
Abstract
Background:
Globally about 9 million neonates are diagnosed with birth asphyxia yearly. In Tanzania 40.6% of all neonatal deaths are attributed to birth asphyxia. There is scarcity of evidence on predictors of in-hospital survival among asphyxiated neonates in Tanzania, therefore study aimed to determine trends and predictors of survival among neonates who sustained birth asphyxia at Kilimanjaro Christian Medical Center, Northern Tanzania.
Method and materials:
This was a hospital-based retrospective cohort study, conducted at Kilimanjaro Christian Medical Center among 7,783 admitted asphyxiated neonates from 2000 to 2022. The predictors of survival were determined by using the Weibull survival regression model and the statistically significant results were declared at a p-value of <.05. Data were managed and analyzed using Stata 18.
Results:
Overall finding from this study showed significant increase in the trends of survival from birth asphyxia from 2000 to 2022, from 68% to 80% respectively (p-value < .001). The median survival time was 4 days (95% CI:3.0-6.0). Overall survival rate was 195.32/1000 person-days-of observation (95% CI: 190.57, 200.18). Antenatal care (ANC) stages (AHR: 0.74; 95% CI: 0.62-0.89), gestation age (AHR: 0.81; 95% CI: 0.76-0.86), birth weight (AHR: 1.19; 95% CI: 1.12-1.26), mode of delivery (AHR: 1.69; 95% CI: 1.60-1.78), Aminophylline (AHR: 1.56; 95% CI: 1.52-1.60), oxygen (AHR: 1.32; 95% CI: 1.23-1.42), resuscitation (AHR: 1.32; 95% CI: 1.24-1.42) and HIE(AHR: 1.85; 95% CI: 1.79-1.91) were all independent significant predictors of survival.
Conclusion:
There is a need for health professionals to remain vigilant and promptly assess and stabilize the airway, breathing, and circulation, initiate resuscitation, provide oxygen, administer medications such as aminophylline to neonates who are diagnosed with birth asphyxia.
Background
Birth asphyxia is a critical problem for child survival globally, arising once a newborn's brain and vital organs are deprived of sufficient oxygen prior to, during, or immediately after delivery. 1 The World Health Organization(WHO) defines birth asphyxia as inability to initiate and sustain breathing at birth. 2 This condition stands as a significant contributor to neonatal morbidity and mortality on a global scale contributing as high as 42 million disability-adjusted life years among neonates. 3
Globally, up to 9 million neonates are diagnosed with birth asphyxia each year. 4 Approximately 25% of all neonatal mortalities are linked to birth asphyxia making it one of the top three leading causes of neonatal death. 2 Sub Saharan Africa is responsible for more than two-third of all neonatal deaths that occur due to birth asphyxia worldwide and about 280,000 neonates diagnosed with birth asphyxia die in the first day of life in the region. 5
In Tanzania birth asphyxia is responsible for about 40.6% of all neonatal deaths, preterm births following closely at 24.2%, trailed by infections at 20.9% and congenital malformations at 5.1%. 6 Furthermore, it has significantly contributed to child mortality for about 39%.7,8 At Kilimanjaro Christian Medical Center (KCMC) hospital Birth Asphyxia was identified as prominent condition leading to majority of neonatal death.9,10
Birth asphyxia may result to both long term and short-term adverse outcomes these include but not limited to developmental delays, cognitive impairment, motor disabilities which have significant effects on child life. 11 Survival vary based on the severity of initial injury, about 25% of neonates diagnosed with Birth Asphyxia end up with permanent neurological deficit. 12 Systemic effects can also occur as a result of asphyxia, these effects include neurologic insult, respiratory distress, pulmonary hypertension and dysfunction of the kidney, liver and heart.
Different studies have identified mothers age, gestation age, sex of the child, antenatal care, mother’s education, induction of labor, mother’s occupation birth weight, residence and mode of delivery to be strong predictors of survival among asphyxiated neonates.13 -18 Survival rate may be noticeably greater in regions with highly established healthcare systems and more advanced medical technologies. 19 Studies done in Ethiopia, reported an overall survival rate of 9.9 to 10 per 100 neonatal-days of observation neonates-days of observation.16,20 Tanzania has not conducted any study pertaining in-hospital survival among asphyxiated neonates.
