
Abstract
Introduction:
Globally, it is estimated that 2.2 billion people have a visual impairment, of which around 65.2 million is due to cataract. Cataract is the leading cause of preventable blindness worldwide, with the greatest burden found in low-income countries. That is providing recent epidemiological data is very crucial to design intervention measures. The aim of this study was to assess the magnitude and associated factors of cataract among adults visiting ophthalmic clinic, Debre Markos comprehensive specialized hospital, Northwest Ethiopia, 2020.
Methods:
The sample size was calculated using single population formula and determined to be 174. All adult participants aged ⩾40 were the source population and those fulfilling the inclusion criteria were the study population. An institutional-based cross-sectional study design using a systematic random sampling technique was conducted from July to August, 2020. Semi-structured questionnaires and patients’ card were used to collect data. Data were entered into epi-data version 4.6 and the analysis was conducted using SPSS-25 software. Data were presented using graphs, tables and texts. Bivariable and multivariable binary logistic regression models were used to identify factors associated with cataract. Adjusted odds ratio with corresponding 95% confidence interval was computed to show the strength of association. A p-value < 0.05 was considered statistically significant.
Result:
From a total of 174 samples, 158 participated, giving a response rate of 90.8%. The prevalence of cataract was found to be 90 (57%). The variables—age 60–69 years (adjusted odds ratio = 6.667, 95% confidence interval: (1.662, 13.101)); age 70–79 years (adjusted odds ratio = 9.583, 95% confidence interval: (2.840, 32.342)), and single marital status (adjusted odds ratio = 2.945, 95% confidence interval: (1.241, 6.989))—had a significant association with cataract.
Conclusion:
The prevalence of cataract was found to be very high, which needs immediate intervention. Older age and single marital status were found to be significantly associated with cataract prevalence.
Introduction
Cataract is any opacity of the crystalline lens of the eye, 1 which causes progressive painless loss of vision that cannot be corrected with glasses, contact lenses or corneal refractive surgery. 2 The crystalline lens has three layers, namely nucleus, cortex and capsule. When the entire cortex from the nucleus to the capsule becomes white and opaque preventing the passage of light causing significant reduction of vision and absence of red reflex on ophthalmoscopic examination, the cataract is termed as matured cataract. 3 Cataract is an age-related condition in which the lens inside the eye becomes opaque, blurring vision. 4 In low-income countries, cataract accounts for about half of blindness and has a major impact on poverty. 5 It is estimated that in East Africa, between 3000 and 10,000 new cases per million population develop each year. 6 Cataract is the leading cause of preventable blindness and low vision in Ethiopia: >0.5 million people were blind and 1.2 million were severely visually impaired. 7
Globally, cataract is the leading cause of blindness3,8,9 and the second cause of low vision affecting all ages and ethnic groups which results in an increasing burden to the health care systems. 8 From the total of 2.2 billion with vision impairment globally, 1 billion people have a vision impairment that could have been prevented. Among 1 billion visual impairments that could have been prevented, 65.2 million are due to cataract. 10 Among 39 million (14%) blind and 246 million (86%) peoples with low vision estimated by World Health Organization (WHO) in 2010, cataract accounts for 50% causes of blindness and 33% low vision. 11 From the total of 285 million peoples with visual impairment in the world, 90% live in rural areas with few or underutilized eye-care facilities. 12 In the world, 82% of the blinds and 65% of people with low vision are aged ⩾52 years and 80% of the causes are either preventable or curable. 11
WHO proposed that between 2000 and 2020, the number of cataract surgeries performed worldwide need to triple in order to keep the needs of the population. 3 The Ethiopian national blindness and low vision survey 2005/2006 identified cataract as the leading cause of blindness (49.9%) and low vision (42.3%). 7 Matured cataract can have immediate and long-term consequences among adults aged ⩾40 years by causing secondary glaucoma and uveitis, increasing dependency on others and decreased mobility, 13 economic loss and mortality, 3 decreased quality of life, and increasing the risk of failure. 14
Even if cataract can be congenital, metabolic, secondary to ocular and systemic conditions, traumatic or secondary to ultraviolet radiation, about 85% of cataracts are classified as senile or age related which have greatest socioeconomic impact because of its high prevalence. 3 Age-related cataract remains the world’s leading cause of curable blindness 9 and is the main target of VISION 2020 “the Right to sight.” WHO and the International Agency for the prevention of blindness are directed at eliminating avoidable blindness by the year 2020 and its successful implementation requires accurate community-based data because studies done using a rapid assessment of cataract surgical service, which is a WHO validated research tool, tend to underestimate the true burden of cataract visual disability. 12
