
Abstract
Background:
Access to timely and appropriate care for children with congenital heart disease (CHD) remains highly inequitable in low- and middle-income countries (LMICs).
Objectives:
This systematic review synthesizes recent evidence on barriers to healthcare access for pediatric CHD and applies the SHEL human factors framework to analyze system-level determinants.
Design:
This updated systematic review extends a prior analysis, applying PRISMA guidelines. Search was conducted in PubMed/MEDLINE, Scopus, and Web of Science. Regional trends were mapped via WHO classifications.
Results:
Most studies reported barriers related to environmental factors, followed by workforce limitations, infrastructure constraints, and policy or organizational deficiencies. Many obstacles originated at the primary care level, contributing to delayed diagnosis and referral. Although all regions exhibited barriers across SHEL domains, their relative distribution varied by region.
Conclusion:
These findings highlight that improving CHD outcomes in LMICs requires integrated health system strengthening across levels of care.
Keywords
Introduction
Access to healthcare is a central component of any health system. It extends beyond the mere presence of facilities and personnel 1 ; it involves the complex interaction between healthcare infrastructure, policies, and the users who depend on them, including the provision of adequate information, financial coverage, and effective referral mechanisms. 1
Congenital heart disease (CHD) encompasses a broad spectrum of structural cardiac anomalies present at birth. 2 Most affected children require either corrective or palliative surgical interventions within their first few years of life. When treatment is provided promptly, survival outcomes are favorable, and most patients can reach adulthood. 3 Nevertheless, in many parts of the world, particularly in low- and middle-income countries (LMICs), access to timely and appropriate healthcare remains a major challenge for this group of patients. 2
Children with CHD in resource-limited settings encounter multiple barriers to care, contributing to an estimated 260 000 global deaths each year, most of which occur in LMICs. 4 The treatment of CHD shares features with other complex pediatric conditions—such as cancer—that require intensive use of specialized facilities and costly technologies. 5 In many contexts, these services are concentrated in a few hospitals, making them geographically inaccessible and financially prohibitive for families without adequate insurance coverage. 6 Furthermore, early detection is often hampered by limited diagnostic capacity, poor referral systems, and insufficiently trained healthcare providers. 7
To better understand and address these inequities, it is necessary to systematically synthesize the existing evidence on healthcare access for children with CHD in LMICs. Identifying the principal barriers can guide the design of context-specific interventions and evidence-based policies aimed at improving service delivery and reducing preventable mortality. A growing body of research highlights the value of applying human factors analysis to healthcare delivery. In this study, the SHEL model—originally developed in aviation safety and later adapted for medical error analysis—was used to examine systemic and behavioral interfaces affecting access to care. By conceptualizing healthcare delivery as the interaction of Software (protocols and procedures), Hardware (infrastructure and equipment), Environment (organizational and sociocultural context), and Liveware (health professionals and patients), 8 this approach provides a complementary perspective for identifying mismatches that hinder access and quality of care for children with CHD in LMICs. Expanding research in this area is crucial, as CHD remains a significant and largely preventable cause of disability and death among children in resource-constrained settings, where stronger health systems and targeted policies could substantially improve outcomes. This systematic review aims to synthesize evidence on barriers and facilitators to healthcare access for children with congenital heart disease (CHD) in low- and middle-income countries (LMICs), using the SHEL model to categorize systemic mismatches across software, hardware, environment, and liveware components.
Methods
Search Strategy and Study Selection
This systematic review builds upon a previously published review on access to healthcare for children with congenital heart disease (CHD) in low- and middle-income countries (LMICs). 9 These reviews use the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA; see checklist in Supplemental Annex 1). A protocol was developed and registered in PROSPERO for the previous systematic review and was followed in this opportunity (ID number 470589). The same search strategy and inclusion criteria used in the original review were applied to identify additional studies published since the previous search period. Searches were conducted across major biomedical and multidisciplinary databases, including PubMed/MEDLINE, Scopus, and Web of Science, using combinations of keywords and controlled vocabulary related to “congenital heart disease,” “access to care,” and “low- and middle-income countries.” Search strings are available in Supplemental Annex 2.
