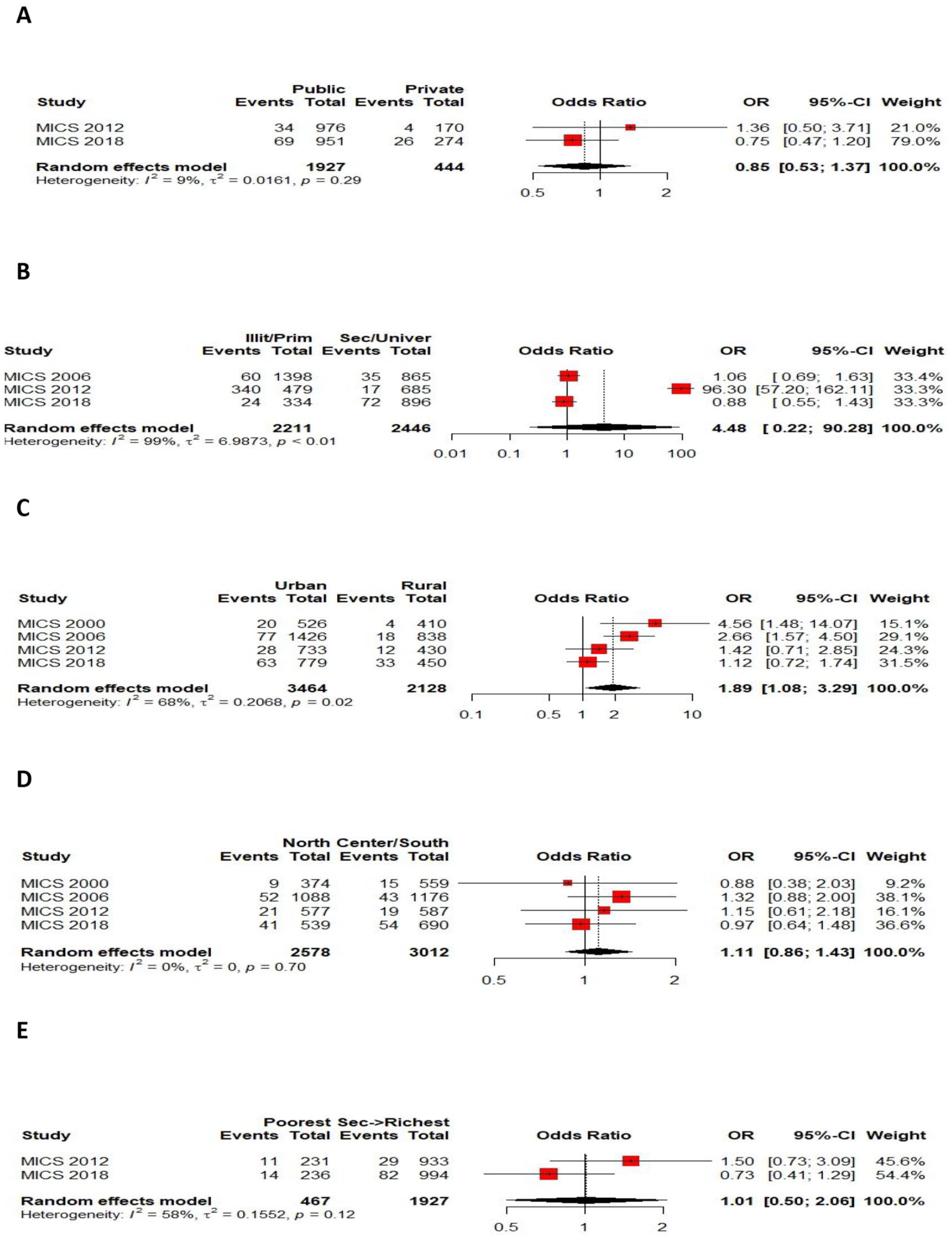
Forest plots of the pooled OR estimating the association between Never breastfeeding and: (A) Place of birth; (B) Mother Educational level; (C) Environment of residence; (D) Region of the country; (E) economic well-being level.
2.
Three MICS studies (2006-2012-2018) were included in the analysis with a total of 4657 mothers. The mother educational level (Primary or less compared to secondary or higher) was not significantly associated with never breastfeeding (pooled OR = 4.48; 95% CI [0.22-90.28]; P = .32; Table 2). According to the Q-test, the result was heterogenous (P < .01) and I2= 99%. The Forest plot is illustrated in Figure 2B.
3.
Four MICS studies (2000-2006-2012-2018) were included in the analysis with a total of 5592 mothers. The environment of residence (Urban compared to rural) was significantly associated with never breastfeeding with a higher prevalence in urban area (pooled OR = 1.89; 95% CI [1.08-3.29]; P = .02; Table 2). According to the Q-test, the result was heterogenous (P = .02) and I2 = 68%. The Forest plot is illustrated in Figure 2C.
4.
Four MICS studies (2000-2006-2012-2018) were included in the analysis with a total of 5590 participants. The never breastfeeding was not significantly different between regions (North of the country compared to the center/south). The pooled OR = 1.11; 95% CI [0.86-1.43]; P = .41; Table 2). According to the Q-test, the result was homogenous (P = .7) and I2= 0%. The Forest plot is illustrated in Figure 2D.
5.