Different factors are associated with cataract development in different countries. One study concocted in Ghana showed that marital status was significantly associated with cataract development. 15 Another study in Nigeria showed that age was significantly associated with cataract as it is true in many countries including Ethiopia. 16 Other studies in different countries reported the risk factors associated with cataract, which includes educational status, 17 smoking, 18 diabetes, 19 sunlight exposure 20 and body mass index (BMI). 21
Although cataract is the leading cause of blindness and low vision in Ethiopia, 7 no recent study was reported about the magnitude and related factors at Debre Markos comprehensive specialized hospital, ophthalmic clinic. That is providing epidemiological data is much crucial to design public health intervention measures. Therefore, the main aim of this study was to assess the magnitude and associated factors of cataract among adults with age ⩾40 who visit ophthalmic clinic of Debre Markos comprehensive specialized hospital, Northwest Ethiopia, 2020.
Methods
This study was conducted in Debre Markos comprehensive specialized hospital, East Gojjam Zone, Amhara regional state, Northwest Ethiopia from March to August 2020. The hospital is found 299 km northwest of Addis Ababa, a capital city of Ethiopia and 268 km from Bahir Dar, a capital of Amhara regional state. Debre Markos comprehensive specialized hospital is the only hospital in East Gojjam Zone, which gives a routine health service for an estimated population of 5 million found in the zone and nearby border areas. Institutional-based cross-sectional study design using a simple random sampling technique was employed. All adults with age ⩾40 years of old were included in this study while those who were acutely/severely ill or with traumatic presentation were excluded.
All adults with age ⩾40 years visiting Debre Markos comprehensive specialized hospital, ophthalmic clinic were the source population and those who fulfilling the inclusion criteria were the study populations. The sample size was calculated using single population proportion formula by taking the prevalence of 19.8% from previous study, 16 5% margin of error with 95% confidence interval (CI):

where ni = the initial sample size, P = proportion from previous studies = 19.8%, Z = 1.96 at 95% CI, d = maximum error = 5% and ni = 242

where n = adjusted sample size, N = total population (cataract cases in Debre Markos comprehensive specialized hospital during the study period = 450)

By considering 10% non-response rate, the final sample size was found to be 174. The participants were selected using systematic random sampling technique. The first participant was selected with lottery methods using the patient’s order of arrival as a sampling frame. Before undergoing the study, ethical approval was obtained from Research and review committee of School of Medicine, Debre Markos University with the ethics approval number DMUSOMRCS/03/12/2019. Since there is no risk/no clinical trial, written consent was not applicable and this was waived by the research and review committee of School Medicine, Debre Markos University. Rather verbal informed consent was obtained. General instructions were given for the participants including the benefits of being interviewed. Before starting the actual data collection, the questionnaire was pretested by taking 5% of the sample size. The study was conducted by the principal investigator and three trained nurses at the hospital.
Semi-structured questionnaires having two parts were used to collect the data. The first part of the questionnaires were aimed to collect the sociodemographic information while the second part were used to collect general clinical outcomes/features of the study participants. The questionnaires were pilot-tested before undergoing the study.
Statistical analysis
After data collection, the data were entered into epi data version 4.6 and the analysis was conducted using Statistical Package for Social Sciences (SPSS) version 25 software. Frequency distribution, graphs and tables were used to describe the variables, and for numerical variables, mean value and standard deviation were used. Binary logistic regression was used to assess the association between independent and dependent variables by calculating the odds ratios (ORs) and their 95% CIs. All variables that showed statistical significance in the bivariate analysis were included in the multivariate logistic regression model to determine the independent factors associated with cataract. A p-value of
Operational definitions
Cataract: A clouding or loss of transparency of the lens in the eye as a result of tissue breakdown and protein clumping.
