
Abstract
Introduction:
Recently, stroke is becoming the major public health problem in developing countries including Ethiopia. Atrial fibrillation patients are the most vulnerable group for the occurrence of stroke. Knowing the predictors and being aware for it is important for preventing severe complications and death. Therefore, the aim of this study is to assess the prevalence of stroke and identifying significant predictors.
Methods:
A hospital-based cross-sectional study was performed from 1 December 2018 to 30 September 2019 at University of Gondar Referral Hospital. A total of 242 patients with atrial fibrillation were included in the study. Atrial fibrillation patients were diagnosed by using 12 lead electrocardiographic tracing, in addition to thorough medical history and physical examination and analyzed by the Modular ECG Analysis System (MEANS). We used Epi info 7 and SPSS version 22 software for data entry and analysis purpose, respectively. Both bivariable and multivariable binary logistic regression model were computed to show the relationship of dependent and independent variables.
Result:
The prevalence of stroke among atrial fibrillation patients was 19.4% (95% confidence interval (CI): 14.9–25.2). Patients with heart failure (adjusted odds ratio (AOR): 5.70, 95% CI: 2.50–13.24) and thyroid disorder (AOR: 4.98, 95% CI: 1.47–16.85) are at risk of developing stroke.
Conclusion:
The prevalence of stroke was higher compared with others studies. Patients with heart failure and thyroid disorders were the risk factor for the development of stroke; therefore, physicians and cardiologists may better to consider all these two disorders when they diagnose stroke in patients with atrial fibrillation.
Introduction
Stroke is defined as sudden onset of a focal neurological deficit lasting more than 24 hours. 1 It is classified on the basis of its etiology as either ischemic (87%) or hemorrhagic (13%). Ischemic stroke is caused by obstruction of a cerebral artery; thrombotic or atherosclerotic (50%), embolic (25%) and micro artery, “lacunar stroke,” (25%). 2 Embolic ischemic stroke is more frequent in patients with atrial fibrillation (AF) (80%), myocardial infarction, prosthetic valves, rheumatic heart disease, and larger artery atheroma (artery-artery embolus). 3
Globally, stroke is the second leading cause of death and the third leading cause of disability. 4 In 2016, there were 5.5 million deaths and 116.4 million disability-adjusted life years due to stroke. It is also a leading cause of dementia and depression, 5 of which about 70% of strokes and 87% of stroke-related deaths and disability-adjusted life years occur in low- and middle-income countries. 6 In the last four decades, the incidence has been increased by double; however, in high-income countries, it has been declined by 42%.5,7
AF is the most common cardiac arrhythmia, affecting approximately 1% of the adult population 8 and 0.4% of the overall population.9–11 Its prevalence shows a marked correlation with age, increasing from 0.5% of adult’s age 50–59 years to 9% of those in their 80s. 10 Meanwhile, the incidence of ischemic stroke in patients with AF has decreased significantly between 1980 and 2000, due to substantial increase in the use of antithrombotic therapy and a reduction in systolic blood pressure.10,12
Patients with AF experience troublesome symptoms as a result of the associated hemodynamic disturbances, but the major disturbance of this condition is caused by the increased risk of cerebrovascular accident such as transient ischemic attack (TIA) and ischemic stroke. AF increases the risk of cerebrovascular accident by allowing thrombus formation within the left atrium; if dislodged, such thrombi can obstruct the cerebral circulation, causing a thromboembolic (ischemic) stroke. 13
AF patients having advanced age are at risk of cerebrovascular accident in individuals with AF 14 and the proportion accounts from 6.7% at age 50–59 to 36.2% at age 80–89 years. 15 Current indications for anticoagulation therapy are primarily based on demographic and clinical characteristics. However, the accuracy of these risk score systems to predict ischemic stroke in AF patients is modest, which may lead to overuse of anticoagulation in low-risk patients.16,17 Several cardiac imaging-based variables have been associated with increased risk of stroke in AF patients. 18 There is no published data about the prevalence and determinants of stroke among AF patients in Ethiopia. So this study shows the burden of this rising public health problem in the study area and identifies the associated factors which may be pertinent to the local population which has paramount importance in prioritizing patients for treatment with antithrombotic medications.
