
Abstract
The wait time clients spend during immunization clinic visits in low- and middle-income countries is a not well-understood reported barrier to vaccine completion. We used a prospective, observational design to document the total time from client arrival-to-discharge and all sequential provider-client activities in 1 urban, semi-urban, and rural immunization clinic in Nigeria. We also conducted caregiver and provider focus group discussions to identify perceived determinants of long clinic wait times. Our findings show that the time from arrival-to-discharge varied significantly by the clinic and ranged between 57 and 235 minutes, as did arrival-to-all providers-client activities. Focus group data attributed workflow delays to clinic staff waiting for a critical mass of clients to arrive for their immunization appointment before starting the essential health education talk or opening specific vaccine vials. Additionally, respondents indicated that complex documentation processes caused system delays. Research on clinic workflow transformation and simplification of immunization documentation is needed.
Introduction
Immunization against vaccine-preventable childhood diseases is a public health victory. Worldwide, the proportion of children who received 3 doses of diphtheria, tetanus, and pertussis-containing vaccine rose by 60% between 1980 and 2019. 1 However, due to complex barriers, the global immunization coverage has remained unchanged over the last decade at 85%. 1 Although the literature indicates long clinic wait time is a barrier to immunization completion,2-8 quantification of the total time clients spend at an immunization clinic visit, and the factors contributing to the experienced wait times is not well described. This study aimed to describe and compare the duration of wait times in 3 different immunization clinics in Ondo State, Nigeria, and determine drivers of immunization clinic wait times.
Materials and Methods
Study Design and Setting
We used a prospective observational design consisting of quantitative and qualitative methods to quantify the time caregivers and their babies (clients) spend from arrival-to-discharge, to all provider-client activities, and the determine determinants, consequences of, and potential interventions for long immunization clinic wait times.
We conducted the study in 3 immunization clinics, each representing an urban, semi-urban, and rural setting, located in government-run hospitals in Ondo State, Nigeria. Ondo State is in the southwest region of Nigeria with a project 2016 population size from the 2006 national census of 4 million. 9 The urban site was the Mother and Child Hospital Akure (Akure), the rural site was the Comprehensive Health Center Moferere, Oja (Oja), and the semi-urban site was the Mother and Child Hospital Ondo (Ondo).
Study Population and Sampling
To obtain quantitative measures of clients’ wait time and time to complete provider tasks, we observed all caregivers who brought their child or ward to the immunization clinic and all providers involved in each provider-client activity on the day of the site observation.
For the caregiver focus group discussion, the immunization clinic coordinator and a research assistant gave caregivers an open invitation, explaining the purpose of the discussion, time commitment, and compensation. We then chose a convenience sample of caregivers willing to participate. For the provider focus group, we employed a purposive sampling of clinic providers that included at least 1 senior medical or administrative staff from each clinic. At Oja and Ondo, we included all medical staff in the discussion.
Study Procedures
Procedures for determining time spent on provider-client activities
Each clinic attended to clients according to the order of arrival. Providers completed the provider-client activities in the following general sequence: (1) locate the duplicate immunization card kept in the clinic; (2) complete the immunization card registration by documenting the date and type of immunization to be received, setting the next appointment date, and documenting clinic immunization data in separate Local, State, and Federal government forms; (3) obtain and record the anthropometric measurements of the client; (4) provide a health education talk to caregivers; (5) administer vaccine(s); and (6) discharge clients from the clinic. Although these activities were designed to follow a general sequence, some tasks may have commenced before the prior task was completed. For example, during the immunization registration in the immunization card or clinic immunization register, a client may have their weight checked. Furthermore, all clinic activities were paused during the immunization health talk to ensure all present clients received the same information and were attentive.
Each caregiver received a unique identification number upon arrival. The research assistant stationed at each provider-client activity station observed and recorded client arrival and completion time at each activity station and discharge by the unique identification number. The time each provider activity started and ended was also recorded. At the end of the observation, each research team’s recordings were collated by the unique identification number.
