
Abstract
Background:
Maternal concern over infant skin problems is common in the early postnatal period. Although essential newborn care practices have been studied, evidence on newborn skin care practices among postpartum women in Ethiopia remains limited. This study aimed to assess newborn skin care practices and associated factors among postpartum women in Debre Markos, Northwest Ethiopia, in 2025.
Methods:
A cross-sectional study was conducted at an institution from December 23, 2024, to June 30, 2025, among postpartum women attending newborn immunization services. Data were collected using a structured questionnaire, entered into EpiData 4.4.2.1, and analyzed using Stata 17. Logistic regression was employed, with statistical significance set at P < .05.
Results:
Approximately 44.88% (95% CI: 40.11-49.75) of postpartum women practiced inappropriate newborn skin care. Early newborn bathing (44.9%) and frequent bathing (34.6%) were the most common practices. Although maternal education, age, gravidity, and knowledge were associated in bi-variate analysis, none remained significant after adjustment.
Conclusions:
This study revealed that inappropriate newborn skin care practices were prevalent. Early and frequent newborn bathing was a common newborn skincare practice. Strengthened maternal education and further intervention studies are recommended.
Keywords
Introduction
The skin is a multifunctional organ of great importance that promotes mechanical protection, thermoregulation, and immune surveillance and prevents the loss of bodily fluids. Proper skin care practices play a crucial role in bonding, comfort, and overall well-being in the early days of life.1 -4 The delicate skin of neonates is sensitive, thin, and fragile, and it suffers a progressive adaptation to the extra-uterine environment, and special care/attention is needed during this period.2,4 -6 The delicate skin of neonates is sensitive, thin, and fragile, and it suffers a progressive adaptation to the extra-uterine environment, and special care/attention is needed during this period. 7
Due to the characteristics of the skin of newborn babies and children, cosmetic products intended for their care and protection require special attention in the formulation.2,4 Although washing and skin treatment of infants has a long tradition, Opinions vary widely on what appropriate cleansing agents are for newborns and infants, which leads to variations in skin care practice.1,7 Child skin care practice strategies for optimizing epidermal barrier integrity, including bathing and emollient practices, umbilical cord care, diaper area care, preventing and managing infections and skin injury, and minimizing heat or percutaneous absorption of toxins, are emphasized in previous studies conducted in different countries.1,2,7,8
Standard neonatal skincare practices are guided by international and national recommendations aimed at preserving skin integrity and preventing infections. The World Health Organization (WHO) recommends gentle skincare practices for newborns, including delayed bathing for at least 24 hours after birth, maintaining skin cleanliness and dryness, avoiding harsh soaps or antiseptics, and promoting thermal care through skin-to-skin contact.9 -11 For preterm and low-birth-weight infants, WHO also recognizes the potential role of topical emollients in improving skin barrier function and reducing the risk of infection when used appropriately.
Postpartum mothers have a vital role in the comprehensive care of their newborns, including appropriate skin care, and postnatal age is an important consideration in determining skin-care practices. Studies indicate that child skin care practices are guided by personal experience rather than evidence-based practice, and practices are different across different settings, households, and among postpartum mothers.1,7,12 Postpartum mothers have a deficiency in the implementation of proper and optimal newborn skin care practice.4,13
The mixed-method study conducted in welfare clinics in Onitsha, Nigeria, revealed that approximately 50.5% had poor practice of newborn skin hygiene care shortly after birth.3,13 Another systematic review result showed the existence of a wide range of newborn skin cleansing practices across the countries, and cultural influences appear to drive parental practice. 12
An Observational study conducted in Southwest Nigeria indicates that the neonatal skin care regimen at the rural licensed traditional birth attendant centers comprised herb-infused water, traditional black soap, and vegetable oil moisturizers, while the skin care regimen in urban centers included tap water, olive oil, baby soaps, and proprietary moisturizers. 14
According to a study conducted on current neonatal skin care practices in 4 African sites, including the Oromia region of Ethiopia, the results show that emollient application in the first months of life was a normative, long-standing tradition. In Ethiopia, neonatal skincare is incorporated within national newborn and child health guidelines and integrated into essential newborn care packages. These include clean delivery and postnatal hygiene, delayed bathing, umbilical cord care, avoidance of potentially harmful traditional substances applied to the skin, and early identification of skin infections. 15 Despite the availability of these recommendations, adherence to standard neonatal skincare practices may vary due to cultural beliefs, resource limitations, and gaps in caregiver knowledge, underscoring the need to assess current practices and associated factors in the local context. Although an agreement exists on the importance of proper newborn skin care practice, there is little evidence available on newborn skin care practice among postpartum women in Ethiopia. Therefore, this study aimed to determine the newborn skin care practice and its associated factors among postpartum women in Debre Markos, North-west Ethiopia.
