
Abstract
This study evaluated the accuracy of a long-wave infrared camera–based nostril temperature flow method for estimating respiratory rate across different breathing patterns. Five participants (four males and one female; aged between their mid-20s and mid-40s) were monitored using five sensors: a long-wave infrared camera, red–green–blue webcam, red–green–blue camera, respiratory belt, and electrocardiogram sensor. Participants performed regular (17–19 breaths per minute), shallow (32–98 breaths per minute), and deep (5–8 breaths per minute) breathing. The long-wave infrared camera demonstrated the highest accuracy among all devices, with mean absolute errors of 0.6 (regular), 2.4 (shallow), and 0 (deep) breaths per minute. The respiratory belt demonstrated similar performance for regular (0.2 breaths per minute) and deep (0 breaths per minute) breathing; however, it exhibited a significantly higher error (26.0 breaths per minute) during shallow breathing. In contrast, the red–green–blue webcam, red–green–blue camera, and electrocardiogram sensor produced higher mean absolute errors during shallow breathing (44.4, 32.4, and 34.2 breaths per minute, respectively). Overall, the long-wave infrared camera consistently outperformed the other modalities across all breathing patterns, particularly excelling in scenarios with extreme respiratory rates. These findings highlight the long-wave infrared camera’s potential for accurate, noncontact respiratory rate monitoring in clinical and remote health settings, particularly where conventional sensors may fail due to motion artifacts or irregular breathing.
Introduction
Respiratory rate (RR) is a vital clinical parameter for monitoring patient health and detecting early signs of respiratory distress, sleep disorders, and cardiorespiratory abnormalities. 1 Accurate RR measurement is therefore considered essential in clinical practice. Although RR is commonly assessed by visually observing chest wall movement, this method is prone to inaccuracy and is limited by the impracticality of long-term, continuous bedside monitoring by medical staff. 2 Electrocardiogram (ECG) sensors can also be used to estimate RR. 3 As respiration influences ECG waveforms, RR can be inferred from breathing-induced waveform alterations. However, this method yields indirect estimations rather than direct measurements and may have limited accuracy.3,4 Conventional red–green–blue (RGB) cameras enable RR estimation either by tracking thoracoabdominal movement using optical flow algorithms 5 or by extracting remote photoplethysmography (rPPG) signals from facial regions. 6 These approaches, however, are highly susceptible to motion artifacts when the patient’s position shifts or when chest movement is obscured by garments such as thick or loose-fitting clothing.7,8
Recent advancements in thermal imaging, particularly the use of long-wave infrared (LWIR) cameras, offer promising alternatives for accurate RR measurement.9–13 LWIR cameras enable contactless, noninvasive monitoring by detecting thermal radiation emitted from the human body, making them well suited for capturing nostril temperature fluctuations associated with respiration. Unlike RGB cameras, LWIR devices perform reliably under low-light conditions and are less affected by clothing coverage or patient movement. 10
In this study, we evaluated the performance of RR measurement using an LWIR camera under varying respiratory conditions, including regular, shallow, and deep breathing. The results were compared with those obtained using an RGB webcam, an RGB camera, a respiratory belt, and an ECG sensor.
Methods
Participants
Five participants (four males and one female), whose ages ranged from their mid-20s to mid-40s, volunteered for this study. They reported no relevant medical history and were not taking any medication at the time of the experiment. This study was conducted at Yeungnam University Hospital in May and September 2025. The participants provided written informed consent for the study and publication of this case report. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was approved for publication by the institutional review board of the Yeungnam University Hospital (Daegu; Number: 2025-03-062; date of approval, 03 April 2025). The reporting of this study conforms to the Case Report (CARE) guidelines. 14
Implemented sensors
Five sensors were employed to estimate RR from synchronized multimodal recordings. Detailed information on each sensor is provided below and summarized in Table 1.
Summary of sensors for measuring the respiratory rate, corresponding measurement principles, key advantages, and limitations.

