
Abstract
Objective
Length of hospital stay is a sensitive indicator of short-term prognosis. In this retrospective study, we investigated how pancreas preservation time affects length of hospital stay after pancreas transplantation.
Methods
Patients receiving pancreas transplantation (1998.7–2018.6) were identified from the Scientific Registry of Transplant Recipients database and grouped according to pancreas preservation time. We analyzed the relationship of pancreas preservation time with graft and patient survival and prolonged length of stay (PLOS; i.e., hospital stay ≥20 days).
Results
We included 18,099 pancreas transplants in the survival analysis. Pancreas preservation time >20 hours had a significantly higher risk of graft failure than 8 to 12 hours. Pancreas preservation time was not significantly associated with patient survival. We included 17,567 pancreas transplants in the analysis for PLOS. Compared with 8 to 12 hours, pancreas preservation time >12 hours had a significantly higher PLOS risk, which increased with increased pancreas preservation time. In simultaneous pancreas–kidney transplantation, we also found that pancreas preservation time was positively associated with PLOS risk with pancreas preservation time >12 hours.
Conclusion
Pancreas preservation time is a sensitive predictor of PLOS. Transplant centers should minimize pancreas preservation time to optimize patient outcomes.
Keywords
Introduction
Pancreas transplantation in patients with diabetes can improve quality of life and reduce the risk of diabetic complications. The first pancreas transplantation was performed in 1966. 1 Since then, there have been many advances in surgical techniques and in the use of immunosuppressive agents; thus, pancreas transplantation is currently an accepted method for the treatment of diabetes.2,3 However, pancreas transplantation is a complex procedure that is associated with many postoperative complications.3–6 The quality of the donor graft 7 and the pancreas preservation time are important factors influencing the success of transplantation.8,9 Prolonged pancreas preservation time is associated with graft failure and technical failure; consequently, prolonged pancreas preservation time has been included in the Pancreas Donor Risk Index (PDRI), used to predict risk of graft failure.8,10
Length of stay (LOS) is an important indicator of short-term prognosis and is also associated with use of medical resources.11–14 Understanding of the impact of pretransplant factors on LOS can help predict the risk of prolonged length of stay (PLOS) and facilitate rational use of medical resources. The aim of this retrospective cohort study was to determine the impact of pancreas preservation time on PLOS.
Methods
Data source
This study was based on the Scientific Registry of Transplant Recipients (SRTR), which includes data on all donors, wait-listed candidates, and transplant recipients in the United States, submitted by members of the Organ Procurement and Transplantation Network (OPTN). The Health Resources and Services Administration (HRSA), U.S. Department of Health and Human Services, oversees the activities of the OPTN and SRTR contractors. 15 This was a retrospective study and did not involve patient-specific identifying information; therefore, ethics committee approval and patient consent were not required.
Study sample
Patients (n = 24,397) registered in the SRTR database from July 1998 to June 2018 were eligible for inclusion in this retrospective analysis. Patients were excluded if they 1) had a history of organ transplantation other than kidney transplantation for pancreas transplantation, or a history of any organ transplantation for pancreas–kidney transplantation (n = 2347); 2) were aged <18 years (n = 558); 3) had received a living donor transplant (n = 27); 4) had received simultaneous transplant with other organs besides the pancreas and kidneys (n = 679); or 5) the data on pancreas preservation time were unavailable (n = 2687). For the analysis of PLOS and postoperative complications, we further excluded patients with missing discharge data (n = 62) and those who underwent re-transplantation (n = 51) or died (n = 419) within 20 days of transplantation.
We analyzed recipient and donor characteristics considered potential confounding factors (Table 1). Recipient factors included the following: age; sex; body mass index (BMI); ethnicity (White, Black, Hispanic, Asian, and other); human leukocyte antigen mismatch; panel-reactive antibody; years since diabetes onset; exocrine drainage (enteric drainage, bladder drainage, and other); endocrine drainage (systemic system, portal system, and other); transplant year (1998.7–2003.6, 2003.7–2008.6, 2008.7–2013.6, 2013.7–2018.6); transplant center (n = 165) ranked according to the total transplant volume of 1998.7–2018.6 and divided into tertiles (low-volume [n = 119], medium-volume [n = 33], and high-volume centers [n = 13]); and type of transplant (pancreas after kidney [PAK], pancreas transplant alone [PTA], and simultaneous pancreas–kidney [SPK] transplantation).
