
Abstract
Introduction:
Neonatal surgery is complex and time-sensitive, with a narrow margin for error. While neonatal surgical conditions account for approximately 11% of the global disease burden, data on their impact in Ethiopia remains limited.
Methods:
A hospital-based cross-sectional study was conducted at the University of Gondar Comprehensive Specialized Hospital by reviewing medical records of 268 neonates who underwent surgery between 2017 and 2023. Data were analyzed using Stata version 14. Multivariable logistic regression was used to identify predictors of mortality. Statistical significance was set at P < .05.
Results:
The overall mortality rate was 14.18%. Key predictors of mortality included preoperative sepsis (AOR: 4.45; 95% CI: 1.49-13.27), postoperative hypothermia (AOR: 3.19; 95% CI: 1.17-8.71), low birth weight (AOR: 3.7; 95% CI: 1.12-12.43), preterm birth (AOR: 3.88; 95% CI: 1.04-14.46), and prolonged hospital stay (AOR: 3.34; 95% CI: 1.15-9.84). Conversely, neonates aged 9 to 28 days had significantly lower odds of death (AOR: 0.22; 95% CI: 0.05-0.998).
Conclusion:
Neonatal surgical mortality was significantly influenced by preoperative, intraoperative, and postoperative factors. Targeted interventions focusing on infection control, thermal regulation, and care of preterm and low birth weight neonates may improve outcomes.
Introduction
Newborns requiring intensive care are admitted to the neonatal intensive care unit (NICU). The first 28 days of life, known as the neonatal period, are the most critical for a child’s survival. Globally, approximately 2.6 million infants die within their first month, with around 7000 newborn deaths occurring daily, the majority within the first week of life. Neonatal mortality is a major contributor to under-five deaths, and neonatal surgical conditions play a significant role in this mortality. 1
Neonatal surgery encompasses a variety of procedures performed on newborns, depending on the type and severity of the condition. Timely surgical intervention is crucial to prevent progressive organ damage that could occur if treatment is delayed. The majority of neonatal surgeries are performed on an emergency basis due to the urgent nature of these conditions. In Africa, common neonatal surgical conditions include congenital diaphragmatic hernia, anorectal malformations, Hirschsprung’s disease, omphalocele, gastroschisis, esophageal atresia with tracheoesophageal fistula, intestinal atresia, intestinal perforation, and necrotizing enterocolitis. 2
Understanding surgical outcomes is essential for identifying the best evidence to guide patient care. These outcomes also help evaluate the processes that lead to optimal results by critically assessing a procedure’s impact on patient health, well-being, satisfaction, functional status, lifespan, and the healthcare system. Transparent and reproducible outcome measurement is fundamental to assessing surgical performance and perioperative care.3,4 Effective management of neonates with surgical conditions requires a multidisciplinary approach, particularly in postoperative care. 5
In developing countries like Ethiopia, neonatal surgery faces numerous challenges, including late presentation, limited medical facilities, and shortages of healthcare professionals. As a result, neonatal surgical procedures are often associated with unacceptably high rates of morbidity and mortality.5,6 Advances in diagnostic techniques and perioperative care have significantly improved neonatal surgical outcomes. However, a considerable disparity persists between high-income countries and low- and middle-income countries in neonatal surgical outcomes.5 -8
Neonatal surgical conditions are believed to be relatively common, with a significant number of neonates admitted to the NICU requiring surgical intervention. 7 Managing surgical newborns is highly challenging and demands the continuous involvement of skilled neonatologists to achieve favorable outcomes. 9
Despite advancements in postnatal and transitional neonatal care, mortality rates among surgical newborns can exceed 60% in developing countries. Several preoperative, intraoperative, and postoperative factors have been associated with poor survival outcomes in these infants. 10 Neonatal surgical mortality (NSM) is a significant contributor to neonatal mortality. Reported rates of NSM vary geographically, ranging from 4% in the USA, 6% to 7% in Japan, 35% to 45% in India, 52.7% in Uganda, to 62.2% in Nigeria.11,12
This study aims to assess the outcomes of neonatal surgeries and determine factors associated with neonatal surgical mortality at the University of Gondar Comprehensive Specialized Hospital. This may help to prognosticate and stratify patients in different risk groups, and to study the trends in results over time to see if there are any improvements in services.