LWIR: long-wave infrared; RGB: red–green–blue; PPG: photoplethysmography; ECG: electrocardiogram; EDR: ECG-derived respiration; RR: respiratory rate; SNR: signal-to-noise ratio.
LWIR camera (nostril temperature flow measurement). LWIR camera captures thermal variations in the nostril region. Airflow temperature shifts during inhalation (cooler) and exhalation (warmer). These temperature oscillations were extracted after basic denoising, and the peaks corresponding to individual breathing cycles were counted and converted into breaths per minute (bpm).9,15 In this study, the nostril temperature signal was bandpass filtered within 4–150 bpm to ensure accurate estimation across a wide range of RRs.
RGB webcam (rPPG measurement). RGB webcam captures facial images and extracts rPPG signals, which reflect blood volume pulse variations caused by changes in light reflectance from the cheeks and forehead. Respiratory-related oscillations in the rPPG signal were isolated after signal processing and denoising, and the dominant frequency was converted into bpm.16,17 In this study, the combined green-channel intensity from the cheek and forehead regions was bandpass filtered (4–150 bpm) to capture respiration-related fluctuations across a wide frequency range.
RGB camera (thoracoabdominal movement measurement). Thoracoabdominal movement was monitored using an RGB camera that calculated dense optical flow changes within the thoracoabdominal region. The motion signal was extracted, and the peaks in the motion waveform corresponding to breathing cycles were counted and converted into bpm after post-processing.18,19 In this study, the optical flow signal from the thoracoabdominal area, derived using the Kanade–Lucas–Tomasi (KLT) algorithm, 20 was processed using a 4–150 bpm bandpass filter to capture diverse respiratory patterns.
Respiratory belt (pressure flow measurement). Respiratory belt detects pressure changes associated with chest expansion and contraction during breathing. After denoising, the signal peaks corresponding to individual breathing cycles were identified and converted into bpm. 4 In this study, RR signal was estimated using a Vernier Go Direct® Respiration Belt in combination with Vernier Graphical Analysis™ software.
ECG sensor (ECG-derived respiration measurement). ECG-derived respiration (EDR) is calculated using a single-lead ECG sensor. R-peaks were detected, and three respiration-related features were extracted: beat-to-beat QRS amplitude, electrical axis shifts, and R–R interval variability, indicating respiratory sinus arrhythmia. The feature exhibiting the strongest respiratory oscillation was selected, and its dominant frequency was converted into bpm.
Experiment
The experiment was conducted in a patient ward room at a university hospital. During the procedure, room lighting was kept on during daytime to account for the characteristics of the RGB webcam and camera, and the ambient temperature was maintained at approximately 25°C to reflect the operating conditions of the LWIR camera in a typical indoor environment. The participants lay supine on a bed and performed controlled breathing under each of the following conditions: regular, shallow, and deep breathing. Each breathing pattern was tested once, and a 1-min video recording was captured for each case across five participants. All five sensors simultaneously measured the RR during each session. The experimental setup is illustrated in Figure 1, and the model and key specifications of each sensor are listed in Table 2. For ground truth (GT) measurement, RR was independently determined by a trained medical specialist through manual counting of thoracoabdominal excursions.