Focus group procedures
We conducted 1 caregiver and provider-focused group discussion at each site between March and April 2019. Two research assistants coordinated the discussions under the supervision of the local study principal investigator. The research assistants received informal training on conducting focus group discussions by the study principal investigator and underwent 2 mock interview sessions in preparation. A focus group guide with broad opening questions targeted perceptions of wait times, determinants, consequences, and potential interventions related to clinic wait times. The interviews were conducted in English and the local dialect, Yoruba, recorded and transcribed verbatim into English. Each session lasted 30 to 45 minutes and occurred on a different day from the workflow observations.
Data analyses
We described the mean duration of time for each provider-client encounter and compared the time interval between arrival to discharge and each provider-client activity among sites using a 1-way ANOVA. Because 2 sites conducted their immunization talk before 10:00 AM, we grouped clients into early or late arrivals based on presentation to the immunization clinic before or after 09:00 AM. We compared the total duration of time spent in the clinic between the early and late arrivals using the unpaired students’ t-test. We also performed a simple linear regression to compare total time spent in the clinic based on arrival hour.
For focus group qualitative analysis, the primary (OAE) and senior (AR) author first coded 2 transcripts independently using an emergent thematic analysis approach10,11 and devised an initial set of codes. After discussion and revision of the code-set, the primary author coded all 6 focus group transcripts. The senior author reviewed each transcript independently as well, making additional comments and suggested codes. Both authors met to discuss and resolve coding discrepancies and compare memos and impressions of the overall coding. Then each major code theme was assigned to an author for further summarization and synthesis with the explicit charge to compare and contrast response themes by both site and respondent type to discern consistent or contradicting elements relevant to the functioning of each clinic.
Ethical approval and informed consent
The Ondo State ethical review board approved the study (Protocol # OSHREC/17/12/2018/080). Indiana University institutional review board assessed this research exempt from full ethical review (Protocol # 1809642347). Each focus group participant gave written informed consent before any study activity.
Results
On the observation days, Akure, Oja, and Ondo’s immunization clinics had 81, 35, and 26 clients, respectively. The Figure 1 summarizes the mean time from arrival-to-discharge and provider-client activity. Briefly, the duration of time from arrival-to-discharge, vaccination, and card sorting differed significantly across sites. Clients at Akure spent significantly more time from arrival-to-card registration compared to clients Oja and Ondo, and from arrival-to-the start of the health talk compared to clients at Ondo.

Box plot comparing the mean duration of time from arrival to patient-provider activity and discharge by study site.
Time for providers to complete all provider-client activity ranged between 1 and 2 minutes across sites (Table 1). However, the health talk was the lengthiest provider-client encounter—15, 8, and 21 minutes at Akure, Oja, and Ondo, respectively—and most variable. The health talk session began at 09:23 AM at Akure, 10:06 AM at Oja, and 09:36 AM at Ondo. There were 17 (21%), 2 (8%), and 7 (20%) of caregivers from Akure, Ondo, and Oja, respectively, who arrived after the health education talk had commenced. Arrival at or before 09:00 AM, resulted in an average of more 52 minutes in the clinic compared to arrivals after 09:00 AM. Every additional hour of a client’s arrival resulted in 25 minutes less time spent in the immunization clinic.
Mean Time in Minutes Observed for Providers to Complete Each Clinic Activity by Site.
