
Abstract
Objectives:
The major aim of this study was to assess the magnitude of pelvic organ prolapse and its associated factors among patients admitted to the gynecology ward at Hiwot Fana Specialized University Hospital, eastern Ethiopia.
Methods:
A retrospective review of records was undertaken at Hiwot Fana Specialized University Hospital. We used a simple random sampling technique to pick 387 gynecology ward–admitted patient records from 30 December 2020 to 10 January 2021. Data were extracted from maternal medical charts using a pretested checklist. The extracted data were entered into EpiData version 3.1 and then exported into SPSS version 25 for analysis. Binary logistic regression was carried out to observe a significant correlation between independent and pelvic organ prolapse. An adjusted odds ratio and 95% confidence interval was used to report the result. A p-value of less than 0.05 was used to declare statistical significance.
Results:
Among 387 responded women, 39 (10.1%; 95% confidence interval = 8.3–15.6) of them had at least one stage of pelvic organ prolapse. Multiparty (adjusted odds ratio = 1.88, 95% confidence interval = 1.41–10.60), grand multiparty (adjusted odds ratio = 2.63, 95% confidence interval = 1.53–12.90), older maternal age (adjusted odds ratio = 2.29, 95% confidence interval = 1.220–7.52), lifting a heavy object (adjusted odds ratio = 4.61, 95% confidence interval = 2.31–15.83), and having chronic cough (adjusted odds ratio = 2.39, 95% confidence interval = 1.10–5.19) were significantly associated with pelvic organ prolapse.
Conclusion:
Among women admitted to the hospital because of gynecological morbidity, one in ten of them had pelvic organ prolapse. Multiparty, advanced maternal age, having a chronic cough, and lifting heavy objects were identified to be risk factors for pelvic organ prolapse. Tailored primary prevention would enhance the well-being of reproductive-age women.
Keywords
Introduction
According to the International Continence Society, the primary definition of pelvic organ prolapse (POP) is anatomical alteration, which refers to a sliding, descent or moving downward of one or more of the vaginal wall, the uterus, or the apex of the vagina. 1 POP is caused by a combination of high-risk factors that raise intra-abdominal pressure: chronic pulmonary illness, constipation, obesity, and hard manual labor, as well as age, pregnancy, delivery, and prior pelvic surgery. 2 In low-income countries, it is a significant public health issue that has a detrimental influence on the lives of millions of adult women.3,4
Globally, 3.3–4.9 million women have been suffering from POP, which makes the worldwide prevalence of POP around 9%. However, in developing countries, the prevalence of POP is rapidly increasing, which recently has been estimated to be 20%.5,4 POP may have a significant negative impact on a woman’s quality of life by compromising her physical, social, psychological, and sexual functions, as well as causing significant discomfort and distress. Many women with POP have also been suffering from depressive symptoms. 6 It is thought that low-income countries have a more significant burden of POP than developed countries. 7 It is extremely common in women over the age of 40 years, elderly women, and postmenopausal women, with a prevalence of 41%–50%. 8
The Ethiopian Federal Ministry of Health emphasized the strategy to expand services in governmental and private healthcare facilities to treat women living with POP and prevent its occurrence under the theme “Ending Fistula and Transforming Lives by 2020.” 9 However, a systematic review and meta-analysis report in 2020 showed that the prevalence of POP was estimated to be 23.52% in Ethiopia. 10 Ethiopia is thought to be among the countries with the highest rates of POP in the world due to multiple risk factors, including a high proportion of home deliveries, early marriage and delivery, high fertility, a high proportion of malnutrition and obstructed labor, and rural women. 9 According to the 2019 Ethiopian Demographic Health Survey (EDHS) report, only 48% of Ethiopian women give birth in health facilities, despite the country’s high fertility rate, which is attributed to the incidence of gynecological disorders. 11 For instance, POP accounted for more than 40.7% of major gynecological procedures in the Jimma University Specialized Hospital. 12 It causes a variety of physical disabilities, such as the inability to work, difficulty in walking or standing up, peeing or defecating, painful intercourse, increasing social stigma, and economic destitution. 13 POP mostly affects women between the ages of 50 and 70 years, many women spend a significant portion of their lives dealing with its effects as it became a more serious issue as women’s life expectancies have been increasing, and it is anticipated to double in the next 25 years.2,14