Two MICS studies (2012-2018) were included in the analysis with a total of 2394 mothers. The economic well-being level (the poorest compared to other levels) was not significantly associated with never breastfeeding (pooled OR = 1.01; 95% CI [0.50-2.06]; P = .97; Table 2). According to the Q-test, the result was homogenous (P = .12). The Forest plot is illustrated in Figure 2E.
Early breastfeeding initiation indicator
Pooled prevalence of early breastfeeding initiation
The pooled prevalence of early breastfeeding initiation was 56% (95% CI [20%-87%]), among an overall sample size of 4658 (from MICS 2006, 2012 and 2018). The results were heterogenous (I2=100%; 95% CI [100% -100%]; P < .01; Figure 3).
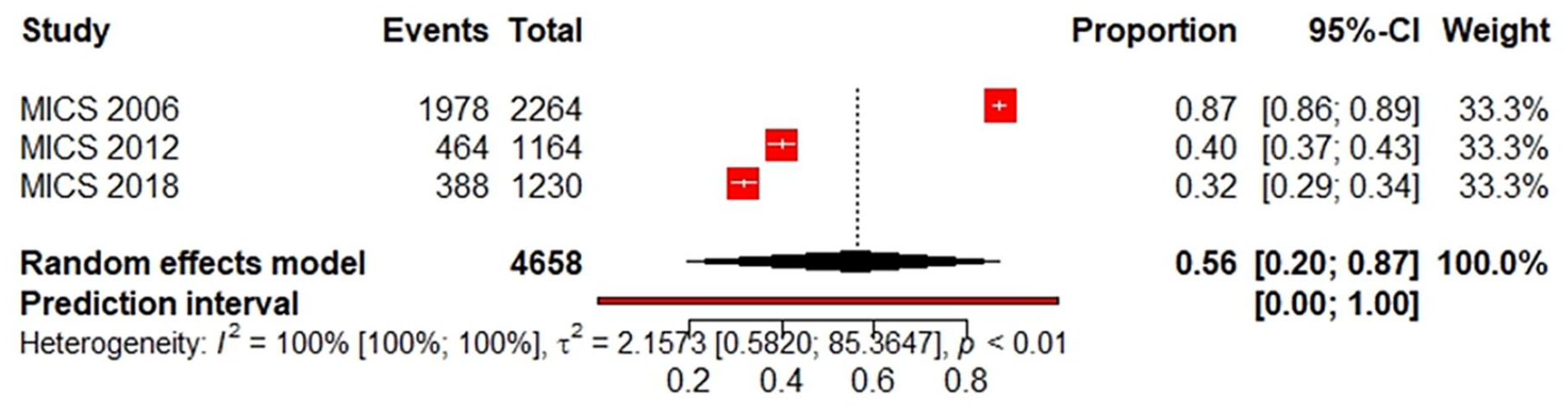
Forest plot of pooled prevalence of early breastfeeding initiation according to the MICS Tunisian surveys (2006-2012-2018).
The stratified pooled prevalence of early breastfeeding initiation is represented in Table 3. The lowest prevalence of early initiation of breastfeeding was noted in private healthcare facilities with a prevalence of 27% [21%-34%]. This prevalence was lower in urban (54%) compared to rural environment, in the Northwest region of the country (48%) compared to other regions, among mothers having a secondary or higher educational level (52%) compared to other educational levels, among mothers who have given birth in a private facility (27%) compared to public facility and among mothers having the richest economic well-being index (31%) compared to other economic levels.
Stratified Pooled Prevalence of Early Breastfeeding Initiation by Socioeconomic and Demographic Characteristics of Mothers (Data From Tunisian MICS 2000-2006-2012-2018).

