
Abstract
We modeled the trajectories of respiratory rate and recovery time among children under 5 years of age admitted to at Arba Minch General Hospital, Southern Ethiopia. A retrospective study design was conducted on 201 patients, and a joint modeling approach was adopted. Results revealed that a higher value of the respiratory rate is associated with a lower hazard of recovery (α = −.067, P-value < .05). Severity of pneumonia, presence of danger signs and presence of hyperactive airway disease (P-value < .05 for each) were the factors associated with the evolution of respiratory rate. Patients with moderate and severe levels of malnutrition had 69% (Adjusted Hazard Ratio (AHR) = 0.31, 95% CI 0.098-0.842) and 97.4% (AHR = 0.026, 95% CI 0.005-0.106) lower hazard of recovery, respectively. Patients with comorbidities and a history of tuberculosis had a 55.9% (AHR = 0.441, 95% CI 0.279-0.689) and 80.2% (AHR = 0.198, 95% CI 0.081-0.418) lower hazard of recovery, respectively.
Introduction
Background
Pneumonia, commonly referred to as inflammation of the parenchymal structures of the alveoli and bronchioles, is the leading cause of sickness and death in children under 5 years of age. 1 In developing countries, respiratory tract diseases cause more than 2 million fatalities annually. 172 people die for every 1000 live births in sub-Saharan African countries, primarily from pneumonia. In Africa, this ranges from 11 000 in Sudan to 162 000 in Nigeria and 32 000 in Ethiopia. 2 In Ethiopia, pneumonia is the most common disease that kills children under 5. Over 40 000 children under 5 die from pneumonia each year in Ethiopia, where it is estimated that 3 370 000 children get the illness each year, accounting for 18% of all causes of death. 3
Despite interventions and sustained efforts by several stakeholders, pneumonia remains the leading cause of illness and mortality among children under 5 in Ethiopia. It accounts for 18.0% of all causes of death and kills over 40 000 children in this age range annually. 4 Pneumonia in children under 5 years old is very common in Ethiopia.4 -6 Additionally, research indicates that pneumonia is the primary cause of death in referral hospitals and accounts for 38.6% of all emergency ward admissions. Pneumonia in children is most frequently caused by viruses (61.4%), followed by bacteria (27.3%). 7
According to reports, the prevalence of pneumonia was considerably greater in the in the Gamo zone, southern Ethiopia.2,4 In addition to addressing risk factors that can be altered to speed recovery, knowing the factors impacting recovery time can aid in prognosticating patients. Although there are several different methods for modeling longitudinal and survival data independently, separate analyses of the repeated measures of longitudinal and time-to-event data may result in biased findings. For such data, joint models are likely to generate reliable and efficient inferences.8,9 In addition, many studies provide insight into the background and clinical predictors of survival of pneumonia patients among children aged under 5 years. 10 These studies did not consider the true and unobserved effects of longitudinal measures, which correlate with time to recovery for under 5 pneumonia patients. Therefore, this study attempted to investigate the factors that jointly affect the change in respiratory rate and time to recovery among under 5 children with severe pneumonia admitted at Arba Minch General Hospital.
Materials and Methods
Study Design and the Data
A hospital-based retrospective study was conducted from January 2020 to January 2023 among under 5 children admitted with Severe Community-Acquired Pneumonia (SCAP). The data used in this study was extracted from the patient’s registration chart and medical cards under follow-up during the study period at Arba Minch General Hospital. A total of 201 children under 5 whose respiratory rate was measured at least 3 times and who had complete medical charts were included in the study. Patients whose medical cards were incomplete and registered during the data collection time were excluded.
Variables Considered
The longitudinal measurement of the respiratory rate (in breaths per minute, or bpm) and the time to recovery (in hours) are the response variables taken into consideration in this study. The respiratory rate was a longitudinal outcome variable measured every 12 hours for every child, and the time to recovery was a survival outcome variable measured in hours. The following explanatory variables are taken into consideration in this study: the child’s sex (male or female), age (in months), residence (rural or urban), weight (in kilograms), degree of malnutrition (none, moderate, or severe), presence of fever (yes, no), co-morbidity (yes, no), malaria (yes, no), anemia (yes, no), vaccination status (vaccinated, not vaccinated), pneumonia severity (severe, not severe), vomiting (present, absent), presence of danger signs at admission (yes, no), history of tuberculosis (yes, no), and presence of hyperactive airway disease (HAAD; yes, no).