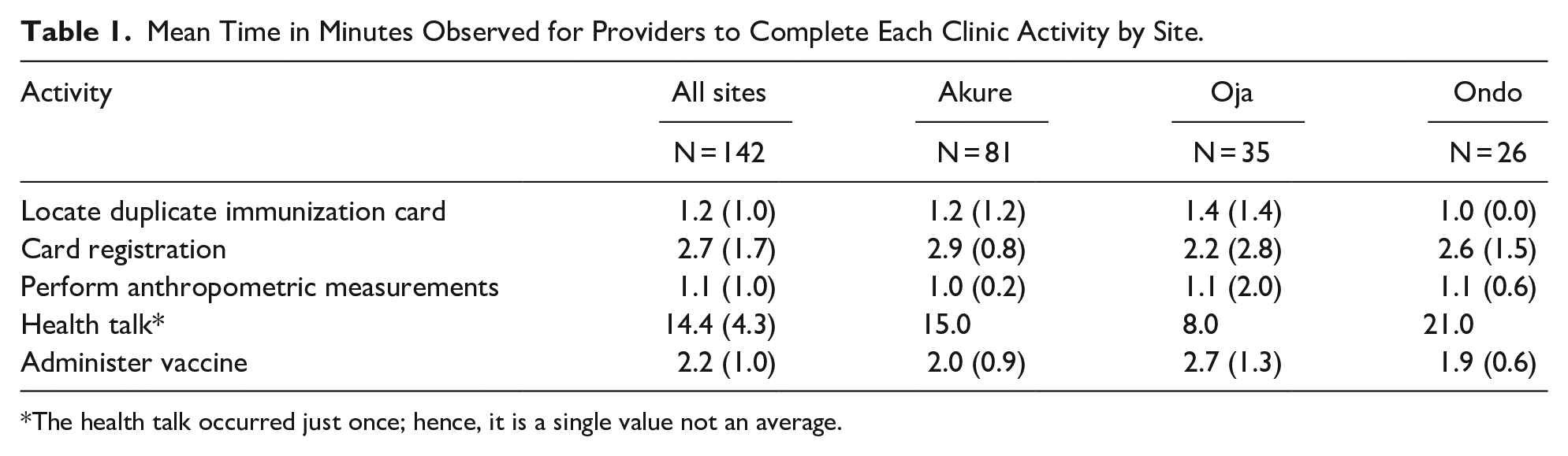
The health talk occurred just once; hence, it is a single value not an average.
The caregivers’ focus group discussions included 6 subjects from Akure and 5 each from Oja and Ondo. The provider focus group included 6 out of the 8 medical staff from Akure, and all 4 and 3 medical staff from Oja and Ondo, respectively. The demographic information of participants are presented in Table 2.
Demographic Distribution of Focused Group Participants by Study Site.

All caregivers were the mothers of the infant receiving the immunization.
Major topics and their themes from the caregiver and provider focus group. For privacy, we anonymized the clinics as site 1, 2, and 3.
Perceptions About Time Spent in the Clinic
All the caregivers at site 1 felt the immunization
Factors Contributing to Long Wait Times
As a justification, providers indicated the need to have a reasonable number of clients before starting because they
Providers at site 1 identified
The Consequence of Long Wait Times
Caregivers at site 1 were most concerned that the long wait at the vaccine clinic
Potential Solutions for Long Wait Times
At site 1, the providers suggested they needed
The subtheme of solutions for waiting for a critical mass of clients to use certain vaccines revolved around batching. One caregiver suggestion was to
Several caregivers and providers at site 2 and 3 emphasized the need for
Discussion
We evaluated the duration and determinants of immunization clinic wait time in an urban, semi-urban, and rural setting in southwest Nigeria. Mean time to clinic and discharge varied significantly by site and was perceived to be determined by both workflow and system-related factors. Providers waiting for the arrival of a critical mass of clients before starting the health talk was a notable workflow barrier. The health talk is an essential clinic activity and primary source of information on vaccinations, maternal, and child health issues. 12 In a study on vaccine communication in Cameroon, waiting for the health talk to begin was a cause of long clinic wait time. 13 We expected that the health talk start time would relate to total time in the clinic. However, caregivers in the study site (Akure) with the earliest health talk start time (09:23 AM), on average, spent the longest time in the clinic compared to the other sites. Interestingly, the proportion of total clinic clients present before the start of the health talk was associated with longer overall clinic wait times.