Inclusion and exclusion criteria were established using the PICOTS framework, encompassing: (1) studies targeting children with CHD; (2) those detailing healthcare access processes or specific obstacles; (3) publications from 2000 onward; (4) research conducted in LMICs; (5) qualitative, quantitative, or mixed-methods designs; (6) reports in English, French, Spanish, or Portuguese. Studies failing to satisfy these standards were removed from consideration. Further details on the criteria are provided in Supplemental Annex 3.
Article selection proceeded in 3 phases. Initially, titles and abstracts underwent screening to pinpoint studies aligning with the inclusion criteria. Next, full-text reviews confirmed articles examining healthcare access for this group. Lastly, reference lists from chosen publications were checked against the same standards. All sources’ suitability was evaluated based on the outlined inclusion and exclusion criteria.
Data Extraction and Analysis
Data from all included studies were extracted using a structured template in Microsoft Excel (v. 16.78.3). Information on study design, country, population, healthcare level, and key findings was summarized. For the analytical phase, a thematic analysis was conducted following the principles of the SHEL model (Software, Hardware, Environment, Liveware).8,10 One author (RL) extracted the data into the chart, which another author (SA) then reviewed, resolving any discrepancies through discussion. Data was analyzed globally and by region.
Regional Classification
To facilitate geographic comparison, the countries represented in the included studies were grouped according to the World Health Organization (WHO) regional classification (Africa, Americas, South-East Asia, Europe, Eastern Mediterranean, and Western Pacific). 11 This classification enabled the identification of regional trends and disparities in access to CHD care across LMICs.
Results
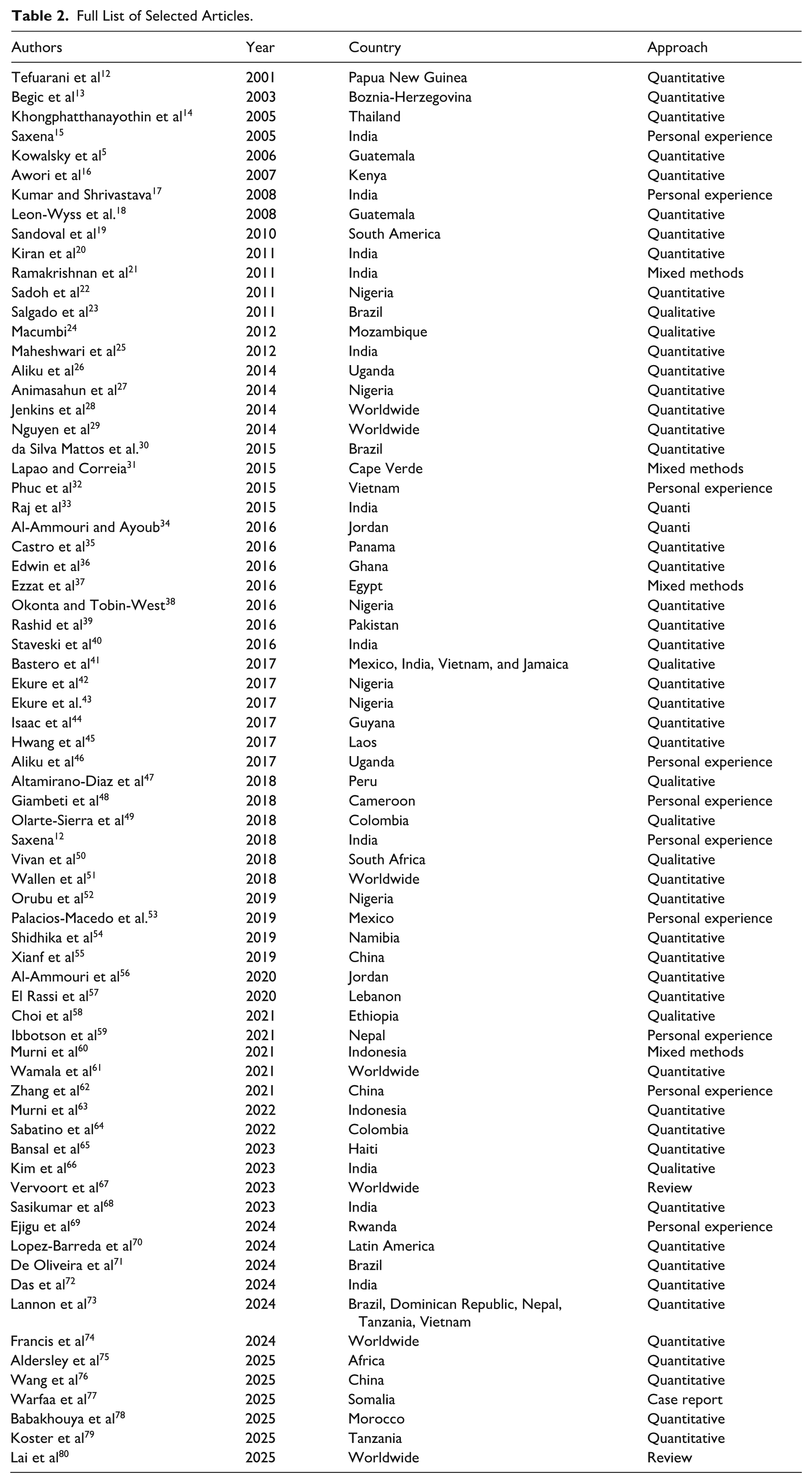
After removing duplicates, studies were screened by title and abstract, and full-text articles were reviewed for relevance. Only studies addressing barriers, facilitators, or determinants of access to healthcare for children with CHD in LMICs were included. 14 new articles meeting the eligibility criteria were identified and added to the 57 reports identified in our previous systematic review, reaching a total of 71 articles. Figure 1 shows the selection process, Table 1 provides information regarding the included articles, and Table 2 shows all selected articles.