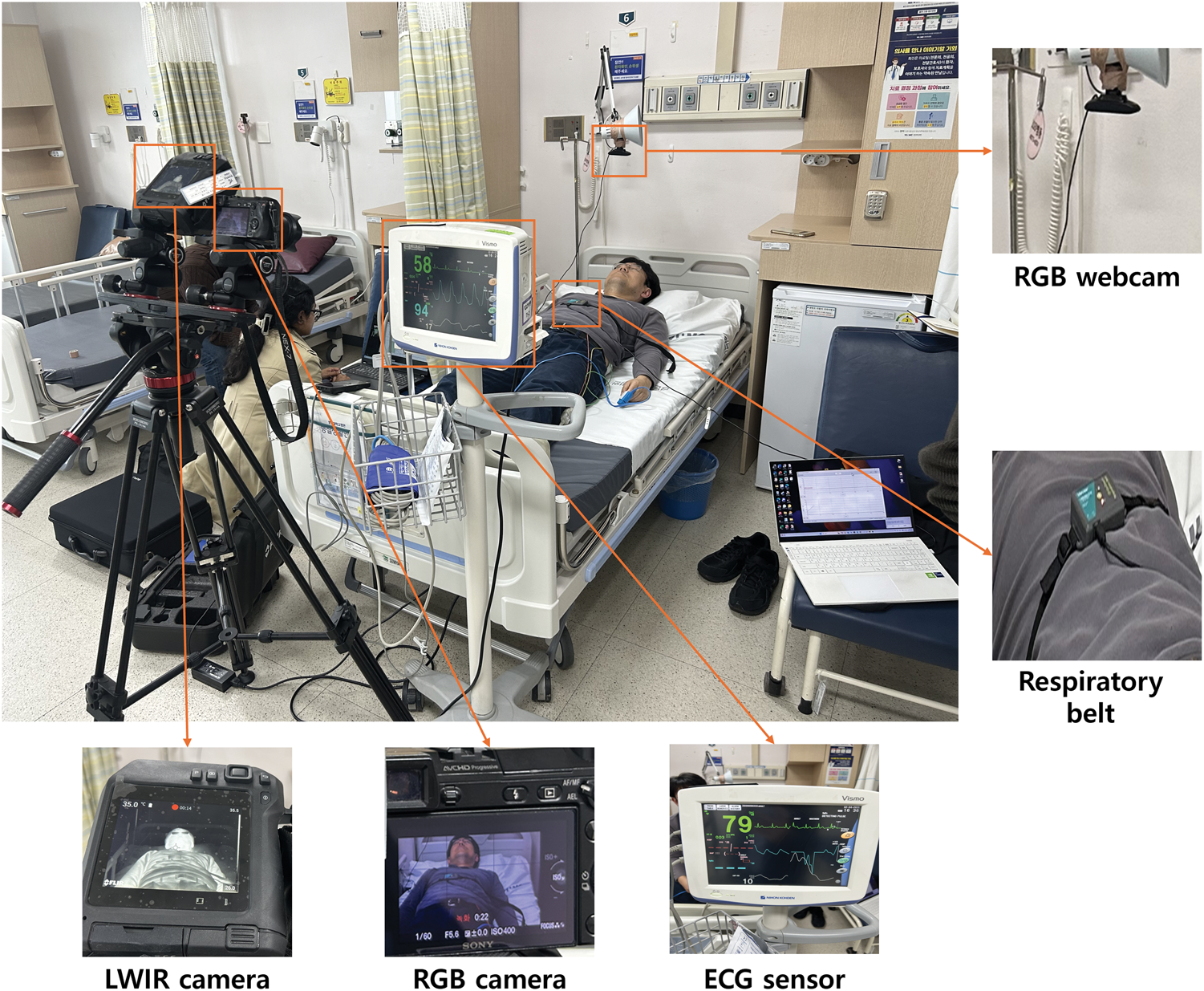
Visualization of the experimental setup and sensor placement. The LWIR camera was positioned to capture the lower face region. The RGB webcam recorded the participant’s face, whereas the RGB camera was directed at the thoracoabdominal region. The respiratory belt was wrapped around the chest, and ECG electrodes were affixed to the chest with an auxiliary sensor placed on the finger. LWIR: long-wave infrared; RGB, red–green–blue; ECG, electrocardiogram.
Devices and key technical specifications used for respiratory rate measurement.

LWIR: long-wave infrared; RGB: red–green–blue; PPG: photoplethysmography; ECG: electrocardiogram; EDR: ECG-derived respiration; VGA: video graphics array; NETD: noise equivalent temperature difference; FHD: full high definition; MP: mega pixel; DFOV: diagonal field of view; BSI-CMOS: back-side illuminated complementary metal-oxide-semiconductor; HDMI: high-definition multimedia interface; EVF: electronic viewfinder; TFT: thin-film transistor; NIBP: noninvasive blood pressure; USB: universal serial bus; SpO2: peripheral oxygen saturation.