The report of studies done across the world has identified risk factors for the development of POP such as obesity, 2 age at last birth,15–17 parity,15,18 gravidity, 15 mode of delivery, 19 delivery by unskilled birth attendants,16,18 family history of POP, 18 prolonged labor, 17 educational status, 18 occupational status,15,18 genetic factors, anemia, 17 body mass index, 18 and carrying heavy objects.7,17
Even though POP affects the physical, social, psychological, and sexual well-being of the women, merely it is neglected by clients, care providers, and the community. As well as it is not well explored in sub-Saharan Africa, especially concerning the magnitude and associated factors. Furthermore, the Ethiopian government has not yet developed a distinct strategy to prevent and manage POP in both private and public health institutions. Therefore, identifying risk factors of POP helps responsible bodies to take interventional action at the earliest stages of the disease. Hence, this work aimed to assess the magnitude of POP and associated factors among women admitted to the gynecology ward at the Hiwot Fana Specialized University Hospital (HFSUH).
Methods
Study design, area, and period
A facility-based cross-sectional study with retrospective data was undertaken at HFSUH, gynecology ward which is located in Harari town. Harari town is the capital city of Harari regional state, which is 526 km to the east of Ethiopia’s capital city Addis Ababa. HFSUH is one of the tertiary referral hospitals and a teaching center in eastern Ethiopia, which offers a variety of healthcare services. The hospital services of more than 5.8 million people who come from the Harari region, Oromia region, Dire Dawa Administration, and Somali region. The hospital gives services under different clinical disciplines including internal medicine, gynecology and obstetrics, surgery, and pediatrics. 20 The study was conducted from 30 December 2020 to 10 January 2021.
Populations
All women admitted to the gynecology ward of HFSUH were the source population, while all women admitted to the gynecology ward from 1 January 2017 to 31 December 2019 were the study population.
Inclusion and exclusion criteria
All randomly selected medical charts of women admitted to the gynecology ward were included, while women with incomplete medical records were excluded from the study.
Sample size determination and sampling procedure
The single population proportion formula was used to estimate the required sample size. (n = (Za/2)2p(1 − p)/d2), with the assumptions of Z = 1.96, confidence interval (CI) = 95%, a margin of error (d = 0.05), and the proportion of POP (p = 0.407) from the study done in Southwest Ethiopia. 12 The total sample size was 408 after adding 10% of the no retrieval rate.
Between 1 January 2017 and 31 December 2019, 1136 women were admitted to the gynecological ward. Using the Medical Registration Number (MRN), which was obtained from their medical records, the sample frame was then generated. Finally, using a simple random sampling procedure (computer-based) from the sample frame (N = 1136), the study subjects who had been included in the investigation were identified.
Data collection methods and quality assurance
Data were extracted from the medical record charts using a semi-structured, pretested checklist. A checklist was adapted after reviewing different literature, which was modified and contextualized to fit the research objectives.18,21,22 The checklist includes socio-demographic characteristics, obstetrics and gynecology history, and the reproductive health and medical problems of the study participants. Detailed obstetrics and gynecologic history were taken from the patient’s medical records. The tool was pretested on the 5% of sample size before the data collection was commenced. Then, the reliability of the tools was assessed, and its Cronbach’s alpha value was 0.88. Three well-trained nurses with a BSc in nursing collected the data under the supervision of one medical doctor. The principal investigator and supervisors reviewed the questionnaires to check the completeness and consistency of the data every day.
Study variables
Dependent variable
The dependent variable is pelvic organ prolapsed.