Methods and materials
Study area and setting
Institution-based cross-sectional study was done from 1 November 2018 to 30 September 2019 at University of Gondar Referral Hospital, North West Ethiopia. It has more than 600 bed capacities which are used as the referral center for more than seven million catchment populations. It provides both specialty and subspecialty services, including pediatrics, surgery, gynecology, internal medicine, psychiatry, ophthalmology, and so on in its inpatient and outpatient clinics. Basic investigation modalities are available including electrocardiogram (ECG) and computed tomographic (CT) scan. Diagnosis of stroke is initially clinical and then confirmed by CT scan. 19
Population of the study with eligibility
All adult medical patients with AF at chronic follow-up and medical wards in Gondar University Referral Hospital during the study periods were the study population. Patients who do not have ECG or documented ECG finding by clinician, cannot speak, and did not have attendant were excluded in the study.
Sample size and sampling procedures
Samples were selected by consecutive sampling technique and estimated by using single population proportion formula with the following assumption. Considering prevalence of stroke among AF patients was 18% which obtained from the previous study 20 with 95% confidence level and 5% margin of error. Finally, the estimated sample size was 251.
Data collection procedures and quality control
Data were collected by using pre-tested (10% of the total sample) structural questionnaire and chart reviewing. All patients with AF were interviewed, and their charts reviewed by two medical doctors after training was given on how to interview and document relevant information on the questionnaire related to the study.
In addition to thorough medical history and physical examination, tests were made to diagnose AF and stroke. ECGs were registered using an electrocardiograph (ACTA; Esaote, Florence, Italy), digitally processed, and analyzed by the Modular ECG Analysis System (MEANS) at baseline and during follow-up exams. The MEANS software registered high sensitivity (96.6%) and specificity (99.5%) in coding arrhythmias.21–23
To check the diagnosis of AF, all ECGs with a diagnosis of AF were autonomously recoded by two research physicians blinded to the diagnosis of MEANS. In those cases where dispute between the coding physicians persisted, a cardiologist’s opinion was sought and taken as critical. Those patients who experience AF during a serious disease, resulting in death very shortly after the detection of AF, which was not the cause of the serious disease, were not considered as having AF. They were censored on the date of detection of AF. Furthermore, subjects with transitory AF during myocardial infarction or heart surgery were not included among cases.
Missing data were handled by using multiple imputation techniques. It acknowledges the uncertainty by generating a set of plausible values for each unobserved data point, resulting in complete data sets, each with one unique estimate of the missing values.
Statistical analysis
Data entry and cleaning were done by using Epi info and exported to SPSS 22 software for analysis purpose. Descriptive statistics such as frequency, mean, and median were done. Factors were independently evaluated in bivariable analysis and association was determined using cross-tabulation and crude odds ratio (COR) at 95% confidence interval (CI). All variables associated with stroke at a p-value < 0.2 on the bivariable analysis were entered into a multivariable logistic regression analysis to control confounders.
Results
Socio-demographic characteristics
From 251 patients screened for eligibility, 96.4% (242) satisfied inclusion criteria for study participation. Majority (71.5%) of them were females. The median age of patients was 53.68 (SD ± 17.35) years. More than half of them (132 (54.5%) & 140 (57.8%)) were from rural area and farmers, respectively (Table 1).
Socio-demographic characteristics of AF patients at chronic follow-up and medical wards at University of Gondar Referral Hospital, Northwest Ethiopia, 2019 (n = 242).