Methods and Materials
Study Setting and Period
This cross-sectional study was conducted at the Debre Markos comprehensive referral hospital from December 23, 2024, to June 30, 2025. The hospital is in the West-Gojam zone, Debre Markos town in the north-west part of Ethiopia, and is approximately 298 km away from Addis Ababa, the capital city of Ethiopia.
Study design
An institution-based cross-sectional study was conducted among postpartum women
Population
Source population: The study included all postpartum women who had delivered healthy, full-term infants within the last 6 months and who attended Debre Markos Comprehensive and Referral Hospital for newborn immunization services.
Study population: All sampled and selected postpartum women who gave healthy full-term births in the last 6 months and came for immunization to Debre Markos comprehensive and referral hospital during the data collection period were considered as the study population.
Inclusion and Exclusion Criteria
Inclusion Criteria: Postnatal mothers with healthy newborns were included in the study to minimize variability related to neonatal illness or prematurity. Newborns with medical conditions and preterm infants often require specialized care and interventions that can influence routine skin care practices, which could confound the study findings.
Exclusion Criteria: Women who came for immunization and were present with a preterm infant to the hospital, and women who did not participate in childcare (bathing, newborn skin care) at home were excluded during the data collection period.
Sample Size Determination
The sample size was calculated using a single population proportion formula, based on the following assumptions: 95% confidence level, 5% margin of error

n (1.96)2×0.5× (1−0.5)/(0.05)2 =384, after adding a non-response rate of 10% (19.2 ≈ 20), the final sample size was 422.
Sampling Technique and Data Collection Procedure
Before data collection, the average number of clients visiting the child immunization at the hospital during the month preceding the data collection period was estimated from the registration logbook, which was approximately 620. A systematic sampling method was used to select participants and include postnatal mothers who were available and willing to participate during the study period. Newborn immunization card numbers were used to systematically select study participants(mothers) at every KTH interval, taking K = N/n = 620/422) = 1.469, which is approximately 2: N is the source population, and n is the total sample size calculated for this study. Data were collected using a structured, interviewer-administered, and pretested questionnaire through face-to-face interviews administered by trained data collectors. The questionnaire was developed based on a review of relevant literatures,1,2,4,7,12 initially prepared in English, translated into Amharic, and then back-translated into English to ensure clarity and consistency. The face-to-face interviews were conducted by 2 BSc midwives, who received a full day of training on the study objectives and interview procedures. Supervision was provided by an MSc clinical midwife at the hospital to ensure adherence to the study protocol and maintain data quality. go-to actual data collection. One MSc clinical midwife was assigned as a supervisor in the hospital.
Variables of Study
Dependent variable: Newborn skin care practice
The independent variables of the study included:
Maternal and Neonatal demographics variables: Sex of neonate, maternal age in years, Ethnicity, Religion, Marital status, educational status, maternal residency, Maternal Occupation
Obstetrics and healthcare service utilization related variables: Gravidity, place of delivery, Type of pregnancy, Mode of delivery, antenatal care follow-up, and postnatal follow-up
Knowledge and information related variables: Confidence in newborn skincare practice: maternal knowledge, maternal confidence to provide newborn skin care, and cultural influence
Operational Definitions
Knowledge on newborn bath: know the appropriate time for bathing the newborn after birth. Mothers were asked if they knew the appropriate time for first bathing newborn after birth, and they were considered to have good knowledge if they answered the appropriate time for first bathing newborn was 24 hours or more, while the women were considered to have poor knowledge if they answered the appropriate time for first bathing newborn was below 24 hours. 16
Newborn skin care practice: Newborn skin care practices were assessed using a structured questionnaire that included key components such as timing of the first bath, frequency of bathing after the first 24 hours, water temperature used for bathing, cord care practices, and the use of skin emollients. Each item was scored individually, with a score of 1 assigned to practices consistent with recommended standards and 0 assigned to practices that were not consistent with recommendations. Newborn skin care Practices were classified as appropriate if they aligned with the World Health Organization (WHO) recommendations on newborn health, and as inappropriate if they deviated from WHO recommendations.7,9
Early bathing practice: The immersion of all or part of the body of a newborn in water or some other liquids for cleansing or refreshment within 24 hours after birth. 17
Knowledge of newborn skincare practice: Post-partum women were asked to respond to the timing of the first bath, frequency of bathing, temperature of water used to bathe, the appropriate emollient used, and cord care recommendations. Finally, A score of <50% was considered as they have inadequate knowledge, and a score of ≥50% was considered as they have adequate knowledge. 13
Data Quality Control and Quality Assurance
To ensure the quality of data, different measures were undertaken. The questionnaire was initially prepared in English, then translated into the local language, Amharic, and then translated back to English to maintain consistency. Before actual data collection, a pretest was conducted on 5% of the total samples in another health center. Based on pretest results, editions and modifications were made on the actual data collection tool before using it for the final data collection. One day of training was given to the data collectors. During the data collection period, the data were checked for completeness and consistency of information by the supervisor.
