
Abstract
Background:
In low- and middle-income countries (LMICs), nearly 21 million adolescents become pregnant every year. Half of these pregnancies are unplanned, and more than half of unintended pregnancies result in unsafe abortion, which accounts for a major proportion of adolescent pregnancies worldwide. This study intended to assess the pooled proportion of adolescent pregnancy and associated factors in LMICs.
Methods:
A community-based cross-sectional study design was employed. The data were taken from 47 LMICs from 2015 to 2024. A total of 327,394 (weighted = 323,767) adolescents aged 15 to 19 years were included. The data were sourced from the demographic and health survey (DHS) datasets available online. Data were analyzed using STATA V.17. We used multivariable multilevel logit regression for the outcome variable. The p-values < 0.05 were regarded as statistically significant, and the adjusted odds ratios with 95% confidence intervals (CIs) were computed from the final model. The candidate model was evaluated using the Deviance Information Criterion.
Results:
The pooled proportion of adolescent pregnancy among all adolescent girls in 47 LMICs was 23% (95% CI: [20, 26]). It ranges from 10% (95% CI: [6, 14]) in North Africa/West Asia/Europe to 28% (95% CI: [25, 32]) in sub-Saharan Africa (SSA). No formal education (AOR = 1.10, 95% CI: [1.04, 1.16]), primary education (AOR = 1.58, 95% CI: [1.51, 1.66]), middle wealth index (AOR = 0.83, 95% CI: [0.80, 0.87]), rich wealth index (AOR = 0.58, [0.55, 0.61]), media exposure (AOR = 0.86, 95% CI: [0.83, 0.89]), aged 18 to 20 (AOR = 4.33, 95% CI: [4.17, 4.49]), female household heads (AOR = 1.40, 95% CI: [1.35, 1.46]), condom use (AOR = 0.79, 95% CI: [0.74, 0.85]), contraceptive use (AOR = 0.44, 95% CI: [0.42, 0.46]), knowledge of contraception (AOR = 0.38, 95% CI: [0.35, 0.41]), being married (AOR = 9.02, 95% CI: [8.91, 9.73]), having a bank account (AOR = 0.89, 95% CI: [0.83, 0.96]), being from SSA (AOR = 8.79, 95% CI: [6.96, 10.24]), Central Asia (AOR = 2.96, 95% CI: [2.16, 3.67]), South and Southeast Asia (AOR = 1.65, 95% CI: [1.35, 2.03]), Oceania (AOR = 4.11, 95% CI: [2.66, 5.01]), Latin America and the Caribbean (AOR = 5.83, 95% CI: [4.93, 6.49]) were significantly associated with adolescent pregnancy.
Conclusion:
The pooled proportion of adolescent pregnancy is high in the study area with significant disparity. Improving women’s education, media exposure, financial support, knowledge, and access to contraceptive and condom use among adolescents were potential modifiable factors to reduce adolescent pregnancy. The WHO regions, such as SSA and the South and Southeast Asia regions, need particular attention to lower adolescent pregnancy rates.
Background
Adolescence is the stage between childhood and adulthood during which individuals undergo physical, mental, and social development. 1 During this period, they explore their environment and form new relationships. Peer pressure can influence adolescents and expose them to risky behaviors, potentially leading to frequent unprotected sex.2,3 Adolescent pregnancy can be influenced by a complex structural, cultural, and socioeconomic factors, 3 such as marriage, substance abuse, family experiences of adolescent birth, a lack of sex education, and limited health services. 2
As of 2023, nearly 17% of adolescent girls worldwide gave birth before the age of 18, although this rate varies significantly across regions. 4 According to 2020 estimation, approximately 21 million girls aged 15 to 19 become pregnant every year, demonstrating adolescent pregnancy as a persistent public health concern in low- and middle-income countries (LMICs). Notably, half of these pregnancies are unintended, and more than half (55%) of unintended pregnancies end in unsafe abortions. 5 While early childbearing has decreased overall, the rate of change has varied across countries and regions. It is important to note that the vast majority (90%) of births to adolescent girls aged 15 to 19 occur in LMICs. 6
In a global context, adolescent pregnancy can increase the risks of various adverse outcomes, including infections 7 and complications such as obstetric fistula, 8 preeclampsia/eclampsia, low birth weight, preterm birth, 9 and postpartum hemorrhage 10 because the bodies of young adolescents may not be physically or biologically mature enough to handle pregnancy and childbirth.4,11,12 According to previous studies, mothers aged 10 to 19 have a significantly higher risk (6.7%) of developing preeclampsia/eclampsia globally, and the risk becomes nearly double (11.5%) in LMICs. 13 Similarly, adolescent pregnancy is associated with postpartum hemorrhage. 7 Adolescent pregnancy remains a leading cause of maternal mortality.1,14 According to 2023 data, maternal conditions were among the top five causes of morbidity and mortality globally in adolescent girls aged 15 to 19 years. 4 Newborns are also at risk; studies show that infants born to adolescent mothers have a higher risk of mortality. 15 Furthermore, premature membrane rupture, cephalo-pelvic disproportion, and low birth weight were among the adverse birth outcomes associated with adolescent pregnancy.6,16–18 In addition to the direct health risks, pregnancy during adolescence has socioeconomic repercussions, including school dropout, drug abuse, unemployment, poverty, and intimate partner violence.6,19