Medical history of AF patients
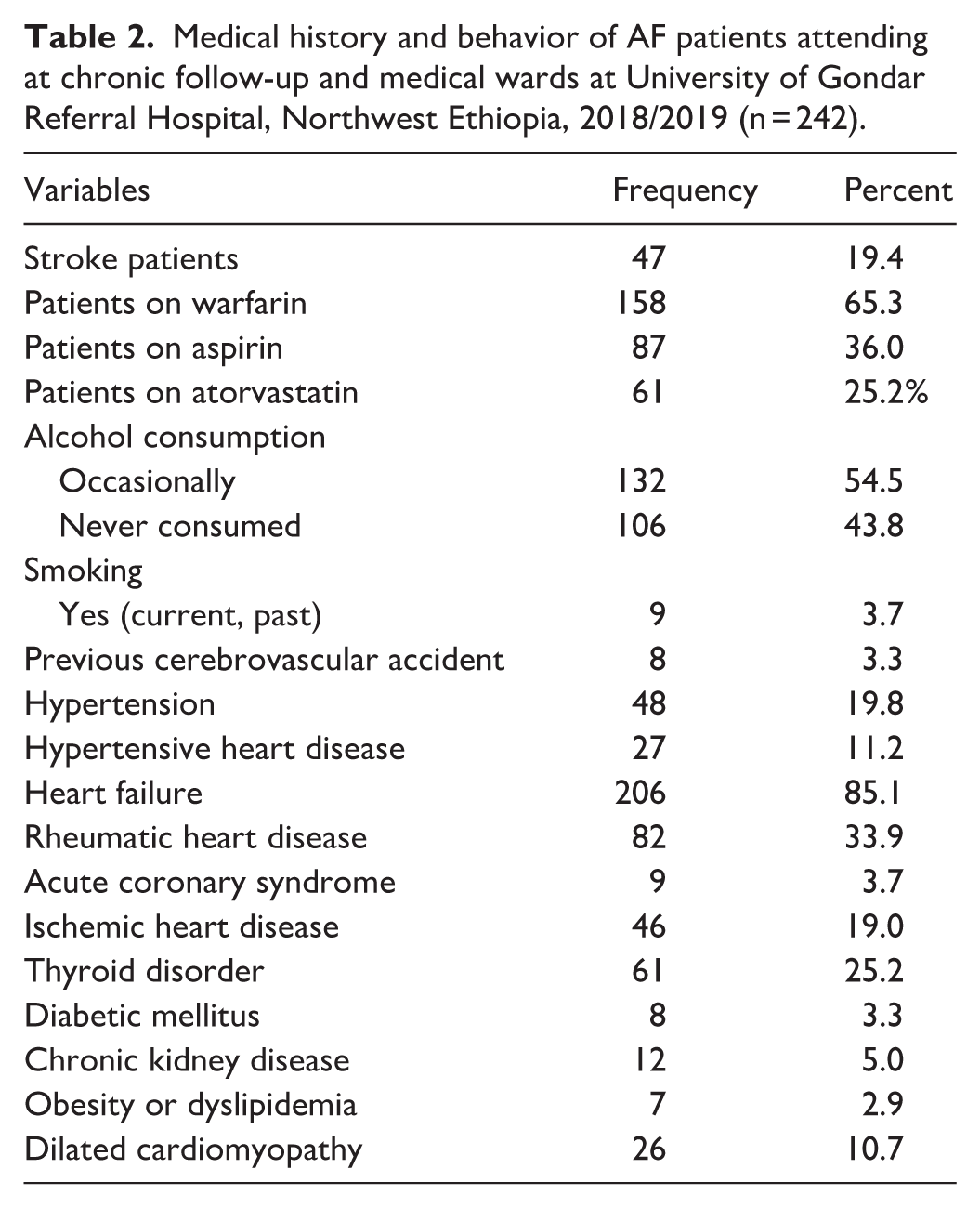
The prevalence of stroke among AF patients in the study area was 19.4% (95% CI: 13.7–24.8). Number of patients who were currently on warfarin and aspirin is 65.3% and 4.5%, respectively. About 3.3% of patients had previous history of stroke. Among AF patients, history of hypertension (19.8%), heart failure (85.1%), rheumatic heart disease (33.9%), and thyroid disorder (25.2%) were present (Table 2).