Associated factors to early breastfeeding initiation
1.
A total of 2 MICS studies (2012-2018) were included in the analysis with a total of 2389 mothers. The place of birth (Public structure compared private structure) was not significantly associated with early breastfeeding initiation (pooled OR = 1.2 (95% CI: 0.97-1.47); P = .08; Table 4). According to the Q-test, the result was homogenous (P = .31) and I2= 2%. The Forest plot is illustrated in Figure 4A.
Associated Factors to the Early Initiation of Breastfeeding (Combined Results From Tunisian MICS Surveys).


Forest plots of the pooled OR estimating the association between early breastfeeding initiation and: (A) Place of birth; (B) Mother Educational level; (C) Environment of residence; (D) Region of the country; (E) economic well-being level.
2.
A total of 3 MICS studies (2006-2012-2018) were included in the analysis with a total of 4657 mothers. The mother educational level (Primary or less compared to secondary or higher) was significantly associated with early breastfeeding initiation higher prevalence among mothers who are illiterate or having a primary educational level (pooled OR = 1.39 (95% CI: 1.05-1.84); P = .02; Table 4). According to the Q-test, the result was heterogenous (P = .03) and I2 = 72%. The Forest plot is illustrated in Figure 4B.
3.
A total of 3 MICS studies (2006-2012-2018) were included in the analysis with a total of 4656 mothers. The environment of residence (rural compared to urban) was not significantly associated with early breastfeeding initiation (pooled OR = 1.25 (95% CI: 0.86-1.81); P = .24; Table 4). According to the Q-test, the result was heterogenous (P = .001) and I2= 85%. The Forest plot is illustrated in Figure 4C.
4.
A total of 3 MICS studies (2006-2012-2018) were included in the analysis with a total of 4657 mothers. The early breastfeeding initiation was significantly different between regions (Center or south of the country compared to the North) with higher prevalence in the center or south of the country compared to the North. The pooled odds ratio OR was equal to 1.22 (95% CI: 1.03-1.44); P = .02), (Table 4). According to the Q-test, the result was homogenous (P = .23) and I2 = 32%. The Forest plot is illustrated in Figure 4D.
5.
A total of 2 MICS studies (2012-2018) were included in the analysis with a total of 2394 mothers. The economic well-being level (the poorest compared to other levels) was not significantly associated with early breastfeeding initiation ( pooled OR = 1.17 (95% CI: 0.91-1.52); P = .22; Table 4). According to the Q-test, the result was homogenous (P = .22) and I2= 34%. The Forest plot is illustrated in Figure 4E.
Exclusive breastfeeding during the first 6 months
Pooled prevalence of exclusive breastfeeding during the first 6 months
The pooled prevalence of exclusive breastfeeding during the first 6 months was 15% (95% CI [5%-35%]), among an overall sample size of 1841 (from MICS 2000, 2006, 2012 and 2018). The results were heterogenous (I2=99%; 95% CI [98% -99%]; P < .01; Figure 5).
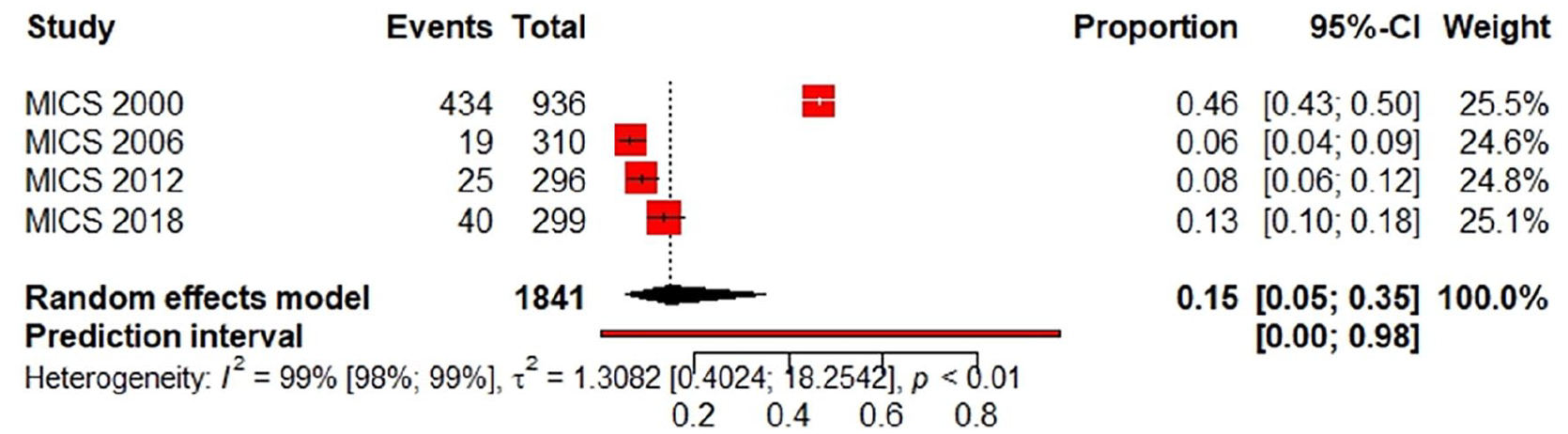
Forest plot of pooled prevalence of exclusive breastfeeding during the first 6 months according to the MICS Tunisian surveys (2000-2006-2012-2018).
The stratified pooled prevalence of exclusive breastfeeding during the first 6 months is represented in Table 5. This prevalence was lower in urban (14%) compared to rural environment, in the Northeast region of the country (9%) compared to other regions, among mothers having a secondary or higher educational level (7%) compared to other educational levels and among mothers having a medium economic well-being index (5%) compared to other economic levels.
Stratified Pooled Prevalence of Exclusive Breastfeeding During the First 6 Months by Socioeconomic and Demographic Characteristics of Mothers (Data From Tunisian MICS 2000-2006-2012-2018).