For provider-client encounters, Akure had the longest wait times. These findings may be attributed to Akure having a larger client population. However, workflow inefficiency may also be a factor. Akure completed its clinic, local, state, and federal government registers in real-time, while the other centers completed them separately from clients’ care time, contributing to the overall longer wait time experienced in Akure.
The discrepancy in knowledge between different administrators and their staff, as well as between caregivers and providers regarding multi-dose vial vaccines implies a need for provider education. This is very important because the measles vaccine uptake is the lowest amongst the routine vaccinations in Nigeria and other low-resourced countries.1,14,15 In a study from Nigeria on vaccine wastage, 45% of surveyed providers had a knowledge gap in multi-dose vial policy. 16 Furthermore, of the surveyed caregivers, 30% who had been turned away for vaccination at least once due to prevailing multi-dose vial usage policy, and of these, 53% had not received the missed dose when assessed. 16
Recommendations
Based on these findings, we proffer potential solutions to identified barriers. One strategy is to create an audio or audio-visual recording of the health talk that plays on a loop every 15 to 30 minutes, with intermittent periods for questions and answers. After this, a group of clients who listen to the audio or audio-visual health talk can move on to receive their immunization without further delay. With this solution, providers need not wait for a critical mass of clients to give the health talk. Secondly, sites could limit the concurrent completion of all registers and focus on client workflow. However, this means that time must be set aside at the end of the clinic session to complete this task, which will cause delays in providers’ closing time and could lead to error entry. Finally, a digital registry could be introduced, where the information filled out in 1 digital sheet can populate all registers and be transmitted in real-time to stakeholders and policymakers. However, the cost of such a system may limit widespread adoption in the resourced limited sub-Saharan Africa and South Asia countries. One estimate puts it between US$3.6 to US$4.2 million. 17
Our study has several limitations. We only sampled one site per region, and we only evaluated sites on one clinic day. However, from the caregivers’ and providers’ comments, the long wait times observed in this study are similar to past experiences. We did not specifically collect data on time to complete the immunization registries for local, state, and federal governments. Nonetheless, we could infer the time based on the overall caregiver wait times, as well as provider comments about the burden of repetitive documentation. Finally, we did not record the actual sequence order of each provider-client encounter which could impact wait times. However, we aimed to evaluate the current workflow and how it affects efficiency. Additionally, client arrival time and the timing of the health talk appeared to be key determinants of wait time and were carefully measured in this study.
Conclusion
Time from arrival to discharge and provider-client activities varied among sites and were determined by workflow and system factors. Simple and innovative changes to the workflow and investment in a simplified documentation process could make the clinic workflow more efficient and satisfactory to client caregivers and providers.
Footnotes
Acknowledgements
We would like to thank the clients and staff of the Mother and Child Hospital Akure, the Comprehensive Health Center Moferere, and the Mother and Child Hospital Ondo. We also want to thank the study research assistants, Ms. Tosin Akinrinlola and Ms. Bukola Fasoyinu.
Author Contributions
OAE, ROO, AO, BM, PB, EM, and AR all made a substantial contribution to the concept or design of the work; or acquisition, analysis, or interpretation of data, OAE drafted the article and ROO, AO, BM, EM, and AR revised it critically for important intellectual content, All authors approved the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by the IU School of Medicine Program to Launch those Underrepresented in Medicine Toward Success (PLUS) program.
Ethics Approval and Informed Consent
The Ondo State ethical review board approved the study. Indiana University institutional review board assessed this research as meeting the exemption conditions from full ethical review under section 45 code of federal regulation 46.101(b). Each focus group participant gave written informed consent before any study activity.
Consent for Publication
All authors have read and approved the final version of this manuscript.
Research Ethics and Patient Consent
The study protocol was approved by the Ondo State ethical review board approved the study. Indiana University institutional review board assessed this research as meeting the exemption conditions from full ethical review under section 45 code of federal regulation 46.101(b).
Availability of Data and Material
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.