Potential confounding factors.

BMI, body mass index; HLA, human leukocyte antigen; PRA, panel-reactive antibody; DM, diabetes mellitus; DCD, donation after cardiac death.
Donor factors included the following: age; sex; BMI; ethnicity (White, Black, Hispanic, Asian, and other); donation after cardiac death; cause of death (anoxia, cerebrovascular accident, head trauma, and other); and serum creatinine level. Post-transplant complications included infection, pancreatitis, and leak (as recorded in the SRTR database, defined as occurring after transplantation and before discharge).
To assess how pancreas preservation time was associated with patient and pancreatic graft survival and PLOS, patients were separated into seven groups according to pancreas preservation time (0–4, 4–8, 8–12, 12–16, 16–20, 20–24, and > 24 hours). The 8–12-hour group was considered the reference group (according to the nominal time of the PDRI). 4 The date of patient death was determined from the SRTR. Pancreas re-transplantation, pancreatic graft resection, or reuse of insulin were considered evidence of graft failure. PLOS was defined as post-transplant hospital stay ≥20 days (the 90th percentile of hospital stay).
Statistical analysis
We used IBM SPSS version 25.0 (IBM Corp, Armonk, NY, USA) for the statistical analysis. Continuous variables were expressed as mean ± standard deviation and were compared using the Student t-test and Mann–Whitney test. Categorical variables were expressed as counts or percentages and were compared with the chi-square test. Univariate and multivariate Cox regression analyses were performed to estimate hazard ratios (HRs) and 95% confidence intervals (CIs). Univariate and multivariate logistic regression analyses were performed to estimate risk (odds ratios [ORs] with 95% CIs) of PLOS and postoperative complications. P ≤ 0.05 was considered statistically significant.
Results
Characteristics of the study population
A total of 18,099 pancreas transplants (2641 PAK, 1475 PTA, and 13,983 SPK) met our inclusion criteria and were included in the analysis. The mean patient age was 41.5±8.7 years, and 59.7% (10,814) of patients were male. The mean pancreas preservation time was 12.2 ± 5.6 hours. Mean follow-up time was 6.9 ± 5.0 years. A total of 17,567 pancreas transplants (2558 PAK, 1393 PTA, and 13,616 SPK) were included in the analysis for PLOS. Mean LOS was 11.4 ± 13.2 days. PLOS (≥20 days) was seen in 9.7% of patients. Table 2 shows the general characteristics of recipients and donors and the proportion of missing data.
Characteristics and missing values.

SD, standard deviation; BMI, body mass index; HLA, human leukocyte antigen; PRA, panel-reactive antibody; DM, diabetes mellitus; DCD, donation after cardiac death; PAK, pancreas after kidney transplantation; PTA, pancreas transplant alone; SPK, simultaneous pancreas–kidney transplantation.