A concerted and coordinated effort is required in LMICs to achieve the Sustainable Development Goals (SDGs), particularly Goals 3, 4, and 5, with a focus on the sexual and reproductive health and rights of adolescents. Goal 3 specifically aims to ensure healthy lives and promote well-being for all individuals from birth onward. This broad goal encompasses critical health-related targets, including reproductive, maternal, neonatal, child, and adolescent health. 20 Adolescents are disproportionately affected by sexual violence, especially adolescents who live in rural areas and have lower educational levels.21,22 To effectively prevent the risks that expose adolescents to pregnancy and unsafe abortions, interventions must be grounded in reliable evidence. This is essential to achieving Goal 5, which seeks to empower all women and girls and attain gender equality. 23 Adolescent pregnancy is a key issue that the World Health Organization (WHO) is actively addressing. In collaboration with partners, WHO has been raising awareness of the problem, establishing evidence-based actions, developing program tools and supportive policies, building capacity, and assisting countries in tackling adolescent pregnancy. 6 WHO also prioritizes adolescent health by preparing guidelines, expanding comprehensive sexuality education, and emphasizing sexual and reproductive health research for the coming years to prevent adolescent pregnancy and its associated consequences. 24 Furthermore, providing comprehensive sexuality education to all young people, especially adolescent girls and young women, is crucial for preventing unintended pregnancies. 23
Adolescent girls aged 10 to 19 have a significantly higher proportion of unmet needs related to pregnancy prevention compared to all women of reproductive age. 5 They also face unmet needs in sexuality education and have limited access to desired healthcare services. These factors increase their vulnerability to child marriage and adolescent pregnancy.5,25 Reducing adolescent pregnancies and preventing pregnancy-related mortality and morbidity are essential for achieving the SDGs concerning maternal and newborn health, as well as for promoting optimal health outcomes throughout life. 6
Early marriage, poverty, social norms, cultural beliefs, and lack of education contribute to the high prevalence of adolescent pregnancy.26,27 It is essential to break the cycle of adolescent pregnancies by empowering girls with access to accurate information, enabling them to make informed decisions about when to have children and their reproductive futures. However, there is limited evidence regarding global and regional coverage, as well as the factors contributing to adolescent pregnancy. Identifying the magnitude, understanding the contributing factors, and developing prevention strategies for adolescent pregnancy are crucial. To support young mothers and prevent future adolescent pregnancies by addressing these contributing factors, this study aimed to assess the proportion and associated factors of adolescent pregnancy in LMICs, as well as to pinpoint target areas for intervention. Our study provides nuanced, policy-relevant evidence by focusing on demographic and health survey (DHS)-participating LMICs.
Methods and materials
Study area and data source
A community-based cross-sectional study design was employed. Data were obtained from six WHO regions, as stated in Table 1, classified according to the DHS, encompassing LMICs from 2015 to 2024. A total of 47 eligible countries were selected for analysis. When more than two standard DHS datasets were available after 2015, the most recent dataset was used. The surveys used a multistage cluster sample and were created to collect and present data on demographic and key health indicators. The DHS program utilizes standardized model questionnaires that are developed through a rigorous protocol. According to the guidelines provided in the DHS record manuals (DHS-7 and DHS-8), the women’s questionnaire is reviewed by a technical advisory group. It is then adapted to fit the local context, translated, and must undergo pre-testing in the field to ensure its validity and reliability before the main survey.28,29 Each survey employed a cross-sectional study design, collecting data on both the independent and outcome variables simultaneously. LMICs represent diverse nations and are categorized as low-income, lower-middle-income, and upper-middle-income countries, based on the World Bank’s 2025 classification. The analysis included 13 low-income, 26 lower-middle-income, and 8 upper-middle-income countries. 30 Among these, 28 countries were from sub-Saharan Africa (SSA), 11 countries from South and Southeast Asia, 4 countries from North Africa/West Asia/Europe, 2 countries from Latin America and the Caribbean, and 1 country each from Central Asia and Oceania. The data were accessed online via the link https://dhsprogram.com/data/dataset_admin/index.cfm after a formal request.
The weighted frequencies of the surveys for the study of adolescent pregnancy in 47 low- and middle-income countries, demographic and health surveys from 2015 to 2024.

LMICs: Low- and middle-income countries.
To ensure consistency across countries and survey rounds, adolescent pregnancy and its associated reproductive, demographic, and socioeconomic factors were assessed and classified using the standard DHS definitions and coding from the DHS7 and DHS8 Recode Manuals.28,29
Population
The target population comprised all adolescent girls aged 15 to 19 in LMICs, while the study population included all adolescent girls aged 15 to 19 in 47 selected LMICs.
Inclusion criteria and exclusion criteria
This study included all recorded adolescent girls aged 15 to 19 in the selected LMICs. Participants with missing or unknown values for adolescent birth, history of termination, or pregnancy within 5 years of data collection in the given age range were excluded.
Sample size determination and sampling procedure
Since this study was based on secondary data, we did not calculate the sample size. The sample includes all recorded adolescent girls who gave birth, had a history of terminated pregnancy, or were pregnant before age 20 within 5 years of data collection. Therefore, according to Table 1, the current study involved 327,394 participants, which, after weighting, was adjusted to 323,767. Of these, 45.86% were from India (weighted). The countries’ sample sizes, which constitute the overall sample size, are presented in Table 1.
