
Abstract
Background. Maternal education may influence child supervision practices in low-and middle-income countries (LMIC). However, little is known about the maternal factors that can improve child supervision in LMIC with scarce childcare facilities. Objective. To investigate the prevalence of children under 5 years home alone and examine the association between mother’s formal education and children home alone across 63 LMIC. Methods. The study used data from 50 Multiple Indicator Cluster Surveys and 13 Demographic and Health Surveys with a sample of 501 769 children. We estimated Prevalence Ratios (PRs) for the association between maternal education and children home alone using multivariable Poisson regression, adjusting for covariates such as child’s age and sex, mother’s age and marital status, number of adults inhabiting the households, and urbanicity. Results. Prevalence of children home alone across 63 LMIC ranged from 1.1% to 50.1%. A significant negative association between mothers with more years of formal education and children home alone was found across 16 LMIC. However, the opposite trend was observed in Nigeria, Senegal, and Côte d’Ivoire. Null association was found across 44 LMIC. Conclusions. The varied pattern of the associations observed across LMIC underscores the importance of regional and local factors when developing policies and interventions to ensure safety and adequate care for children aged under 5 years in LMIC.
Introduction
Leaving young children home alone is often considered inadequate supervision linked with multiple negative health outcomes.1-3 With nearly 559 million children under 5 years in low-and middle-income countries (LMIC), ensuring they receive adequate supervision is crucial to prevent developmental risks, injuries, and promoting healthy growth. 4 For instance, inadequate supervision has been associated with unintentional injuries such as poisoning, drowning, burns, and even deaths.5-8 In addition, children under 5 years are particularly vulnerable to drowning in LMIC, and inadequate supervision can be considered as a contributing factor to the increased risks.9-11 Similarly, children under 5 years in LMIC are 8 times more likely than their peers in high-income countries to face unintentional injuries, which may be prevented through adequate child supervision.7,12
Child supervision practices are associated with structural and socio-cultural factors, including parental beliefs and perceptions. 13 One of the structural predictors of child supervision is maternal education. 14 Evidence suggests that formal education shapes a mother’s ability to process health information and make related decisions, such as supervising children’s eating. 15 Besides providing greater receptivity to health messages, education may raise mother’s awareness of close supervision and their knowledge of environmental and other risks associated with inadequate supervision.16,17 Formal education enhances mother’s social and problem-solving skills, gathering and utilization of information in various situations. 18 Social skills may broaden mother’s social networks and interaction with well-educated individuals or childcare organizations usually serve as sources of information on childcare. 19 Thus, mother’s with more years of education can be in a privileged position to ensure their children’s well-being and to provide adequate supervision. 20 For instance, mothers with higher education are more inclined to enroll their young children in Early Childhood Education and Care programs which may advance children’s academic achievement through quality care and development. 21 Moreover, evidence suggests higher maternal education leads to greater maternal involvement and better academic performance of their children. 22 Despite this substantial evidence indicating the importance of mother’s formal education on child health and care,19,21-23 very few studies have examined the association of mother’s formal education and child supervision, particularly in LMIC. 24
Previous literature identified several predictors of child supervision practices such as child age, sex, spatial factors, number of household members, maternal education, and household socioeconomic status (SES).14,24,25 Evidence suggests higher SES may have positive and negative effects on child supervision across countries and regions. 14 However, households with higher SES may offer greater access to affordable childcare options, flexible work environments, social networks, and neighborhood safety.26-28 Thus, families with higher SES can reduce the risk of children left unsupervised, irrespective of mother’s educational background. Ruiz-Casares et al. 14 studied nonadult supervision in LMIC using the number of days children aged under 5 years were home alone and supervised by another child aged less than 10 years. The study included Multiple Indicator Cluster Surveys (MICS) and Demographic and Health Surveys (DHS) conducted during the years of 2010 to 2016. The study indicated that mother’s higher education was one of the contributing factors associated with the decrease in children home alone for countries in South Asia, East Asia and the Pacific, and Latin America and the Caribbean regions. However, previous studies did not explore the effect of any specific modifiable risk factors on child supervision14,24,25 that has motivated us to further study the effect of maternal education on child supervision practices in LMIC. Evidence suggests that mothers with higher education in LMIC can contribute to childcare costs, 29 and provide more attention to child supervision by ensuring their economic solvency.