The LWIR camera was mounted to capture the lower face, with a focus on the nostril region to monitor the temperature flow, and positioned at a distance of approximately 2 m from the participant’s face. The RGB webcam was placed at approximately 0.5 m facing the participant’s face to acquire rPPG signals. The RGB camera was positioned approximately 2 m away and aimed at the abdomen of the participants to record thoracoabdominal movements. Both RGB sensor–based approaches were conducted at the same resolution (1920 × 1080 pixels) and frame rate (30 frames per sec) to minimize potential bias from camera specifications. The respiratory belt was worn around the chest to monitor thoracic expansion and contraction. Furthermore, ECG signals were obtained using adhesive chest-patch electrodes and a finger-contact sensor, with real-time waveform monitoring on a display unit.
Evaluation metric
The mean absolute error (MAE) was used as the evaluation metric to validate the performance of each sensor. MAE was computed by comparing the RR estimated by each sensor with the GT value obtained through manual counting. For each breathing pattern, MAE was calculated across all the participants as follows:

Results
RR estimates obtained from five sensors were compared with the corresponding GT values across three distinct breathing conditions.
Regular breathing
For regular breathing, the LWIR camera (MAE = 0.6 bpm), respiratory belt (MAE =0.2 bpm), and ECG sensor (MAE =0.6 bpm) closely matched the GT value, demonstrating higher performance than the other sensors. In contrast, the RGB webcam (MAE = 5.2 bpm) and camera (MAE =1.2 bpm) exhibited noticeable deviations from the GT value (Figures 2 and 3; Tables 3 and 4).
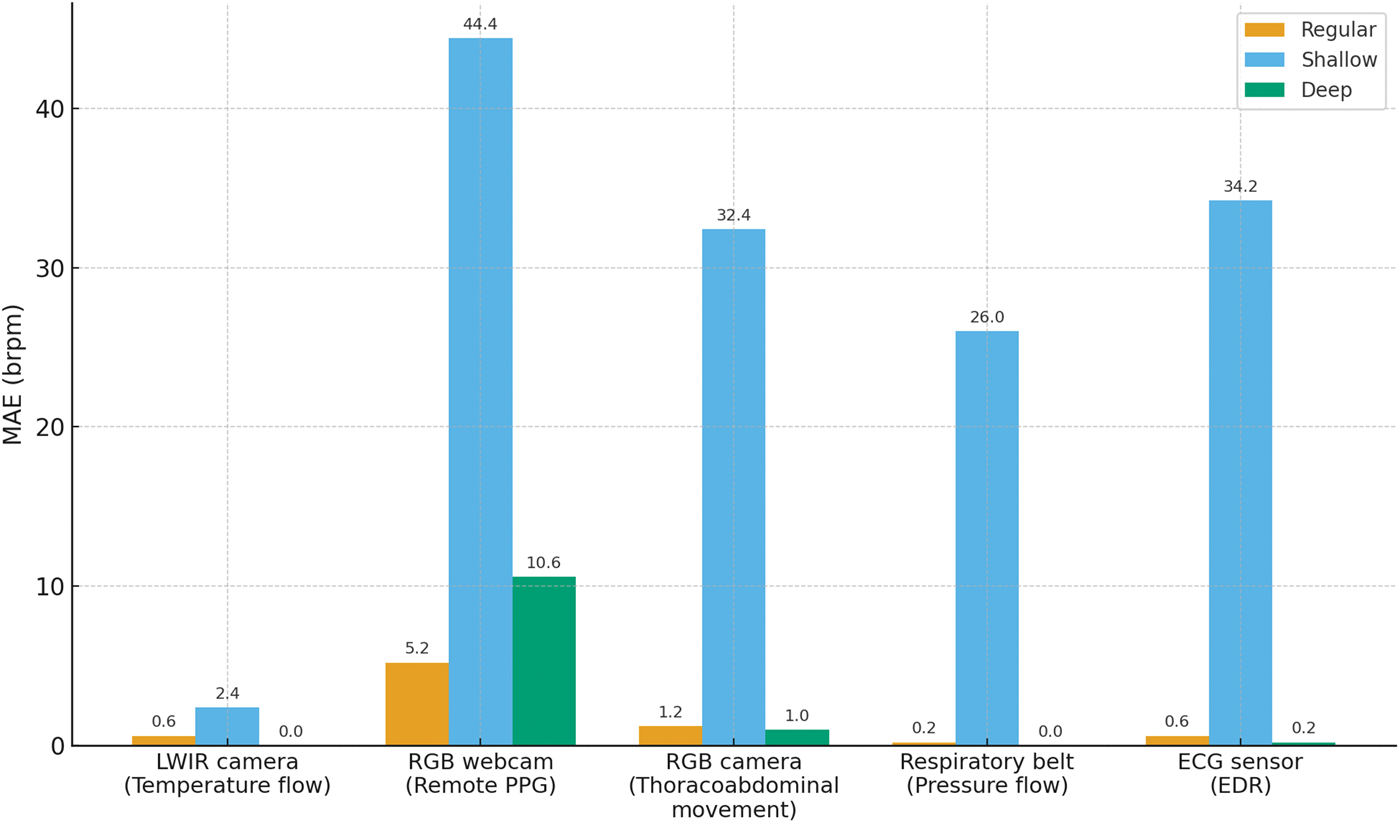
Distribution of MAE across three breathing conditions (regular, shallow, and deep) for all five sensors. The LWIR camera consistently achieved the lowest MAE across all conditions, particularly outperforming the other modalities during shallow breathing. In contrast, the RGB webcam, RGB camera, respiratory belt, and ECG sensor exhibited larger errors for shallow breathing. MAE: mean absolute error; LWIR, long-wave infrared; RGB: red–green–blue; PPG: photoplethysmography; ECG: electrocardiogram sensor (electrocardiogram-derived respiration).

A representative example of the respiratory rate estimation of participant 1 using the LWIR camera for each breathing condition. RR was calculated by counting thermal signal peaks corresponding to exhalation, synchronized with the ground truth value. Valleys indicate inhalation phases. (a) Regular breathing (ground truth RR, 19 bpm; estimated RR with LWIR camera, 19 bpm); (b) shallow breathing (ground truth RR, 98 bpm; estimated RR with LWIR camera, 103 bpm); and (c) deep breathing (ground truth RR, 5 bpm, estimated RR with LWIR camera, 5 bpm). LWIR: long‑wave infrared, RR: respiratory rate.
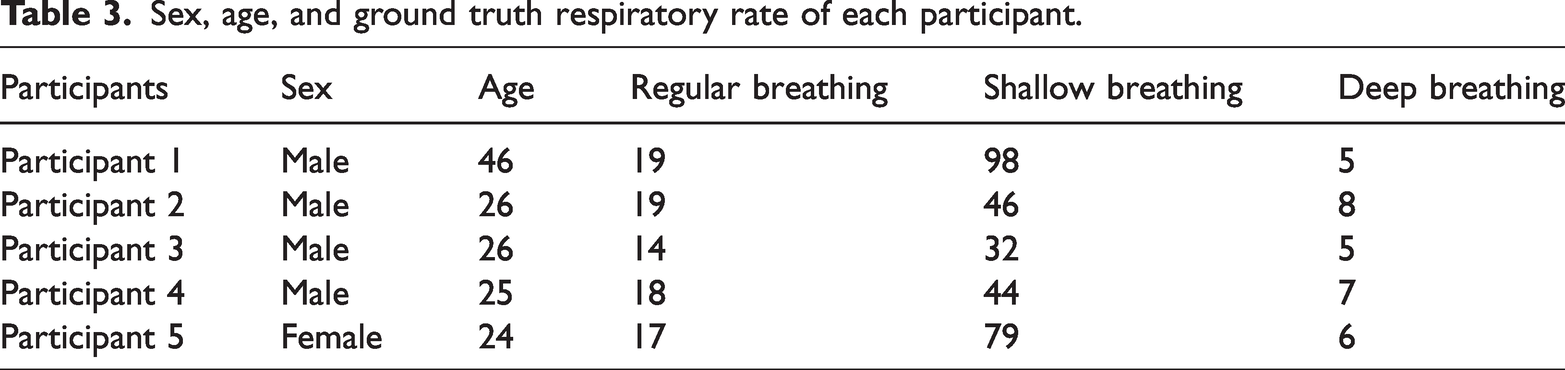
Sex, age, and ground truth respiratory rate of each participant.