Study variables
Dependent variable: Adolescent pregnancy, also known as teenage pregnancy, is an individual giving birth before the age of 20 years. 11 It is based on self-reported birth history and is categorized as yes (coded 1) if the aggregate of v212 (age at first birth), v213 (currently pregnant), an v228 (history of terminated pregnancy) had codes of an adolescent who gave birth, had a history of terminated pregnancy, or was pregnant during and/or within 5 years of data collection, and no (coded 0) otherwise. Adolescent pregnancy in DHS is assessed through self-reported reproductive histories, including age at first birth (v212), current pregnancy status (v213), and terminated pregnancies (v228). While DHS applies standard and widely accepted data collection methods, measures could be susceptible to reporting bias. Where early marriage is legally prohibited, reporters might over-report their age at marriage or first birth. Also, within settings where pregnancy during adolescence is being stigmatized, there may be unrecorded or underreported pregnancies that end in unsafe abortion.
Independent variables
Individual-level factors: Assessed for their association with the outcome variable included the respondent’s educational attainment (no education, primary, secondary, and above), wealth index (poor, middle, rich), respondent’s age (15–17, 18–19), sex of household head (male, female), condom use (yes, no), contraceptive use (yes, no), mobile phone ownership (has, does not have), bank account ownership (has, does not have), and knowledge of contraception methods (knows, no knowledge).
Community-level variables included WHO region (North Africa/West Asia/Europe, SSA, Central Asia, South and Southeast Asia, Oceania, Latin America, and the Caribbean), residence (urban or rural), and media exposure (none or media exposure).
Data collection procedure and quality
Data collection procedure
The research utilized data from the DHS, collected using a standardized women’s questionnaire that included multiple sections, some of which were specifically tailored for women and households. Trained data collectors conducted face-to-face interviews at participants’ homes with eligible women aged 15 to 19 who had given birth within the past 5 years. The questionnaire included women’s health characteristics within sociodemographic, socioeconomic, and pregnancy-related contexts. 31
Data quality control
The goal of the DHS is to generate high-quality, easily accessible data consistently and systematically. However, national surveys in developing countries often encounter issues such as omitted or partially reported responses. Additionally, complex questions frequently yield inconsistent answers, resulting in incomplete or unreliable datasets that complicate analysis. 32 To address these challenges, the DHS employs editing and imputation techniques to ensure the dataset is suitable for research and accurately represents the population.32,33
Data management, processing, and analysis
The data extracted from DHS datasets, available online, were collected from 47 LMICs between 2015 and 2024. The data were cleaned, recoded, and analyzed using STATA version 17. Following the survey report’s recommendations, the data were weighted for sampling probabilities and non-response using the weighting factor to restore representativeness and produce reliable statistical estimates before analysis. All analyses applied DHS sample weights (v005) and cluster numbers (v001) to account for the complex survey design. Consequently, the proportions reported represent nationally weighted estimates for female adolescents. Multicollinearity was validated for independent variables and assessed using variance inflation factors (VIFs), revealing no significant issues. Bivariable multilevel logistic regression analyses with a p-value < 0.20 were included in the final model. Multivariable multilevel logistic regression was employed for the outcome variable. The p-values less than 0.05 were considered statistically significant, and adjusted odds ratios (AORs) with 95% CIs were calculated from the final model. These AORs and their 95% CIs served as measures of association in the full model, which examined the relationship between adolescent pregnancy and independent factors at individual and community levels. Assumptions of chi-square tests were validated and fulfilled.
We obtained statistically accurate estimates of the regression coefficients by incorporating clustering information. Before appending the datasets, cluster numbers were recoded sequentially, starting from one, to prevent overlapping of cluster identifiers across multiple countries. Therefore, a multilevel analysis was performed to estimate mixed effects, including fixed effects for predictors at both the individual and community levels, and a random effect to capture variation between clusters. The likelihood ratio test was employed to assess the significance of the random intercept variation. Additionally, the intra-class correlation coefficient (ICC), proportional change in variance (PCV), and median odds ratio (MOR) were used to quantify the variation attributable to the random effects.
To determine the overall variation at each model attributable to individual and/or community-level characteristics, we employed PCV. PCV was calculated using the formula PCV = ((VA−VB)/VA) × 100, where VA represents the variance of the empty model and VB represents the variance of the model with additional components. The candidate model was evaluated using the Deviance Information Criterion (DIC), calculated as deviance = −2 × log-likelihood.
Model building and comparison
Four models incorporating variables of interest were fitted to identify the factors contributing to adolescent pregnancy. Without explanatory variables, the null model was fitted to test for random variation in the intercept and to estimate ICC. The ICC is a measure of variation within a cluster. Model I examined how individual-level characteristics affect adolescent pregnancy. Model II analyzed the factors at the community level that influence the outcome. Model III (the full model) analyzed how individual and community-level factors jointly impact the outcome of interest. The PCV, which represents the change in community-level variance between the empty model and subsequent models, and ICC, which indicates the percentage of variance explained by the higher level, were reported as measures of variation for community-level variables.