To fill the existing knowledge gap, our study aims to estimate the current prevalence of children home alone and examine the association between mother’s formal education and under 5 years children home alone in 63 LMIC. Our study has included 35 additional eligible recent DHS and MICS surveys, which were released between 2016 and 2020, and were not included in the previous study. 14 Thus, this study provides an updated global prevalence of children home alone and explains how maternal education determines child supervision practices in LMIC.
Materials and Methods
Data Sources
This study used data from the most recent waves of 50 MICS and 13 DHS conducted between 2010 and 2020. MICS and DHS are multistage, stratified sampling surveys representative of each country’s general population, including indicators of children’s health and well-being. 30 The total eligible sample consisted of 589 452 children aged under 5 years from 81 countries (Figure 1). To draw statistically meaningful conclusions and model stability by preventing bias, countries with outcome prevalence less than 1% were excluded, and the resulting sample was 528 651 from 63 countries. The sample was finalized after excluding missing values in the mother’s education, covariates, and the outcome children home alone. We assumed and verified that missingness was completely at random because missingness did not affect the effect estimates. We, therefore, followed case-wise deletion to handle missing data and avoid any potential bias in the nationally representative sample size. We used original survey weight variable generated and suggested by MICS and DHS to avoid non-response and sampling bias for ensuring national representativeness of respective study sample. The resulting survey weighted total sample consisted of 501 769 children from 63 countries. Supplemental Tables S2 and S3 provide the list of countries with the initial sample and final sample, respectively.
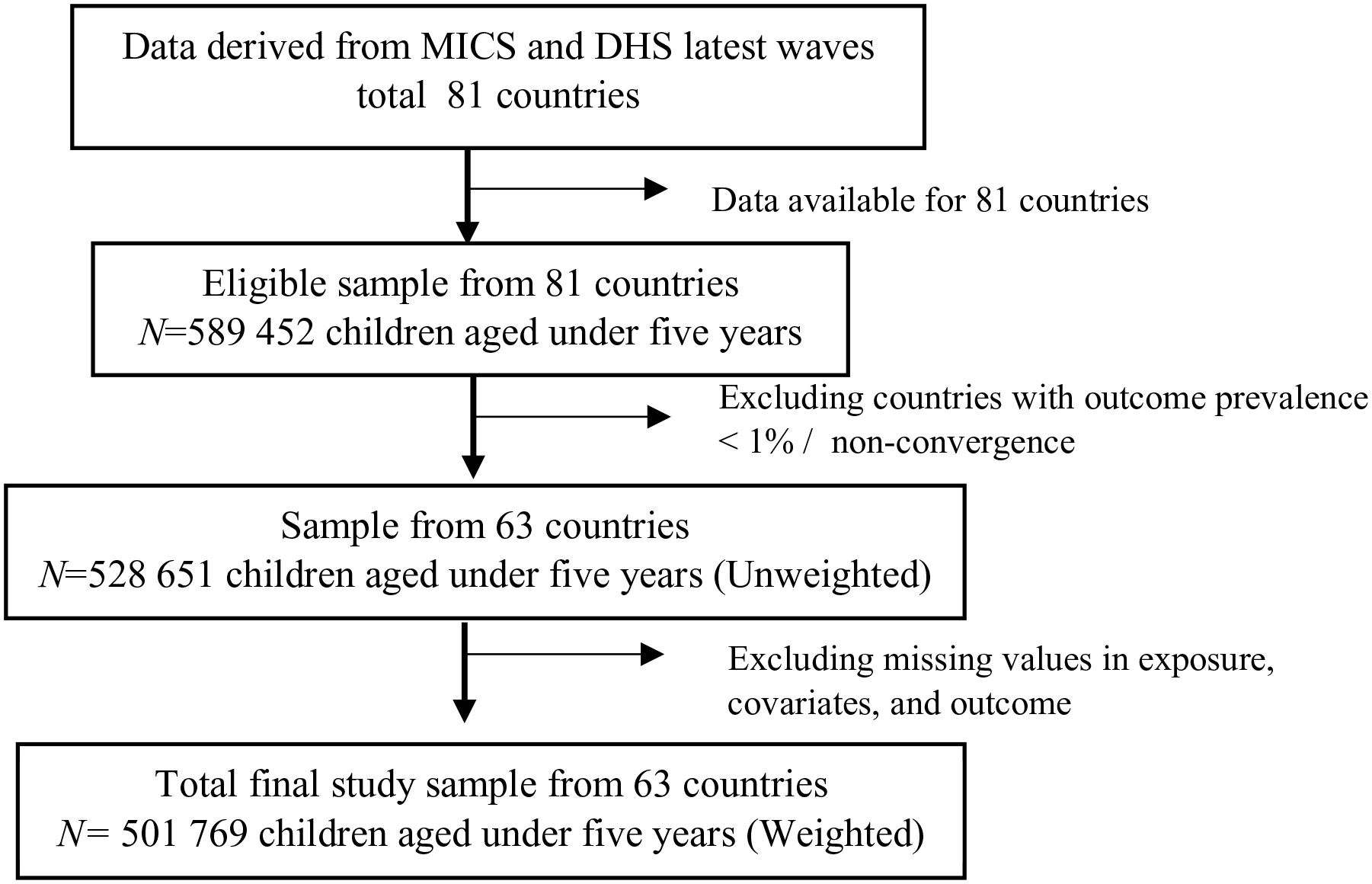
Schematic diagram of study sample.