Visual acuity: ability to resolve detail at 6 m on a Snellen chart. 22
Blindness: a presenting visual acuity of <3/60 in the better eye. 11
Low vision: a presenting visual acuity of <6/18 but ⩾3/60 in the better eye. 11
BMI: measured by dividing the weight of the individual in kilogram (kg) to the square of his or her height in meters (m) and categorized as: Lean (<18.5), Normal (⩾18.5 but <25), Overweight (⩾25 but <30) and Obese (⩾30). 16
Positive ocular history: if the participant had diagnosed eye disease of glaucoma, myopia or had a previous history of ocular trauma. 3
Results
Out of a total of 174 samples, only 158 participants were involved in this study, giving a response rate of 90.8%. The mean age of the participants was 59.91 years with 11.803 standard deviation. The prevalence of cataract was found to be 90 (57.0%) as indicated in Figure 1. Of the participants, 91 (57.6%) were rural residence. The detailed sociodemographic characteristics of the participants are indicated in Table 1. The variables, in bivariate analysis including age, sex, residency, BMI, glaucoma, educational status, occupational and marital status, were significantly associated with cataract. From the variables found to be significant in the bivariate analysis, only age and marital status were found to be significantly associated with cataract in multivariable logistic regression analysis (Table 2). Participants in the age group of 60–69 years were 6.7 times (adjusted odds ratio (AOR) = 6.667, 95% CI: (1.662, 13.101)) more likely to have cataract than those patients in the age group of 40–49 years. The odds of respondents in the age group of 70–79 years were 9.6 times (AOR = 9.583, 95% CI: (2.840, 32.342)) more likely to develop cataract than in the age group of 40–49 years. Participants with single marital status (divorced, widowed, unmarried) are 2.9 times (AOR = 2.945, 95% CI: (1.241, 6.989)) more likely to develop cataract than married individuals (Table 2).
Participants’ presence and absence of cataract at Debre Markos comprehensive specialized hospital, Northwest Ethiopia, 2020.
Sociodemographic characteristics of the participants at Debre Markos comprehensive specialized hospital, ophthalmic clinic, Northwest Ethiopia, 2020.