Methods of Data Analysis
Joint Model
The joint model comprises 2 interconnected sub-models, referred to as the longitudinal sub-model and the survival sub-model, which were applied as described below.
Longitudinal Sub-Model
A longitudinal study is an observational research design in which the same subject was used to collect many measurements of the same response variable over time. 11 Longitudinal response may arise when measurements are taken on the same subject or when measurements taken are on related subjects. In both cases, the responses are likely to be correlated.12 -15 The linear mixed model (LMM) is a parametric linear model for longitudinal or repeated measurement data that quantify the association between a continuous dependent variable and a large number of predictors. It is a development of the traditional linear regression model, which accounts for both fixed effects and random effects. The fixed effect contains a set of predictors that are constant across individuals or the same for all subjects, whereas the random effect contains subject-specific effects. In LMM, random effects are specific to individual subjects within a population, whereas fixed effect parameters reflect the correlations of the predictors to the dependent variable for the entire population. The random variation in the dependent variable was therefore directly modeled using random effects at various levels. 15 In this study, the dependent variable, respiratory rate, was measured on the same subject at various times with different baseline characteristics. We are interested in examining the relationship between a set of explanatory variables and a longitudinally measured dependent variable. Hence, LMM was utilized to investigate the effect of predictor variables on longitudinal measurements of respiratory rate taken on the same subject at various time points. The longitudinal submodel is provided by equation (1):



Where
Survival Sub-Model
The Cox proportional hazard model, which Cox first proposed, was one of the most widely used categories of regression model employed in survival analysis. Although proportional hazards are the basis of the model, no specific type of probability distribution was assumed for the survival times. As a result, the model is known as a semi-parametric model.
17
A proportional hazards model proposed by Cox assumes that the hazard function


Where,
Joint models are a desirable modeling paradigm that is currently quite popular in the medical and statistical literature for both longitudinal and time-to-event data.18,19 These models are utilized in follow-up studies where interest is in associating a longitudinal response with an event time outcome. Hence, the joint model that links the longitudinal response to the time-to-event process through current value parameterization has the form given in equation (3) 16 :

where
Ethical Approval and Informed Consent
The study was checked and approved by the ethical clearance committee of Arba Minch University, department of statistics. In this regard, the official letter referenced to stat/621/2015 was written to the ethics approval committee at Arba Minch General Hospital. Then, the ethical committee approved the letter and gave permission to collect data from patients’ medical records and to use it in the study. Then, all methods were carried out in accordance with relevant guidelines and regulations. For the purpose of confidentiality, there were no links with individual patients, and all data had no personal identifiers. Therefore, informed consent from the patient has been waived by the Arba Minch General Hospital ethics committee.
Results and Discussion
Descriptive Analysis
Table 1 shows descriptive statistics of baseline characteristics of under-five children with severe community acquired pneumonia (SCAP) patients by survival status. From a total of 201children included in the study, 56.72% were males and the remaining 43.28% were females. Regarding the place of residence, 52.24% were from urban areas and the remaining 47.76% were from rural areas. Regarding the vaccination status, 90.05% of the children were vaccinated. Likewise, among under-five children admitted with severe pneumonia, 68.15% of them had comorbidity and 34.80% had hyperactive airway disease. Regarding the level of malnutrition, 93.53% had normal, 3.48% had moderate malnutrition, and 2.98% had severe malnutrition.
The Baseline Characteristics of Under-Five Children With SCAP Patients at Arba Minch General Hospital From January 1, 2020 to January 30, 2023.

Regarding the presence of danger signs at admission, 8% showed a danger sign, and the remaining 92% did not. Out of 201 total study participants admitted with severe pneumonia, about 175 (87.1%) developed an event (recovered; see Figure 1). The median survival time to recovery was 60 hours. The average respiratory rate was 39.85 bpm with minimum and maximum of 10 and 78 bpm, respectively. The average weight was 9.26 kg, and the average age of children was 15.49 months (See Table 1).

Simple bar chart of survival status of patients.