New article selection process.
Description of Articles Included in the Systematic Review.

Full List of Selected Articles.
Most articles (64; 90.14%) reported issues regarding environment, followed by liveware (60; 84.51%), hardware (59; 83.1%), and finally software (47; 66.2%). Among the most reported problems regarding software, the most important issue was the lack of policies and guidelines, such as “There is no national policy for pediatric heart care.” 15 These policies may be related to general aspects of the care provision or, in some cases, refer to more specific features, such as diagnostics, registries, or the way that family members are involved in the treatment. Other important factor was difficulties in collaboration, as depicted by “There is limited coordination between tertiary hospitals and primary care facilities for follow-up of children with congenital heart disease.” 17 Some articles show cases of miscommunication between national actors, whereas other studies show the problems in international cooperation initiatives. Finally, the lack of appropriate health insurances schemes was another relevant problem “Only 3.9% of families had some form of health insurance to support the costs.” 33
Regarding hardware, the problems ranged from some pieces of equipment, as reflected by “Only one hospital had consistent access to echocardiography equipment,” 47 the lack of specialized centers in the region: “Ten countries had no pediatric and congenital heart disease service” 75 or the uneven distribution of them, to financial issues such as “High cost of surgery above INR 50,000 associated with reduced access to treatment.” 21
Undoubtedly, the environment is another potential source of barriers. Most of them related to geographical issues, for example, Kiran et al 20 reports “Patients from rural regions face long travel distances and multiple referrals before definitive diagnosis.” Other studies show how poverty is an impeding factor: “Families in low-income regions struggled with travel costs and lack of nearby facilities.” 49 Finally, politics also plays a role in this regard “Political instability and import restrictions delayed mission deployment,” 51 including the situation suffered by people in refugee camps.