Pancreatic graft survival
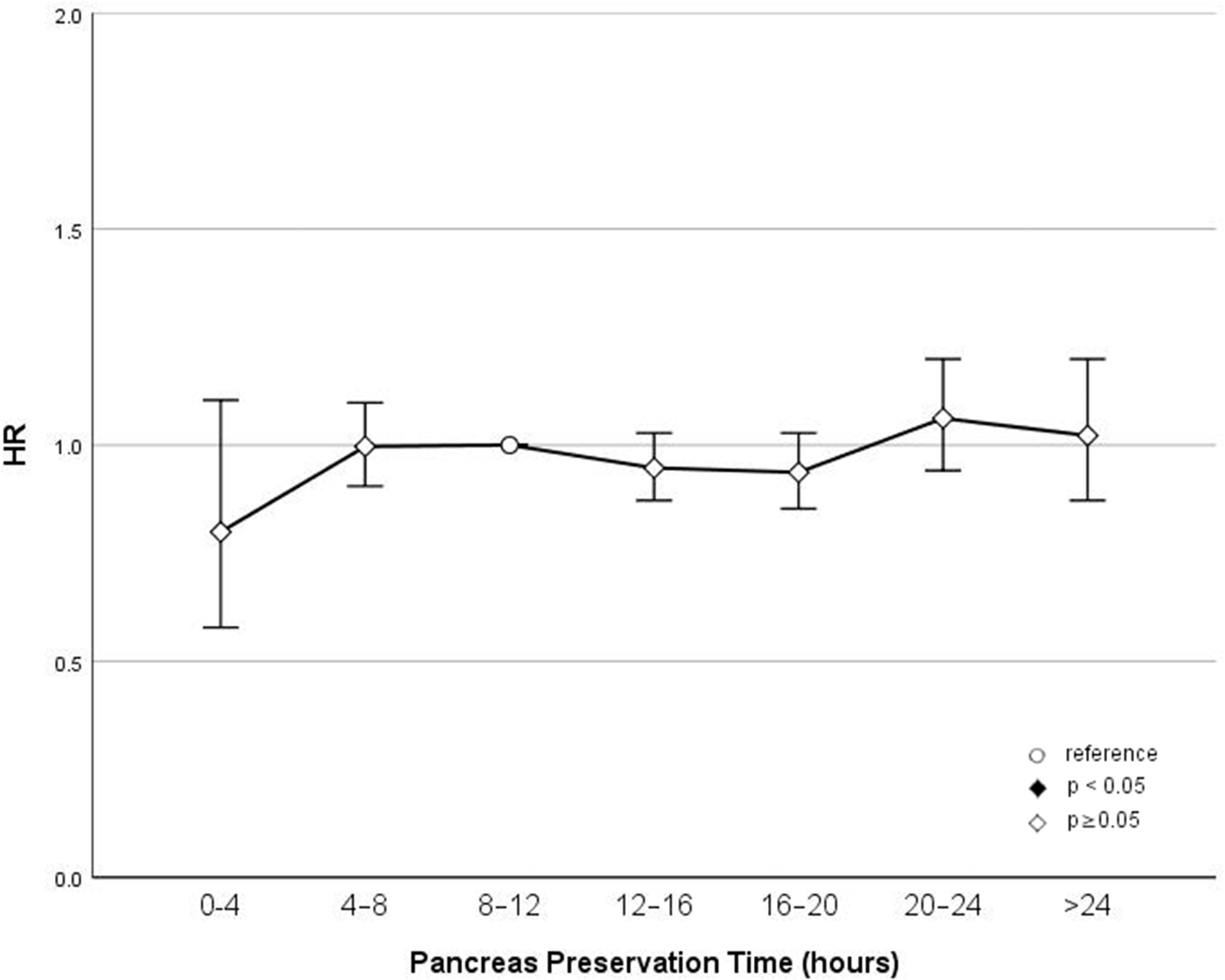
In univariate and multivariate Cox regression analysis, we found that pancreas preservation time >20 hours was significantly associated with increased risk of graft failure compared with 8–12 hours. The HR was 1.164 (95% CI: 1.031–1.315; P = 0.014) for the 20–24-hour group and 1.241 (95% CI: 1.057–1.456; P = 0.008) for the >24-hour group. There was no statistical difference in the other groups compared with the reference group. The HR was 0.983 (95% CI: 0.746–1.307) in the <4-hour group, 0.946 (95% CI: 0.860–1.041) in the 4–8-hour group, 1.034 (95% CI: 0.953–1.122) in the 12–16-hour group, and 1.075 (95% CI: 0.979–1.181) in the 16–20-hour group. Thus, the risk of graft failure was found to be associated with pancreas preservation time. Pancreas preservation time > 20 hours was also significantly associated with an increased risk of graft failure. (Figure 1).

Pancreas preservation time and graft survival.
Patient survival
In univariate and multivariate Cox regression analysis, we found that pancreas preservation time was not associated with patient survival (Figure 2).