Independent variables
Socio-economic variables: age, occupation, ethnicity, religion, residency, and educational status.
Reproductive variables: parity, mode of delivery for the last birth, family history of POP, history of prolonged labor, history of abortion, and history of home delivery.
Medical status: chronic cough and chronic constipation.
Work-related factors: lifting heavy objects.
Operational definitions
POP: it is a record of any stage of POP diagnosed by health professionals during admission of the patient and documented on the patient’s medical record chart.23,24 The health workers used the results of the pelvic examination based on the maximal extent of prolapse relative to the hymen and the patient’s stated symptoms to identify symptomatic POP and the stage.
Chronic cough: it is characterized as one that lasts for more than 8 weeks. 25
Chronic constipation: it is a frequency of fewer than three stools per week that persists for at least 3 months. 26
Statistical analysis
The extracted data were entered using EpiData version 3.1 and then exported into SPSS version 25 for data analysis. A descriptive analysis was computed to describe predicted variables. The result was displayed using frequencies, tables, and figures. The outcome variable (POP) was dichotomized into yes (coded as 1) and no (coded as 0).
Binary logistic regression was performed to examine the relationship between independent variables and POP. All variables with p-values of 0.25 in the bivariate analysis were retained for the multivariable analysis. The Hosmer–Lemeshow statistic and the omnibus test were used to evaluate the model’s goodness of fit. Given that it is significant for the omnibus tests (p = 0.000) but