Objectives
General Objectives
Despite neonatal surgical conditions contributing significantly to global neonatal mortality, their burden in Ethiopia is poorly documented, and there is limited data on outcomes and contributing risk factors in local tertiary care settings. A clear understanding of these outcomes is essential to inform clinical decision-making, guide interventions, and improve survival rates. The aim of this study was to evaluate the outcomes of neonates undergoing surgery and identify factors associated with unfavorable outcomes in newborns admitted to the NICU.
Specific Objectives
✓ To assess the outcomes of neonates who undergo surgery.
✓ To identify factors associated with neonatal surgical outcomes.
Methods and Materials
Study Area
The study was conducted at the University of Gondar Comprehensive Specialized Hospital, a tertiary teaching hospital and one of the oldest healthcare institutions in Ethiopia, established in 1954. The hospital provides a range of health services to the populations of Central, North, and Western Gondar, serving a total of 475 172 people, including 251 466 females and 223 706 males, according to the 2023 Gondar City Administration vital registration data. It is located in the northwest part of Ethiopia, 727 km from Addis Ababa, in the Amhara National Regional State, North Gondar Zone (12.50° N latitude and 37.24° E longitude). The area is situated at an altitude of approximately 2380 m above sea level.
With over 1 million annual patient visits across various clinics, the Pediatrics and Child Health Department serves both rural and urban populations, offering services such as outpatient clinics, an emergency department, a malnutrition ward, the main ward, an infant room, an oncology ward, PICU, and NICU. The neonatal ward of the hospital is a Level III NICU, providing the highest level of care for neonates with a gestational age (GA) of ≥28 weeks. Care is provided by senior pediatricians, pediatric residents, medical interns, and neonatal nurses. On average, the ward admits 300 patients per month. The Surgical Department is also actively involved in providing emergency and elective surgical services. It has 9 operating rooms and approximately 190 beds distributed across various units and wards. The department currently has 35 surgeons, including 12 subspecialists, of whom 2 are pediatric surgeons.
Study Design and Period
Study Design
An institution-based retrospective cross-sectional study was performed by reviewing medical records of neonates who underwent surgery between January 2017 and January 2023.
Study Period
The study was conducted from November1 2023 to January 31 2024
Source Population
Neonates with surgical conditions who were admitted to the NICU at the University Comprehensive Specialized Hospital between January 2017 and January 2023.
Study Population
All neonates who were admitted to the NICU and undergo surgery at university Specialized Hospital between January 2017 and January 2023 (both inborn and outborn neonates who underwent surgery at the University of Gondar Comprehensive Specialized Hospital [UOG]).
Inclusion and Exclusion Criteria
Inclusion Criteria
- Neonates with surgical procedure done from January 2017 to January2023
Exclusion Criteria
- Data with incomplete documentation
Sample Size and Sampling Technique
Sample Size Determination
The primary outcome of interest is poor neonatal surgical outcomes, primarily death. The overall mortality rate for neonates requiring surgical interventions at Tikur Anbessa Referral Hospital was 24.4%. 13 Thus, taking 24.4% of magnitude and P value of .244, the sample size will be as follows.

Where: - n = sample size
Z = standard deviations corresponding to the 95%
Confidence interval = 1.96

Based on the above calculation, the estimated sample size is 283.
Given the estimated sample size of 283 and an expected total population of approximately 5000 neonates over the study period, the sample size was adjusted using the finite population correction formula, resulting in a final sample size of 268. This adjustment was made to maintain statistical validity in a smaller source population.
Study Variables
Dependent Variable
Surgical outcome
Independent Variables
Socio Demographic Characteristics of the Mother and the Newborn
Maternal age
Age and sex of new born
Residence
parity and gravidity
Place of delivery (This variable categorized the location where the delivery occurred, including home, health center, or hospital).
Birth location status (This variable distinguished between neonates born at the study hospital (inborn) and those born elsewhere and referred to the study hospital (outborn)).
Antenatal care (ANC) follow-up
Neonatal Characteristics
Gestational age
Birth weight
Age at the time of surgical intervention
Preoperative Variables
Heart rate, temperature, respiratory rate, presence of sepsis
Intra-Operative and Post-Operative Variables
Duration and site of surgery
Respiratory rate, pulse rate, temperature
Estimated blood loss
Time of initiation of feeding after surgery
Presence of Congenital Surgical Anomaly
Surgical Diagnosis Other Than Anomaly
Operational Definition
Outcome—is defined as:-
Death—neonate died after surgery done Survived—A neonate who underwent surgery and was discharged alive.