Model equation
Let P(Yij = 1) be the probability of adolescent pregnancy for individual I in cluster j. Then, the multilevel logistic regression model can be expressed as:

where Yij is the binary outcome variable (1 if adolescent
Results
Sociodemographic characteristics
Table 2 reveals that a total of 327,394 (weighted 323,767) adolescents were included in the current study. Most participants, 240,321 (74.23%), had secondary education and higher. Nearly two-thirds of respondents, 202,236 (62.46%), had media exposure; they were exposed to media at least once a week (radio, newspapers, or television). Out of all participants, two-fifths, 131,309 (40.56%), of women had poor wealth status. Among all study participants, nearly two-thirds, 205,823 (63.57%), were rural dwellers. Almost three-fifths, 185,829 (57.40%), of women were from the South and Southeast Asian region (see Table 2)
Sociodemographic characteristics of adolescent age (15–19 years) women who experienced adolescent pregnancy: evidence from recent surveys in low- and middle-income countries demographic health surveys from 2015 to 2024.

The magnitude of adolescent pregnancy
The pooled proportion of adolescent pregnancy is 23% (20–26%). Across regions, it ranges from 10% (6–14%) in North Africa/West Asia/Europe to 28% (25–32%) in SSA. The proportion across countries also ranges from 4% (3–5%) in the Maldives to 45% (43–47%) in Mali (see Figure 1).
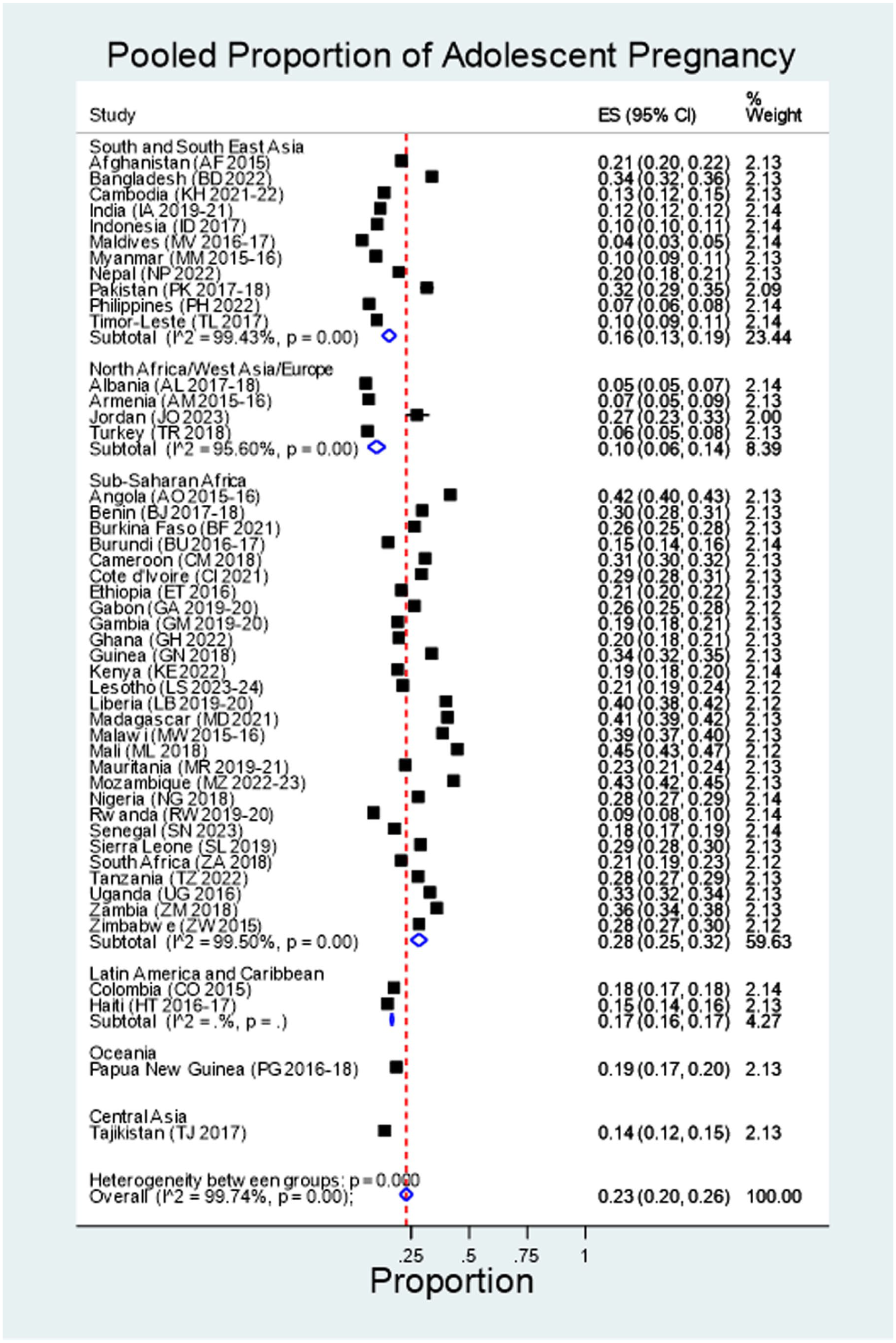
The pooled proportion of adolescent pregnancy in 47 low- and middle-income countries, as evidenced from DHS 2015–2024.