Associated factors to exclusive breastfeeding during the first 6 months
1.
A total of 3 MICS studies (2006-2012-2018) were included in the analysis with a total of 905 mothers. The infant sex (male compared to female) was not significantly associated with exclusive breastfeeding practice during the first 6 months (pooled OR = 1.07 (95% CI: 0.68-1.70); P = .76; Table 6). According to the Q-test, the result was homogenous (P = .39) and I2 = 0%. The Forest plot is illustrated in Figure 6A.
Associated Factors to the Exclusive Breastfeeding Practice During the First 6 Months (Combined Results From Tunisian MICS surveys).

2.

Forest plots of the pooled OR estimating the association between exclusive breastfeeding practice and: (A) Infant sex; (B) Mother Educational level; (C) Environment of residence; (D) Region of the country; (E) economic well-being level.
A total of 3 MICS studies (2006-2012-2018) were included in the analysis with a total of 897 mothers. The mother educational level (Primary or less compared to secondary or higher) was significantly associated with exclusive breastfeeding practice during the first 6 months with higher prevalence among mothers who are illiterate or having a primary educational level (pooled OR = 2.27 (95% CI: 1.36-3.79); P = .001; Table 6). According to the Q-test, the result was homogenous (P = .61) and I2 = 0%. The Forest plot is illustrated in Figure 6B.
3.
A total of 4 MICS studies (2000-2006-2012-2018) were included in the analysis with a total of 1841 mothers. The environment of residence (rural compared to urban) was significantly associated with exclusive breastfeeding practice during the first 6 months with higher prevalence among mothers from rural area (pooled OR = 1.27 (95% CI: 1.01-1.59); P = .04; Table 6). According to the Q-test, the result was homogenous (P = .65) and I2= 0%. The Forest plot is illustrated in Figure 6C.
4.
A total of 3 MICS studies (2000-2012-2018) were included in the analysis with a total of 1527 mothers. The exclusive breastfeeding practice during the first 6 months was not significantly different between regions (Center or south of the country compared to the North). The pooled OR = 1.82; 95% CI [0.87-3.79]; P = .1; Table 6). According to the Q-test, the result was heterogenous (P = .05) and I2 = 66%. The Forest plot is illustrated in Figure 6D.
5.
A total of 2 MICS studies (2012-2018) were included in the analysis with a total of 596 mothers. The economic well-being level (the poorest compared to other levels) was significantly associated with exclusive breastfeeding practice during the first 6 months with higher prevalence among mothers having the poorest economic level (pooled OR = 1.86 (95% CI: 1.03-3.36); P = .04; Table 6). According to the Q-test, the result was homogenous (P = .39) and I2 = 0%. The Forest plot is illustrated in Figure 6E.
Predominant breastfeeding during the first 6 months
Pooled prevalence of predominant breastfeeding during the first 6 months
The pooled prevalence of predominant breastfeeding during the first 6 months was 41% (95% CI [31%-51%]), among an overall sample size of 1841 (from MICS 2000, 2006, 2012 and 2018). The results were heterogenous (I2 = 94%; 95% CI [88%-97%] with P < .01; Figure 7).

Forest plot of pooled prevalence of predominant breastfeeding during the first 6 months according to the MICS Tunisian surveys (2000-2006-2012-2018).
The stratified pooled prevalence of predominant breastfeeding during the first 6 months is represented in Table 7. The lowest prevalence of predominant breastfeeding during the first 6 months was noted among mothers having the richest level of economic well being with a prevalence of 23% [16%-32%]. This prevalence was lower in urban (39%) compared to rural environment, in the Center East region of the country (33%) compared to other regions and, among male infant sex (34%) compared to female and among mothers having a secondary or higher educational level (33%) compared to the other educational levels.
Stratified Pooled Prevalence of Predominant Breastfeeding During the First 6 Months by Socioeconomic and Demographic Characteristics of Mothers (Data From Tunisian MICS 2000-2006-2012-2018).

Associated factors to predominant breastfeeding during the first 6 months
1.
A total of 3 MICS studies (2006-2012-2018) were included in the analysis with a total of 905 mothers. The infant sex (male compared to female) was not significantly associated with predominant breastfeeding during the first 6 months (pooled OR = 0.82 (95% CI: 0.61-1.09); P = .16; Table 8). According to the Q-test, the result was homogenous (P = .34) and I2 = 8%. The Forest plot is illustrated in Figure 8A.
Associated Factors to Predominant Breastfeeding During the First 6 Months (Combined Results From Tunisian MICS Surveys).