Medical history and behavior of AF patients attending at chronic follow-up and medical wards at University of Gondar Referral Hospital, Northwest Ethiopia, 2018/2019 (n = 242).
Echocardiography findings and conclusions of patients
Most of the patients have normal ejection fraction (71.6%, 63.1 %) and dilated Left atrium (63.8%, 63.8%) in both baseline and recent echocardiography, respectively (Table 3).
Echocardiography findings of AF patients at chronic follow-up and medical wards at University of Gondar Referral Hospital, Northwest Ethiopia, 2019.

The conclusion of baseline echocardiography done in 190 patients indicated that 26% of AF patients were diagnosed to have dilated cardiomyopathy and 23% of them have chronic rheumatic valvular heart disease (Figure 1).

Baseline echocardiography finding conclusion AF patients in University of Gondar Referral Hospital, Gondar, Northwest Ethiopia, 2018/2019.
Recent echocardiography was done in 83 patients. Chronic rheumatic valvular heart disease (CRVHD) (37%) and ischemic heart disease (IHD) (28%) were the consecutive highest diagnosed cases (Figure 2).

Recent baseline echocardiography finding conclusion atrial fibrillation patients in University of Gondar Referral Hospital, Northwest Ethiopia, 2018/2019.
Predictors associated with the development of stroke among AF patients
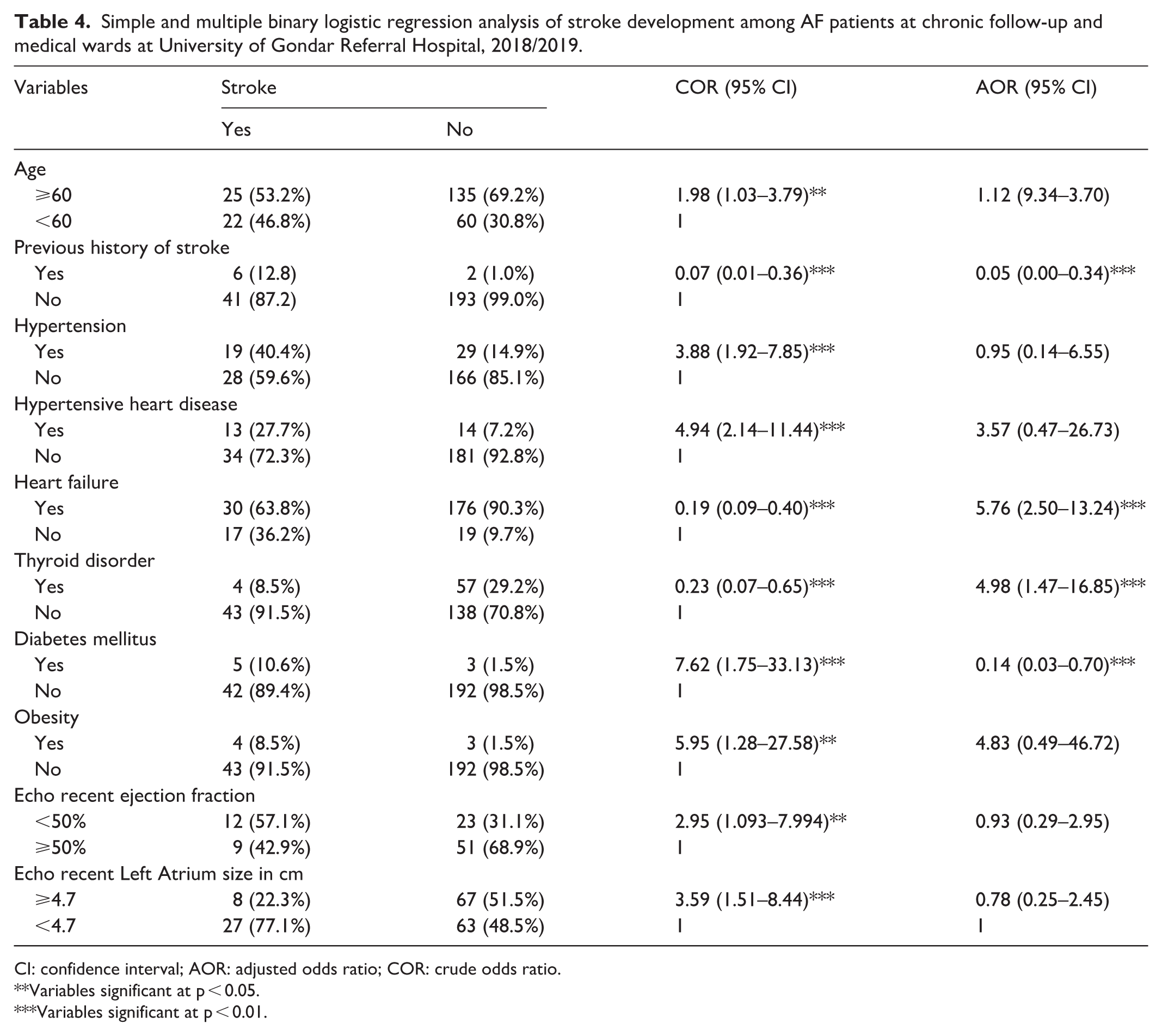
Sex, age of patients, occupational status, educational status, marital status, religion, place of residency, patients on warfarin, patients on aspirin, patients on atorvastatin, alcohol consumption, smoking, previous cerebrovascular accident, hypertension, hypertensive heart disease, heart failure, rheumatic heart disease, acute coronary syndrome, ischemic heart disease, thyroid disorder, diabetic mellitus, chronic kidney disease, obesity or dyslipidemia, dilated cardiomyopathy, ejection fraction, and left atrium size (cm) were included in the analysis. Some variables like sex, occupational status, educational