Factors associated with cataract prevalence among adults visiting Debre Markos comprehensive specialized hospital, ophthalmic clinic, Northwest Ethiopia, 2020.
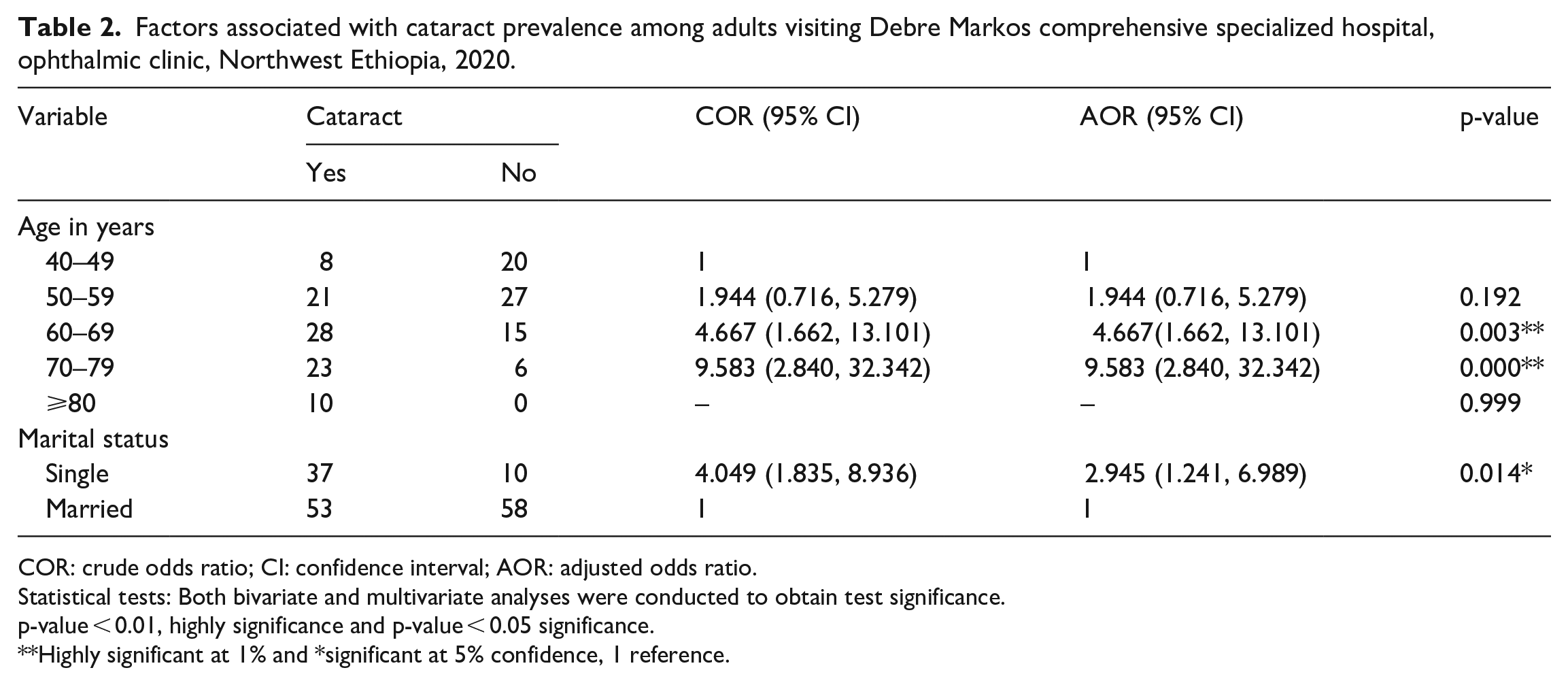
COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio.
Statistical tests: Both bivariate and multivariate analyses were conducted to obtain test significance.
p-value < 0.01, highly significance and p-value < 0.05 significance.
**Highly significant at 1% and *significant at 5% confidence, 1 reference.
Discussion
In our study, the prevalence of cataract was found to be 90 (57.0%). This was relatively higher than the study conducted in Gurage Zone, central Ethiopia among adults in which the leading cause of blindness was cataract (46.1%). 23 This may be due to geographical variations. The prevalence of cataract in our study was also higher than the studies conducted in Ethiopia: Abeshge and Kebena district, South of Addis Ababa, 2.4%; 24 Merhabete, 11.4%; 25 and Waghimra zone, 20.1%. 26 This might be due to the difference in the study populations and the outcome variables. Study conducted in Merhabete was concerned on people with blindness and in Abeshge it was limited to cataract that resulted in blindness. Whereas in our study we have considered all types of cataracts that cause visual impairment.
The prevalence of cataract in this study was higher than that in studies conducted in African settings: 19.8%, Nigeria; 16 2%, South Nigeria; 12 48.9%, Ghana; 15 2.1%, Tanzania; 8 and 46.2%, Malawi. 9 These differences may be due to the result of the differences in methodology, geographical variations and socioeconomic differences. The study design employed in Nigeria, Ghana and Tanzania was a community-based but in our study it was an institutional based.
In this study, the prevalence of cataract was also much higher than the study conducted in developed countries: 1.92% in Los Angeles, 27 9.7% in Singapore 28 and 24.86% in India. 29 This difference in prevalence might be due to the socioeconomic differences and variations in the methodological approaches adopted by authors from time to time and the racial and geographical differences in the populations studied as stated. 29 The other reason might be because study conducted in these developed countries did not include immature cataract, whereas in our study we included both mature and immature cataracts.