Data Processing, Analysis, and Presentation
The collected data were coded, entered into EpiData version 4.4.2.2.1, and then exported to Stata version 17 for statistical analysis. Data cleaning was performed to check for completeness, consistency, and accuracy before analysis. Descriptive statistics were used to summarize the characteristics of the study participants. Bivariate logistic regression analysis was conducted to examine the association between each independent variable and the dependent variable. Variables with a P-value of less than .25 in the bivariate analysis were selected as candidates for the multivariable logistic regression model.
Multivariable logistic regression analysis was then performed to control for potential confounding variables and to identify factors independently associated with newborn skin care practices among postpartum women. Variables with a P-value of less than .05 in multivariable analysis were considered statistically significant. Model fitness was assessed using the Hosmer–Lemeshow goodness-of-fit test, which indicated that the model was adequately fitted. Unfortunately, after conducting a comprehensive analysis, variables were found to be statistically significant at the .05 level of significance in predicting newborn skin care practice of postpartum women in this study. Finally, the results were presented using tables, pie charts, and descriptive text in the results section
Patient and Public Involvement
Study participants were not involved in the development of research questions or design, or conduct, or reporting, or implementation or dissemination plans, or evaluation.
Ethics Approval and Informed Consent
Ethics approval for this study was obtained from the Institutional Review Board (IRB) of the Department of Midwifery, College of Medicine and Health Sciences, Debre Markos University, under reference number MW/IRB/011/2025 (please refer to Supplemental Material). Prior to participation, the purpose of the study was explained to all participants, and oral informed consent was obtained. The use of oral consent was specifically approved by the Institutional Review Board (IRB). In addition, written informed consent for the publication of the study was retrospectively obtained from the legally authorized representatives of all study participants. This ensures compliance with ethical standards for the dissemination of research involving human subjects. To protect participant confidentiality, names were not recorded on any part of the questionnaire. All study procedures were conducted in accordance with the ethical principles outlined in the Declaration of Helsinki for medical research involving human subjects.
Results
In this study, of the 422 sampled participants (post-partum women), only 410 participants with a 97.16% response rate participated and completed the data collection process and provided complete information.
Infant and Maternal Demographic Characteristics
In this study, most of the participants were found under the age category of 20 to 34 years, which is approximately 69.9% of whom only 46.83% had inappropriate newborn skincare practice. Approximately 28.5% of the participants were illiterate, and 43.59% of them had had inappropriate newborn skincare practice.
The majority (72.0%) of the participants (postpartum women) resided in urban residences, and approximately 46.10% of them had newborn skincare practice. Most of the participants were housewives (65.6%), and around 46.10% of them had practiced newborn skincare inappropriately (Table 1).
Newborn and Maternal Demographic Characteristics Among Postpartum Women at Debre Markos Comprehensive and Referral Hospital, Northwest Ethiopia, 2025 (N = 410).

Maternal Obstetrics and Healthcare Service Utilization Status
In this study, 88% of the postpartum women were multi-gravid, and approximately 43.77% of them had inappropriate newborn skin care practices. More than 95% of post-partum women had a pregnancy history of at least 1 antenatal care (ANC) follow-up during the recent pregnancy, and approximately 45.5% of them had practiced newborn kin care inappropriately (Table 2).
Maternal Obstetrics and Healthcare Service Utilization Among Postpartum Women, Debre Markos Comprehensive and Referral Hospital, Northwest Ethiopia, 2025(N = 410).