Outcome: Children Home Alone
“Children home alone” was derived from responses on whether children aged 0 to 59 months were left alone at home for more than an hour during the week preceding the interview. More specifically, the question asked to mothers or caregivers was: “Sometimes adults taking care of children have to leave the house to go shopping, wash clothes, or for other reasons and have to leave young children. How many days in the past week was (name) left alone for more than an hour?” Responses ranged from 0 to 7 depending on the number of days the child was left alone. Later, responses were dichotomized with 0 referring to no days in the past week, and 1 referring to 1 to 7 days in the past week. 31 We have dichotomized the count outcome due to overdispersion, where the variance of the count data was way larger than the mean. Dichotomizing the count data addressed the overdispersion and made the data more amendable to Poisson regression modeling. Plus, dichotomizing the count data simplified the interpretation of study findings. However, additional analyses were also conducted using children home alone as count data to check robustness of our findings that are included in Supplemental Material (Table S7).
Exposure: Mother’s Formal Education
Mother’s formal education was classified differently across different countries in DHS and MICS datasets. For example, 1 country may have 3 distinct categories of post-secondary education while another may have only 2 or even just a single post-secondary category. In this study, mother’s formal education was dichotomized as: “low education” (ie, “no education and/or primary”) and “high education” (ie, “secondary or higher”) to avoid the heterogeneity of categorization, facilitate cross-country comparisons, and reduce the inflated effect estimates that may occur due to disproportionate samples in mother’s formal education.14,32 Mother’s formal education was thus coded as 0 (“low education”) and 1 (“high education”). We have also analyzed mother’s education as a continuous variable, represented by the number of years of education to investigate the potential misclassification of dichotomous maternal education variable and acknowledge country-specific diversity in education level (Supplemental Table S8).
While acknowledging the significance of father’s involvement in childcare and supervision, 33 we excluded father’s education from our statistical model due to its correlation with the main exposure “mother’s formal education,” and household wealth index. This addresses the issue of multicollinearity, reducing inflated standard errors and ensuring accurate estimates of the association between mother’s formal education and children home alone.
Covariates
Based on the prior literature,14,24,28,34 the following variables were included as covariates. Child age was in months ranging from 0 to 59. Child sex variable was coded “male” as 0 and “female” as 1. The variable urbanicity was coded as 0 (“none”) and 1 (“yes”). We have used the original variable “household wealth index” constructed by MICS and DHS. The household wealth index was constructed based on the possession of durable and non-durable assets including plough, livestock, tractor electricity, television, radio, watch, bicycle, tractor, source of drinking water, type of toilet, sharing of toilet facilities, the material of the principal floor, walls, roof, types of windows cooking fuel, agricultural land size owned, bank account, etc. 35 Using principal component analysis (PCA) and its first PCA component, each of these assets was assigned a score, and individual households were then placed on a continuous score presenting the relative wealth. Subsequently, the households were split into 5 quintiles, poorest at the bottom and richest at the top, representing the highest quintile. Household wealth index is recommended and usually used as a proxy of household income in LMIC.24,25 Mother’s marital status for women aged 15 to 49 years was classified into 3 values. Thus, mother’s marital status was coded as 1 (currently married/ in union), 2 (formerly married/ in union), and 3 (never married/ in union). The variable “number of adults aged 15 years or older” constructed by a count of household members aged 15 and up from the household roster. The variable household size was defined as the total number of individuals in the household and mother’s age was in years ranging from 15 to 49 years.