Forest plots of the pooled OR estimating the association between predominant breastfeeding practice and: (A) Infant sex; (B) Mother Educational level; (C) Environment of residence; (D) Region of the country; (E) economic well-being level.
2.
A total of 3 MICS studies (2006-2012-2018) were included in the analysis with a total of 897 mothers. The mother educational level (Primary or less compared to secondary or higher) was significantly associated with predominant breastfeeding during the first 6 months with higher prevalence among mothers who are illiterate or having a primary educational level (pooled OR = 1.39 (95% CI: 1.04-1.85); P = .02; Table 8). According to the Q-test, the result was homogenous (P = .96) and I2 = 0 %. The Forest plot is illustrated in Figure 8B.
3.
A total of 4 MICS studies (2000-2006-2012-2018) were included in the analysis with a total of 1841 mothers. The environment of residence (rural compared to urban) was not significantly associated with predominant breastfeeding during the first 6 months (pooled OR = 1.19 (95% CI: 0.88-1.62); P = .26; Table 8). According to the Q-test, the result was heterogenous (P = .09) and I2 = 54%. The Forest plot is illustrated in Figure 8C.
4.
A total of 3 MICS studies (2000-2012-2018) were included in the analysis with a total of 1527 mothers. The predominant breastfeeding during the first 6 months was significantly different between regions (North of the country compared to center or south) with a higher prevalence in the North. The pooled odds ratio (OR) was equal to 1.31 (95% CI: 1.06-1.61); P = .01; Table 8). According to the Q-test, the result was homogenous (P = .93) and I2 = 0%. The Forest plot is illustrated in Figure 8D.
5.
A total of 2 MICS studies (2012-2018) were included in the analysis with a total of 596 mothers. The economic well-being level (the poorest compared to other levels) was significantly associated with predominant breastfeeding during the first 6 months with a higher prevalence among mothers having the poorest economic level (pooled OR = 1.62 (95% CI: 1.06-2.50); P = .02; Table 8). According to the Q-test, the result was homogenous (P = .88) and I2 = 0%. The Forest plot is illustrated in Figure 8E.
Continued breastfeeding up to the age of 2 years
Pooled prevalence of continued breastfeeding up to the age of 2 years
The pooled prevalence of continued breastfeeding up to the age of 2 years was 19% (95% CI [16%-22%]), among an overall sample size of 1272 (from MICS 2000, 2006, 2012 and 2018). The results were not homogenous (I2=44%; 95% CI [0%-81%] with P = .15), (Figure 9).

Forest plot of pooled prevalence of continued breastfeeding up to the age of 2 years according to the MICS Tunisian surveys (2000-2006-2012-2018).
The stratified pooled prevalence of continued breastfeeding up to the age of 2 years is represented in Table 9. The lowest prevalence of continued breastfeeding up to the age of 2 years was noted among mothers having a secondary or higher educational level with a prevalence of 12% [7%-19%]. This prevalence was lower in urban (17%) compared to rural environment, in the Northeast region of the country (16%) compared to other regions and among mothers having fourth level of economic well being (13%) compared to the other economic levels.
Stratified Pooled Prevalence of Continued Breastfeeding up to the Age of 2 Years by Socioeconomic and Demographic Characteristics of Mothers (Data From Tunisian MICS 2000-2006-2012-2018).

Associated factors to continued breastfeeding up to the age of 2 years
1.
A total of 4 MICS studies (2000-2006-2012-2018) were included in the analysis with a total of 1273 mothers. The infant sex (male compared to female) was not significantly associated with continued breastfeeding up to the age of 2 years (pooled OR = 0.96 (95% CI: 0.73-1.27); P = .79; Table 10). According to the Q-test, the result was homogenous (P = .57) and I2 = 0%. The Forest plot is illustrated in Figure 10A.
Associated Factors to Continued Breastfeeding up to the Age of 2 Years (Combined Results From Tunisian MICS Surveys).


