
Abstract
Objective:
To assess the preference of birth attendant gender and associated factors among antenatal care attendants in Debre Markos town public health facilities, northwest Ethiopia, 2021.
Method:
A facility-based cross-sectional study was conducted from 8 January 2021 to 28 February 2021 at Debre Markos town public health facilities. A total of 662 study participants were selected by systematic random sampling technique. Pretested interviewer-administered structured questionnaires were used for data collection. Data were entered using Epi Data version 3.1 and analyzed using SPSS version 25. Bivariable and multivariable logistic regression were applied to identify factors associated with birth attendant gender preference. Association was described by the “odd ratio” along with a 95% confidence interval. Finally, a P value < 0.05 in the adjusted analysis was used to declare a significant association.
Result:
In this study, 644 women participated making a response rate of 97.3%. Of the total study participants, 108 (16.8%; 95% confidence interval: 13.8–19.4) preferred male birth attendants, while 232 (36%; 95% confidence interval: 32.5–39.8) preferred female birth attendants. Age (15–24) (adjusted odds ratio = 4.81, 95% confidence interval: 1.79, 12.94), no formal education (adjusted odds ratio = 2.94, 95% confidence interval: 1.32, 6.52), and primary education (adjusted odds ratio = 2.42, 95% confidence interval: 1.07, 5.47) were significantly associated with female birth attendant preference. A lack of formal education (adjusted odds ratio = 0.08; 95% confidence interval: 0.01, 0.68), secondary education (adjusted odds ratio = 0.34; 95% confidence interval: 0.16, 0.71), and history of assisted vaginal delivery (adjusted odds ratio = 3.72; 95% confidence interval: 1.40, 9.87) were significantly associated with a male birth attendant preference.
Conclusion:
A female birth attendant is preferred by almost one-third of pregnant mothers, while one-sixth preferred a male. The clients who were younger in age and lower in educational status were more likely to prefer female birth attendants, whereas those who had a history of assisted vaginal delivery were more likely to prefer male birth attendants. To have a mother in the continuum of care, it is crucial to take her preferences into account when providing services.
Introduction
About 295,000 women died during and after pregnancy and childbirth in the entire world in 2017. The vast majority of these fatalities (94%) happened in areas with little resources, and the bulk of them could have been avoided. 1 Developing countries account for about 99% of global maternal mortality with sub-Saharan African alone accounts for 66%. 2
One of the keys to lowering maternal mortality rates is increasing institutional delivery rates. 3 Despite offering free maternity services, few skilled birth attendants are used.4,5 Low usage of maternal health care services was one of the reasons contributing to the delayed reduction in maternal mortality. 6
The preference of a birth attendant was one strong barrier to the utilization of maternity services. 7 The gender of health care providers influenced place of birth because most clients preferred female health care providers while some preferred male health care providers. 8 Some expectant mothers were not comfortable to be examined by the male health care provider. 9 Because of the gender of the healthcare provider, a patient may avoid seeking care or seek care at specific facilities. 10 Studies in Nigeria and Afghanistan showed that about 5% and 6% of women refused to deliver in a health facility due to the absence of female health care providers.11,12
Gender refers to characteristics of women, men, girls, and boys that are socially constructed. This includes norms, behaviors, and roles associated with being women, men, girls, and boys. 13 In obstetrics and gynecology, where intimate procedures are part of clinical management, the preference of patients for the same gender healthcare provider is very important. Most female clients prefer female obstetrician-gynecologist to male obstetrician-gynecologist.14,15 According to a different cross-sectional survey conducted in Asian countries, male healthcare providers are preferred by 1.6%–14.2%, whereas female healthcare providers are preferred by 32.3%–90.1%.16–18
Some women say they prefer male birth attendants because they feel they are treated more respectfully and are more willing to assist them when needed. 19
Women who mentioned they felt shy when the care providers were male were less likely to prefer institutional delivery in Bench Maji zone, Ethiopia. 20 A cross-sectional study conducted in Jigjiga, Somali region, indicated that 32.5% of women prefer to give birth at home, of which 30.7% was due to similarity in the gender of a birth attendant. 21
According to the researcher’s knowledge, there is not much data regarding pregnant mother preference of birth attendant gender in the study area and in Ethiopia at large.