The role of liveware is concentrated on the lack of trained workforce and training programs, as described by Ezzat et al 37 “Shortage of trained pediatric cardiologists and surgeons affected timely management.” A few articles describe how stress and cultural factors may be another aspect to be tacked if we want to improve patient’s access to specialized care, as depicted by this sentence: “Parents frequently develop depression, distress, anxiety, and hopelessness when navigating care.” 70
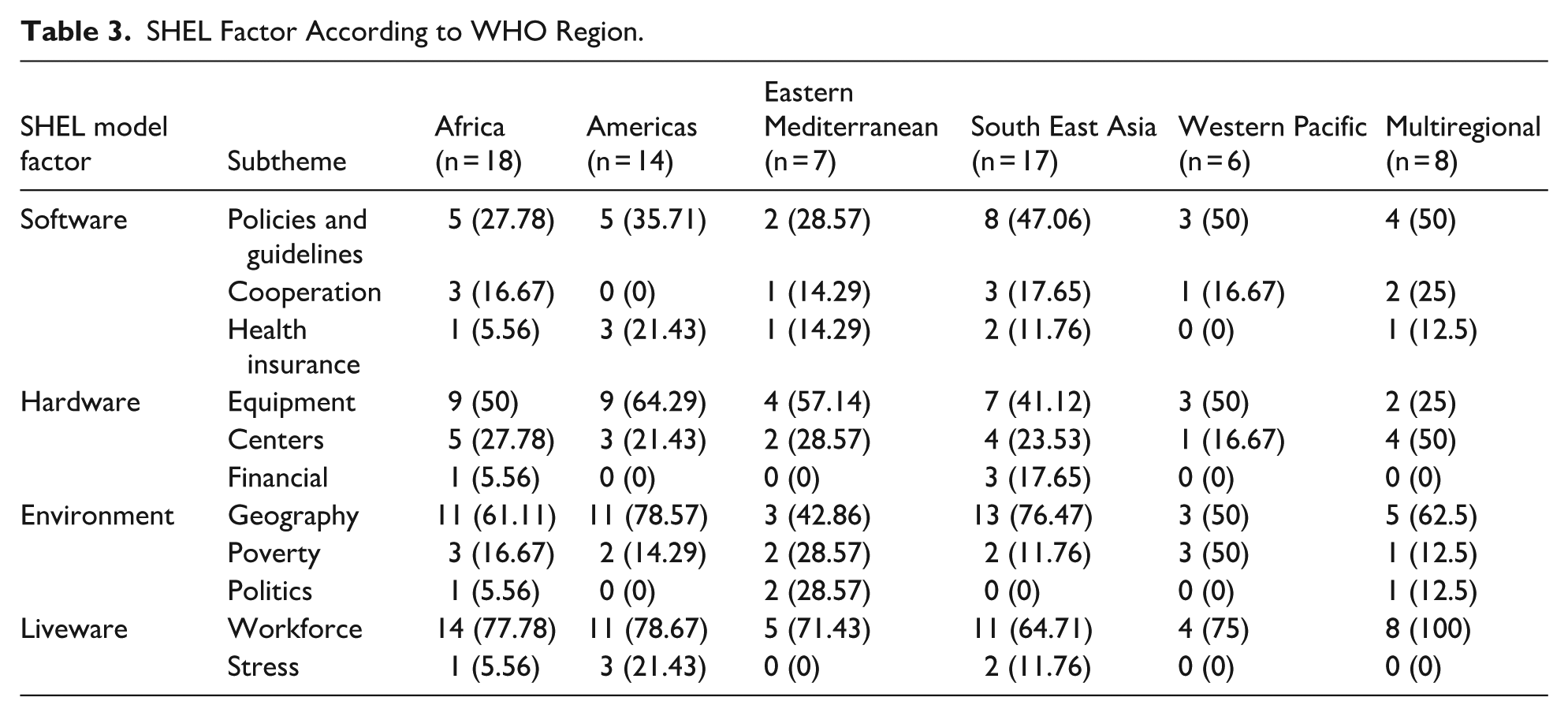
While all WHO regions represented in the review experienced barriers across the SHEL categories, the relative distribution varied. For example, geographical barriers were particularly prominent in Africa, the Americas, and South-East Asia, whereas deficiencies in workforce capacity were nearly universal. Hardware limitations were especially common in African and American regions, while policy gaps were more frequently cited in South-East Asia and multiregional studies. Table 3 shows these findings by region.
SHEL Factor According to WHO Region.