To address birth asphyxia, the government of Tanzania alongside other collaborators have put in place different interventions and programs to improve survival of the newborns, these included but not limited to, Help Baby Breath program (HBB) with the main aim of building capacity of health care workers ensuring they can effectively oversee and implement improved neonatal care practices.21,22
There is a scarcity of evidence on the in-hospital survival rates and predictors of survival among asphyxiated neonates in Tanzania. Moreover, global trends in survival and survival rate have not been adequately studied. Unlike other studies, addressing this gap requires time-to-event analysis to accurately assess the risk of survival over time. Additionally, there is a pressing need to analyze data spanning multiple years aligning with ongoing programs and interventions. Therefore, this study aimed to determine trends, rate and predictors of survival among neonates who sustained birth asphyxia in Northen Tanzania.
Methods and Materials
Data Source and Study Design
The study utilized birth cohort data from the medical birth registry at KCMC established in 1999 to collect maternal reproductive histories and support reproductive health research and perinatal care monitoring. 23 KCMC is the zonal referral hospital which serves a population of about 15 million people, including local women and referred cases from neighboring regions and countries. Kilimanjaro region has a population of 1,861,934 with a density of 124 people per km². About 4,000 births occur at KCMC each year. 24 The primary socio-economic activities in Kilimanjaro encompass tourism, agriculture and industrial activities.25 -27 The birth registry is situated on the hospital premises within the Reproductive and Child Health Center (RCH).
The current study was retrospective cohort study from 2000 to 2022, conducted at Kilimanjaro Christian Medical Centre (KCMC) Zonal Referral Hospital in Moshi Municipality, Kilimanjaro region, Northern Tanzania.
Data Collection Methods
A detailed description of the data collection procedure and the data collected for the KCMC birth registry has been documented in previous publications.10,23,28 In summary, birth data at KCMC were recorded through a standardized questionnaire. Data collection was carried out by specially trained project midwives, who interviewed mothers within the first 24 hours after a normal delivery, or on the second or third day following a complicated delivery, depending on their condition, after obtaining informed consent. While the printed questionnaires were in English, the project midwives conducting the interviews were fluent in English, Swahili, and another local language. Patient files and antenatal care cards were used to verify interview data and gather additional information. Data for admitted neonates were recorded separately in a neonatal registry form and later linked to the mother’s data in the birth registry using unique identification numbers. Additionally, each woman was assigned a unique identification number upon initial admission, which was used to trace her medical records during subsequent admissions.
Study Population, Sample Size and Sampling
The study population was neonates who experienced birth asphyxia and captured at KCMC medical birth registry from 2000 to 2022. A total of 70,541 deliveries were documented in the KCMC medical birth registry from 2000 to 2022. After excluding 62,284 deliveries without a diagnosis of birth asphyxia, the study retained 7,783 asphyxiated neonates (Figure 1). Neonates with diagnosis of birth asphyxia available in the registry from 2000 to 2022 were included in the study. Neonates born with congenital malformations as well as neonates whose admission and/or discharge date was unknown were excluded from the study.

Flow chart for selection of asphyxiated neonates from 2000 to 2022 in the KCMC medical birth registry.