Forest plots of the pooled OR estimating the association between continued breastfeeding up to the age of 2 years and: (A) Infant sex; (B) Mother Educational level; (C) Environment of residence; (D) Region of the country; (E) economic well-being level.
2.
A total of 4 MICS studies (2000-2006-2012-2018) were included in the analysis with a total of 1267 mothers. The mother educational level (Primary or less compared to secondary or higher) was not significantly associated with continued breastfeeding up to the age of 2 years (pooled OR = 2.13 (95% CI: 0.95-4.78); P = .06; Table 10). According to the Q-test, the result was heterogeneous (P = .007) and I2 = 75%. The Forest plot is illustrated in Figure 10B.
3.
A total of 4 MICS studies (2000-2006-2012-2018) were included in the analysis with a total of 1272 mothers. The environment of residence (rural compared to urban) was not significantly associated with continued breastfeeding up to the age of 2 years (pooled OR = 1.4 (95% CI: 0.98-2.02); P = .06; Table 10). According to the Q-test, the result was homogenous (P = .32) and I2= 15%. The Forest plot is illustrated in Figure 10C.
4.
A total of 3 MICS studies (2000-2006-2018) were included in the analysis with a total of 1085 mothers. The continued breastfeeding up to the age of 2 years was not significantly different between regions (Center or south of the country compared to the North). The pooled OR was equal to 0.78 (95% CI: 0.56-1.09); P = .14; Table 10). According to the Q-test, the result was homogenous (P = .38) and I2 = 0%. The Forest plot is illustrated in Figure 10D.
5.
A total of 2 MICS studies (2012-2018) were included in the analysis with a total of 407 mothers. The economic well-being level (the poorest compared to other levels) was not significantly associated with continued breastfeeding up to the age of 2 years (pooled OR = 1.12 (95% CI: 0.52-2.42); P = .76; Table 10). According to the Q-test, the result was homogenous (P = .2) and I2= 39%. The Forest plot is illustrated in Figure 10E.
Breastfeeding Trends
Temporal trend of never breastfeeding
The prevalence of children who were never breastfed increases significantly (P < 10−3) from 2000 (2.4%) to 2018 (7.8%); (Figure 11).
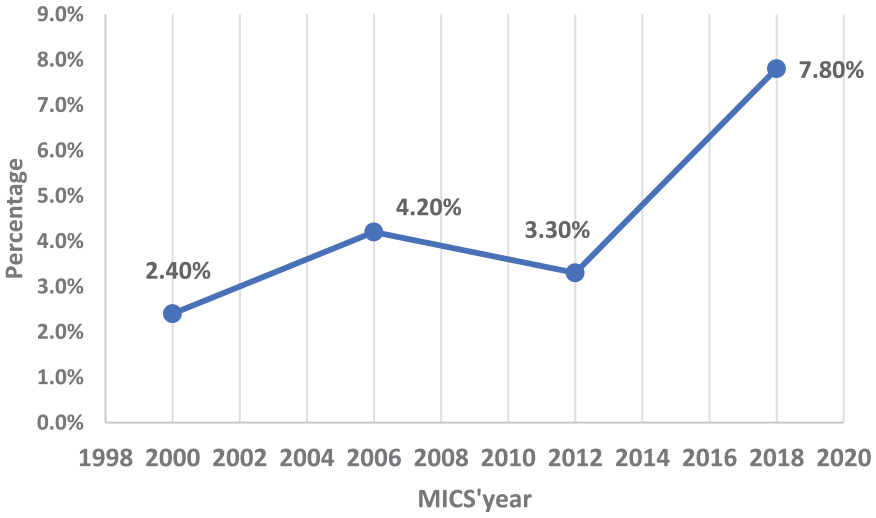
Trend of prevalence of children who were never breastfed according to the MICS Tunisian surveys (2000-2006-2012-2018).
Temporal trend of early breastfeeding initiation
The prevalence of early breastfeeding initiation decreases significantly(P < 10−3) from 2006 (87.4%) to 2018 (31.5%); (Figure 12).

Trend of early initiation of breastfeeding according to the MICS Tunisian surveys (2006-2012-2018).
Temporal trend of exclusive breastfeeding during the first 6 months
The prevalence of exclusive breastfeeding during the first 6 months decreases significantly (P < 10−3) from 2000 (46.4%) to 2018 (13.4%); (Figure 13).

Trend of the prevalence of exclusive breastfeeding during the first 6 months according to the MICS Tunisian surveys (2000-2006-2012-2018).
Temporal trend of predominant breastfeeding during the first 6 months
The prevalence of predominant breastfeeding during the first 6 months decreases significantly (P < 10−3) from 2000 (50.5%) to 2018 (30.4%; Figure 14).

Trend of the prevalence of predominant breastfeeding during the first 6 months according to the MICS Tunisian surveys (2000-2006-2012-2018).
Temporal trend of continued breastfeeding up to the age of 2 years
Months
There was no significant decrease (P = .09) of the prevalence of continued breastfeeding up to the age of 2 years from 2000 to 2018 (Figure 15).

Trend of the prevalence of continued breastfeeding up to the age of 2 years according to the MICS Tunisian surveys (2000-2006-2012-2018).
Discussion
We summarized evidence of breastfeeding practice from results of four published Tunisian MICS surveys reports from 2000 to 2018.
Never breastfeeding prevalence, early breastfeeding initiation, exclusive breastfeeding, predominant breastfeeding and continued breastfeeding up to the age of 2 years were 4% (95% CI [3%-7%]); 56% (95% CI [20%-87%]); 15% (95% CI [5%-35%]), 41% (95% CI [31%-51%]) and19% (95% CI [16%-22%]), respectively.
Breastfeeding practice in Tunisia was globally low compared to other countries of the Middle east and North Africa (MENA) region, especially concerning exclusive breastfeeding, and continued breastfeeding until 2 years.
The results of the latest MICS studies conducted in countries of the MENA region are summarized in the Table 11. 14 Never breastfeeding ranged from 4.1% in Palestine to 12.9% in Algeria. Early breastfeeding initiation ranged from 32.4% in Iraq to 68.7% in Sudan. Exclusive breastfeeding ranged from 2.2% in Yemen to 55.4% in Sudan. Predominant breastfeeding ranged from 5.6% in Yemen to 80.8% in Sudan. And continued breastfeeding until 2 years ranged from 11.3% in Palestine to 48.8% in Sudan. We have acceptable prevalence of never breastfeeding and early breastfeeding initiation comparing to these rates. But our rates of exclusive, predominant and continued breastfeeding were among the lowest in the region (Table 11).
Breastfeeding Practice Among Countries of Middle East and North Africa According to the Latest MICS Surveys.