The prevalence of adolescent pregnancy in several countries which have higher than 30% was as follows, as shown in Figure 1, Mali (45%), Mozambique (43%), Angola (42%), Madagascar (41%), Liberia (40%), Malawi (39%), Zambia (36%), Bangladesh (34%), Guinea (34%), Uganda (33%), Pakistan (32%), Cameroon (31%), Benin (30%), Cote d’Ivoire (29%), Sierra Leone (29%), Nigeria (28%), Tanzania (28%), Zimbabwe (28%), and Jordan 27%. There are also countries with a proportion of 10% or less: the Maldives (4%), Albania (5%), Turkey (6%), Armenia (7%), the Philippines (7%), and Rwanda (9%), Indonesia (10%), Myanmar (10%), and Timor-Leste (10%).
Factors associated with adolescent pregnancy
With a p-value of less than 0.2 in the bivariable analysis, all variables for both (individual and community level) factors were included in the multivariable multilevel analysis. In the final model, both the individual-and community-level factors were included simultaneously; women’s education, respondent’s age, household wealth index, sex of household head, contraceptive use, condom use, marital status, having a bank account, and knowledge of contraception were individual-level factors significantly associated with adolescent pregnancy.
Table 3 shows that women who had no formal education increased the likelihood of adolescent pregnancy 1.10 times (AOR = 1.10, 95% CI: [1.04, 1.16]), while women who had primary education increased the likelihood of adolescent pregnancy by 58% (AOR = 1.58, 95% CI: [1.51, 1.66]) compared with women who had secondary and higher education. The odds of adolescent pregnancy decreased by 17% (AOR = 0.83, 95% CI: [0.80, 0.87]) among women from middle-income families and by 42% (AOR = 0.58, 95% CI: [0.55, 0.61]) among women from wealthy households, compared to those from low-income households. The odds of adolescent pregnancy were increased more than four times (AOR = 4.33, 95% CI: [4.17, 4.49]) among women aged between 18 and 20 compared with those less than 18 years of age. Similarly, the likelihood of adolescent pregnancy was increased by 40% (AOR = 1.40, 95% CI: [1.35, 1.46]) among female household heads. The odds of adolescent pregnancy were reduced by 56% (AOR = 0.44, 95% CI: [0.42, 0.46]) among participants who used contraception, and the likelihood of adolescent pregnancy decreased to 0.38 (AOR = 0.38, 95% CI: [0.35, 0.41]) among individuals who knew contraceptive methods. Among condom-using individuals, the odds of adolescent pregnancy decreased by 21% (AOR = 0.79, 95% CI: [0.74, 0.85]). The odds of adolescent pregnancy among married women increased 9 times (AOR = 9.02, 95% CI: [8.91, 9.73]).
Multilevel analysis of factors associated with adolescent pregnancy in adolescent women 15 to 19 years in 47 low- and middle-income countries: based on demographic health surveys from 2015 to 2024.

CI: confidence interval; ICC: intra-class correlation coefficient; MOR: median odds ratio; PCV: proportional change in variance; SSA: sub-Saharan Africa; VIF: variance inflation factors
P-value < 0.05. **P-value < 0.01. ***P-value < 0.001.
Additionally, the likelihood of teenage pregnancy decreased by 11% (AOR = 0.89, 95% CI: [0.83, 0.96]) among women who had bank accounts.
Regarding community-level factors in the final model analysis, the WHO region and media exposure were significant predictors of adolescent pregnancy. In the SSA and Central Asia regions, the odds of adolescent pregnancy were 8.79 times (AOR = 8.79, 95% CI: [6.96, 10.24]) and 2.96 times (AOR = 2.96, 95% CI: [2.16, 3.67]) higher, respectively, compared to the North Africa/West Asia/Europe region. Likewise, the likelihood of adolescent pregnancy rose by 1.65 times (AOR = 1.65, 95% CI: [1.35, 2.03]) in South and Southeast Asia, and by 4.11 times (AOR = 4.11, 95% CI: [2.66, 5.01]) in Oceania, relative to the North Africa/West Asia/Europe region.
The likelihood of adolescent pregnancy was 5.83 times (AOR = 5.83, 95% CI: [4.93, 6.49]) in Latin America and the Caribbean region. Among individuals who had media exposure, the likelihood of adolescent pregnancy was decreased to 14% (AOR = 0.86, 95% CI: [0.83, 0.89]) compared with those who had not.
Random effects and model comparison
According to Table 3, in the empty model, the intra-enumeration area correlation coefficient (ICC) revealed that variations between cluster areas account for 30.21% (ICC = 0.3020569) of the overall variation in adolescent pregnancy, with individual differences accounting for the remaining 69.79% of the variability. In the final model (Model III), the total variation in adolescent pregnancy at the cluster level was reduced to 25.33% (ICC = 0.2533126) and may be attributable to other unobserved community-level factors. Model fitness was compared using deviance, and the model with the lowest deviance (Model III) was considered the best-fitting model. The final model (Model III), which has the lowest deviance value of 932.436 compared to the other models, is utilized to determine significant factors associated with adolescent pregnancy among mothers aged 15 to 19 in the DHS data from 47 LMICs. The effects of community heterogeneity were also minimal, as evidenced by the lowest MOR value of Model III (2.97), which was lower than the MOR of the null model (3.12). According to the PCV, the complete model, which incorporated factors at both the individual and community levels, accounted for 25.34% of the differences in adolescent pregnancy across communities. Additionally, the average VIF across all models was very low (<10), indicating that there was no multicollinearity among the predictor variables (see Table 3).