not for the Hosmer–Lemeshow statistic (p = 0.63), it was deemed to be a good fit. The variance inflation factors (VIFs) and tolerance test were used to determine the presence of multicollinearity among independent variables. No variables were seen with VIF >10 and tolerance test <1. The adjusted odds ratio (AOR) along with 95% CI was used to report the result. A statistically significant association was declared at a p-value less than 0.05.
Results
Socio-demographic characteristics
From the total of 408 patients’ medical records, 387 patients’ cards were retrieved and analyzed, resulting in a 95% response rate. The mean age of the respondents was 34.6 with a standard deviation of ±12.7 years. One hundred sixty-eight (43.4%) of the participants were in the age group of 25–34 years. More than half (57.4%) of the respondents were rural residents. In terms of educational status, the majority of respondents (87.6%) have no formal education (Table 1).
Socio-demographic characteristics of patients admitted to the gynecology ward at HFSUH, eastern Ethiopia 2021.
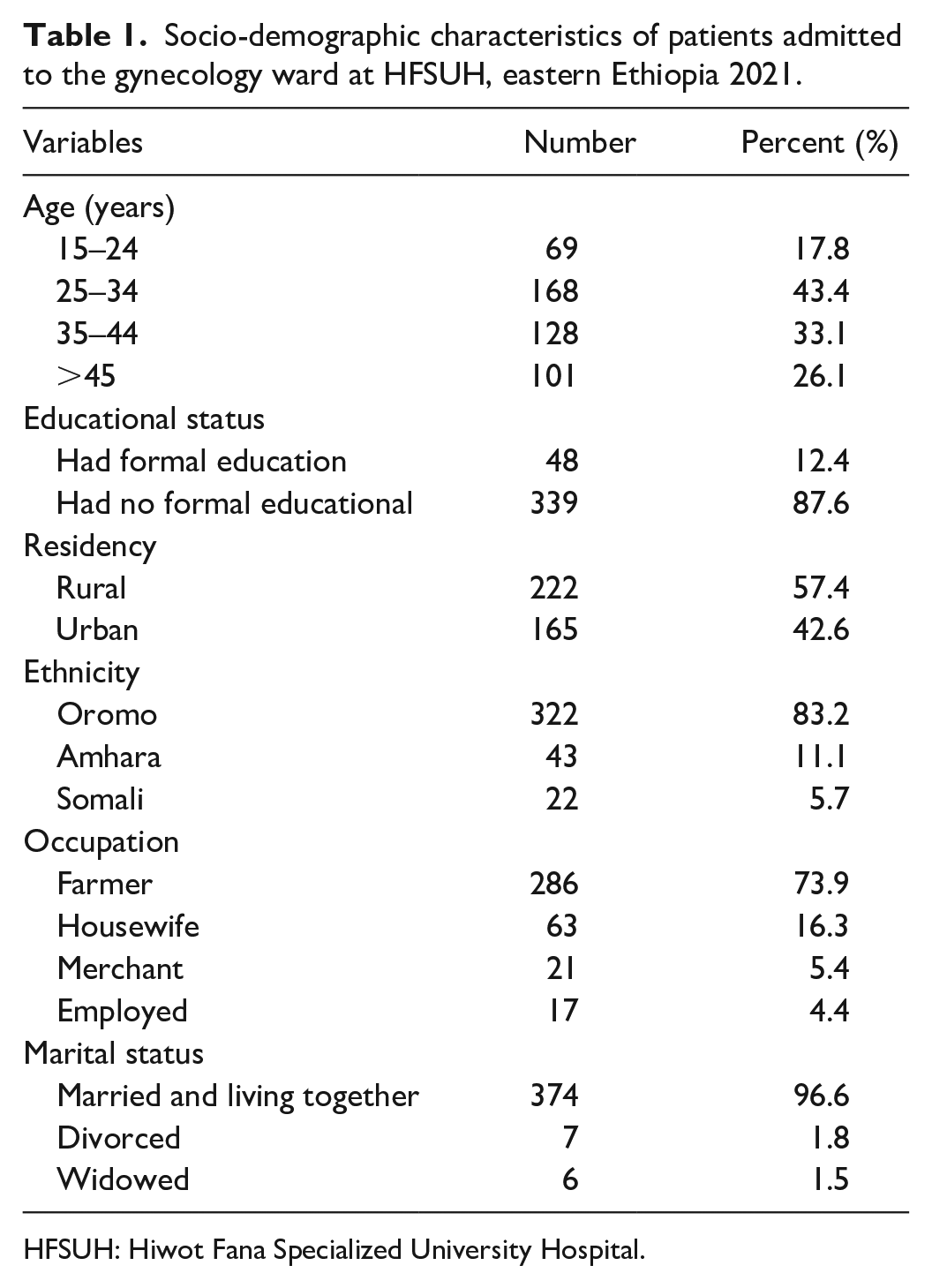
HFSUH: Hiwot Fana Specialized University Hospital.
Reproductive health history
One hundred sixty-three (42.1%) of the women had previously delivered their babies at home, while only 45 (11.6%) of the women had experienced prolonged labor. Approximately 69 (17.8%) of the respondents have previously had an abortion. The largest proportion of the women 366 (94.6%) gave their last births through vaginal delivery. Only, 49 (12.6%) of the women had a family history of POP (Table 2).
Reproductive health characteristics of the women’s admitted to the gynecology ward at HFSUH, eastern Ethiopia 2021 (n = 387).