Discussion
This updated systematic review highlights the persistent and multifaceted barriers that limit access to timely and appropriate healthcare for children with congenital heart disease (CHD) in low- and middle-income countries (LMICs). By applying the SHEL framework, this analysis demonstrates that obstacles to care arise from interacting structural, organizational, sociocultural, and human-resource factors. Although the relative contribution of each component varies by setting, the overall pattern confirms that improving CHD outcomes in LMICs requires comprehensive and systems-level reform rather than isolated clinical interventions.4,81 -83
The applicability of the SHEL framework extends beyond specialized pediatric cardiac services and is highly relevant to primary care delivery in LMICs, where many of the same systemic mismatches are observed.10,84 In primary care settings, software deficiencies—such as absent clinical guidelines, weak referral protocols, and limited insurance coverage—often result in delayed recognition and referral of complex conditions, including congenital heart disease.85,86 Hardware constraints, including shortages of basic diagnostic tools and essential medications, further limit the capacity of frontline providers to deliver timely and effective care.84,86 Environmental factors, such as geographic isolation, transportation barriers, and socioeconomic hardship, disproportionately affect primary care access and continuity,87,88 while liveware challenges—including workforce shortages, inadequate training, and high provider turnover—undermine care quality and patient trust.89,90 Together, these interacting failures mirror those identified in specialized CHD care and highlight that weaknesses at the primary care level frequently initiate the cascade of failures leading to poor CHD outcomes. 91 In LMICs, late diagnosis of congenital heart disease is frequently rooted in system failures at the primary care level, which represent the first point of contact for most children and families.15,83 Collectively, these interacting failures shift CHD detection downstream to emergency or tertiary care settings, often after irreversible complications have developed. 91
The expansion of the SHEL framework to primary care highlights the critical role of frontline health systems in shaping pediatric CHD outcomes.8,10 Strengthening primary care capacity through SHEL-informed interventions—such as integrating newborn and infant screening, enhancing provider training in early CHD recognition, improving referral coordination, and reducing environmental barriers to follow-up—has the potential to shift diagnosis earlier in the disease course and improve access to definitive treatment.86,91 Ultimately, addressing pediatric CHD in LMICs requires health-system strengthening strategies that bridge primary and specialized care, prioritize equity, and recognize early diagnosis as a system-dependent outcome rather than an isolated clinical event.84,91 Leveraging the SHEL framework across levels of care provides a structured and actionable approach to reducing preventable morbidity and mortality among children with CHD in resource-constrained settings.10,91
This study has some limitations, including the fact that it is based on studies post-2000 in 4 languages which may exclude relevant gray literature or non-covered publications, potentially introducing bias toward reported barriers. Moreover, there are a significant number of articles that come from a few countries, while other territories are not represented, so the information is not necessarily representative of the whole world. On the other hand, the thematic SHEL analysis, while structured, depends on author interpretations and could overlook nuanced quantitative trends.
In conclusion, access to care for children with congenital heart disease in low- and middle-income countries remains constrained by a complex and interdependent set of policy, infrastructure, environmental, and workforce barriers.83,91 This review demonstrates that these challenges are not confined to specialized pediatric cardiac services but originate earlier within primary care systems, where initial opportunities for detection, referral, and prevention are frequently missed.85,86 Applying the SHEL framework across the continuum of care reveals how software deficiencies (including absent screening protocols and referral guidelines), hardware limitations (such as lack of basic diagnostic tools), environmental constraints (notably geographic and socioeconomic barriers), and liveware challenges (workforce shortages and limited training) collectively contribute to delayed CHD diagnosis and presentation at advanced stages of disease.84,87,89 Future research should prioritize interventional studies testing SHEL-informed strategies, like enhanced primary care screening protocols and referral networks. Longitudinal evaluations in underrepresented LMICs, incorporating patient outcomes and cost-effectiveness, would clarify policy impacts. In this endeavor, collaborative efforts with WHO regions could standardize data collection on workforce training and insurance schemes to guide scalable reforms.
Supplemental Material
sj-docx-1-gph-10.1177_30502225261430472 – Supplemental material for Barriers to Healthcare Access for Children With Congenital Heart Disease in Low- and Middle-Income Countries: A Systematic Review Using the SHEL Framework
Supplemental material, sj-docx-1-gph-10.1177_30502225261430472 for Barriers to Healthcare Access for Children With Congenital Heart Disease in Low- and Middle-Income Countries: A Systematic Review Using the SHEL Framework by Rodrigo Lopez-Barreda, Silvia Amesty, Milena Pavlova and Wim Groot in Sage Open Pediatrics
Footnotes
Acknowledgements
None.
Ethical Considerations
This study does not involve the participation of research subjects, therefore approval from a research ethics committee and a consent form were not required.
Author Contributions
- Rodrigo Lopez-Barreda: Conceptualization, methodology, investigation, analysis, visualization, writing.
- Silvia Amesty: Analysis, validation, writing.
- Milena Pavlova: Conceptualization, methodology, supervision, reviewing.
- Wim Groot: Conceptualization, methodology, supervision, reviewing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this manuscript are published in scientific journal articles, properly identified, and are public.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.