Furthermore, boxplots and normal Q-Q plots were used to evaluate the normality of the longitudinal measures of respiratory rate (RR). The assumption of normality was met for the respiratory rate measurement data (result not shown here). The respiratory rate (RR) values in the individual profile plot varied over time both within and between individuals (see Figure 2). There appears to be a linear relationship between respiratory rate and follow-up time, as indicated by the horizontal loess smoothing technique, which showed that the mean structure of respiratory rate was almost linear with a decreasing trend over time (see Figure 3).
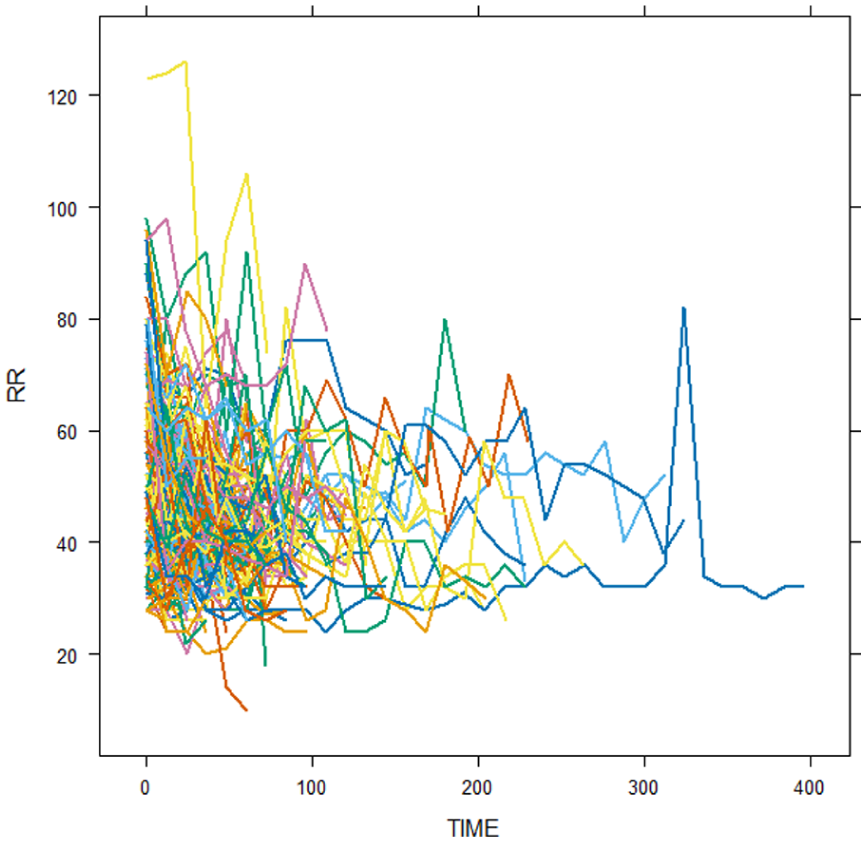
Individual profile plot of respiratory rate (RR) versus follow-up time of pneumonia patients.

The mean profile plot of respiratory rate (RR) versus follow-up time of pneumonia patients.
Joint Modeling of Longitudinal and Time to Event Outcomes
Initially, the longitudinal measurement of the respiratory rate and survival outcome time to recovery were separately modeled using a linear mixed model and the Cox proportional hazard model. This led to the fitting and comparison of a linear mixed-effect model with random intercept, random slope, and random intercept and slope. Therefore, the linear mixed-effect model with a random intercept and slope was selected as the parsimonious model to fit the data on the longitudinal change of respiratory rate (see Table 2) because it had lower values of
Selection of Random Effect in the Linear Mixed Effect Model.