Surgical neonate—defined as a neonate who is either:-
(i) Born at 37 weeks of gestation and above (term neonate) and is <29 days at the day of surgery or (ii) Born at <37 weeks of gestation (preterm neonate) and is <29 days at day of surgery
Data Collection Procedure
Data were collected retrospectively from patient records at the University of Gondar Comprehensive Specialized Hospital (UOGCSH) from January 2017 to January 2023. Surgical neonates were identified using operating room and NICU registration logs. Medical records of eligible neonates were reviewed to extract relevant variables using a structured data extraction sheet.
The variables collected included:
Data were collected by trained medical interns and residents using a standardized form. To ensure accuracy, the principal investigator closely monitored data extraction, and records were cross-checked with the hospital’s electronic and paper-based systems. Only neonates with complete data were included in the final analysis.
Data Quality Assurance
To ensure data quality, three medical interns and two pediatric residents received structured training on data abstraction using the standardized form. Data collection was supervised by the principal investigator. Daily meetings were held to review accuracy, resolve inconsistencies, and ensure completeness. A 10% sample of records was re-reviewed to assess inter-rater reliability.
Data Processing and Analysis
Data coding, entering and cleaning was done using the Epidata 4.6 software version. Data were analyzed using Stata version 14. Descriptive statistics were used to summarize the demographic and clinical characteristics of the study population. Continuous variables were reported as means (± standard deviation) or medians (interquartile range), while categorical variables were reported as frequencies and percentages.
To identify factors associated with neonatal surgical mortality, we first performed bivariate logistic regression analysis for each independent variable. Variables with a P-value of <.2 in the bivariate analysis were included in a multivariable logistic regression model to control for potential confounders. Adjusted odds ratios (AOR) with 95% confidence intervals (CI) were reported to quantify the strength of associations.
Potential confounders, such as gestational age, birth weight, sepsis, and postoperative hypothermia, were included in the multivariable model. We assessed multicollinearity among independent variables using the variance inflation factor (VIF), with all values below 5, indicating no significant collinearity. Since the study involved categorical and clinical variables, internal consistency (eg, Cronbach’s alpha) was not applicable. All analyses were performed using Stata version 14.
A P-value of <.05 was considered statistically significant, in line with established conventions in biomedical research. This threshold was chosen to balance the risk of Type I and Type II errors while ensuring the interpretability of our findings within the context of existing literature.
Result
Socio-Demographic Characteristics
A total of 268 neonates who underwent surgery were included in the analysis. The majority of mothers (83.96%) were between the ages of 21 and 34, with a mean maternal age of 27.83 ± 4.66 years. Most mothers (86.94%) had at least one antenatal care (ANC) follow-up visit, and over half of the neonates (56.34%) were from urban settings. Regarding place of delivery, 49.25% delivered in health centers, 43.28% in hospitals, and 7.46% at home as shown in Table 1.
Socio Demographic Characteristics of the Mothers and Surgical Newborns Admitted to NICU.