Pancreas preservation time and patient survival.
Prolonged length of stay (PLOS)
In univariate and multivariate Cox regression analysis, we found that pancreas preservation time > 12 hours was significantly associated with increased risk of PLOS, as compared with 8 to 12 hours. The OR was 1.151 (95% CI: 1.003–1.320; P = 0.045) for 12 to 16 hours, 1.333 (95% CI: 1.135–1.565; P < 0.001) for 16 to 20 hours, 1.487 (95% CI: 1.202–1.840; P < 0.001) for 20 to 24 hours, and 1.961 (95% CI: 1.528–2.518; P < 0.001) for > 24 hours. There was no statistical difference in the other groups compared with the reference group. The HR was 0.948 (95% CI: 0.597–1.505) for < 4 hours and 0.868 (95% CI: 0.738–1.020) for 4 to 8 hours (Figure 3).

Pancreas preservation time and prolonged length of stay.
PLOS in simultaneous pancreas–kidney (SPK) transplantation
In univariate and multivariate logistic regression analysis, we also found that pancreatic preservation time > 12 hours was significantly associated with an increased risk of PLOS. compared with 8 to 12 hours in SPK transplantation. The OR was 1.194 (95% CI: 1.022–1.394; P = 0.025) in the 12–16-hour group, 1.371 (95% CI: 1.140–1.649; P <.001) in the 16–20-hour group, 1.587 (95% CI: 1.234–2.040; P < 0.001) in the 20–24-hour group, and 2.122 (95% CI: 1.593–2.827; P < 0.001) in the > 24-hour group. There was no statistical difference in the other groups compared with the reference group. The HR was 0.790 (95% CI: 0.442–1.414) for < 4 hours and 0.833 (95% CI: 0.694–1.000) for 4 to 8 hours (Figure 4).

Pancreas preservation time and prolonged length of stay in simultaneous pancreas–kidney (SPK) transplantation.
Discussion
This retrospective analysis of SRTR data showed that pancreas preservation time was associated with graft failure and prolonged hospital stay; however, pancreas preservation time was not associated with patient survival.
Pancreas preservation time is an important factor affecting the prognosis of pancreas transplantation. Several studies have shown that with pancreas preservation time >12 hours, the risk of transplant failure is significantly increased.8,16,17 Additionally, pancreas preservation time has been included in the PDRI calculation formula, with 12 hours set as the cutoff value. Pancreas preservation time > 12 hours is considered to be harmful to donor pancreas quality. 8 However, few previous studies have investigated the specific effects of different pancreas preservation times on the prognosis of pancreas transplantation. In this study, patients were divided into 4-hour groups according to pancreas preservation time, with 8 to 12 hours considered the reference group. We then investigated the influence of different pancreas preservation times on the prognosis of transplantation. Our study findings demonstrated that pancreas preservation time > 20 hours was significantly associated with an increased risk of graft failure and that the longer the pancreas preservation time, the higher the risk. With pancreas preservation time 0 to 20 hours, the risk of transplant failure was not significantly different from that of the reference group.
We did not find an association between pancreas preservation time and patient survival. A previous study also found no significant difference in the survival rate between patients with diabetes receiving pancreas transplantation and insulin therapy. 18 We believe that this might be owing to post-transplantation patients with graft failure who survived using insulin therapy.
The length of postoperative hospital stay is an important indicator to evaluate the short-term prognosis of patients. Prolonged hospital stay often means slow postoperative recovery. Few studies have focused on the effect of pancreas preservation time on postoperative hospital stay. In this study, we found that pancreas preservation time was closely related to PLOS, and this relationship was stronger than that between pancreas preservation time and graft survival. With pancreas preservation time > 12 hours, the risk of PLOS increased significantly with pancreas preservation time. The risk of PLOS was highest (OR =1.961, 95% CI: 1.528–2.518; P < 0.001) with pancreas preservation time > 24 hours. When the pancreas preservation time was 0 to 8 hours, the risk of PLOS was not significantly different from that of the reference group (8–12 hours). We obtained similar results in patients with SPK transplantation. Therefore, we believe that with pancreas preservation time < 12 hours, patients can remain within the normal postoperative length of hospital stay. Further, prolonged hospital stay often means higher costs.11,12,19 Therefore, we can predict a patient's hospitalization duration using pancreas preservation time, to rationally allocate medical resources and hospitalization costs.