Maternal Knowledge and Other Characteristics
In this study, approximately 79.02% Postpartum women had family support to care for their newborn, of which more than fifty percent (56.48%) had appropriate newborn skin care practice. Most of the post-partum women (62.93%) declared the presence of cultural influence while caring for their newborn, but approximately 54.95% had practiced newborn skincare appropriately. The majority (60.73%) of postpartum women had inadequate knowledge of appropriate newborn skin care recommendations, and approximately 42.57% of them had inappropriate newborn skin care practices (Table 3).
Maternal Knowledge and Other Influencing Characteristics on Newborn Skin Care Postpartum Women, at Debre Markos Comprehensive and Referral Hospital, Northeast-west Ethiopia, 2025 (N = 410).

Newborn Skincare Practice Among Postpartum Women
The majority (65.4%) of the postpartum women have washed their newborn after 24 hours of birth, and most of them wash their newborn every other day (48.3%). Approximately 119 (29.02%) post-partum women use baby lotion, and only 65 (15.9%) use traditional substances such as cow-butter, herbs, etc. (Supplemental Table 1).
Overall Newborn Skincare Practice Among Postpartum Mothers
In this study, the overall skin care practice among postpartum women was 44.88% (95% CI: 40.11-49.75), and 55.12% (95% CI: 50.25-59.89), respectively, inappropriate and appropriate newborn skincare practice (Figure 1).

Overall newborn skin care practice among postpartum women, at Debre Markos Comprehensive and Referral Hospital, Northwest Ethiopia, 2025 (N = 410).
Common Skin Problems of Newborns Reported by Post-Partum Women
In this study, approximately 178(43.41%) post-partum women observed and reported the most common newborn skin problems, such as skin rash (24.88%), dry skin (13.90%), and skin irritation (4.63%; Figure 2).

Common skin problems of newborns reported by post-partum women at Debre Markos Comprehensive and Referral Hospital, Northwest Ethiopia, 2025 (N = 410).
Factors Associated With Maternal Newborn Skincare Practice
In binary logistic regression analysis, variables such as maternal age, maternal educational status, maternal knowledge of newborn skincare, and maternal gravidity level were associated with newborn skincare practice below the significance level of 0.25 at a 95% confidence level. Then these variables were transferred and considered for multivariate logistic regression analysis to determine the final predictors of newborn skincare practice among post-partum women. Unfortunately, in the final multiple logistic regression model, no single variable was found to be an independent predictor of newborn-skin care practice in post-partum mothers at a 95% confidence level with a 0.05 level of significance (Table 4).
Bivariate and Multivariate Analysis of Newborn Skincare Practice Among Postpartum Women, at Debre Markos Comprehensive and Referral Hospital, Northwest Ethiopia, 2025 (N = 410).