Variables
Dependent variable was survival status which was dichotomized into survived and Censored. Independent variables were neonatal characteristics such as sex (male and female), gestation age (preterm and term), birth weight (normal birthweight i.e. ≥2,500 grams and low birthweight i.e. <2,500 grams), maternal characteristics such as mode delivered (vaginal delivery and cesarean section), maternal age (≤19, 20–34, 35–39 and 40+) in years and antenatal care (yes and no) and clinical characteristics such as use of Aminophylline (yes and no), Oxygen (yes and no), resuscitation (yes and no) and the stages of HIE (mild, moderate and severe). The study’s choice and categorization of independent variables were informed by previous literatures.16,27 -29
Operational definitions
Data Processing and Analysis
Data was extracted from the electronic database of KCMC medical birth registry. Data exploration was done to check for missingness. Missingness of data was dealt by doing complete case analysis. Data cleaning and analysis performed using STATA version 18 (Stata Corp, College Station, TX). Descriptive statistics were summarized using frequencies and percentages. Pearson Chi-square was used to assess distribution of independent variables around dependent variable. The significance level was set at P < .05 (2-tailed). A test (nptrend test) for trend by years was performed to rollout if the observed trends were statistically significant. A Kaplan-Meier (KM) survival curve was employed to estimate the survival time and probability from survival of birth asphyxia. The overall survival rate and the cumulative survival probabilities was calculated as number of survivals per person days (PDs) at Risk for all study participants. The survival rates were calculated by neonatal characteristics and the Mantel-Cox method was used to explore the effect modification. Wilcoxon–Breslow–Gehan estimate test was used to compare the probabilities of survival curves between different categorical independent. To maintain uniform follow up time the plotted cumulative hazards rates was truncated at 28 days.
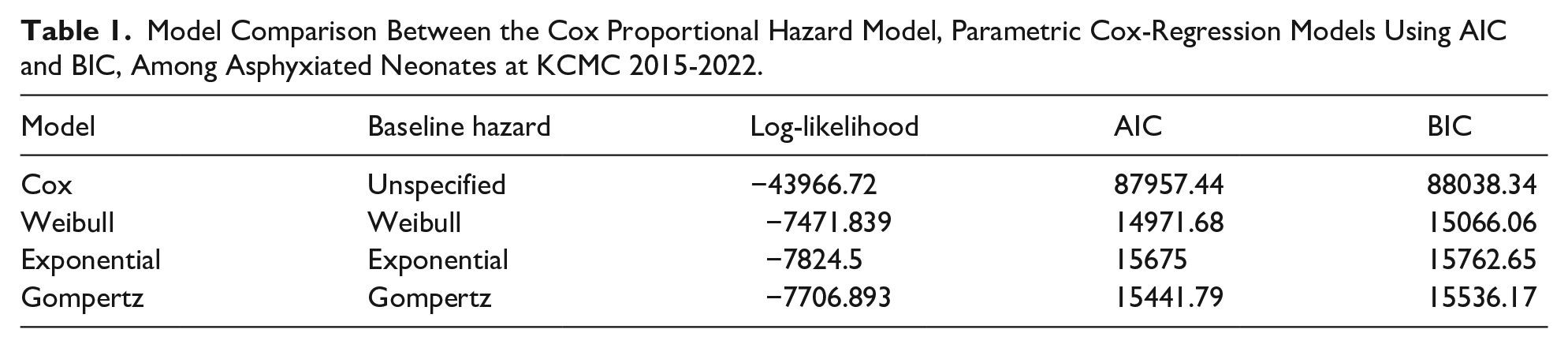
Akaike's information criterion (AIC), Bayesian information criterion (BIC) and Log-likelihood were used to identify the best-fitting model, with the model having the lowest AIC value being considered the best fit model (Table 1). The goodness of fit of the model was evaluated by Cox-Snell residuals and the Nelson-Aalen cumulative hazard function graph (Figure 2).
Model Comparison Between the Cox Proportional Hazard Model, Parametric Cox-Regression Models Using AIC and BIC, Among Asphyxiated Neonates at KCMC 2015-2022.

Goodness of fit using Cox-Snell residual.
To determine predictors of survival, bivariate and multivariable Weibull regression models were used. Bi-variate Weibull regression model was fit for each explanatory variable. Considering biological plausibility, clinical relevance, literature and using backward elimination method those variables with a p-value ≤ .2 were fit to multivariable Weibull-regression analysis to identify independent predictors of survival of asphyxiated neonates. A significance level of ≤ 0.05 was used in adjusted analysis. The variables reported were those found to be significantly associated based on adjusted hazard ratios.