Several studies have found that the incidence of postoperative complications is significantly increased in patients with a prolonged postoperative hospital stay. Librero et al. 20 showed that patients with postoperative complications were hospitalized twice as long as those without complications. Our study also found that the incidence of postoperative complications was significantly higher in patients with a prolonged hospital stay than in those with a normal LOS (OR = 9.085, 95% CI = 8.020 – 10.290; P < 0.001, Figure 5). This may be owing to an increase in postoperative complications, leading to a prolonged hospital stay. 13 However, only complications of infection, leak, and pancreatitis are recorded in the SRTR database; therefore, we were unable to conduct further comprehensive analysis.
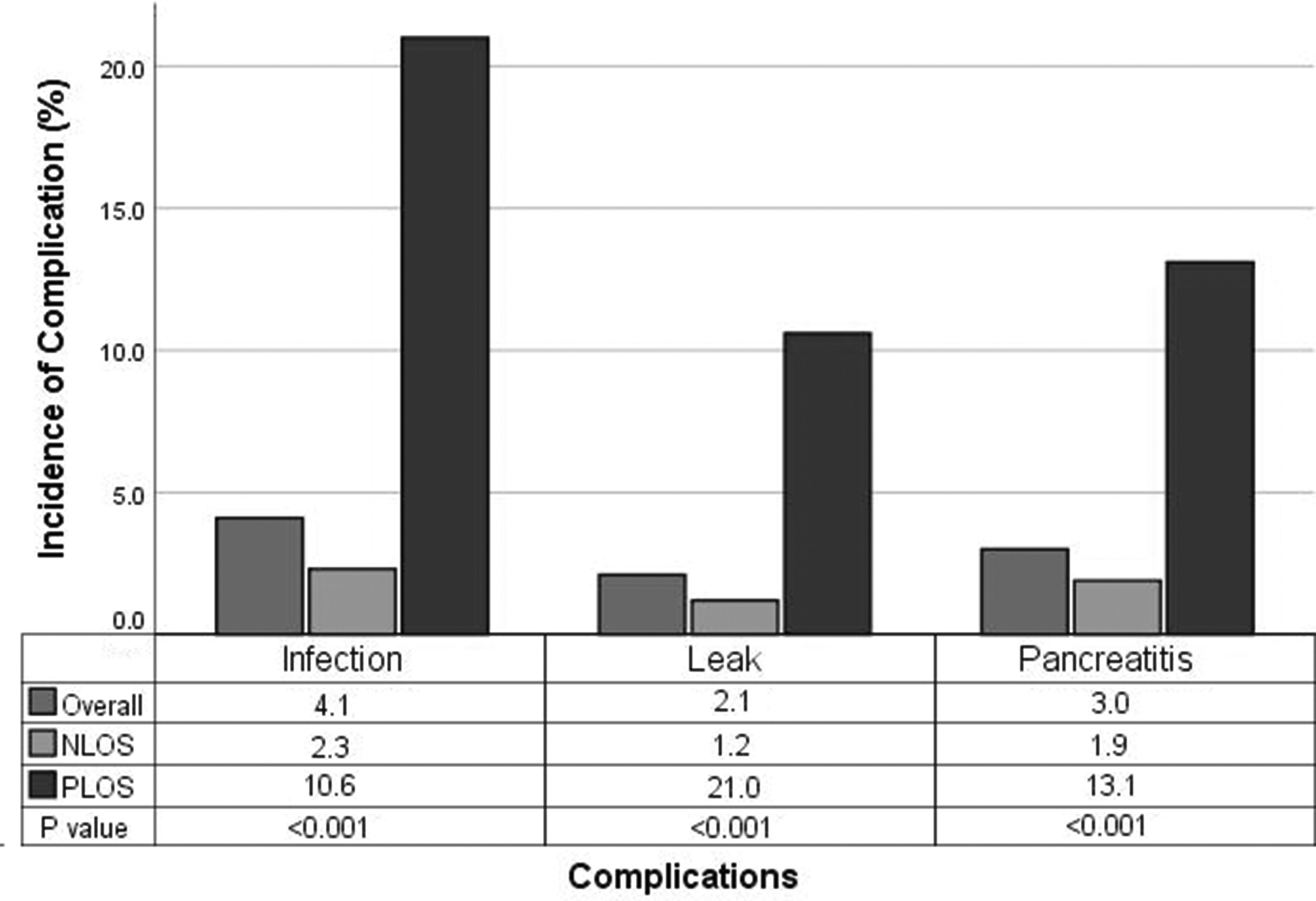
Post-transplant complications in patients with prolonged length of stay (PLOS) and normal length of stay (NLOS).