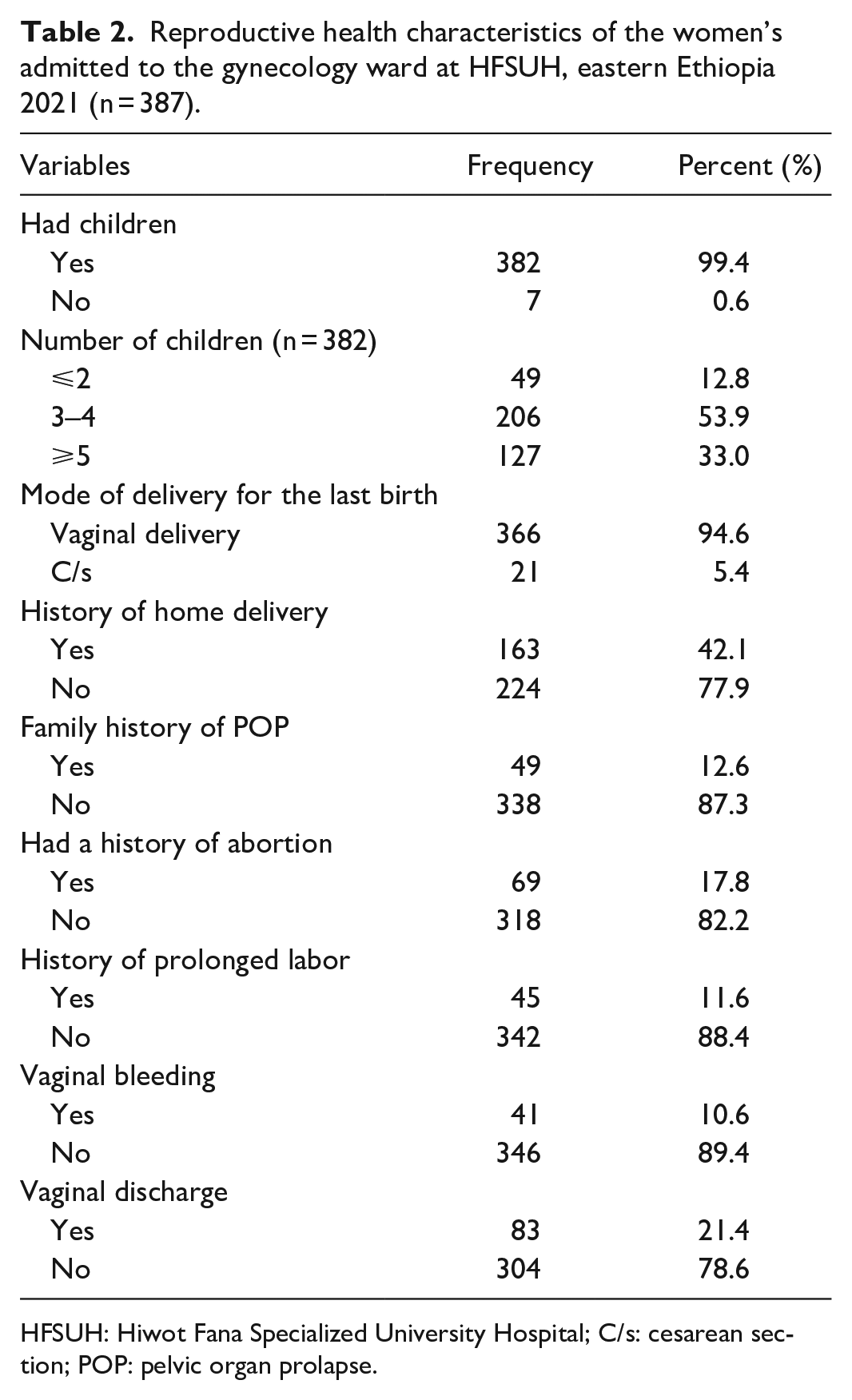
HFSUH: Hiwot Fana Specialized University Hospital; C/s: cesarean section; POP: pelvic organ prolapse.
Medical health status of the respondents
Regarding the medical health status of the women, 121 (31.3%) had a chronic cough and only 11 (2.8%) had ever had a history of constipation. About 91 (23.5%) of the participants had complained of abdominal pain. Only, seven (1.8%) of the study subjects had encountered genital ulcers (Table 3).
Medical characteristics of the women’s admitted to the gynecology ward at HFSUH, eastern Ethiopia 2021 (n = 387).