Ethical Consideration
Ethical approval to carry out the current study was obtained from Kilimanjaro Christian Medical College Clinical Research Ethics and Review Committee (KCMU-CREC) with clearance number PG 127/2023. For practical purposes, oral consent was obtained since the interviews took place shortly after the women had given birth. The midwife-nurse provided each woman with verbal information about the birth registry, the required data, and its intended use for research purposes. Women were informed that the goal was to generate new knowledge that would ultimately benefit mothers and children in the future. Participation was entirely voluntary and did not affect the care they would receive. After providing consent, mothers retained the right to decline answering specific questions. To ensure privacy and confidentiality, unique identification numbers were used to link mothers with their children’s records. No personally identifiable information was stored in any electronic database; only unique identification numbers were used. Midwives also took appropriate measures to maintain privacy during the interviews.
Results
Characteristics of the Mothers With Asphyxiated Neonates
The mean (SD) age of 7,783 mothers who gave birth to asphyxiated neonates was 29(7) years. Majority (73.5%) of mothers who gave birth to asphyxiated neonates aged 20-34 years. Almost half (48.3%) of the mothers with asphyxiated neonates were residing in urban. Three-fifths (61.3%) of the mothers with asphyxiated neonates had primary education. Majority (85.1%) of mothers who gave birth to asphyxiated neonates were married/cohabiting. Large proportion (76.6%) of mothers who gave birth to asphyxiated neonates were Christians by religion. Majority (76.9%) of mothers with asphyxiated neonates were employed. Almost two-fifths (38.7%) of mothers who gave birth to asphyxiated neonates were referred for delivery. Almost all (97.9%) mothers with asphyxiated neonates attended ANC but majority (78.1%) started late and more than three-tenths (34.9%) had less than four visits (Table 2).
Characteristics of the Mothers With Asphyxiated Neonates Admitted at KCMC (N = 7,783).

n = 7735; bn = 7753 cn = 7725; dn = 7732; en = 7715; fn = 7236; gn = 7747; hn = 7245.
Frequencies (n) do not tally to the total due to missing values in these variables.
Characteristics of Neonates With Birth Asphyxia Admitted at KCMC
Slightly more than half (53.7%) of the study participants were males. Majority of the Asphyxiated neonates were born term (76.9%). Almost two-third (65.6%) of the asphyxiated neonates were born with normal birth weight. Majority (76.4%) of the study participants had their mother’s pregnancy induced and more than half (61.1%) of the asphyxiated neonates were born vaginally. Most of the asphyxiated neonates (92.9%) presented with vertex (Table 3).
Characteristics of Neonates With Birth Asphyxia Admitted at KCMC (N = 7,783).

n = 7679; bn = 7648; cn = 7681; dn = 7229; en = 7670.
Frequencies (n) do not tally to the total due to missing values in these variables.
Clinical Characteristics of Neonates With Birth Asphyxia Admitted at KCMC
Majority (78.9%) of the asphyxiated neonates at KCMC did not receive aminophylline. Majority (74.9%) of the asphyxiated neonates did receive oxygen. Large proportion (73.5%) of the asphyxiated neonates were resuscitated. Additionally, three-fifth (61.7%) of asphyxiated were staged moderate HIE (Table 4).
Clinical Characteristics of Neonates With Birth Asphyxia Admitted at KCMC (N = 7,783).

n = 7736.
Frequencies (n) do not tally to the total due to missing values in these variables.
Trends of In-hospital Survival Among Asphyxiated Neonates Admitted at KCMC From 2000 to 2022
The overall finding from this study showed significant increase in the trends of survival among neonates who sustained birth asphyxia from 2000 to 2022 the increase was from 68% to 80% respectively (p-value < .001). There was decline in trend from 2000 to 2003 from 68% to 62% respectively. In the years 2004 up until 2008 the proportions of survival from birth asphyxia were relatively constants and small ranging from 69% to 70%. In the years 2009 to 2018 there was gradual increase in proportions of survival, raising from 73% to 90% respectively. There was significant decrease in proportion of survival to 78% in 2020 then remained fairly low in 2021 at 76% before its rise to 80% in 2022 (Figure 3).

Trends of in-hospital survival among asphyxiated neonates admitted at KCMC from 2000 to 2022.
Median Survival Time of Neonates Who Sustained Birth at KCMC From 2015 to 2022
The median survival time of neonates who sustained birth asphyxia from 2015 to 2022 at KCMC was found to be 4 days (95% CI:3.0-6.0) (Figure 4).