In this study, we analyzed 20 years of pancreas transplantation data. During these years, pancreas transplantation has undergone considerable advancement. Therefore, we included the pancreas transplantation procedure and year of transplantation as confounding factors in the analysis. Previous studies have shown that pancreatic bladder drainage tends to cause more urinary complications, so its application has been gradually reduced.3,21 The pancreatic jejunal drainage procedure is more compatible with normal human physiology; therefore, most transplant centers currently use pancreatic jejunal drainage as the procedure of choice. Our results showed an increasing proportion of intestinal drainage and a decrease in the proportion of bladder drainage as the type of exocrine pancreatic drainage during recent years (P < 0.05, Figure 6). However, we found that the proportion of systemic drainage and portal vein drainage in endocrine drainage has not changed much. This may be because there is no significant difference in postoperative complications and survival rates between systemic drainage and portal drainage.22,23
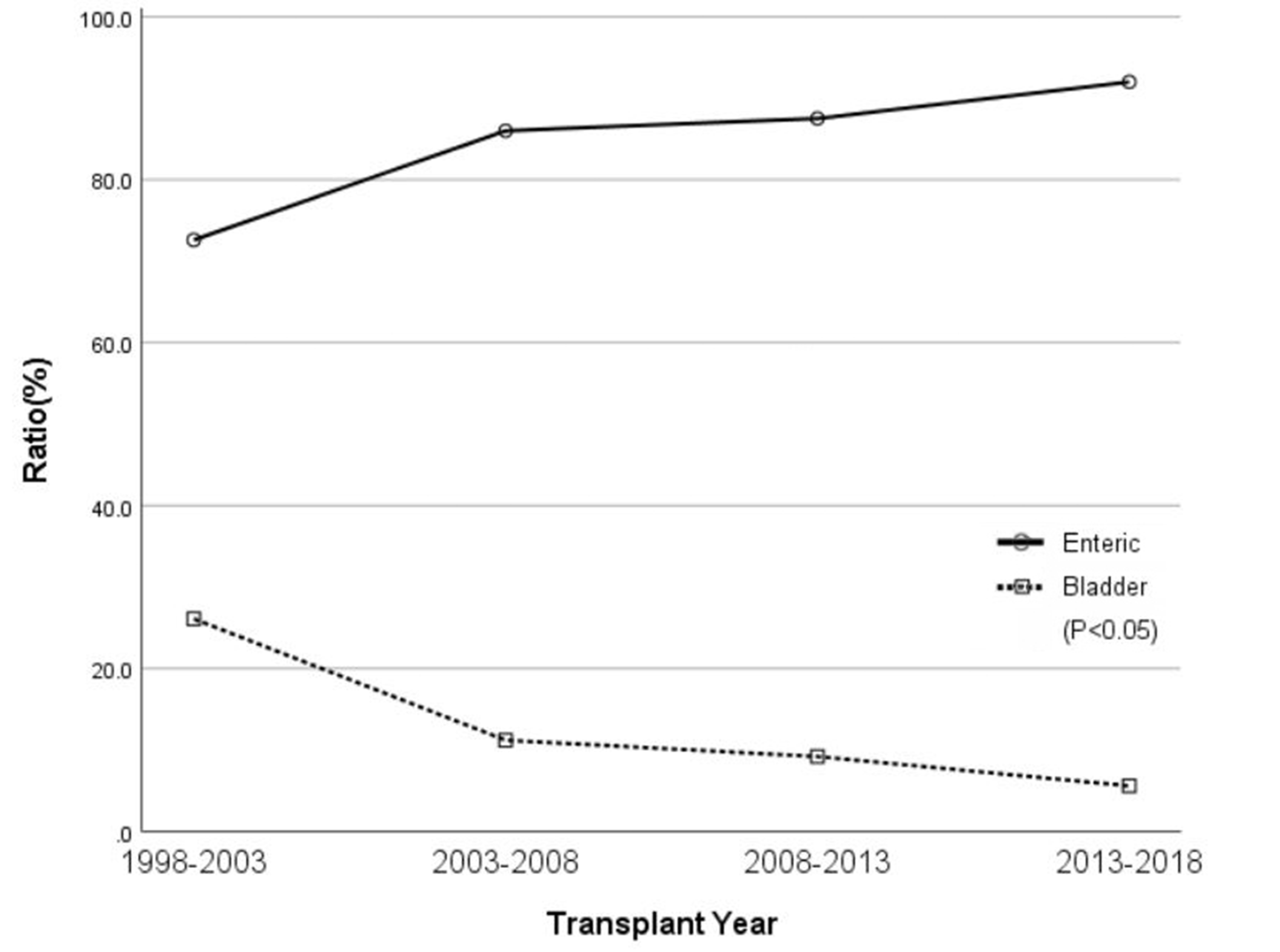
Processes of pancreatic exocrine drainage.
In this study, we stratified transplant centers according to transplant volume. We found that low-volume centers had the highest incidence of patient PLOS whereas high-volume centers had the lowest incidence of PLOS. The reasons for this may be complex. We believe that high-volume centers tend to have more comprehensive multidisciplinary support and can better manage post-transplant complications whereas low-volume centers may have some limitations in this regard. Previous studies have also found a significantly higher incidence of graft loss after transplantation among patients in low-volume centers. 24