Discussion
Adolescent pregnancy remains a significant global public health issue. Approximately 21 million girls aged 15 to 19 become pregnant every year, with nearly half of these pregnancies being unintended. More than half (55%) of unintended pregnancies end in abortion. 5
The pooled proportion of adolescent pregnancy among all adolescent girls in 47 LMICs was 23% (95% CI: [20, 26]) with
Previous evidence indicates that child marriage rates in most SSA countries were higher,37,38 which might contribute to the increased prevalence of adolescent pregnancy in the region. Child marriage in countries such as Cote d’Ivoire, Guinea, Liberia, Mali, Mauritania, Nigeria, Sierra Leone, Uganda, and most SSA countries continues to be high.39,40 According to the findings of this study, which was supported by other studies, 41 married adolescents were nine times more likely to be pregnant compared to unmarried ones. Modern contraceptive coverage in SSA countries is still extremely low, 42 and some studies revealed that in most countries in the region, adolescent women have unmet needs for contraception.43,44 Additionally, this study included all adolescent girls who had a birth, a history of terminated pregnancy, or who were pregnant during data collection, which could contribute to the increased reported rates of adolescent pregnancy. However, underreporting of terminated pregnancy and over-reporting of age at first marriage for various reasons are still possible in the majority of restrictive settings. 45 In Bangladesh, Pakistan, and Jordan, the individual record datasets included only ever-married women, unlike in other countries. This could contribute to the increased adolescent pregnancy rate. In South Asia, perspectives on gender have mostly stayed unchanged. In most developing countries, a lack of awareness among adolescents about sexual and reproductive health, social and cultural influences, family beliefs, and low educational and financial status remain significant drivers of adolescent pregnancy. 34 Despite improvements in social indicators, gender inequality continues to be an important concern in South Asia, 46 which may contribute to the substantially higher prevalence of adolescent pregnancy in these countries. Studies in Bangladesh and South Asia revealed a significantly high rate of adolescent marriage,47,48 which could be linked to the increased prevalence of adolescent pregnancy. In Pakistan, earlier studies showed that adolescent births accounted for 42.5%, 49 and family planning coverage was below 50%. 50 This low contraceptive utilization indicates an unmet need for such services among women, particularly adolescents. In Jordan, the higher prevalence of adolescent pregnancy may be attributed to the inclusion of refugees in the data, whether formally residing in refugee camps or informally living in communities outside camps. 51
It was 10% or less in some countries, such as the Maldives, Albania, Armenia, Turkey, the Philippines, Rwanda, Indonesia, Myanmar, and Timor-Leste. An explanation for the lower proportion in these countries might be the inclusion of all unmarried and ever-married adolescents. This proportion is also likely linked to stronger investments in education, reproductive health services, and different gender norms. 52 Child marriage in some countries, such as Albania, Rwanda, Turkey, Indonesia, Myanmar, the Philippines, and Timor-Leste, was relatively lower.39,41,48 The increase in women’s ability to choose marriage and make decisions within the family in Albania 52 might contribute to lowering the rate of adolescent births.
The pooled proportion of adolescent pregnancy in the current study was higher than the findings from Ethiopia, Ghana, SSA, and a systematic review of global studies.9,53–55 One possible explanation for this discrepancy is demographic differences. For instance, whereas a previous study was conducted in a single town using a cross-sectional method, our research analyzed combined data from several countries, including some of the most marginalized populations globally. This broader scope may have led to a higher overall rate of adolescent pregnancy in our analysis. Adolescent pregnancy rates are strongly influenced by socioeconomic status and tend to be relatively low in most developed countries.36,56 Conversely, our findings are lower than those reported in studies from East Africa, Ethiopia, Tanzania, and Zambia.56–60 However, some previous studies were based on single cross-sectional designs,58,59 making it difficult to directly compare a single snapshot study with the pooled proportion derived from global data. For example, a study in Ethiopia was conducted in a refugee camp, 60 which may have elevated the prevalence due to higher risks of sexual violence and unmet needs of contraception in such settings.61,62 Furthermore, the East African study used only women who had ever had sex as the denominator, unlike our study, which could have inflated the reported prevalence. 56
Adolescent pregnancy is consistently associated with substantial adverse maternal and neonatal outcomes, and these risks are amplified in LMICs where maternal healthcare services are poor and with considerable disparities across countries.15,63,64 Evidence shows that adolescent mothers face a higher risk of obstetric complications, including hypertensive disorders, anemia,9,65 obstructed or prolonged labor due to cephalo-pelvic disproportion, postpartum hemorrhage, 10 and a greater likelihood of requiring cesarean section (CS) delivery.65–67 CS is a common incidence in adolescents, due to some indications, such as non-reassuring fetal status and labor dystocia. 68 Prolonged or obstructed labor can lead to CS delivery in adolescents. 69 CS delivery is currently on the rise in all parts of the world. 70 Neonatal risks are also elevated, with increased risks of stillbirth, preterm birth,9,65 low birth weight,7,65 birth trauma, 71 and neonatal mortality. 15 Systemic challenges, such as limited access to quality antenatal and intrapartum care and delays in obtaining emergency obstetric services, combined with broader structural and socioeconomic constraints in LMICs, significantly worsen maternal and neonatal outcomes among adolescents.72,73 Recent studies in LMICs reported that adolescents experienced nearly a fourfold higher risk of stillbirth and a twofold increase in neonatal mortality compared to adult mothers. 15 Adolescent pregnancy also leads to higher risks of maternal and neonatal mortality,4,15 a greater likelihood of mental health problems, and constraints for educational and economic prospects, which contribute to cycles of poverty and inequality that can span across generations.6,19 Its impact extends beyond the mother and her child to affect the entire society.11,49