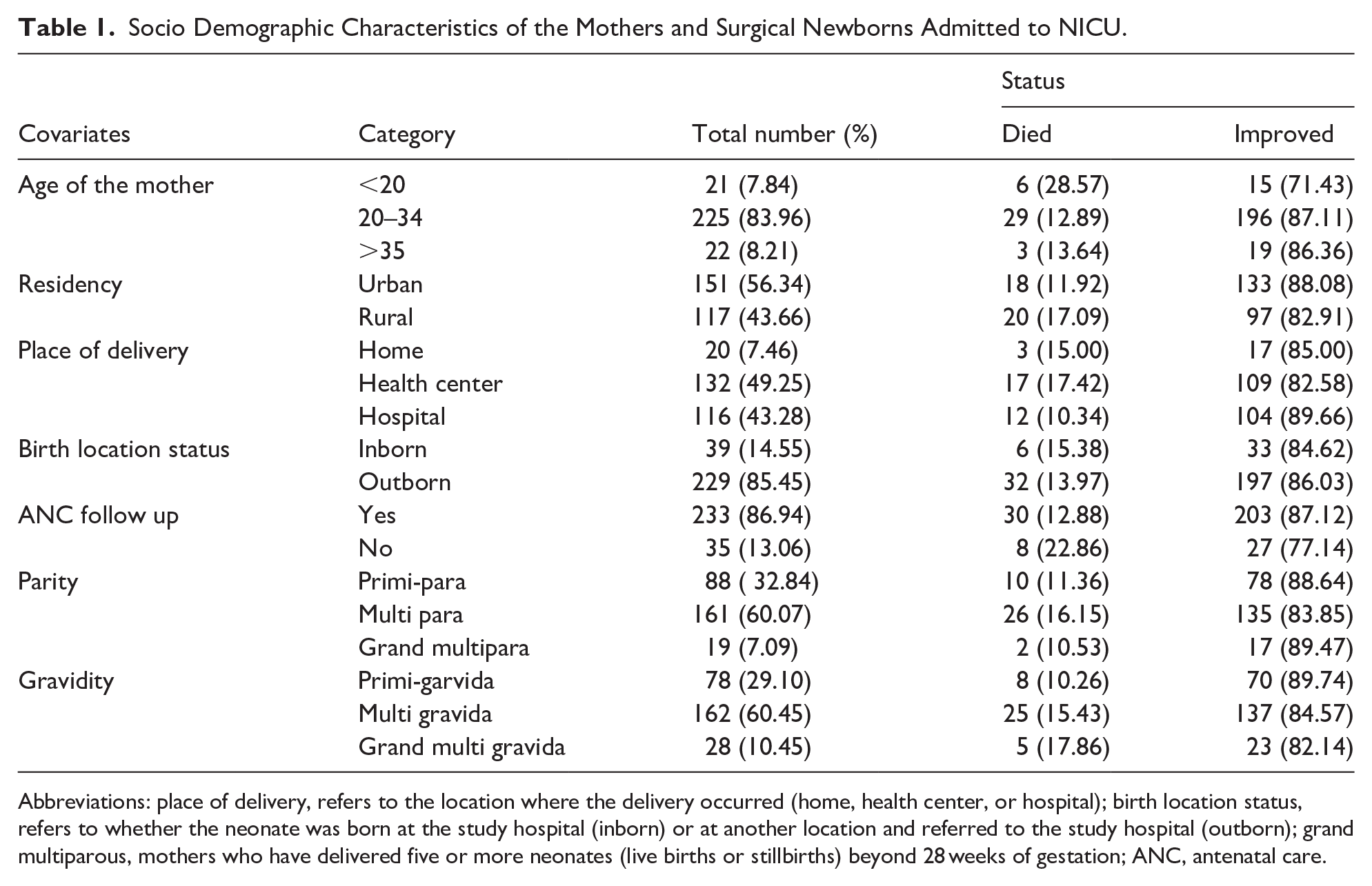
Abbreviations: place of delivery, refers to the location where the delivery occurred (home, health center, or hospital); birth location status, refers to whether the neonate was born at the study hospital (inborn) or at another location and referred to the study hospital (outborn); grand multiparous, mothers who have delivered five or more neonates (live births or stillbirths) beyond 28 weeks of gestation; ANC, antenatal care.
Neonatal Characteristics
Of the neonates, 76.87% had normal birth weight, while 19.40% had low birth weight. The majority (86.94%) were born at term, with a mean gestational age of 38.14 weeks. Neonates aged 9 to 28 days had the lowest mortality rate (3.9%) compared to those aged 0 to 3 days (18.1%) and 4 to 8 days (25.4%). Male neonates made up 53.36% of the sample as shown in Table 2.
Surgical Neonates Related Factors Admitted to NICU at UOGCSH.

Abbreviations: LBW, low birth weight; NBW, normal birth weight.