Pancreas preservation time includes warm ischemia, cold ischemia, and anastomosis time. The pancreas organ is highly sensitive to ischemia-reperfusion injury, especially warm ischemic injury. 25 Transportation time is the main reason for the increase in pancreas cold ischemia time. 26 The best outcomes of pancreas transplantation can be achieved with cold ischemia time < 12 hours. 27 Therefore, transplant centers should ai to improve their pancreas allocation policy so as to reduce the distance between donor and recipient, thereby reducing the transit time of the donor pancreas.
This study has some limitations. First, this was a retrospective analysis of information extracted from a database; therefore, the presence of unknown confounders cannot be ruled out. Second, the pancreas preservation time in this study included pancreatic warm ischemia time, cold ischemia time, and surgical anastomosis time. These have different injurious effects on the pancreas, 28 but detailed data were not available for further analysis. Third, in this study, we defined PLOS as ≥20 days (90th percentile of hospital stay); however, this is a subjective cutoff.
Conclusion
Our study findings showed that the risk of PLOS after pancreas transplantation increased with increased pancreas preservation time. Transplant centers should strive to minimize pancreas preservation time, to optimize patient outcomes and reduce medical costs. Patients assigned to receive a graft with a prolonged preservation time should be informed of the risks in advance.
Footnotes
Acknowledgements
The data reported here have been supplied by the Hennepin Healthcare Research Institute (HHRI) as the contractor for the Scientific Registry of Transplant Recipients (SRTR). The interpretation and reporting of these data are the responsibility of the authors and should in no way be seen as an official policy of or interpretation by the SRTR or the U.S. Government.
This study was supported by the National Natural Science Foundation of China (No.81770645), the Public Welfare Technology Application Research Plan of Zhejiang Province, China (No. 2017C33025), and the Key Research and Development Programs of Zhejiang Province (No. 2020C03057).
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.