In order to deliver services in accordance with mother preferences and increase service utilization, this study will give baseline data regarding maternal gender preference and identify characteristics related with it.
Materials and methods
Study setting
The study was conducted in Debre Markos town, located in East Gojjam zone, Amhara regional state, Northwest Ethiopia. It is 299 km from Addis Abeba, the capital city of Ethiopia, and 265 km from Bahardar, the capital city of Amhara regional state. According to the population projection of Ethiopia from 2014 to 2017, the total population of the town was estimated to be 92,470, of which about 46,738 were female.
In the town, there is one compressive specialized university hospital and three public health centers. All four public health facilities provide ANC, Labor and delivery, and postpartum care services.
Study design and period
An institution-based cross-sectional study was conducted from 08 January 2021 to 28 February 2021.
Source population
All pregnant women who received antenatal care at public health facilities in Debre Markos.
Study population
All pregnant mothers who received ANC service in Debre Markos town public health facilities during the study period were included.
Exclusion criteria
All pregnant mothers who were seriously ill were excluded from the study.
Sample size determination and sampling procedure
The required sample size for this study was calculated by using a power approach, considering factors associated with female gender preference in the previous study.
22
The Epi Info version 7 software stat calc was used with the following assumptions: 95% confidence level, Power 80%, and Ratio 1:1. Factors from previous studies, educational status was used, proportion of gender preference among primary education, diploma and above was used as proportion among exposed and unexposed, an adjusted odd ratio was considered, and the sample size became 630. After considering the possible non-response rate of 5%, a total of 662 participants were required to conduct this study. A systematic random sampling technique was used to select study participants visiting public health facilities in Debre Markos town for ANC service. Proportional allocation of study participants to each public health facility based on their previous 3-month client flow was done (Figure 1). Sampling interval was determined by dividing the total study population who to have ANC follow-up during the study period by total sample size, then sampling fraction or

Schematic presentation of the sampling procedure for assessment of preference of birth attendant gender and associated factor among ANC service attendants in Debre Markos public health facility, Northwest Ethiopia, 2021.
Operational definition
Skilled birth attendants
Skilled birth attendants refers exclusively to health professionals with midwifery skills such as a midwife, doctor, nurse, and others who have been educated and trained to proficiency in the skills needed to manage normal pregnancies, childbirth and the immediate postnatal period, and in the identification, management, and referral of complications in women and newborns. 23
Birth attendant gender preference
Birth attendant gender preference is a gender-based choice of a woman among health professions; either male, female, or no preference for birth attendance. Study participants were asked about which gender they prefer for birth attendance and female, male, and no gender preference options were provided. 21
Data collection tools and procedure
The questionnaire was developed by reviewing different literature related to the area of study,16,17,20,22–27 pretested and commented on by an expert. Structured interviewer-administered questionnaire were used for data collection. The dependent variable was preference of birth attendant gender, whereas independent variables like socio-demographic characteristics, obstetric characteristics, and preference-related characteristics were collected.
Data quality assurance
To ensure data quality, the tool was first prepared in English and translated to the local language (Amharic) and then translated back to English to check the consistency. Data were collected by four BSc Midwifery professionals. An MSc clinical midwifery professional supervised each data collection site. Two-day training was given for data collectors and supervisors about the objective of the study and the confidentiality of information. A pretest was conducted a week before data collection outside of the study area, at Guzamen health center, on 5% (33) of the total sample size, and necessary modification was made.
Statistical Analysis
The data were checked for completeness and consistency, before being coded, cleaned, and entered into Epi Data version 3.1 before being exported to SPSS version 25 for analysis. Tables, figures, and texts were used to summarize the descriptive statistics of the study. The median and interquartile range were used for numerical data. Bivariable and multivariable logistic regression were done to identify an association between a predictor variable and gender preference. All variables with a p value of less than 0.25 were included in the final model of multivariable logistic regression to control for confounding variables. The goodness of model fit was tested by Pearson’s and Deviance value.