Overall Kaplan Meier survival estimate.
In-hospital Survival Rate of Neonates With Birth Asphyxia admitted at KCMC From 2015 to 2022
A total of 1,562 neonates were followed for 7178.7 person-days with a minimum of 1 day and a maximum of 28 days, the overall survival rate was 195.32/ 1000 person-days-of observation (95% CI: 190.57, 200.18).
Asphyxiated male neonates had a higher survival rate of 198.6 per 1,000 person-days of observation (95% CI: 192.0, 205.4) compared to their female counterparts. Similarly, term neonates with birth asphyxia exhibited a higher survival rate of 208.6 per 1,000 person-days of observation (95% CI: 198.3, 219.5) compared to preterm neonates. In contrast, low birth weight neonates with birth asphyxia recorded a lower survival rate of 184.6 per 1,000 person-days of observation (95% CI: 179.0, 190.4) compared to those with normal birth weight. Neonates delivered after induced labor demonstrated a higher survival rate of 207.2 per 1,000 person-days of observation (95% CI: 196.6, 218.4) compared to those delivered without induction. Additionally, vaginally delivered asphyxiated neonates had a higher survival rate of 163.9 per 1,000 person-days of observation (95% CI: 157.6, 170.4) compared to those delivered via cesarean section. Neonates presenting with a vertex position had a survival rate of 195.7 per 1,000 person-days of observation (95% CI: 190.8, 200.8) compared to those with non-vertex presentations. Furthermore, asphyxiated neonates who received aminophylline or oxygen therapy showed higher survival rates of 225.5 per 1,000 person-days of observation (95% CI: 219.4, 231.7) and 221.2 per 1,000 person-days of observation (95% CI: 215.0, 227.5), respectively, compared to those who did not receive these interventions. Resuscitated neonates had a survival rate of 220.5 per 1,000 person-days of observation (95% CI: 214.4, 226.8), and those diagnosed with mild hypoxic-ischemic encephalopathy (HIE) had the highest survival rate of 248.6 per 1,000 person-days of observation (95% CI: 236.5, 261.4) compared to neonates with severe HIE (Table 5).
In-hospital Survival Rate of Neonates With Birth Asphyxia Admitted at KCMC From 2015 to 2022 (N = 1562).

Mantel-cox P-value for effect modification, PDARs- Person days at Risk, SR- Survival rate, CI – Confidence interval.
Predictors of In-hospital Survival Among Asphyxiated Neonates Admitted at KCMC From 2015 to 2022
Adjusted analysis for predictors of survival among asphyxiated neonates is found in Table 6. Antenatal care (ANC), gestation age, birth weight, mode of delivery, Aminophylline, oxygen, resuscitation and HIE stages were all independent significant predictors survival of the asphyxiated neonates in an adjusted Weibull regression model at a p-value of .05.
Predictors of In-hospital Survival Among Asphyxiated Neonates Admitted at KCMC From 2015 to 2022 (N = 1562).

Significant (P-value < .05). **significant (p-value < .001) and HR = 1 is reference variable.
Asphyxiated neonates whose mother did not attend ANC were found to have 26% less hazards of survival compared to those who did (AHR: 0.74; 95% CI: 0.62-0.89). Asphyxiated neonates who were delivered prematurely had 19% less hazards of survival from birth asphyxia compared to term neonates (AHR: 0.81; 95% CI: 0.76-0.86). Additionally, asphyxiated neonates with normal birth weight were found to have 19% more hazards of survival from asphyxia compared to those with low birth weight (AHR: 1.19; 95% CI: 1.12-1.26). Furthermore, asphyxiated neonates who were delivered vaginally had 70% higher hazards of survival (AHR: 1.69; 95% CI: 1.60-1.78) compared those delivered by cesarean section.
Moreover, asphyxiated neonates who were administered aminophylline had 60% higher hazards of survival compared to those who were not put into aminophylline (AHR: 1.56; 95% CI: 1.52-1.60), asphyxiated neonates who were put in oxygen had 32% higher hazards of survival compared to those who were not (AHR: 1.32; 95% CI: 1.23-1.42). Neonates who were resuscitated had 32% higher hazards of survival compared to their counterparts (AHR: 1.32; 95% CI: 1.24-1.42). Lastly neonates who had mild birth asphyxia had 85% higher hazards of survival compared to those who had severe birth asphyxia (AHR: 1.85; 95% CI: 1.79-1.91).