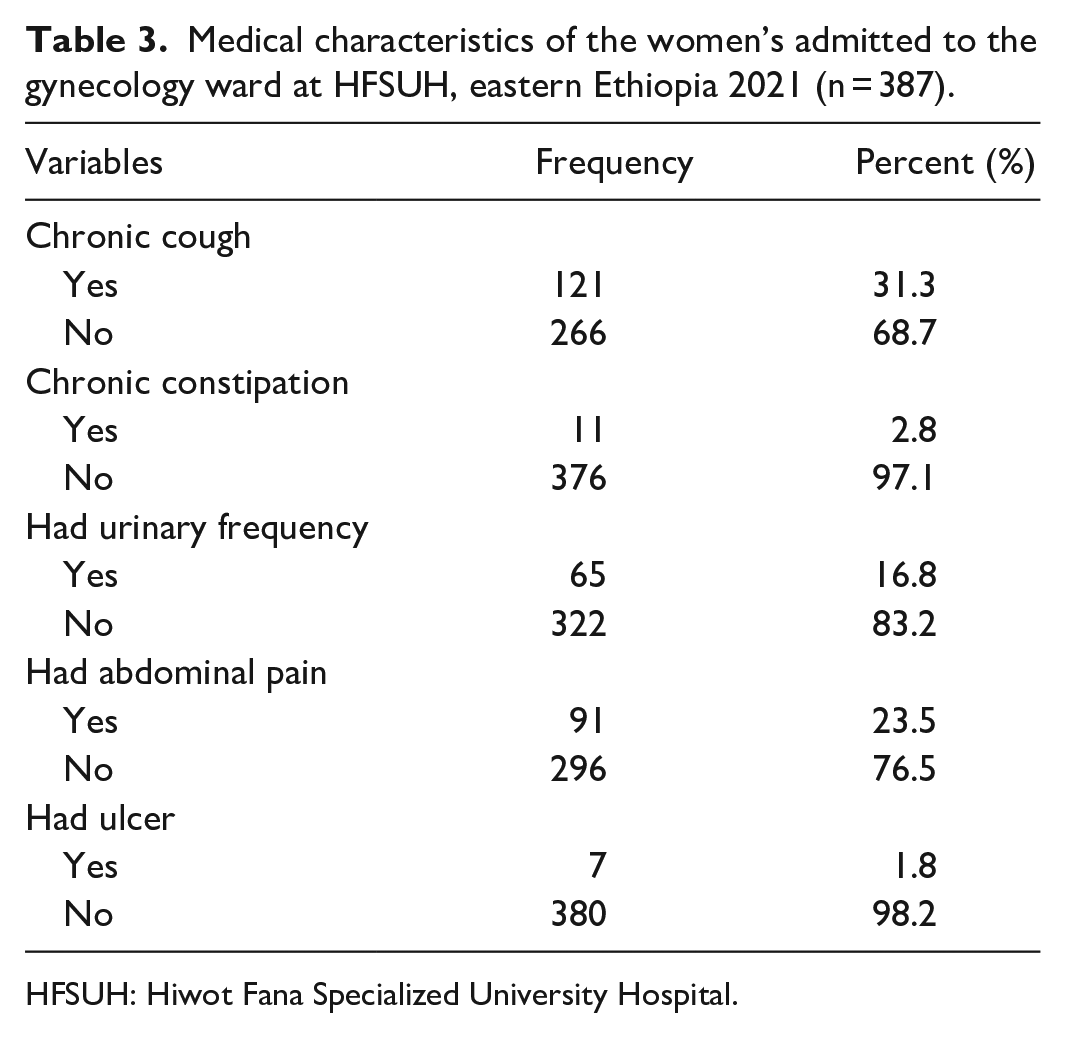
HFSUH: Hiwot Fana Specialized University Hospital.
The magnitude of POP and clinical characteristics
Of the total study participants, 39 (10.1%, 95% CI = 5.8–15) experienced at least one type of POP. The documented grade of POP was 5 (12.8%) grade I, 9 (23.1%) grade II, 14 (35.9%) grade III, and 11 (28.2%) grade IV with the most predominant type were being cystocele, rectocele, and followed by urethrocele. Urinary incontinence and impaired sexual function were the most commonly documented symptom followed by pelvic heaviness and feeling pressure in the lower abdominal. These were reported by 43.6%, 43.6%, and 69.4% of the women with POP, respectively (Figure 1).