Respiratory rate obtained from the five sensors.

LWIR: long-wave infrared; RGB: red–green–blue; PPG: photoplethysmography; ECG: electrocardiogram; EDR: ECG-derived respiration; GT: ground truth; RR: respiratory rate; bpm: breaths per minute; MAE: mean absolute error.
Shallow breathing
For shallow breathing, the LWIR camera again demonstrated a relatively low error (MAE = 2.4 bpm), whereas the RGB webcam (MAE = 44.4 bpm), RGB camera (MAE = 32.4 bpm), respiratory belt (MAE = 26.0 bpm), and ECG sensor (MAE = 34.2 bpm) exhibited considerably higher errors (Figures 2 and 3; Tables 3 and 4).
Deep breathing
For deep breathing, the GT value was 5 bpm. The LWIR camera and respiratory belt achieved perfect agreement with the GT value (MAE = 0 bpm). The RGB camera (MAE = 1.0 bpm) and ECG sensor (MAE = 0.2 bpm) produced comparatively accurate results, whereas the RGB webcam (MAE = 10.6 bpm) exhibited larger deviations (Figures 2 and 3; Tables 3 and 4).
Discussion
In this study, five sensor types, including LWIR camera (nostril temperature flow measurement), RGB webcam (rPPG), RGB camera (thoracoabdominal movement measurement), respiratory belt (pressure flow measurement), and ECG sensor (EDR), were evaluated and compared for their accuracy in measuring RR against GT values. Among these sensors, the LWIR camera demonstrated the highest accuracy across all breathing conditions, including regular, shallow, and deep. It exhibited a distinct thermal contrast suitable for detecting breathing peaks and remained robust to variations in the breathing amplitude and frequency (Figure 3). An additional advantage of the LWIR camera is its ability to detect temperature changes even in low-light conditions. 10 Because the LWIR camera measures RR by capturing thermal fluctuations near the nostrils, it is not affected by clothing coverage, which is common in clinical settings. Although the LWIR camera exhibited a slightly higher error (an MAE of approximately 2 bpm) during shallow breathing, which can be attributed to the diminished thermal contrast between inhalation and exhalation, it still outperformed the other sensors. Given that hospitalized patients often exhibit variable breathing patterns and that hospital rooms are typically dimly lit during nighttime, with patients wearing gowns that may obscure chest movements, the LWIR camera appears particularly well suited for RR monitoring in real-world clinical environments.