Multinomial logistic regression was performed. Strength and direction of association were measured by the odd ratio. The adjusted odds ratio along with the 95% confidence interval (CI) was estimated by using multivariable analysis to identify factors associated with the outcome variable. A P value of <0.05 was considered to declare a statistically significant association.
Ethical consideration
Ethical approval was obtained from the Ethical Review Board of the University of Gondar college of medicine and health science school of midwifery research ethics committee on behalf Institutional Review board (IRB) of University of Gondar (Ref no: MIDW 18/2013 EC). Written and verbal informed consent was obtained from participants before the study. Written informed consent was obtained from legally authorized representative for minor and those with no formal education.
Results
Socio-demographic characteristics
Out of the 662 sample size, 644 participated in the study, making a response rate of 97.3%. The median age of study participants was 27, with an interquartile range of 24–30. Almost two-thirds (412, or 63.9%) of study participants were within the age group of 25–34. Most of the study participants (93.6%) were urban residents. The majority (613, or 95.2%) of study participants were Orthodox Christian religion followers, as shown in Table 1.
Socio-demographic characteristics of pregnant mothers attending an antenatal care unit in Debre Markos public health facilities, Ethiopia, 2021 (N = 644).

Obstetric history and service utilization of study participants
Of the total study participants, 586 (91%) pregnancies were planned. Of the total study participants, 373 (57.9%) study participants had given birth, whereas 247 (38.4%) study participants were primigravida. Of the total study participants, 27.6% had four and more ANC visits. Female birth attendants were present for 65 (22.8%) of the mothers who gave birth at a health facility by SVD or with assistance, as opposed to 216 (75.8%), who had male birth attendants. as shown in Table 2.
Obstetric history and service utilization of pregnant mothers attending the ANC unit in Debre Markos public health facilities, North West Ethiopia, 2021.