Magnitude of POP among women’s visited the gynecology ward at HFSUH, eastern Ethiopia 2020 (n = 387).
Factors associated with POP
All variables with a p-value of 0.25 in the bivariable analysis were taken into multivariable analysis. Accordingly, age, parity, chronic cough, and lifting heavy objects were significantly associated with POP.
The odds of having POP were 2.3 (AOR = 2.39, 95% CI = 1.10–5.19) times higher among participants who had a history of chronic cough compared to those who did not have a history of chronic cough. Women who carried heavy object were 4.6 (AOR = 4.61, 95% CI = 2.31–15.83) times more likely to develop POP than women who did not have a history of carrying heavy objects. Parity was also a risk factor for POP, with the likelihood of POP being higher among multiparous (AOR = 1.88, 95% CI = 1.41–10.60) and grand multiparous (AOR = 2.63, 95% CI = 1.53–12.90) compared to their counterpart. Furthermore, the odds of developing POP were 2.3 times higher among women older than 55 years (AOR = 2.29, 95% CI = 1.22, 7.52) as compared to women below 41 years (Table 4).
Bivariate and multivariable analysis of factors associated with POP among patients admitted to gynecology ward at HFSUH, eastern Ethiopia 2021 (n = 387).

POP: pelvic organ prolapse; COR: crude odd ratio; CI: confidence interval; AOR: adjusted odd ratio.
Discussion
In this study, the prevalence of POP based on the physician record diagnosis was found to be 10.1% (95% CI = 5.8–15), which implies the magnitude of the problem is continuing to be high in Ethiopia. This finding is consistent with the result of studies conducted in Nepal (10.3%), 21 Ghana (12.03%), 27 and China (14.8%). 28 However, the current prevalence is lower than a report of studies conducted in the United Arab Emeritus (UAE, 29.6%), 29 Turkey (27.1%), 30 Tanzania (64.6%), 7 Northwest Ethiopia (56.3%), 31 and Amhara Regional State, Ethiopia (37.6%). 17 The observed discrepancy might be explained by the fact that different data collection instrument was used between the studies. For example, the study in Tanzania, Amhara Region, and Turkey was community-based and used interviews and physical examination to measure the POP, whereas in this study, we used only physician diagnoses from the client’s medical records. Some of the former studies relied solely on participant-reported symptoms to measure POP, which may uncertainly estimate the prevalence. In addition, in Tanzanian study, the median age of the study subjects was 46 years which is higher than this study of 34.5 years, potentially increases the prevalence.
The prevalence of POP in this study is higher than the report of studies done in Southwest Ethiopia (5.9%), 13 Nigeria (3.9%), 32 and Ghana (2.6%). 33 The discrepancy in the estimation of the prevalence of POP might be due to variations in sample size, study setting, and study participants. For instance, these studies included only women who visited the gynecology ward which could increase the prevalence, while most previous studies recruited participants from different wards. Besides, variation in socio-economic status, sample size, and methodological differences may explain the observed discrepancies.