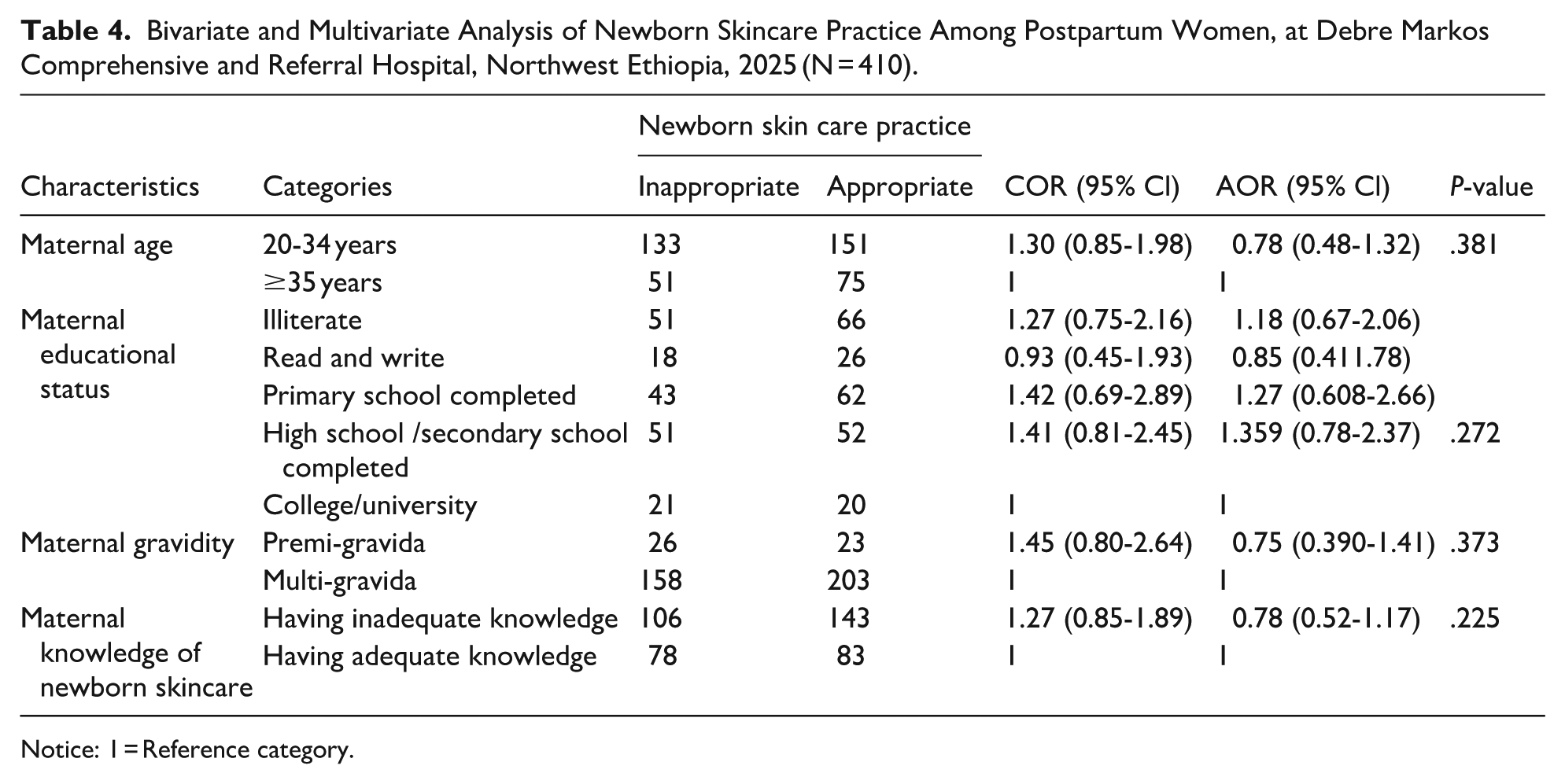
Notice: 1 = Reference category.
Discussion
This institution-based cross-sectional study was conducted to determine the newborn skin care practice among post-partum women giving birth to healthy full-term infants for the last 6 months in Debre Markos.
This study revealed that from the overall skin care practices, approximately 44.88% (95% 40.11-49.75) was inappropriate, which is lower than the study conducted in Onitsha, Nigeria, 13 where 50.5% of postpartum women had poor skin care practices. The possible reason for the difference might be due to the variations in the study area and sociodemographic variables among participants. This study was conducted at a single public hospital, but the study in Nigeria was multicentric.
In this study, early newborn bathing was 34.6% among postpartum women. This result is in line with the cross-sectional study conducted in Jimma town, 17 and Harar town, 18 Ethiopia, where the early newborn bath practice was, about early bathing practice among postpartum women was approximately 32.5% and 35.4% respectively. The result of this study is higher than the study conducted in India, where only 8% of the post-partum women bathe their newborn on day 1. 19 This shows that early newborn bath is still practiced against the recommended evidence-based practice of newborn skin care in Ethiopia.
This study revealed that the most common inappropriate skin care practice among postpartum women was bathing newborns daily, 44.9% which is lower than the study conducted in India, 19 where 78.6% of post-partum mothers bathed the baby daily. The variation might be due to the difference in demographics and cultural beliefs between study participants. In India, there is the belief that blood/vernix, which stays on newborn skin, is impure and must be removed thoroughly.
Approximately 119 (29.02%) post-partum women use baby lotion, and only 65 (15.85%) use traditional substances such as cow butter. This is in line with the scoping review result 20 and study conducted in 4 African countries, including Ethiopia, 21 where emollient application was usually done in all sites and butter application usually started in the second week of life in Ethiopia. However, this is open for further investigation, especially into the amount of product, the duration of intervention, and the application specification.
Inappropriate newborn skin care practices have various clinical implications, such as increased risk of skin infections, impaired skin barrier function, and potential systemic effects,4,22,23 In this study, skin rash (24.88%) was the most common newborn skin problem that was observed and reported by post-partum women, and this highlights the importance of educating parents and healthcare professionals about evidence-based newborn skin care practices.