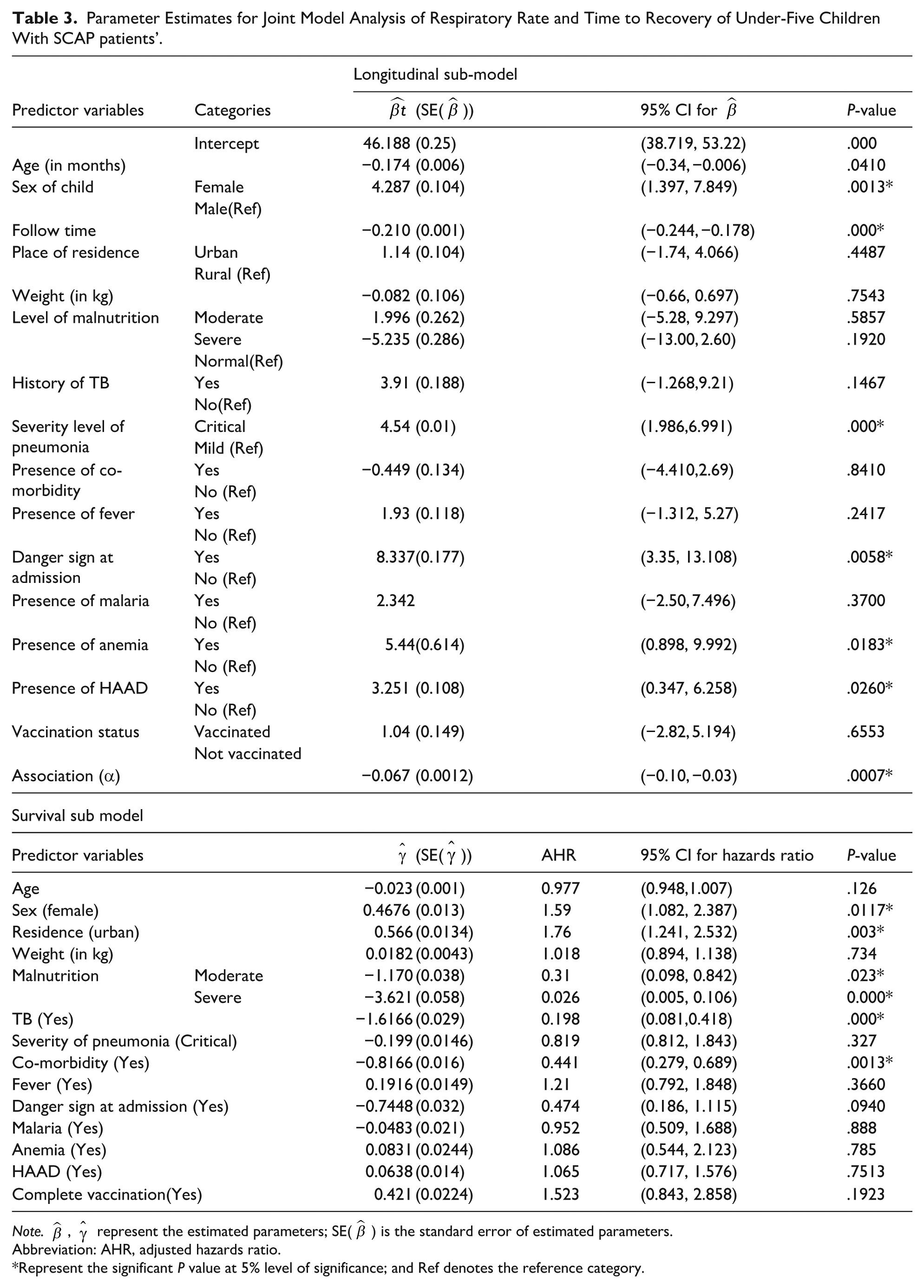
A proportional hazard assumption was also examined for every categorical covariate in the Cox proportional hazard model. Therefore, all covariates satisfied the proportionality assumption of the Cox model, as indicated by the P-values of each individual covariate and the GLOBAL test statistic being greater than the 5% level of significance (result not shown here). A joint model that connects longitudinally measured respiratory rate to time to recovery was fitted in R software after separate models were developed. The joint model analysis of respiratory rate (RR) and time to recovery for patients with pneumonia at Arba Minch General Hospital is shown in Table 3.
Parameter Estimates for Joint Model Analysis of Respiratory Rate and Time to Recovery of Under-Five Children With SCAP patients’.
Note.
Abbreviation: AHR, adjusted hazards ratio.
Represent the significant P value at 5% level of significance; and Ref denotes the reference category.
The result revealed that the predictors age, sex, follow-up time, level of severity, presence of danger sign, anemic status, and presence of hyperactive airway disease had statistically significant relationships with the average longitudinal change in respiratory rate. Hence, keeping all the predictors constant, as the follow-up time increased by 12 hours, the average longitudinal change in respiratory rate decreased by 0.210. The average longitudinal change of respiratory rate increased by 4.32 for female pneumonia patients compared to males. For patients who had danger signs at admission, the average change in respiratory rate increased by 8.092 compared to patients who had no danger signs. For anemic pneumonia patients, the average longitudinal change of respiratory rate increased by 5.439 as compared with non-anemic patients. For patients who had HAAD, the average longitudinal change in respiratory rate increased by 3.143 compared with patients who had no HAAD. Having critical pneumonia at the baseline increases the average value of respiratory rate by 4.262 compared with those having mild level pneumonia. It was also observed that the estimated association parameter in the joint model was negative and statistically significantly different from zero α = −.067, P-value < .05). This shows that the higher respiratory rate slows the hazard of recovery of under-five children with severe community acquired pneumonia (SCAP).