Abbreviation: BF, breastfeeding.
The prevalence of exclusive breastfeeding practice in the Eastern Mediterranean Region, varies across countries. In the Eastern Mediterranean Region, the regional average for exclusive breastfeeding was estimated at 30.9%, with the lowest rates observed in Yemen (9.7%) and Djibouti (12.4%), while the highest rates were reported in Afghanistan (57.5%), Sudan (55.6%), Iran (46%), Palestine (43.8%), Morocco (42.4%), and Libya (41.3%). While the regional average prevalence of never breastfeeding, mixed milk feeding and continued breastfeeding, was estimated at 15.7%, 42.9% and 41.5% respectively.18,19
All our estimated breastfeeding indicators falls below the recommendations and are far from the target rates set by the WHO which aims to at least 70% for initiation in the first hour, 70% for exclusive breastfeeding, and 60% at 2 years by the year of 2030. 20
The prevalence of breastfeeding practices can vary significantly across different regions and countries due to a multitude of socio-cultural, economic, and healthcare factors. Several factors contribute to these relatively lower prevalence observed in Tunisia compared to some neighboring countries4,21:
✓
✓
✓
✓
✓
The mother educational level was significantly associated with early breastfeeding initiation, exclusive and predominant breastfeeding with higher rates among mothers who are illiterate or having a primary educational level. This result was comparable to some other studies conducted in the MENA region like Saudi Arabia and United Arab Emirates.24-26 Our finding can be explained by several factors:
✓
✓
✓
✓
The environment of residence was significantly associated with exclusive breastfeeding, with a higher prevalence among mothers from rural areas. The economic well-being level was also significantly associated with exclusive and predominant breastfeeding with higher prevalence among mothers having the poorest economic level. Living in rural area is often associated with lower socioeconomic status, including higher levels of poverty. Rural communities often have strong cultural norms and traditional practices that prioritize breastfeeding as the primary mode of infant feeding. These cultural beliefs may emphasize the nutritional and immunological benefits of breast milk and discourage the use of formula milk or other substitutes. As a result, mothers living in rural areas may be more likely to exclusively breastfeed their infants due to adherence to these cultural norms and traditions. Moreover, rural areas often have lower socioeconomic status compared to urban areas, with higher rates of poverty and unemployment. Mothers living in rural areas may face fewer barriers to exclusive breastfeeding due to the availability of social support networks, less pressure to return to work, and lower exposure to formula milk marketing compared to their urban counterparts.31,32
In the other hand, there were disparities in breastfeeding practice between regions of the country which can arise due to a variety of factors. Regions within a country may vary widely in terms of socioeconomic status, with some areas experiencing higher levels of poverty, unemployment, and income inequality than others. Socioeconomic disparities can influence breastfeeding practices through factors such as access to healthcare services, availability of breastfeeding support programs, and employment opportunities that may affect mothers’ ability to breastfeed. Moreover, different regions within a country may have distinct cultural norms, beliefs, and traditions regarding infant feeding practices. Cultural factors, including attitudes toward breastfeeding, family support for breastfeeding, and perceptions of formula feeding, can vary significantly between regions and influence breastfeeding behaviors among mothers. Also, geographic, and environmental characteristics, such as urbanization and rural isolation can affect breastfeeding practices. Urban areas may have higher rates of maternal employment and formula feeding due to factors such as workplace demands and access to formula milk marketing.33,34
Otherwise, we observed a general decline in the practice of breastfeeding between 2000 and 2018. Never breastfeeding prevalence significantly increased (P < 10−3) from 2000 (2.4%) to 2018 (7.8%). Early breastfeeding initiation significantly decreased (P < 10−3) from 2006 (87.4%) to 2018 (31.5%). Exclusive breastfeeding during the first 6 months significantly decreased (P < 10−3) from 2000 (46.4%) to 2018 (13.4%). And the predominant breastfeeding during the first 6 months significantly decreased (P < 10−3) from 2000 (50.5%) to 2018 (30.4%).
This decline indicates a concerning trend in breastfeeding practices over the years, highlighting potential challenges or shifts in societal norms and healthcare policies that may have impacted breastfeeding initiation and continuation rates in Tunisia.
The decrease in breastfeeding practice in Tunisia between 2000 and 2018 can be attributed to several factors:
✓
✓
✓
✓
Policies and Measures Adopted in Tunisia to Support and Promote Breastfeeding
Breastfeeding practices in Tunisia have faced some challenges in recent decades, but there have also been efforts to promote and improve breastfeeding rates. Tunisia has implemented the International Code of Marketing of Breast-milk Substitutes since 1983,38,39 which was established by the World Health Organization (WHO) to regulate the marketing of breast milk substitutes. The Code aims to protect and promote breastfeeding by ensuring that breast milk substitutes, such as infant formula, are not marketed in ways that undermine breastfeeding practices.
These regulations include restrictions on advertising, promotion, and sponsorship of breast milk substitutes, as well as measures to ensure that information provided to families about infant feeding is accurate and unbiased.
While Tunisia has taken steps to implement the Code, challenges such as monitoring and enforcement of regulations may still exist. Tunisia has legal measures that contain a few provisions with lower coverage of the Code articles in legislation. Only 3 articles of the code were respected. Continuous efforts are needed to ensure compliance with the Code and to address any gaps or issues that may arise in its implementation. Tunisia has also implemented the Baby-friendly Hospital Initiative (BFHI) in 93 hospitals, 40 which promotes best practices in maternity services to support breastfeeding initiation and duration.