Preference of birth attendant gender among pregnant mothers attending ANC unit at Debre Markos public health facility
A total of 232 (36%; 95% CI: 32.5–39.8) of the study participants choose female birth attendants, while 108 (16.8%; 95% CI: 13.8–19.4) prefer male birth attendants (Figure 2).

Preference of birth attendant gender among pregnant mothers attending ANC unit at Debre Markos public health facilities, North West Ethiopia, 2021 (N = 644).
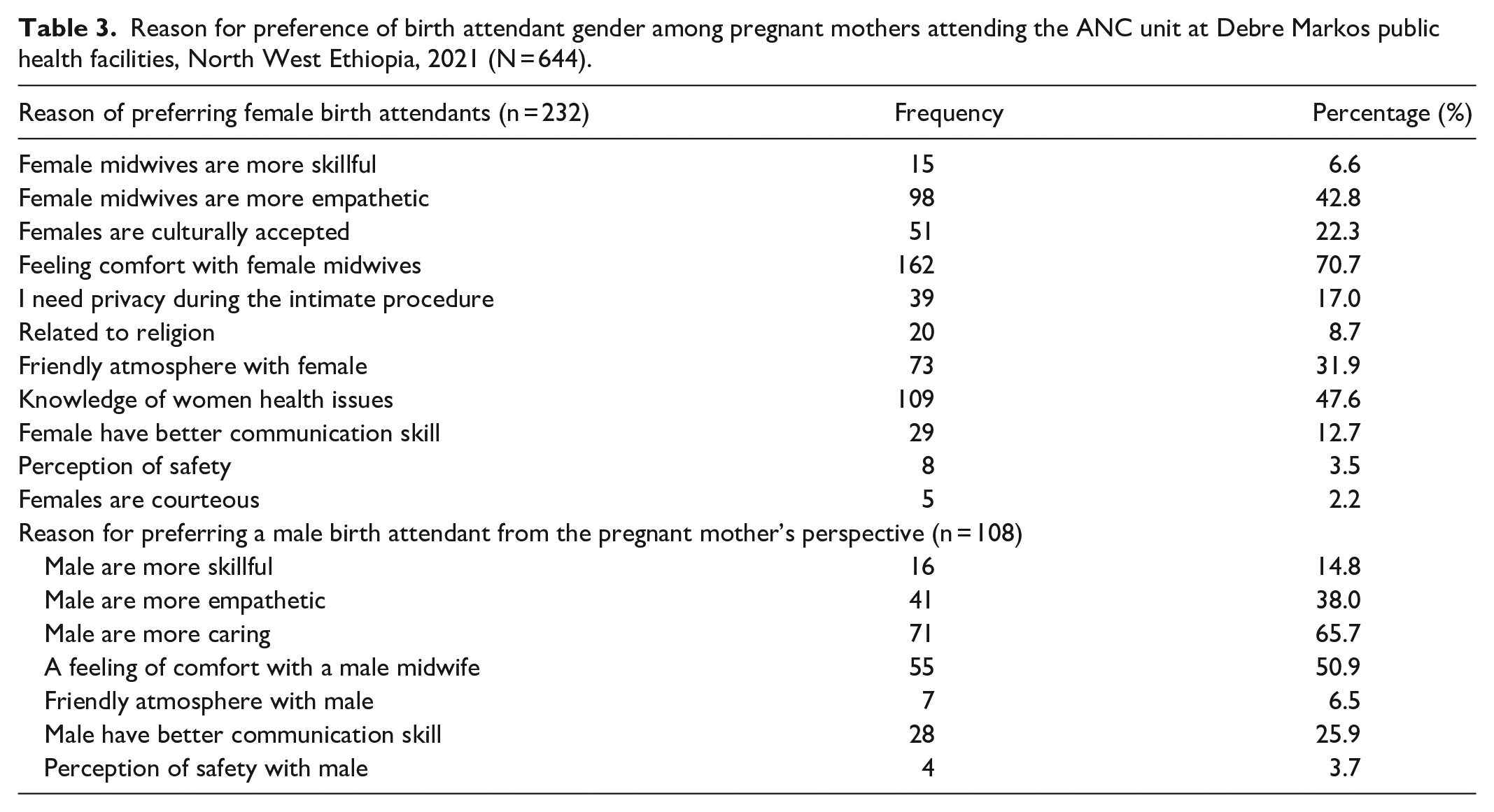
Women’s reasons for birth attendant gender preference
Among 232 respondents who indicated a preference for female health providers, their main preferential attributes were felt comfort with female health care providers (70.1%), perceived female health care providers to know more about women’s health issues (47.6%), and perceived female midwives were more empathetic (42.8%). On the contrary, those who preferred to be attended by a male midwife, their main preferential attributes were perception that male midwives are more caring (65.7%), feeling of comfort with the male midwife (50.9%), and perception that males are more empathetic (38%) as shown in (Table 3).
Reason for preference of birth attendant gender among pregnant mothers attending the ANC unit at Debre Markos public health facilities, North West Ethiopia, 2021 (N = 644).
A factor associated with gender preference
In binary logistic regression, age, residence, educational status of the study participant, and status of pregnancy were associated with female gender preference. However, in multivariable logistic regression, age category and educational status of study participants were associated with female gender preference (Table 4). The educational status of study participants and mode of delivery of the last child were associated with male gender preference (Table 5).
Bivariable and multivariate logistic regression models of factors predicting preference of female birth attendants among pregnant mothers attending the ANC unit at Debre Markos public health facilities, Northwest Ethiopia, 2021 (N = 644).