status, marital status, religion, and place of residency were above the cutoff point (p-value < 0.25) during the bivariable analysis. Other variables like patients who took warfarin, aspirin and atorvastatin, alcohol consumption, and smoking were removed from the analysis due to multi-collinearity.
However, in the final analysis age, aspirin, previous history of stroke, hypertension, hypertensive heart disease, heart failure, thyroid disorder, diabetes mellitus, obesity, echo recent ejection fraction, and echo recent left atrium size in cm were risk factors in bivariable logistic regression analysis. However, only previous history of stroke (adjusted odds ratio (AOR): 0.05, 95% CI: 0.01–0.34), diabetes mellitus (AOR: 0.14, 95% CI: 0.03–0.70), heart failure (AOR: 5.76, 95% CI: 2.50–13.24), and thyroid disorder (AOR: 4.98, 95% CI: 1.47–16.85) were significant in the multivariable regression model (Table 4).
Simple and multiple binary logistic regression analysis of stroke development among AF patients at chronic follow-up and medical wards at University of Gondar Referral Hospital, 2018/2019.
CI: confidence interval; AOR: adjusted odds ratio; COR: crude odds ratio.
Variables significant at p < 0.05.
Variables significant at p < 0.01.
Discussion
The prevalence of stroke in this study was higher than studies done in Cameroon (12.5%), 24 the United Kingdom (3.6%), 25 Geneva (2.7%), 26 and Framingham (5% and 6.7%).14,27 But, it is consistent with meta-analysis study done in developing countries (2.8%–24.2%). 20 Studies are limited in Africa to compare the prevalence; however, the high burden of the disease might be due to the rise in obesity-related lifestyle risk factors of people, including hypertension, diabetes, and high cholesterol. The over use of processed foods might also another reasons to increase the magnitude of the disease. The types of study, sample size and sociocultural profile difference of the participants may influence the outputs of the study.