Statistical Analyses
The prevalence and 95% confidence intervals (CIs) of children home alone aged 0 to 59 months were calculated (Figure 2, Supplemental Figure S1, and Supplemental Tables S2 and S3). We estimated Prevalence Ratios (PRs) using multivariable Poisson regression to investigate the association between mother’s formal education and children home alone. Instead of using odds ratios (ORs) from logistic regression, we used Poisson regression because ORs can inflate the coefficient of common outcomes measured in cross-sectional studies.36,37 Our final model adjusted for covariates associated with children home alone.14,24 Supplemental Table S1 provides the details of the covariates and modeling strategies.

Prevalence of children 0 to 59 months home alone as a percentage of all children within that age group in the country, N = 514 230 (weighted sample).
As a part of the sensitivity analysis, the study used Quasi-Poisson regression to model the association between mother’s formal education and “children home alone” as a count outcome to check robustness of our main analysis (Supplemental Tables S6 and S7). We conducted additional analysis treating mother’s formal education as a continuous variable to check distortion of the main effect estimates due to the potential misclassification of binary maternal education variable (Supplemental Table S8). Results are presented as Prevalence Ratios (PRs) with 95% CIs. We used survey weights and robust error variance for all statistical analyses to reduce non-response bias 38 and estimate precise standard errors. 39 A 2-sided P-value ≤.05 was considered statistically significant, and Stata version 17 was used in all the statistical analyses. 40
Results
Regional Analysis of Prevalence of Children Home Alone
Figure 2 and Supplemental Table S3 illustrate the prevalence of children home alone across 63 countries in 7 regions.
In East Asia and Pacific region (EAP), the lowest prevalence was 1.3% (95% CI: 1.0%-1.8%) in Vietnam and the highest prevalence was 27% (95% CI: 25.1%-29.1%) in Kiribati. In Eastern and Southern Africa (ESA) region, the lowest prevalence was 5.3% (95% CI: 4.0%-6.0%) in Lesotho and the highest prevalence was 25.8% (95% CI: 25.0%-26.7%) in Uganda. Europe and Central Asian (ECA) region had very low prevalence of children home alone. The lowest prevalence was 1.4% (95% CI: 0.9%-2.1%) in Moldova and the highest prevalence was 2.8% (95% CI: 1.9%-4.1%) in Macedonia. In Latin America and Caribbean (LAC) countries, the lowest prevalence of children home alone was 1.1% ( 95% CI: 0.8%-1.6% ) in Paraguay and the highest prevalence was 14.6% (95% CI: 13.3%-16.1%) in Haiti. In Middle East and North Africa region (MENA), the lowest prevalence of children home alone was found in Egypt at 3.1% ( 95% CI: 2.8%-3.4%) and Jordan had the highest prevalence of children home alone at 12.8% (95% CI: 11.5%-14.2%). Among South Asian (SA) countries, the lowest prevalence was 5.6% (95% CI: 5.0%-6.4%) in Bhutan and the highest prevalence was 29.3% (95% CI: 28.4%-30.2%) in Afghanistan. Finally, the West and Central African (WCA) region showed the highest prevalence of children home alone worldwide. The lowest prevalence was 9.4% (95% CI: 8.6%-10.2%) in The Gambia and the highest prevalence was 50.1% (95% CI: 49.2%-51%) in Chad.
Association Between Mother’s Formal Education and Children Home Alone
Figure 3 (Supplemental Tables S5, S7, and S8) shows how the covariate-adjusted association between children home alone and mother’s formal education varies across 63 countries.

Mother’s formal education and children home alone aged under 5 years old in 63 LMIC.