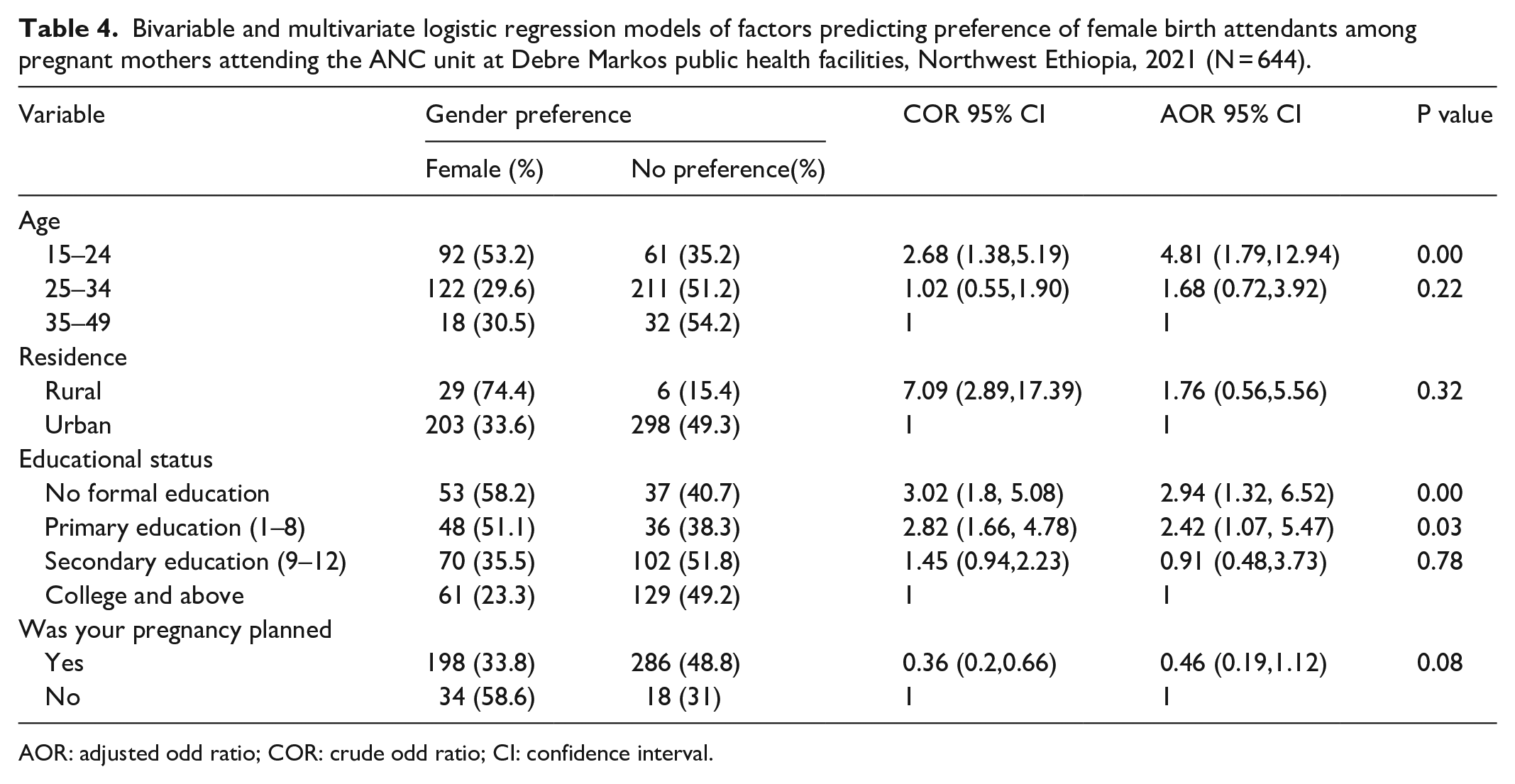
AOR: adjusted odd ratio; COR: crude odd ratio; CI: confidence interval.
Bivariable and multivariate logistic regression model of factors predicting preference of male birth attendants among pregnant mothers attending ANC unit at Debre Markos public health facilities, Northwest Ethiopia, 2021 (N = 644).

AOR: adjusted odd ratio; COR: crude odd ratio; CI: confidence interval.
The odds for female gender preference rather than no preference for a client who has no formal education was 2.94 times (adjusted odds ratio (AOR) = 2.94, 95% CI: 1.32–6.52) greater than those who have been educated to the level of a diploma and above. The odds of male gender preference rather than no preference was 3.72 times (AOR: 3.72, 95% CI: 1.40–9.87) more likely among mothers who gave birth by assisted vaginal delivery in the last delivery than those who gave birth by SVD.