In this study, no predictor variables were found to be associated with skin care practices among post-partum women despite conducting a comprehensive analysis and extensive data examination. Therefore, additional community-based studies using alternative analytical techniques or larger sample sizes might be required to identify significant predictors of newborn skin care practice among postpartum women. The role of unmeasured factors, such as environmental and cultural influences, maternal attitude, and behavioral patterns on newborn skincare practice should also be examined in the future.
Strengths and Limitations
Strengths: This is the first study in Ethiopia, and the study was conducted using primary data, which increased data accuracy and reliability; it will also be an input for future research, medical education, and clinical practice on newborn skincare until further research is available.
Limitations: This study has been conducted on a small sample size, which may result in less precise estimates and less representative of the large study population. In addition, the study was conducted only at a single public hospital, which might not be representative of private, public health institutions and the community in Debre Markos, Ethiopia. Therefore, community-based study is required. This study was limited to only postnatal mothers with healthy newborns; therefore, the findings may not be generalizable to mothers of newborns with health conditions, including premature infants. These groups often face different care practices and challenges, and future studies should consider including them to provide a more comprehensive understanding of newborn care practices and to better inform targeted interventions. Another limitation is that the age-specific type of vaccination was not recorded during data collection.
Conclusions and Recommendations
In this study, a substantial number of postpartum women were found to practice inappropriate newborn skin care practices and have limited knowledge regarding proper newborn skin care. Inappropriate newborn skin care practices, such as early bathing and frequent bathing of newborns, were common. These findings highlight an urgent need for maternal education to improve knowledge and promote evidence-based newborn skincare practices. To address this, routine postnatal visits and immunization appointments should include counseling on newborn skin care, accompanied by practical demonstrations for mothers and caregivers. The Ministry of Health and relevant stakeholders should also ensure that clear, culturally appropriate national guidelines for neonatal skincare are available to both healthcare providers and mothers. Health facilities and community health workers should provide structured education programs emphasizing delayed bathing, gentle cleansing, and appropriate use of oils or emollients. Furthermore, follow-up studies are needed to evaluate the effectiveness of educational interventions on maternal knowledge and practices, and to identify barriers to adherence to recommended skincare practices.
Supplemental Material
sj-docx-1-gph-10.1177_30502225261431442 – Supplemental material for Newborn Skin Care Practice and Its Associated Factors Among Postpartum Women in Debre Markos, Northwest Ethiopia, 2025
Supplemental material, sj-docx-1-gph-10.1177_30502225261431442 for Newborn Skin Care Practice and Its Associated Factors Among Postpartum Women in Debre Markos, Northwest Ethiopia, 2025 by Belete Fenta Kebede, Fekadu Baye Yitayew, Yalemtsehay Dagnaw Genie, Tsegaw Biyazin Tesfa, Aynalem Yetwale Hiwot, Esmelealem Mihretu Kassegn, Mihret Gulilat, Mekuanint Abebe, Burtukan Teshome, Tarikua Shiferaw and Mekides Yimer in Sage Open Pediatrics
Footnotes
Acknowledgements
It is our pleasure to thank the hospital administrative staff immunization unit pediatrics staff of the hospital for giving us the necessary information that we require. Our special appreciation extended to the study participants (post-partum mothers and care givers), data collectors, and supervisors.
Abbreviations
ANC: Antenatal Care, AOR: Adjusted odds ratio, CI: Confidence interval, COR: Crude odds ratio, MCH: Maternal and child health, OPD: Outpatient department, OR: Operating room
Ethical Considerations
Ethical approval for this study was obtained from the Institutional Review Board (IRB) of the Department of Midwifery, College of Medicine and Health Sciences, Debre Markos University (Reference No. MW/IRB/011/2025) (see Supplementary Material). All study procedures were conducted in accordance with the ethical principles of the Declaration of Helsinki for medical research involving human subjects. To ensure participant confidentiality, no personal identifiers, including names, were recorded on the questionnaires.
Informed Consent
Prior to participation, the purpose of the study was explained to all participants, and oral informed consent was obtained. The use of oral consent was specifically approved by the Institutional Review Board (IRB). In addition, written informed consent for publication was retrospectively obtained from the legally authorized representatives of all study participants.
Author Contributions
All authors made equal contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data file could be provided for research purposes only, upon request, using email address from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.