Pre-Operative Related Factors
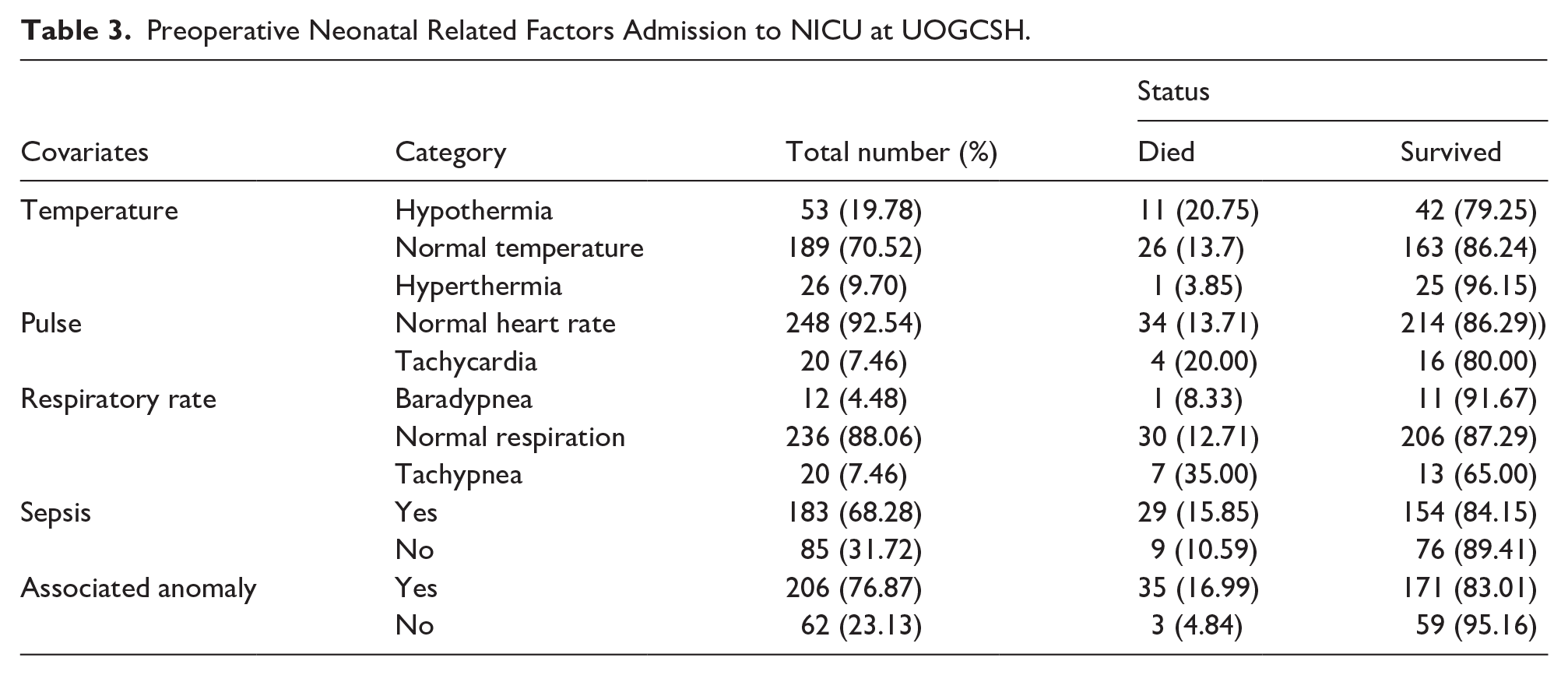
Sepsis was diagnosed in 68.28% of neonates before surgery. Hypothermia occurred in 19.78% preoperatively. Congenital anomalies were present in 76.87% of cases. Tachypnea was observed in 7.46% of neonates, and tachycardia in 7.46% as shown in Table 3, Figures 1 and 2.
Preoperative Neonatal Related Factors Admission to NICU at UOGCSH.
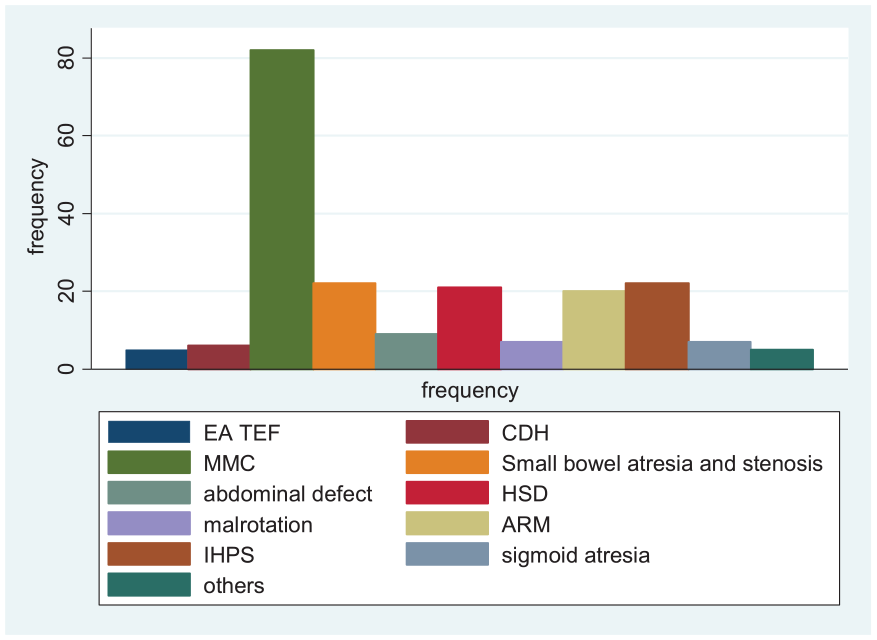
Disease distribution.