Recommendations to Promote Breastfeeding Practice in Tunisia41,42
✓
✓
✓
✓
✓
Strengths and Limitations of the Study
MICS surveys typically involve large sample sizes, providing robust and representative data on breastfeeding practices at national level. The large sample size enhances the statistical power of analyses and increases the generalizability of findings to the broader population. These studies follow standardized methodologies endorsed by UNICEF, ensuring consistency in data collection methods across surveys. This consistency enhances the reliability and comparability of results over time, enabling meaningful comparisons between different survey periods. Combining results from multiple MICS studies conducted in Tunisia between 2000 and 2018 can offer a comprehensive understanding of breastfeeding practices across different regions and demographic groups. The aggregated findings serve as valuable research evidence for advocacy efforts aimed at promoting breastfeeding. It provides a benchmark for monitoring progress in breastfeeding indicators and valuable insights into trends and patterns regarding breastfeeding practices in the country over time. It enables the assessment of the effectiveness of past interventions and guides future strategies to achieve breastfeeding-related targets. In fact, the aggregated data can inform policymakers about the prevalence of breastfeeding and its determinants and guide policy formulation. It enables the development of targeted interventions to promote breastfeeding and improve maternal and child health outcomes.
However, there are some limitations of the study. The latest MICS study was conducted in 2018 and the data is somewhat outdated which may not capture recent developments or changes in breastfeeding practices. Moreover, in many large-scale surveys like MICS studies, there are commonly limitations in the scope of factors studied. In the case of breastfeeding practices in Tunisia, the omission of certain determinants, such as maternal employment, and the delivery mode could indeed limit the comprehensiveness of the analysis. In fact, maternal employment is known as a significant determinant of breastfeeding practices, as it can influence factors such as the duration of maternity leave, access to breastfeeding breaks at work, availability of breastfeeding support in the workplace. Likewise, the mode of delivery, whether vaginal or cesarean section, can influence breastfeeding initiation and duration. Research suggests that cesarean section births may be associated with delayed initiation of breastfeeding and reduced likelihood of exclusive breastfeeding in the early postpartum period. Understanding the impact of delivery mode on breastfeeding practices is essential for tailoring interventions and support strategies for mothers, particularly those who undergo cesarean sections. In addition to these unstudied factors, there may be other important determinants of breastfeeding practices that were not adequately captured in the MICS reports. These could include cultural norms and beliefs surrounding breastfeeding, access to healthcare services and lactation support and availability of formula milk marketing.
Without a comprehensive understanding of the factors influencing breastfeeding practices, the MICS studies may provide an incomplete picture of the challenges and barriers faced by mothers in maintaining breastfeeding. And efforts to promote and protect breastfeeding may not be effective.
Perspectives
Recognizing the importance of these determinants, future iterations of the MICS study in Tunisia could consider including questions related to maternal employment status and delivery mode in the survey questionnaire. By capturing these additional variables, more robust data could be generated to inform evidence-based interventions and policies aimed at promoting optimal breastfeeding practices.
Recognizing the limitations of the existing data, there is a clear need for further research to fill the gaps in knowledge regarding breastfeeding practices in Tunisia. Future studies could explore the association between maternal employment and breastfeeding outcomes in more detail, as well as investigate other relevant determinants identified in the literature. In addition to quantitative surveys like MICS, qualitative research methods can provide valuable insights into the socio-cultural context and individual experiences related to breastfeeding practices. Combining quantitative data with qualitative findings can offer a more comprehensive understanding of the complex factors influencing breastfeeding behavior.
Acknowledging these limitations and advocating for more comprehensive data collection methods, could lead to a better understanding of breastfeeding practices in Tunisia and to the development of effective strategies to support breastfeeding mothers.
Conclusions
In conclusion, Tunisia has been experiencing low rates of breastfeeding practice, with a concerning decline observed over the years. Addressing this issue effectively necessitates a comprehensive, multi-faceted approach that encompasses various aspects of policymaking, healthcare, and society.
There is a crucial need for policy changes accompanied by an increase in political commitment to promoting breastfeeding. This entails enacting and enforcing legislation that supports breastfeeding-friendly environments, such as laws regulating the marketing of breast milk substitutes and providing incentives for workplaces to support breastfeeding mothers. Also, the effective implementation of BFHI is essential in improving breastfeeding rates in Tunisia. Furthermore, comprehensive training for healthcare providers is essential to equip them with the knowledge and skills to support breastfeeding mothers effectively. Community-based interventions also play a pivotal role in fostering societal support for breastfeeding.
Footnotes
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.