At the defined P value no association between mother’s formal education and children home alone was identified in 44 countries. The association between mother’s formal education and children home alone was, however, negative and statistically significant in 16 countries and positive in 3 countries. In EAP region, mother’s high education relative to mother’s low education was associated with a reduction of children home alone in Cambodia by 33% (aPR: 0.67; 95% CI: 0.44-1.00) and Myanmar by 33% (aPR: 0.67; 95% CI: 0.48-0.95). In ESA region, the association between children home alone and mother’s high education in comparison to low education was a reduction of 26% in Burundi (aPR: 0.74; 95% CI: 0.57-0.97), 42% in Lesotho (aPR: 0.58; 95% CI: 0.37-0.97), 36% in Rwanda (aPR: 0.64; 95% CI: 0.47-0.87), and 15% in Uganda (aPR: 0.85; 95% CI: 0.77-0.94). In ECA region, we observed negative association between mother’s high education and children home alone compared to mothers with low education in Kosovo by 65% (aPR: 0.35; 95% CI: 0.13-0.95) and Macidonia by 71% (aPR: 0.29; 95% CI: 0.08-1.00). In LAC region, mother’s high education was significantly associated with reductions in children home alone in Belize by 28% (aPR: 0.72; 95% CI: 0.54-0.96), Colombia by 36% (aPR: 0.64; 95% CI: 0.45-0.91), Haiti by 37% (aPR: 0.63; 95% CI: 0.50-0.80), Mexico by 64% (aPR: 0.36; 95%CI: 0.21-0.59), and Uruguay by 69% (aPR: 0.31; 95% CI: 0.13-0.75) compared to mothers with low education. For MENA region, mother’s high education relative to mother’s low education was associated with reduction in children home alone in Tunisia by 46% (aPR: 0.54; 95% CI: 0.34-0.86). Mother’s high education compared to mother’s low education was not associated with children home alone for any country in the SA region. Lastly, in WCA region, mother’s high education versus mother’s low education was associated with reductions in children home alone in Chad by 9% (aPR: 0.91; 95% CI: 0.86-0.97) and Mauritania by 21% (aPR: 0.79; 95% CI: 0.67-0.93). This relation was also associated with increase in child home alone in Côte d’Ivoire by 25% (aPR: 1.25; 95% CI: 1.01-1.56), Nigeria by 23% (aPR: 1.23; 95% CI: 1.14-1.32), and Senegal by 29% (aPR: 1.29; 95% CI: 1.15-1.44).
The findings from Quasi-Poisson regression were consistent with our main findings (Supplemental Table S7). Futhermore, mother’s formal education as a continuous variable showed almost similar effect on children home alone (Supplemental Table S8).
Discussion
The study reveals variation in the prevalence of children under 5 years of age home alone across 63 LMIC in 7 regions. Overall, the prevalence of young children home alone was lowest in the ECA region and highest in the WCA region. Among all LMIC in our study, the proportion of under 5 children home alone was lowest in Paraguay (1.1%) and highest in Chad (50.1%). This is consistent with findings from previous research by Ruiz-Casares et al. 14 In Chad, higher poverty rates and family needs may compel parents and other family members to work outside home, leaving no adult available for child supervision. 41 In addition, lower female literacy rate in Chad could lead to lack of awareness regarding child injuries and other risks and thus affecting child supervision practices. 42 Furthermore, repeated humanitarian crises such as outbreaks of measles and cholera, floods and higher prevalence of HIV/ AIDS can result in loss of parents or older adults leading to increase in children left home alone.43-45
We found negative, positive, and null associations between mother’s formal education and children home alone across LMIC. More years of maternal education is a protective factor for children less likely to be left home alone in 16 LMIC. Mothers with greater education can make informed decisions or follow evidence-based child supervision practices due to their comprehensive parenting knowledge, access to information and resources, and existing socio-cultural norms.16,46,47 For instance, mothers with more years of education might consider both child’s age and developmental level for supervision. 48 It is likely that mothers with more years of formal education have the ability to assess their children’s socio-emotional, physical, and cognitive development, 48 thus, can decide on the extent to which children require supervision and avoid leaving children unattended. Moreover, mothers with greater education are more likely to delay having children or to have fewer children and, consequently, can extend the duration of childcare, and resources such as arranging childcare facilities for their children. 47 In terms of providing resources to the children, mothers with higher education have higher employability and are in a more advantageous position. The economic solvency of working mothers ensures autonomy and freedom of childcare decisions within the household, ranging from child nutrition to childcare arrangements49,50 and enables mothers to hire additional help for childcare. 51 In addition, the affordability of childcare arrangements can be possible with an increase in income or sometimes through the childcare policies of the workplace. In Mexico, for example, some parents employed in the formal sector may have the option to bring their children to their workplace, thus reducing the need to leave children home alone. However, children were brought to workplaces only during emergencies. 28
The observed protective association of greater maternal education and decrease in children home alone can also be attributed to gendered norms shaped by traditional beliefs that divide the household labor between males and females and influence supervision practices in many LMIC.46,52 Despite higher education women’s prescribed roles such as managing household responsibilities and taking care of the children in some traditional societies can be associated with lower prevalence of children home alone.53,54