Pie chart for site of surgery.
Intra and Post-Operative Factors
Most surgeries (86.57%) lasted less than 60 minutes. Hospital-acquired infections were documented in 23.13% of neonates, with culture-confirmed infections in 10.07%. Postoperative hypothermia occurred in 26.12%. Intra-abdominal surgeries were the most common (42.91%). Most neonates (61.19%) had hospital stays longer than 7 days as shown in Table 4.
Intra-Operative and Post-Operative Neonatal Related Factors Admission to NICU at UOGCSH.

Abbreviations: HAI, hospital-acquired infection; RR, respiratory rate.
Factors Associated With Neonates Surgical Out Come
An analysis of variables was conducted to identify factors associated with surgical outcomes among those admitted and undergoing surgery. Variables including ANC follow-up, anomalies, neonatal infections, culture results, neonatal feeding, pre- and postoperative temperature, postoperative respiratory rate, gestational age, birth weight, neonatal age, maternal age, and hospital stay (P < .2) were included in the multivariable logistic regression analysis as shown in Table 4.
In the multivariable logistic regression analysis, factors significantly associated with the surgical outcome included neonatal infection, birth weight, gestational age, postoperative hypothermia, neonatal age between 9 and 28 days, and prolonged hospital stay, all of which were linked to neonatal surgical-related death.
In this study, neonates with postoperative hypothermia had a 3.19 times higher risk of death compared to those with a normal temperature (AOR: 3.19, 95% CI [1.17, 8.71]). Neonates with infections had a fourfold increased risk of death compared to those without infections (AOR: 4.45, 95% CI [1.49, 13.27]). Similarly, neonates with low birth weight had a fourfold higher odds of death compared to those with normal birth weight (AOR: 3.7, 95% CI [1.12, 12.43]).
Keeping other variables constant, neonates with a hospital stay longer than 7 days had a 3.34-fold higher risk of death compared to those with a stay of less than 7 days (AOR: 3.34, 95% CI [1.15, 9.84]). In this study, preterm neonates had a 3.88 times higher risk of death compared to term neonates (AOR: 3.88, 95% CI [1.04, 14.46]). Neonates aged 9 to 28 days were 78% less likely to die (COR: 0.22, 95% CI [0.05, 0.998]) compared to those aged 0 to 3 days as shown in Table 5.
Multivariate Analysis of Factors Associated with NSM at NICU of UOGCSH (n = 268).

Bold values and asterisks indicate statistical significance.
P < 0.05 is considered statistically significant (*), and P < 0.01 is considered highly significant (**).