Several socioeconomic and sociodemographic factors were found to be significantly associated with adolescent pregnancy, such as lower educational attainment, being married, the respondent’s age, living in a female-headed household, and WHO regions, which were positively associated with adolescent pregnancy. Conversely, higher wealth index, media exposure, contraceptive use, knowledge of contraception, condom use, and owning a bank account were negatively associated with the outcome. As the education level increased, the likelihood of adolescent pregnancy decreased, and vice versa. This finding aligns with studies conducted in Tanzania, Zambia, and South Asia.57,58,74 Education level is a critical factor influencing adolescent fertility. 75 Findings from a systematic review in LMICs are consistent with our results, showing that higher educational attainment protects adolescents from early pregnancy. 76 Adolescent girls who remain in education longer have a greater chance of delaying pregnancy.49,77 Conversely, lack of formal education, inadequate sexuality education, and limited knowledge significantly increase the risk of unplanned early pregnancy.78,79 This finding aligns with studies conducted in Tanzania, Pakistan, and South Asia, which show that wealth status is significantly associated with adolescent pregnancy.49,57,58,74 LMICs are often characterized by low socio-economic communities. 80 Poverty is a critical factor contributing to adolescent pregnancy, particularly in these countries.77,81 Low educational attainment, unemployment, and poverty often come together. 34 Addressing the impact of poverty and empowering adolescent women are essential strategies to reduce adolescent pregnancy. 82 Similarly, in the current study, having a bank account among adolescents was associated with a decreased likelihood of adolescent pregnancy. Apart from DHS data, no other studies have examined this variable. Beyond reducing the risk of early motherhood, economic empowerment opportunities can positively influence their lives. 11
Consistent with our findings, studies conducted in Zambia have shown that women with regular access to media have lower odds of adolescent pregnancy. 57 Media access is an effective tool for reducing adolescent pregnancy, 83 as it facilitates sexuality and reproductive health education, enabling young women to protect themselves from risky behaviors. 57 Adolescents exposed to important information about adolescent pregnancy are better equipped to prevent unplanned pregnancies at an early age.84,85 The media serves as a powerful tool for promoting sexual and reproductive health, significantly influencing adolescents’ health behaviors.86–88 However, excessive exposure to social media can increase risky sexual behavior, leading to a higher incidence of unwanted pregnancies among adolescents. 89 In today’s digital world, adolescents must be selective about the information they consume and actively engage in sexual and reproductive education. Media can provide adolescents with valuable information about contraceptive use, thereby enhancing their utilization of effective contraceptive methods. 84
Place of residence was not a significant factor in the outcome of interest in this study. However, findings from previous studies conducted in Pakistan, Ghana, LMICs, and other regions, rural residency increased the likelihood of adolescent pregnancy.2,49,81,90 Similarly, individuals residing in rural areas are more likely to face poverty and lack of formal education among adolescents and their parents, which may increase the likelihood of pregnancy. 91 However, other studies conducted in Uganda and Tanzania have reported findings that urban residency increased the risk of adolescent births.58,92
Contraception offers significant benefits by preventing unintended and unwanted pregnancies. This, in turn, reduces adverse perinatal outcomes, including maternal deaths and neonatal complications.93,94 Contraceptive use can also decrease the likelihood of adolescent fertility. 95 These findings are consistent with a systematic review of studies conducted in LMICs and a cross-sectional study done in Cameroon.2,79,82 This may be because adolescents often begin using contraception after becoming pregnant.
Additionally, poverty and limited resources can lead to the unavailability of contraceptives. 34 The availability of contraceptives plays a crucial role in reducing adolescent pregnancy rates. 66 However, availability alone is insufficient to address the issue. Therefore, knowledge of contraceptive use is an additional key predictor. Awareness of modern contraceptive methods increases their utilization, thereby reducing unplanned pregnancies at an early age. 96 Limited knowledge of contraception leads to lower service utilization among adolescents, resulting in unintended pregnancies. Effective knowledge of contraception can mitigate this risk by encouraging the use of available services.97,98 Adolescent women who engage in sexual activity without proper information or access to contraception face a higher likelihood of pregnancy. 11 Physical, psychological, and social unmet needs, including unmet contraceptive needs, are particularly high in the developing world. Unmet contraceptive needs are a significant factor in LMICs.78,99 Reports indicate a substantial gap between the demand for contraception and actual access in these regions. Addressing the unmet contraceptive needs of all women in LMICs could reduce unintended pregnancies by more than two-thirds and decrease unsafe abortions by 72%. 5 Condom use is associated with a lower likelihood of adolescent fertility. Promoting correct condom use and dual protection, preventing both sexually transmitted infections and pregnancy, is an important strategy.100,101 Condoms are an effective method to avoid adolescent conception, and ensuring private access to condoms may improve their utilization and consequently reduce adolescent fertility.102,103
In our study, marital status emerged as a significant predictor of early childbearing, consistent with research conducted in Uganda, Ethiopia, and Nigeria.59,92,104 The findings of a systematic review and meta-analysis in Africa support our results. 53 Additionally, increasing age was a strong predictor of adolescent pregnancy in this study. Adolescents aged 18 or older were more likely to experience an adolescent pregnancy compared to those younger than 18 years. Studies from Ethiopia and Uganda corroborate these findings.59,92 This association may be explained by the fact that, in our study, 84% of married adolescents were 18 or older. Married adolescents have a higher likelihood of pregnancy due to increased exposure to sexual intercourse.