Our results indicate that Nigeria, Senegal, and Côte d’Ivoire were the only countries where more years of maternal formal education was associated with increases in children home alone. One of the contributing factors could be religious beliefs and predominant Muslim culture prevalent in these 3 countries. Muslim societies in West and Central African regions often exhibit higher birth rates compared to other religious communities, reflecting a cultural inclination toward larger families. 55 This cultural preference may persist even when mothers have higher education, presenting challenges in adequately caring for many children. Consequently, managing the associated costs of childcare becomes more challenging for them. In addition, the transition from extended to nuclear family contributes to fewer available family members for childcare. 56 Given that mothers are often the primary caregivers, working parents in many societies are left with little or no choice but to leave their children unattended by adults. Further, the existing gender-based inequalities in the labor markets of these 3 countries which may contribute to the scenario where even mothers with more education struggle to find decent employment opportunities with fair pay and work-life balance, and access to childcare facilities. 57 Ultimately, this situation precludes mothers from providing adequate supervision since they have limited time and money to secure alternative child care. 58 Further, short-term paid maternity leave policies in these countries (typically last for 4-6 months) may explain the positive association where mothers with more years of education employed in formal sector have to leave their children home alone.59-61
We did not observe statistically meaningful association between mother’s formal education and children home alone for 44 LMIC across 7 regions. We have, therefore, evaluated sensitivity and robustness of these varied patterns of findings analyzing mother’s formal education as continuous exposure variable and children home alone as count outcome. These additional analyses showed coherence with our main findings. However, the null and inconsistent association of maternal education with children home alone can be explained by culture or changes in primary caregivers which reduce the influence of mother’s education.48,56,62 Moreover, child care is often family oriented 63 and the participation of grandparents or grandmothers should be considered further. For instance, a study in Mexico suggests grandmothers are the primary caregivers and they care for nearly 40% of children aged under 6 years. 64 In addition, some cultures may emphasize on fostering autonomy and independence for children while others may prioritize on obedience and conformity, thus affecting supervision practices. 65 These suggest that child supervision is a multifaceted and contextual practices 66 and may not solely explain by mother’s level of education. Therefore, drawing conclusions from country-level prevalence may not offer adequate insights into the underlying mechanism influencing associations between mother’s education and children home alone.
This study has several limitations. The cross-sectional nature of the data prevents establishing a causal link between maternal education and children home alone. Future studies should compare prevalence across different survey waves and assess changes associated with maternal education and paternal education. The study outcome was based on self-reported data. Relying on self-reported data can introduce the possibility of recall bias and social desirability bias. Furthermore, the study focuses on maternal characteristics due to the emphasis of MICS and DHS surveys on women and household information. However, future studies should also consider fathers’ education and occupation data from a more dynamic perspective, as these factors are closely linked to maternal education and the household wealth index used. This would provide a more comprehensive understanding of child supervision practices. In essence, the methodological limitation of lacking comprehensive information on fathers’ social characteristics and properly isolating their effects on child supervision should not hinder future research efforts. Changes in MICS and DHS questionnaires could facilitate this by incorporating data on fathers, allowing for a more accurate assessment of their impact on child supervision practices. Therefore, future research should explicitly include fathers’ characteristics in analyses to properly isolate their effects not only on child supervision but also on other child outcomes. The term “child supervision” has varying definitions across disciplines. 24 Our study used the definition of UNICEF implemented in MICS and DHS. However, this definition may not capture variations in living conditions, cultural expectations, and local understandings of childcare. When considering child supervision practices and the perception of what it means to be “alone,” it may be imperative to consider context and cultural norms and values that may influence these practices. While our study findings contribute to the existing body of literature by revealing both positive and negative associations between mother’s formal education and children home alone across countries, we also acknowledge several limitations. Our study could not determine the consistency of underlying mechanisms affecting children home alone in different country contexts. To address this gap, conducting country-specific studies is necessary to delve deeper into underlying mechanisms influencing child supervision practices. Country-specific research and policies can help to reduce the prevalence of unsupervised children and achieve sustainable development goals (SDGs), particularly SDG targets 3.2 and 4.3, aimed at under-5 mortality and early childhood development. 67
Conclusions
This study showed diverse patterns of associations between mothers’ education and children home alone across countries, offering nuanced insights into child supervision practices in a global context. The negative association between education and children home alone across countries highlights the importance of maternal higher education in childcare decision-making. However, initiatives aimed at promoting education for girls and mothers, which could potentially improve supervision practices, must not overlook the importance of interventions specifically targeting fathers, as they also play a crucial role in childcare. Therefore, interventions should empower both mothers and fathers by improving access to childcare facilities and ensuring adequate supervision. This, in turn, will contribute to LMICs’ efforts to achieve the Sustainable Development Goals (SDGs) related to ensuring quality care and development for children.