Discussion
This study aimed to examine the outcomes and associated factors of neonates who underwent surgery at the University Comprehensive Specialized Hospital. The overall mortality rate for these neonates was 14.18% (95% CI: 10.47%-18.9%), which is lower than the 24.4% mortality rate reported in a study conducted at Black Lion Hospital. 13
The present study figure is also lower than studies done in Kenya 31.5%, 3 South Africa 32.9%, 6 India 35.15%, 16 which may be due to significant number of patients leaving against medical advice prior to surgery. This outcome is higher than that of Ghana (13.5%). 17 The difference may be attributed to variations in the NICU setup, recruitment of neonates from a different population, the use of different methods and sample sizes, and the application of multiple diagnostic criteria. 17
The current study found a statistically significant association between neonatal surgical mortality (NSM) and the presence of sepsis prior to surgery. Neonates with sepsis were 4.4 times more likely to die compared to those without sepsis (AOR: 4.45, 95% CI [1.49, 13.27]; P = .007). This finding aligns with a study conducted at Black Lion Hospital, where sepsis was also identified as a determinant of mortality (P < .02). 13 Similar findings were reported from Nigeria where Sepsis was the commonest cause of death in 47% 18 and in South Africa 61.4%; P < .001. 6
Sepsis at presentation (OR 1·20 [1·04-1·40], P = .016) was significantly associated with increased mortality in a study done in UK from 264 hospitals in 74 low-income, middle-income and HICs. 19 Similar findings were seen from India where sepsis was associated with increased odds of mortality at OR 3.4; 95% CI (1.09-22.06); P = .049. 16
One possible explanation is that their immune responses may be less effective at identifying and combating pathogens, resulting in the rapid progression of infections and an increased risk of mortality. 20 Additionally, delayed diagnosis and treatment may occur because symptoms can be subtle and nonspecific, potentially leading to organ dysfunction and septic shock, which can be life-threatening. This is particularly true for neonates, whose organ systems are still developing and may be more susceptible to damage. 21 The strong association between sepsis and neonatal surgical mortality underscores the need for strict infection control measures in NICUs and surgical theaters. This includes adherence to sterile techniques, prophylactic antibiotic protocols, and early recognition and treatment of sepsis. Healthcare providers should be trained to recognize the subtle signs of sepsis in neonates, as early intervention can significantly improve outcomes.
The study also found that neonates who developed postoperative hypothermia had a 3.19 times higher risk of death compared to those with normal body temperature. This may be due to complications associated with hypothermia, including an increased risk of infection, respiratory distress, cardiac instability, metabolic abnormalities, coagulopathy, and bleeding. Additionally, hypothermia may contribute to impaired wound healing, delayed recovery, acidosis, electrolyte imbalances, and compromised organ function. 22 To address this, neonatal recovery rooms should be maintained at optimal temperatures, and warming devices (eg, radiant warmers, heated mattresses) should be used during and after surgery. 23 Protocols for monitoring and maintaining normothermia should be implemented as part of standard postoperative care.
Neonates with low birth weight have a fourfold higher risk of death compared to those with normal birth weight (AOR: 3.7, 95% CI [1.12, 12.4], P = .033). This finding is supported by studies conducted in Boston 24 and Canada. 25 The increased risk may be attributed to the unique challenges of performing surgery on low-birth-weight neonates, including their small size, fragile anatomy, underdeveloped organ systems, and physiological immaturity, which make them less capable of tolerating surgical stress. Additionally, these neonates often experience feeding difficulties and are highly susceptible to infections. 26
Neonates born prematurely have a 3.88 times higher risk of death compared to full-term neonates. This finding is supported by studies conducted in the USA,27,28 Ireland. 29 This may be due to an increased risk of respiratory distress syndrome, which can worsen during and after surgery. Additionally, preterm neonates have underdeveloped organ systems, including the lungs, heart, and immune system, which may not function optimally. This makes them more vulnerable during and after surgery, potentially contributing to higher mortality rates. 30
Low birth weight and preterm birth were significant predictors of mortality, highlighting the need for antenatal interventions to reduce the incidence of these conditions. This includes maternal health education, antenatal corticosteroid administration for women at risk of preterm delivery, and improved access to prenatal care. Neonates with low birth weight or preterm birth should receive specialized care, including nutritional support and close monitoring for complications.
Neonates who stayed in the hospital for more than 7 days had a 3.34-fold higher risk of death compared to those with a shorter stay. This finding is supported by studies conducted in Canada, 19 Ethiopia, 31 and Kenya. 9 This could be attributed to the higher prevalence of hospital-acquired infections associated with prolonged hospital stays. Another possible explanation is that neonates with extended hospitalizations may have developed complications, ranging from surgical site infections to necrotizing enterocolitis (NEC) and organ dysfunction, which can lead to delayed recovery and increased mortality rates.
Neonates 9 to 28 days old had a 78% lower risk of mortality compared to those of 0 to 3 days, according to studies conducted in Portugal 32 and Tunisia. 33 This finding suggests that as neonates mature and reach a more advanced age, their physiological stability improves. Older neonates may also have had more time to achieve better nutritional status, which is essential for recovery from surgery and reducing the risk of complications. Another possible explanation is that surgical procedures performed in the early neonatal period may be more complex than those conducted after 9 days of age.