Discussion
This study aimed to determine the trend, rate and predictors of survival among asphyxiated neonates at zonal referral hospital in Kilimanjaro, Tanzania. The study found a significant overall increase in proportion of survival of birth asphyxia trends over the analyzed period (p-value < .001). The study also revealed a survival rate of asphyxiated neonates of 195.3 per 1000 person days at risk with median survival time of 4 days. Antenatal care (ANC), gestation age, birth weight, mode of delivery, Aminophylline, oxygen, resuscitation and HIE stages were predictors significantly associated with survival of the asphyxiated neonates.
Finding from this study showed significant increase in the trends of survival among asphyxiated neonates from 2000 to 2022, with initial decline due to poor maternal and neonatal healthcare practices and possibly due shortage of skilled healthcare workers from 2000 to 2003. A stable phase in 2004 to 2008 suggests consistent healthcare quality. A gradual improvement was observed between 2009 and 2018 which can be linked to Help Baby Breath program which was piloted and executed between those years. 21 This program was said to be reduce Early Neonatal Mortality by 47%, and reduce fresh still birth by 24% 30 and the guidelines for neonatal resuscitation by the American Academy of Pediatrics strongly recommend undergoing certification and refresher training in neonatal resuscitation skills every 2 years for healthcare providers. 3 Lastly, a drop was observed in 2020 and 2021, perhaps as a result of challenges or pressure in the healthcare system due to COVID-19 pandemic, which disrupted healthcare services world-wide, reduced access to prenatal care and increased stress on both healthcare workers and pregnant. 31
This study exhibited the asphyxiated neonates’ median survival time to be 4 days (95% CI:3.0-6.0). While this reflects some neonates recover relatively quickly, it also underscores the challenges faced in managing birth asphyxia and it additionally points out the necessity of improving early diagnosis and immediate care practice to potentially shorten survival time in low-resource settings. This is in contrast to the findings of studies conducted in Ethiopia where the median survival time were 7 days32,33 and 8 days.16,29 The difference in sample size, study duration and study settings account for discrepancies.
The overall survival rate in this study was found to be 195/1000 person-days. Previous studies have reported the survival rate of 100/1000 person days of observation 16 and 99/1000 person days of observation. 20 These discrepancies may be linked to differences in the scope, sites and study duration. The observed differences in survival rate among neonates with birth asphyxia can also be explained by factors like differences in healthcare infrastructure, availability of specialized neonatal care facilities and variations in perinatal care practices across different geographical regions.
While several studies16,34,35 have proven that prematurity can result in poor neonatal prognosis, in line with these studies, the current study showed that asphyxiated neonates who were born prematurely had less hazards of survival compared to their counterparts. This signifies that term and post-term neonates may have better resilience in coping with harsh situations including hypoxemia, metabolic acidosis and other challenges associated with asphyxia. 1 Possible explanation is that, their immature systemic systems which make it more difficulty to respond appropriately to hypoxic and harsh conditions, moreover, their raised susceptibility to medical complications, such as respiratory distress syndrome and intraventricular hemorrhage. 36 Lastly due to their tiny size and lack of brown adipose tissue, newborns are more susceptible to hypothermia, which exacerbates hypoxia 1 and hence lower hazards of survival.