In contrast, the remaining four sensors demonstrated reduced accuracy due to their reliance on indirect estimation and susceptibility to motion artifacts. The RGB webcam, which extracts rPPG signals from the facial region, was found to be highly susceptible to patient motion and ambient lighting variations, demonstrating consistently poor performance, particularly during shallow breathing. The RGB camera and respiratory belt failed to accurately detect subtle respiratory activity under similar conditions, as clothing and minimal thoracoabdominal motion obscured the inhalation and exhalation cycles. Similarly, the ECG sensor, which estimates RRs from cardiac-related modulation signals, failed to detect shallow breathing owing to the inadequate amplitude of R-wave modulation. 21
Several recent studies have employed LWIR cameras for measuring RR under diverse environmental conditions and across various health statuses. In 2011, Lewis et al. 9 recorded LWIR videos of 12 healthy adults performing deep, regular, and shallow breathing in the range of 6–47 bpm while seated. The method demonstrated a mean correlation of 0.90–0.98 compared with that in respiratory inductance plethysmography (RIP), validating its accuracy. In 2015, Pereira et al. 10 recorded LWIR videos of 11 healthy adults in static and mild motion states, with RR ranging from 10 to 40 bpm. During static conditions, their method achieved a mean correlation of 0.968 and an MAE of 0.71 bpm compared to those with piezo-plethysmography. Under dynamic conditions, it achieved a mean correlation of 0.94 and an MAE of 0.96 bpm, confirming that LWIR cameras are suitable for RR measurement even in the presence of mild motion. In 2017, Cho et al. 11 recorded LWIR videos of healthy adults breathing at 10–30 bpm in indoor and outdoor environments. Their approach yielded root mean square errors of 0.42–0.525 bpm compared to that in the respiratory belt signal, demonstrating robustness across ambient conditions. In 2023, Maurya et al. 12 used LWIR cameras to monitor 14 adults and 10 neonates in incubators, observing spontaneous RR between 30 and 60 bpm. The MAE ranged from 0.1 to 1.8 bpm in adults and was approximately 1.5 bpm in neonates, using a respiratory belt as the reference, indicating effectiveness across a wide range of age groups. Additionally, Aldred et al. 22 employed LWIR cameras to monitor 136 patients admitted to the emergency room during the coronavirus disease 2019 (COVID-19) pandemic, and the RR GT values of the patients obtained by manual counting ranged from 16 to 40 bpm. Their method achieved a mean correlation of 0.95 compared to the reference values, demonstrating that the LWIR sensor could capture distinct breathing patterns associated with COVID-19 in a clinical setting. In 2024, Mozafari et al. 13 evaluated 22 healthy participants in seated, standing, and masked conditions using LWIR cameras and a deep learning-based framework. With RRs below 42 bpm, MAE ranged from 1.1 to 2.1 bpm compared to that in piezo-plethysmography, indicating reliable performance even with participants wearing surgical masks.
Building on the demonstrated applicability of LWIR cameras for RR extraction, we extended their use to a clinical setting and validated their effectiveness across a broader range of breathing rates, from 5 to 98 bpm, which surpasses the range reported in previous studies. Furthermore, although earlier studies primarily validated RR estimation against one or two reference sensors such as piezo-plethysmography or respiratory belts, the present study conducted a comprehensive comparison involving contact and noncontact sensors: RGB webcam, RGB camera, respiratory belt, and ECG sensor. This extensive validation confirms that LWIR cameras offer the most accurate and robust solution for RR monitoring in real-world clinical environments.
Conclusions
This study demonstrates that the LWIR camera provides more reliable RR estimation than the RGB webcam, RGB camera, respiratory belt, and ECG sensor. Across all breathing conditions, including regular, shallow, and deep, the LWIR camera consistently maintained an MAE below 2.4 bpm, whereas the other sensors exhibited reduced accuracy in at least one breathing condition. Although the results indicate strong potential for use of LWIR cameras in RR monitoring across diverse respiratory patterns, there are some limitations to this study. First, the small sample size and constant ambient temperature of approximately 25°C during data collection may have constrained the system’s performance under variable real-world conditions. Furthermore, when ambient temperature approaches body temperature, the thermal contrast between inhalation and exhalation phases may diminish or even reverse, potentially introducing ambiguity in respiratory phase interpretation. Future research should include a broader cohort, particularly patients with acute respiratory conditions. Additionally, forthcoming studies should evaluate the performance of the LWIR camera under varying ambient illumination to further validate its clinical applicability.
Footnotes
Acknowledgments
None.
Author contributions
Jaeho Kim, Sungho Kim, Sreya Deb Srestha, Uday Debnath, and Min Cheol Chang designed the study, collected and analyzed the data, and drafted the manuscript and substantively revised it. All authors have read and approved the final manuscript.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The authors declare no conflict of interest.
Ethics statement
The participant provided informed consent for the study and for the publication of this case report. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was approved for publication by the institutional review board.
Funding
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. RS-2023-00219725).