However, the prevalence of cataract in this study was relatively lower than that in the study conducted in India, which was 62.8%. 30 This difference might also be due to the geographical, socioeconomic and methodological variations.
This study revealed that marital status was significantly associated with cataract. Participants with single marital status were 2.9 times (AOR = 9.583, 95% CI: (2.840, 32.342)) more likely to develop cataract than married individuals. Similar study was reported in Ethiopia, 26 Ghana, 15 Kenya, the Philippines and Bangladesh, in which individuals with single marital status were more likely to develop cataract than married individuals. This is because being married is a protective mechanism from developing cataract. 31
In our study, the development of cataract was significantly associated with age distribution. Those participants in the age group of 60–69 years were 6.7 times (AOR = 6.667, 95% CI: (1.662, 13.101)) more likely to have cataract than those in the age group of 40–49 years. Participants in the age group of 70–79 years were 9.6 times more likely to develop cataract than those in the age group of 40–49 years (AOR = 9.583, 95% CI: (2.840, 32.342)). This was supported by studies conducted in Ethiopia, Waghimra Zone, 26 Nigeria 16 and India, 29 in which the probability of developing cataract for older individuals is more likely than younger individuals. All these studies taken individually and as a group demonstrate that cataract increases with age. This may lead us to conclude that in most countries, the burden of cataract is the same despite the difference in proportion.
As a limitation, our study was conducted at one specific hospital so that it may not be representative of the whole population of Amhara region, as well as across the country. Due to resource and time limitations, we could not incorporate all age groups admitted in the hospital. Despite the fact that there was no any respondent who denied his or her age, there could be recall bias of it because most of them are illiterates. Our finding fails to report the association between all independent variables with our outcome variable (cataract) like other chronic diseases complications with the development of cataract. In addition, we could not identify all the possible causes for the development of cataract. In addition, the finding fails to discuss the distribution of cataract between the rural and the urban population so that possible interventions might be conducted. The socioeconomic consequences of cataract were not investigated in the study, which needs to be studied in the future.
Conclusion
The prevalence of cataract among adults aged ⩾40 years of old visiting Debre Markos comprehensive specialized hospital, ophthalmic clinic was found to be very high, which needs immediate intervention by the responsible stakeholders.The most likely reason for this high prevalence of cataract could be due to the low socioeconomic status of the participants and the study includes any lens opacity regardless of maturity and cause. The variables increasing age and single marital status were significantly associated with the development of cataract. By considering this article as a baseline information in the study area, conducting a community-based research across the country, Ethiopia and in Amhara region is highly recommended.
Supplemental Material
sj-pdf-1-smo-10.1177_2050312121989636 – Supplemental material for Cataract and associated factors among adults visiting ophthalmic clinic at Debre Markos comprehensive specialized hospital, northwest Ethiopia, 2020
Supplemental material, sj-pdf-1-smo-10.1177_2050312121989636 for Cataract and associated factors among adults visiting ophthalmic clinic at Debre Markos comprehensive specialized hospital, northwest Ethiopia, 2020 by Mengistu Zelalem Wale, Mengist Derbew, Melkamu Tilahun and Mesenbet Terefe in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank all the study participants and Debre Markos University, School of Medicine for providing ethical approval and permission to do our research.
Author contributions
M.Z.W. wrote the manuscript, participated in data collection with M.D. and M.Ti. M.Te. and M.D. analyzed the data and drafted the paper with M.Z.W. and M.Ti. All the authors revised the draft, and read and approved the final manuscript for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
Ethical approval was obtained from Research Review Committee of Debre Markos University, School of Medicine (with the ethical approval number DMUSOMRCS/03/12/2019 on 14 July 2020). After information was provided about the objectives and importance of the study, verbal informed consent was obtained from the participants. Since no risk/no clinical trial were involved, written consent was not applicable and this was waived by the research and review committee of School Medicine, Debre Markos University. There were no potential risks that may cause any harm in any form on the study subjects. The data will not be transferred to the third body and were used only for the research purpose to ensure confidentiality.
Data Availability
We have sent all the available data and we do not want to share the raw data since we are doing related study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.