Vaginally delivered asphyxiated neonates showed higher hazards of survival from birth asphyxia compared to those delivered via cesarean section, as supported by evidenced research conducted in Japan, 37 Nepal 38 and Ethiopia 39 along with findings from a multinational survey 40 which reported similar findings. In the event of a vaginal delivery, the fetal chest’s compression and release during its passage down the birth canal might facilitate the expulsion of lung fluid and encourage breathing efforts, 41 which may help newborns who are experiencing birth asphyxia adjust to life outside the womb hence better survival. Neonates delivered by cesarean section are more likely to experience transient tachypnea of the newborn (TTN), or wet lung regardless of whether the cesarean delivery was preceded by labor or not. 42
Asphyxiated neonates who were given aminophylline had higher hazards of survival. Aminophylline has bronchodilator characteristics and can stimulate the central nervous system and respiratory muscles. 43 Its potential benefits in neonatal care, especially for asphyxiated infants are significant. The higher hazards of survival found in the study could be ascribed to aminophylline’s ability to improve respiratory function and increase oxygen delivery to tissues, hence minimizing the negative effects of hypoxia. Furthermore, aminophylline’s anti-inflammatory effects may minimize cerebral edema and protect brain tissues from hypoxic-ischemic injury, resulting in a faster and more effective survival. 44 This finding emphasizes the relevance of using aminophylline as a therapeutic option in neonatal intensive care units (NICUs) to treat birth asphyxia. Similar findings were reported by previous studies.16,20,45
As reported from previous studies16,20,45 oxygen therapy was one of the predictors of survival among asphyxiated neonates, birth asphyxia causes hypoxia, a condition in which insufficient oxygen delivery to the brain and other essential organs can result in serious consequences.46 -48 Oxygen should be administered promptly after birth if birth asphyxia is suspected so as to offset these effects and stabilize the neonate’s condition. The fundamental advantage of oxygen treatment is its capacity to rapidly boost arterial oxygen saturation, ensuring that essential organs, including the brain, receive enough oxygen to operate normally and recover from hypoxic insults. 49 Early and proper oxygen treatment can reduce the risk of hypoxic-ischemic encephalopathy (HIE). 44
Resuscitation increases the hazards of survival for asphyxiated neonates. It ensures that oxygenated blood reaches the brain and other essential organs, lowering the risk of hypoxic-ischemic encephalopathy (HIE) and other consequences caused by prolonged oxygen deprivation. 50 Research has shown that infants who undergo timely and professional resuscitation have better neurological outcomes and increased survival. 51 Newborns who require prompt resuscitation after birth are typically hypoxic, with respiratory and metabolic acidosis. Furthermore, the difficulties of doing efficient resuscitation paired with bad technique can result in an unsatisfactory clinical response. 52 These findings are in line with previous studies16,29,45 and the consistency can be explained by similar characteristics of the study participants and similar analytical approach.
Strengths and Limitations
The strength of this study lies in the fact that it utilized data from the KCMC medical birth registry, known for its large sample size and over two decades of data, providing robust statistical power and the ability to assess trends in survival from birth asphyxia over time. It was the first in Tanzania to employ a retrospective cohort design with advanced statistical analyses, including time-to-event methodological approach. The findings contribute to the literature on neonatal birth asphyxia by highlighting survival trends, median survival time, survival rates, and key predictors. The study had limitations which included, using secondary data posed quality challenges, including missing exposure variables. Being a single-center, hospital-based study, the findings are not generalizable to larger populations. Additionally, the study lacked long-term follow-up data for neonates referred to higher-level facilities, leaving some survival outcomes untracked.
Conclusion and Recommendation
The study revealed a significant increase in overall survival trends from birth asphyxia but noted a concerning decline in recent years. The overall survival rate was 195.32 per 1000 person-days with a median survival time of 4 days, influenced by factors like antenatal care, gestation age, birth weight, mode of delivery, and medical interventions. These findings highlight the need for promptly assessment and stabilization of airway, breathing and circulation, initiation of resuscitation, provision of oxygen, administration of medications such as aminophylline to neonates who are diagnosed with birth asphyxia to improve neonatal outcomes. Recommendations include establishing robust monitoring systems, improving prenatal screening and antenatal care, training in neonatal resuscitation, raising awareness among expectant mothers, and conducting future research with longer follow-up periods and broader national representation.
Footnotes
Acknowledgements
We would like to express our gratitude to the midwives who collected the data and to all the women and children whose information made this study possible. We also thank the Birth Registry staff for entering this data into the electronic system. Additionally, we appreciate the Centre for International Health at the University of Bergen in Norway and the Department of Obstetrics and Gynecology at KCMC hospital in Tanzania for establishing the KCMC medical birth registry, which enabled the data collection for this study.