Discussion
This study was conducted to identify preference of birth attendant gender among pregnant mother came for ANC service at Debre Markos public health facility. The findings of this study revealed that 16.8% (95% CI: 13.8–19.4) of study participants preferred male birth attendants and 36% (95% CI: 32.5–39.8) preferred female birth attendants, whereas 47.2% (95% CI: 43.2–51.1) had no gender preference.
The overall finding of our study indicated that 36% of respondents prefer female birth attendants. This finding was lower than the national study done in Ethiopia in 2015 (48%). 28 The reason for the difference may be the scope of the study, as the national study was wider in scope. This study was lower than the study done in Iraq, the United Arab Emirate, and a cross-sectional study done in Syria.17,24,29 This variation may be due to differences in the study population’s social and cultural background. Unlike those studies, about 95% of our study population were Orthodox Christians, whereas most of the study participants of those study were Muslim populations with very strong cultural and religious ties.16,30
Findings of our study revealed that the odds of a female birth attendant rather than no preference were nearly five times (4.81) more likely for those in the age category of 15–24 than those in the age category of 35–49. This finding was supported by a study done in Nigeria. 25 This may be explained as most of the study participants in this age group were primigravida; therefore, there is a shyness about being exposed to the opposite gender. There is a tendency toward decreased shame as age increase. Another possible explanation may be decreased shame as age increases and the life experience of older women enables them to consider other factors rather than gender.27,31
According to this study, those with no formal education or only primary education were 2.94 and 2.42 times more likely to choose female birth attendants. This could be explained by the fact that individuals with less education were more likely to adhere to traditional and cultural norms, and that education has resulted in a decline in religious and traditional observance. 27
According to our study, male gender preference for the birth attendant was 16.8%, this study was in line with a national study done in Ethiopia on male midwife acceptance (13%). 28 However, the finding of our study was greater than the study done in the United Arab Emirates 1.6%, 17 cross-sectional study done in Baghdad 8%. 29 This variation may be due to differences in socio-cultural factors as the more religious belief women prefer female birth attendants than males due to modesty. 32 The other thing is time variation, as acceptance of male birth attendant increase over time. However, this study was smaller than a study done in Nigeria 30.3%. 25 The reason may be the difference in socio-demographic status; as a proportion of those with primary and no formal education was 28.7% in our study, whereas 20.7% in study done in Nigeria.
This study indicated that male birth attendant preference rather than no preference was 99.2% decrease in those with no formal education when compared to those with diploma and above in level of education. Male birth attendant preference rather than no preference was 66% decrease in those with secondary education when compared to those with diploma and above in level of education. This may be explained as those with lower educational status were more prefer same gender birth attendant and feel shy to be examined by opposite gender.
Mode of delivery of previous birth was significantly associated with the preference of gender of birth attendant. Those who gave birth by assisted vaginal delivery were 3.71 times more likely to prefer male birth attendant rather than no preference when compared to those who gave birth by SVD. This can be explained as some females consider male birth attendants to be more competent and physically stronger than female birth attendants and can handle any complication that may occur during labor and delivery. 33
Limitation of the study
The cross-sectional nature of the study was one of limitation, as it cannot clarify the cause–effect relationship between outcome variables and predictive variables.
Conclusion
Nearly half of the pregnant mothers attending ANC at Debre Markos health facility have a preference toward the gender of birth attendant. Pregnant mothers who were young in age and lower in educational status were more likely to prefer female birth attendants. Those with lower educational status was less likely to prefer male birth attendants, whereas those who had history of assisted vaginal delivery were more likely to prefer male birth attendants. In addition to this more caring birth attendants, who have better communication skills, who have a friendly approach with the client, and empathetic were in demand. Considering maternal preference especially in the gender-sensitive area as in obstetrics is important to provide satisfactory health care service.
Footnotes
Acknowledgements
The authors acknowledge data collectors and also thank the study participant for their precious time.
Authors contributions
A.N. and B.A. are involved in the conception of the research idea, design, data obtaining, and interpretation of the finding. All authors drafted the manuscript, and all authors reviewed and contributed content. All authors have read and approved the final manuscript.
Availability of data
All supplemental materials for this article are available from the corresponding authors based on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.