The sex of the household head is another significant factor in the current study. Living in a female-headed household increased the likelihood of adolescent pregnancy. This finding aligns with a study done in Malawi, 105 which may be attributed to the fact that female-headed households often face poverty. Additionally, women in these households typically spend most of their time caring for their children.106,107 They may be less educated, and less educated women residing in rural areas may have restricted decision-making autonomy, 108 which could limit their life choices and could increase their vulnerability to child marriage and early pregnancy. However, this finding contradicts the findings of a study conducted in SSA. 90 A possible explanation is that adolescents living in male-headed households are more likely to be married.
Regarding WHO regions, all regions were found to have a higher likelihood of adolescent pregnancy compared to North Africa/West Asia/Europe. Most of the countries in those regions are low- and lower-middle-income countries, which were included in the current study, unlike the reference region, from which upper-middle-income countries were included. 30
Limitations of the study
Even though DHS data from 47 middle- and low-income countries provide a large, nationally representative, and standardized dataset that enables strong cross-country comparisons, the data used to determine adolescent pregnancy are based on self-reported reproductive histories, which are susceptible to recall bias, over-reporting of age at first birth in contexts where underreporting in restricted settings where adolescent pregnancy is stigmatized or leads to unsafe or illegal abortion. These factors likely decrease the report of adolescent pregnancy. The cross-sectional nature of the surveys limits causal inference, and these factors may result in underestimation or misclassification. Since we used secondary data, some important variables could not be included due to their absence or missing values, such as unmet needs for contraception, partners’ education, age at marriage, and other behavioral factors. Another limitation involves using combined data from 47 LMICs, which poses challenges due to significant regional and sociocultural variations, as reflected by the high heterogeneity (
Conclusion and recommendations
The pooled proportion of adolescent pregnancy is high in the study area with significant variability. The findings indicate that LMICs require a strong commitment to reduce this proportion to an acceptable level. Given the well-documented significant impact of adolescent pregnancy on maternal and child health, addressing this issue in developing countries demands careful attention. Factors positively associated with adolescent pregnancy include lower educational attainment, being married, and age under 18 years, living in female-headed households, and specific WHO regions. Conversely, a higher wealth index, media exposure, contraceptive use, condom use, knowledge of contraception, and owning a bank account are negatively associated with adolescent pregnancy.
Enhancing women’s education, increasing media exposure, improving knowledge and access to contraception, and promoting financial support for adolescent girls are identified as key modifiable factors to reduce adolescent pregnancy. The WHO regions, such as SSA, South and Southeast Asia, require urgent action to lower adolescent pregnancy rates. Significant efforts are essential to achieve the health-related SDGs by 2030. Countries including Mali, Mozambique, Angola, Madagascar, Liberia, Malawi, Zambia, Guinea, Uganda, Cameroon, Benin, Côte d’Ivoire, Sierra Leone, Nigeria, Tanzania, and Zimbabwe require particular attention due to their notably high rates of adolescent pregnancy.
To improve these modifiable factors, the involvement of multiple stakeholders is essential. To reduce adolescent pregnancy, the WHO and the health authorities of these LMICs must take immediate action, particularly in countries where rates exceed the pooled average. Nations in SSA and South and Southeast Asia are strongly encouraged to prioritize efforts to combat adolescent pregnancy. Health authorities, healthcare professionals, and educators should emphasize providing comprehensive sexuality and reproductive health education, especially through schools, mainstream media, and various social media platforms. Expanding community access to media and delivering health education to mothers and influential community leaders via targeted campaigns are effective strategies to enhance knowledge and awareness of the risks and consequences of adolescent pregnancy. For researchers, this study offers a valuable resource for conducting implementation research in diverse contexts within this field.
Footnotes
Acknowledgements
The authors thank the DHS program for allowing us to use online data.
Author contributions
MDB led in conceptualization, data cleaning, formal analysis, methodology development, software use, validation, writing, review, and visualization in drafting and revising the original manuscript. TKY, THE, and MG contributed to data cleaning, formal analysis, methodology, software use, manuscript drafting, writing, review, and editing. All authors reviewed and approved the final version of the manuscript.
Ethical considerations
The ICF Institutional Review Board and the health service ethical review committees of the included countries approved data collection for all DHS surveys. The benefits and risks of the surveys were explained to the participants. Before distributing the Women’s Questionnaire, eligible respondents provided written informed consent. For respondents with no formal education or limited literacy, the consent statement was read aloud in the local language by the interviewers, and verbal informed consent was documented by them. For adolescents under 18, DHS obtained written, and verbal informed consent from their legally authorized representatives (parents or guardians). The survey was entirely voluntary. The names and identification numbers of the respondents were not included in the final datasets. Additional ethical approval for this study was not required and was therefore waived/exempted. For additional information about data and ethical standards, visit ![]() .
.
Consent for publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.