In contrast to this study, other research has found that a surgery duration of more than 120 minutes, being outborn, and undergoing intrathoracic surgery were significantly associated with higher mortality. 9 Additionally, previous studies have shown that the unavailability of ventilation, lack of parenteral nutrition, and the need for reoperations were linked to poorer outcomes.34,35 While maternal age was not significantly associated with neonatal surgical outcomes in our study, we included it as a variable to provide a comprehensive demographic profile of the study population. Maternal age can indirectly influence neonatal outcomes through factors such as prenatal care and maternal health, and its inclusion aligns with standard reporting practices in neonatal research.
Finally, we strongly recommend close collaboration between pediatric and surgical healthcare providers to enhance the outcomes of surgical neonates, as surgical outcomes are significantly influenced by preoperative, intraoperative, and postoperative factors.
To reduce sepsis-related mortality, strict infection control measures must be implemented, including adherence to sterile techniques during surgical procedures, the appropriate use of prophylactic antibiotics, and the early recognition and management of sepsis. Emphasis should also be placed on proper hand hygiene among healthcare professionals, caregivers, and visitors. Maintaining a clean and hygienic environment in neonatal units and surgical theaters—through regular cleaning and disinfection of equipment, surfaces, and patient care areas—is essential.
To minimize postoperative hypothermia, neonatal recovery rooms should be kept warm. Additionally, critically ill neonates requiring surgery should be carefully managed during transfers to and from the operating room, as transporting unstable neonates may contribute to increased mortality.
Preventative measures during pregnancy are also crucial. Screening and managing infections in pregnant women, administering corticosteroids to those at risk of preterm delivery, and optimizing folic acid supplementation before and during pregnancy are recommended strategies to reduce the incidence of preterm birth, low birth weight, and neural tube defects such as myelomeningocele (MMC), which is a common indication for neonatal surgery.
Policy Implications
Investment in NICU infrastructure and thermal regulation equipment.
National guidelines for neonatal perioperative care.
Training programs focused on early detection and management of sepsis and hypothermia.
Strengthened referral systems to facilitate timely surgical care.
Strengths of the Study
Despite its retrospective design, this study has several notable strengths. First, it covers a relatively long study period of 5 years, providing a robust dataset to analyze trends in neonatal surgical outcomes. Second, it includes a comprehensive range of clinical variables—spanning preoperative, intraoperative, and postoperative periods—allowing for a multifaceted analysis of mortality predictors. Third, the study was conducted at one of the largest referral centers in Northwest Ethiopia, adding value to the limited body of literature from low-resource settings.
Limitations
This study has several limitations that may affect the interpretation and generalizability of the findings. First, the retrospective design limited the availability and completeness of key clinical data, such as intraoperative complications, bleeding, and wound infection rates. These missing variables may have introduced information bias and restricted the depth of analysis for postoperative outcomes. Second, the study was conducted at a single tertiary referral hospital, which may serve a different patient population compared to primary or secondary healthcare centers. Therefore, the findings may not be fully generalizable to other hospitals in Ethiopia or similar low-resource settings. Lastly, the absence of data on potential confounders—such as maternal education, socioeconomic status, time to presentation, and quality of antenatal care—could have influenced both exposure and outcome variables, potentially affecting the observed associations.
Conclusion
This study identified several factors associated with neonatal surgical mortality, including sepsis, postoperative hypothermia, low birth weight, and prolonged hospital stay. These findings have important implications for clinical practice and policy, highlighting the need for infection control measures, hypothermia prevention, and antenatal interventions to improve outcomes. By addressing these factors through targeted interventions and policy changes, healthcare systems in similar environments can reduce neonatal surgical mortality and improve the quality of care for this vulnerable population.
Footnotes
Abbreviations and Acronyms
Ethical considerations
Ethical approval for the study was obtained from the Institutional Review Board (IRB) of the University of Gondar, College of Medicine and Health Sciences, with reference number 829/12.
Authors’ contributions
WEM: Conceptualization, data collection, analysis and writing. YHD: Data analysis, manuscript revision. MST: Data analysis, manuscript revision. KGT: Data collection, entry and analysis. MKA: Manuscript writing and revision. ADB: Manuscript writing and revision. SAK: Data curation, entry and analysis. YDM: Revision and submission.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request