It was also observed that the sex, place of residence, status of malnutrition, history of tuberculosis (TB), level of severity, and comorbidity status had statistically significant associations with the time to recovery of patients. Hence, the estimated hazard ratio of female patients relative to males was 1.59 (AHR = 1.59, 95% CI 1.082-2.387) which indicates that female patients were 1.59 times more likely to recover than male patients. The hazard ratio of place of residence 1.76 (AHR = 1.76, 95% CI 1.241-2.532) indicates that the patients from urban areas were about 1.76 times more likely to experience the event of recovery than rural. The hazard ratio of 0.31 with 95% CI of 0.098-0.842 and 0.026 with 95% CI of 0.005-0.106 for level of malnutrition indicates that those patients who had moderate and severe malnutrition had 69% and 97.4% lower hazards of recovery than those patients who did not had malnutrition, respectively. Likewise, patients with comorbidities and a history of TB had 55.9% (AHR = 0.441, 95% CI 0.279-0.689) and 80.2% (AHR = 0.198, 95% CI 0.081-0.418) lower hazards of recovery, respectively.
Discussion
Severe community-acquired pneumonia is a leading cause of illness and death in children under five. 2 This study adopted a joint model, which combines the linear mixed effect model for respiratory rate (RR) with the Cox model for time to recovery. This study found that the median recovery period for pneumonia was 60 hours (2.5 days) and the mean recovery time was 73.14 hours, which is shorter compared to studies.1,20,21 However, the recovery time was similar to that reported in Ref., 22 but longer than in Ref. 23 Approximately 87.1% of the patients recovered from severe community-acquired pneumonia (SCAP). The differences in recovery times may be attributed to various factors such as the variables used in the study, the location of the hospital, and the level of awareness about pneumonia.
The study found that the follow-up time for pneumonia patients had a negative association with the average longitudinal change in respiratory rate (RR), which aligns with previous research. 1 The estimated association parameter in the joint model was −0.067, indicating a statistically significant negative relationship between the longitudinal biomarker, respiratory rate, and time to recovery. This was consistent with the results of the studies done by Refs.1,24 Pneumonia patients with comorbidities were less likely to experience recovery compared to those without co-morbidities, similar to findings.1,22 The hazard ratio for malnutrition showed that patients with moderate or severe malnutrition had longer recovery times compared to those without malnutrition. Place of residence was significantly associated with recovery time of under-five admitted pneumonia patients. This was consistent with results of the study conducted by Refs.1,23 Additionally, patients with tuberculosis (TB) took 1.61 times longer to recover than those without TB. The study also found that for every 1-year increase in the age of pneumonia patients, their respiratory rate (RR) decreased by 0.174, suggesting that older patients experience a decrease in pneumonia severity. This finding is consistent with research by Azmeraw et al and Wootton et al.1,25
Conclusions
The main objective of this study was to identify the determinants that jointly affect longitudinal measurements and time to recovery among those admitted with pneumonia at Arba Minch General Hospital. From a joint model, the estimated association parameter indicated that respiratory rate and the time to recovery were negatively associated, implying higher values of the respiratory rate associated with a worse time to recovery. Moreover, patients who had comorbidity, patients who had a history of TB, and patients with moderate and severe levels of malnutrition were less likely to recover faster than patients who had no comorbidity, history of TB and patients who had no malnutrition, respectively. Therefore, tailored interventions addressing these specific factors could potentially improve patient outcomes. Patients with increased respiratory rates should be closely monitored to ensure vital function disturbances are detected and treated early.
Footnotes
Acknowledgements
We thank the department of statistics at Arba Minch University for providing permission to conduct the study. We are also grateful to Arba Minch General Hospital for their kind cooperation in providing all the data for our study.
Authors Contributions
AAA designed the study, analyzed the data, MAE and BBA supervised data analysis, drafted the manuscript, and critically reviewed the article. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.