In addition, the positive and null results across countries suggest the possibility of additional factors influencing these associations in these specific countries, that highlight the need to consider local factors beyond maternal education. For instance, to what extent in countries such as Nigeria, Senegal, and Côte d’Ivoire, increases in women’s years of education may be ultimately limited by socioeconomic structural conditions or cultural practices (ie, the presence of income ceilings or religion) is a question that needs to be addressed to understand the direction of this association more specifically. Nevertheless, the interconnected nature of maternal education and accessible alternative childcare should be outcomes promoted by policymakers to support child supervision practices more holistically. These strategies can address the diverse needs of families in different regions and localities, contributing to more effective and equitable childcare practices. Building on this multi-country based evidence, country-specific qualitative research can delve deeper into the mechanisms affecting parents or adults leaving their children home alone.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241258179 – Supplemental material for Maternal Education and Children Home Alone in 63 Low- and Middle-Income Countries
Supplemental material, sj-docx-1-gph-10.1177_2333794X241258179 for Maternal Education and Children Home Alone in 63 Low- and Middle-Income Countries by Toufica Sultana, Mónica Ruiz-Casares, René Iwo, Magdalena Janus and José Ignacio Nazif-Muñoz in Global Pediatric Health
Footnotes
Acknowledgements
We would like to thank Dr. Afua Twum-Danso Imoh for her critical remarks and language edits. We also thank Emilia Gonzalez and Yinan Yu for updating and preparing the MICS and DHS databases for analysis. We appreciate Negin Zamani for coordinating meetings with the project team members. Additionally, we extend our gratitude to Dr. Maliphone Douangphachanh, Dr. Camila Pereira, Ruo Ying Feng, and Samaneh Mansouri for their contributions to the larger study.
Author Contributions
TS: Contributed to design, data analysis, and interpretation; Drafted the manuscript; Critically revised the manuscript, Gave final approval, Agrees to be accountable for all aspects of work ensuring integrity and accuracy. MRC: Contributed to conception and design, contributed to fund and data acquisition, Drafted the manuscript, Critically reviewed and revised the manuscript, Gave final approval, Agrees to be accountable for all aspects of work ensuring integrity and accuracy. RI: Contributed to data management, Critically revised the manuscript, Gave final approval, Agrees to be accountable for all aspects of work ensuring integrity and accuracy, MJ: Contributed to conception and design, Contributed to analysis and interpretation, Critically reviewed the manuscript, Gave final approval, Agrees to be accountable for all aspects of work ensuring integrity and accuracy, JINM: Contributed to conception and design, Contributed to analysis and interpretation, Drafted the manuscript, Critically reviewed and revised the manuscript, Gave final approval, Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Data Availability
Publicly available datasets were analyzed in this study. Data can be accessed from these websites: https://mics.unicef.org/ and ![]()
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Social Sciences and Humanities Research Council of Canada, grant number 435-2020-0685, and José Ignacio Nazif-Muñoz was funded by Fonds de Recherche du Québec—Santé, grant number 280-205.
Ethical Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the McGill University Faculty of Medicine and Health Sciences (protocol code A09-E84-09B) and the Ethics Board of Toronto Metropolitan University (protocol code 2022-421). The research is based on publicly available secondary datasets obtained from UNICEF’s MICS and DHS repositories. These surveys were originally conducted by UNICEF and Macro International, and consent was obtained from participants at the source by UNICEF and Macro International. We utilized aggregated and anonymized data that did not involve direct contact with or the need for informed consent from the respondents.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.