This study revealed that multiparous women were more likely to experience POP, which was in agreement with the studies done in Ethiopia,18,31 Turkey, 30 Ghana, 27 Pakistan, 21 and Tanzania. 7 This might be because frequent childbearing weakens the pelvic muscles and ligaments, increasing the risk of POP development due to repeated damage to the pelvic organs’ support systems. Another possible reason is neurological dysfunction according to reports from studies done in Turkey. 34 It has been claimed that frequent vaginal deliveries induce neurological damage, pudendal and/or levator ani nerve damage, as well as traumatic injury to the levator ani muscle from the mechanical forces of vaginal delivery which may contribute to the development of POP. 35
A significant correlation between increasing maternal age and POP was documented in several studies. Similarly, in this study, women aged ⩾45 years or older were more likely to develop POP. This finding was in line with studies conducted in Ethiopia,18,31 Tanzania, 7 and Nepal. 36 This could be justified by the fact that as a mother’s age increases, the pelvic muscles and ligaments get weaker, which in turn causes POP. In addition, maternal age was associated with a decrease in estrogen after menopause, which results in changes in connective tissue composition. 37
Another factor significantly associated with POP was carrying heavy objects. This result is supported by studies done in Dabat District, 31 Bahir Dar Referral Hospital, Ethiopia, 18 Nepal, 38 and Tanzania, 7 which state lifting heavy objects increases the risk of developing POP. This might be explained by the fact that lifting heavy objects exhausts the pelvic floor muscles and pulls down the pelvic organs. Furthermore, in our studies, 57.4% of women with POP lived in rural areas, where their daily activities include carrying objects, assisting in farmland and wood, and engaging in agricultural loads, all of which are physically demanding jobs that contribute to the loss of genitourinary supporting structures. 12 However, this finding contradicts the study done in the UAE, 29 which showed that women who were involved in jobs requiring physical exertion were less likely to have POP than their counterparts. The variation in socio-economic, sample size, and nutritional status of the two areas may justify the observed difference.
Moreover, in this study, having a history of chronic cough was positively associated with POP. A similar report was found from the study conducted in Ethiopia 39 and China, 40 which states smoking and coughing worsen POP. The possible justification is because coughing repeatedly and/or forcefully can stretch pelvic floor tissues, weaken the pelvic floor, which in turn forces the pelvic floor to move downward, worsen prolapse symptoms, and increase the degree of prolapse.41,42
Conclusion
This study highlights that one in ten women have been suffering from POP. These findings suggest that a substantial number of women suffer from POP, which needs close attention by policymakers, programmers, and healthcare practitioners. Parity, women’s age greater than 55 years, history of carrying heavy objects, and having a history of chronic cough were factors that had a significant correlation with POP. Therefore, strengthening emphasis on family planning and women’s education on risk factors, early treatment of chronic disease, and counseling on avoidance of lifting heavy objects are recommended.
Strength and limitation of the study
The main strength of this study is that the entire outcome variable measurement was based on the physician’s diagnosis. It has also some limitations. The primary drawback of this study is that it is retrospective in which some data may be overlooked or lost as a result of incorrect case record input. For instance, important factors like body mass index and birth interval were not assessed. Second, the study was hospital-based; it lacks generalizability to the community at large because the majority of women suffering from POP do not seek healthcare.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221126363 – Supplemental material for Pelvic organ prolapse and associated factors among women admitted to gynecology ward at the Hiwot Fana Comprehensive Specialized Hospital, Harar, eastern Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121221126363 for Pelvic organ prolapse and associated factors among women admitted to gynecology ward at the Hiwot Fana Comprehensive Specialized Hospital, Harar, eastern Ethiopia by Abdek Ali, Elias Yadeta, Addis Eyeberu, Lemesa Abdisa, Miressa Bekana and Merga Dheresa in SAGE Open Medicine
Footnotes
Acknowledgements
The authors are very grateful to Haramaya University for providing the opportunity and assistance to complete this research thesis. The authors also wish to express their gratitude to their friends for their support and enlightening remarks, as well as the women who participated in this study and data collectors.
Author contributions
A.A. contributes to the literature review, training and supervising the data collectors, and checking the completeness of collected data. All authors made a significant contribution to this work. The major contributions include study designing, execution, acquisition of data, analyzing, interpreting the result, and preparing the manuscript. More overall co-authors wrote the final draft of this manuscript and gave final approval of the version to be published.
Availability of data and materials
The data sets that were used and/or analyzed during this work are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of Haramaya University, College of Health and Medical Sciences (IHRERC, 2019).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from hospital administrators. Since due to the nature of the data (secondary data), we were unable to obtain consent from each subject. So, we sought consent from a legally authorized individual, namely, the hospital administrator. The proposal paper was reviewed by the Ethics Review Committee of Haramaya University before the study began, and it was approved.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.