Several studies reported that the presence of high blood glucose or insulin resistance in the body increases the prevalence of stroke.14,28–31 Inversely, other systematic review suggested that the reduction of blood pressure and lipid lowering will reduce the risk of stroke, but there is no evidence about the reduction of blood glucose (by insulin or other drugs) level and the risk of stroke. 29 However, in our study, AF patients with diabetes are 86% less likely to develop stroke than non-diabetics counterpart. As far as other large-scale clinical trials and further investigation is done, we cannot conclude that diabetes is protective for the development of stroke. This association could be the indirect impacts of diabetes; comprehensive treatment may decrease the occurrence of stroke or patients might change their lifestyle which can decrease the prevalence of stroke.
Even though further analysis is needed, in this study previous history of stroke reduces the risk of stroke by 0.95 times. In contrast, other studies stated that previous history of stroke were having more than threefold increased risk of a new stoke.13,32 This association could be one because of small number of patients with history of stroke or patients may get good treatment and lifestyle changes, which can decrease prevalence of stroke. Besides the information, exposure levels of previously exposed individuals might be high and important to change their lifestyle, which have contribution for the development of stroke.
The occurrence of stroke among heart failure patients is more than five folds higher compared with heart failure free patients. There is no controversial studies done regarding with the inverse association of heart failure and stroke. Many studies supported that the presence of heart failure can lead to the down regulation of the thyroid hormone signaling system in the heart. In the failing heart, there is reduction of nuclear thyroid receptor level. In addition, serums levels of T4 and T3 will also decrease within the context of the non-thyroidal illness syndrome. Indeed, T3 generally increases the force and speed of systoliccontraction and the speed of diastolic relaxation.33–36 Another finding of this study is also in line with the above justifications; the occurrences of stroke are 4.98 times higher among patients who have had thyroid disorder as compared with the counterpart. However, advanced analysis is required to investigate the pathologic mechanism underlying the association, researchers are agreed with the significant association of thyroid disorder and stroke.37,38
Limitation of the study
This study may overestimate the prevalence of stroke because patients with paroxysmal AF may not be diagnosed in our setup due to absence of holter monitoring. The prevalence might be predisposed to be higher because of facility-based study while some of the other studies are population based.
Conclusion
The prevalence of stroke among AF patients in the study area was higher compared with other studies done in developed countries. Although, further analysis and large-scale trials are required to clear out the association of previous history of stroke and diabetics on the occurrence of stroke, inverse association was reported in our study. However, heart failure and thyroid disorder were found to be the risk factor for the development of stroke; therefore, physicians and cardiologists may better consider these disorders when they diagnose stroke in AF patients.
Supplemental Material
sj-pdf-1-smo-10.1177_2050312121989509 – Supplemental material for The prevalence and predictors of Stroke among atrial fibrillation patients attending at Gondar University Referral Hospital, Northwest Ethiopia
Supplemental material, sj-pdf-1-smo-10.1177_2050312121989509 for The prevalence and predictors of Stroke among atrial fibrillation patients attending at Gondar University Referral Hospital, Northwest Ethiopia by Yonas Gedamu, Asefa Adimasu Taddese, Mohamed Abdulkadir, Workagegnehu Hailu and Oumer Abdu in SAGE Open Medicine
Footnotes
Acknowledgements
We thank University of Gondar Referral Hospital internal medicine department and staff members for their cooperation during the data collection period.
Author contributions
Y.G. designed the study; developed data collection tools, performed the analysis and interpretation of data, and drafted the paper. A.A.T., M.A., W.H. and O.A. were participated in the development of the study proposal, analysis and interpretation, revised drafts of the paper, revised the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Institutional Review Board of the University of Gondar (IRB reference No: V/P/RCS/05/380/2019).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was taken from study participants. Support letters were obtained from University of Gondar Referral Hospital clinical director office. All the information was kept confidential and no individual identifiers were collected.
Availability of data and materials
The data upon which the result was based could be accessed by a reasonable request made to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.