
Abstract
Schwannoma is a benign, well-circumscribed, and encapsulated peripheral nerve sheath tumor that develops from Schwann cells. The growth pattern is usually slow, tending to clinical indolence. Primary pulmonary neuronal tumors are very rare, accounting for ~0.2% of all lung neoplasms, and are often misdiagnosed due to their nonspecific radiological features. A 50-year-old man presented with a large cystic mass in upper lobe of left lung discovered incidentally on chest X-ray during work up after a blunt chest trauma. Gross examination of the mass following surgical excision revealed a well-circumscribed, encapsulated creamy-gray cystic lesion with gelatinous material measuring 10.5 × 6 × 5.5 cm, attached to a segment of lung. Microscopically, the tumor showed hypo- and hypercellular areas with proliferation of elongated wavy cells in a myxoid background which is characteristic of Schwannoma. Despite intrapulmonary schwannomas’ rarity, it is essential to consider schwannomas in the differential diagnosis of pulmonary masses, particularly when clinical and radiological findings suggest a well-defined, encapsulated lesion.
Introduction
Schwannoma is a benign, well-circumscribed, and encapsulated peripheral nerve sheath tumor that arises from Schwann cells. 1 Macroscopically, these tumors typically appear as firm masses which may be round, ovoid, or lobulated and often exhibit a light-tan appearance surrounded by a fibrous capsule. They usually present as soft-tissue density on computed tomography (CT). 2 They generally exhibit slow growth and follow an indolent clinical course. Commonly, patients present with a slowly enlarging, painless mass, although neurological symptoms may occur depending on the specific nerve involvement. 3 The majority of schwannomas are benign, and malignant transformation is exceedingly rare. 3
Schwannomas most commonly occur in the head and neck regions, retroperitoneum, posterior mediastinum, and chest wall. However, schwannomas originating from the lung parenchyma or bronchial tree are extremely uncommon. 4 Primary intrapulmonary neuronal tumors are very rare, accounting for ~0.2% of all lung neoplasms. 5
In this report, we present an unusual case of a large, solid-cystic intrapulmonary schwannoma that was incidentally discovered in an asymptomatic patient.
Case Presentation
A 50-year-old, Iranian, non-smoker man without family history of neurofibromatosis was referred to cardiothoracic surgery clinic for evaluation of a large cystic mass in the upper lobe of the left lung, discovered incidentally during imaging after a blunt chest trauma. The patient did not have shortness of breath, pleuritic chest pain, tachypnea, or cough. On physical examination, lung auscultation and O2 saturation were normal. His laboratory investigations showed no abnormality.
High-resolution CT scan of the chest demonstrated an oval-shape hypoattenuating structure measuring 81 × 70 × 95 mm in the central aspect of upper lobe of left lung (Figure 1A and B). This structure had a thin wall and homogeneous low density (5-20 HU); possibly representing a cyst. However, the CT was a non-contrast study and therefore enhancement could not be evaluated. The adjacent tracheobronchial system showed no significant luminal narrowing and thoracic aorta and pulmonary vessels grossly seemed to be spared. Also, no significant mediastinal or hilar lymphadenopathy was detected. In light of radiological findings, a hydatid cyst was suggested as a possible diagnosis. No possibility of a malignant process was considered according to imaging study, and due to the possible diagnosis of hydatid cyst; no preoperative biopsy was performed.

Axial (A) and coronal (B) views of high-resolution computed tomography of the chest demonstrate a hypodense, possibly a cystic structure located in upper lobe of left lung.
Left upper lobectomy with partial rib resection to facilitate removal of the lobe was performed via a left posterolateral thoracotomy. It revealed a large left upper lobe mass with adhesion to the pulmonary artery, aorta, and middle mediastinum.
Gross examination revealed a well-circumscribed encapsulated creamy-gray cystic mass measuring 10.5 × 6 × 5.5 cm, attached to a segment of lung measuring 12 × 11 × 3 cm. Cut sections of the mass showed solid-cystic areas with gelatinous consistency (Figure 2A–D).
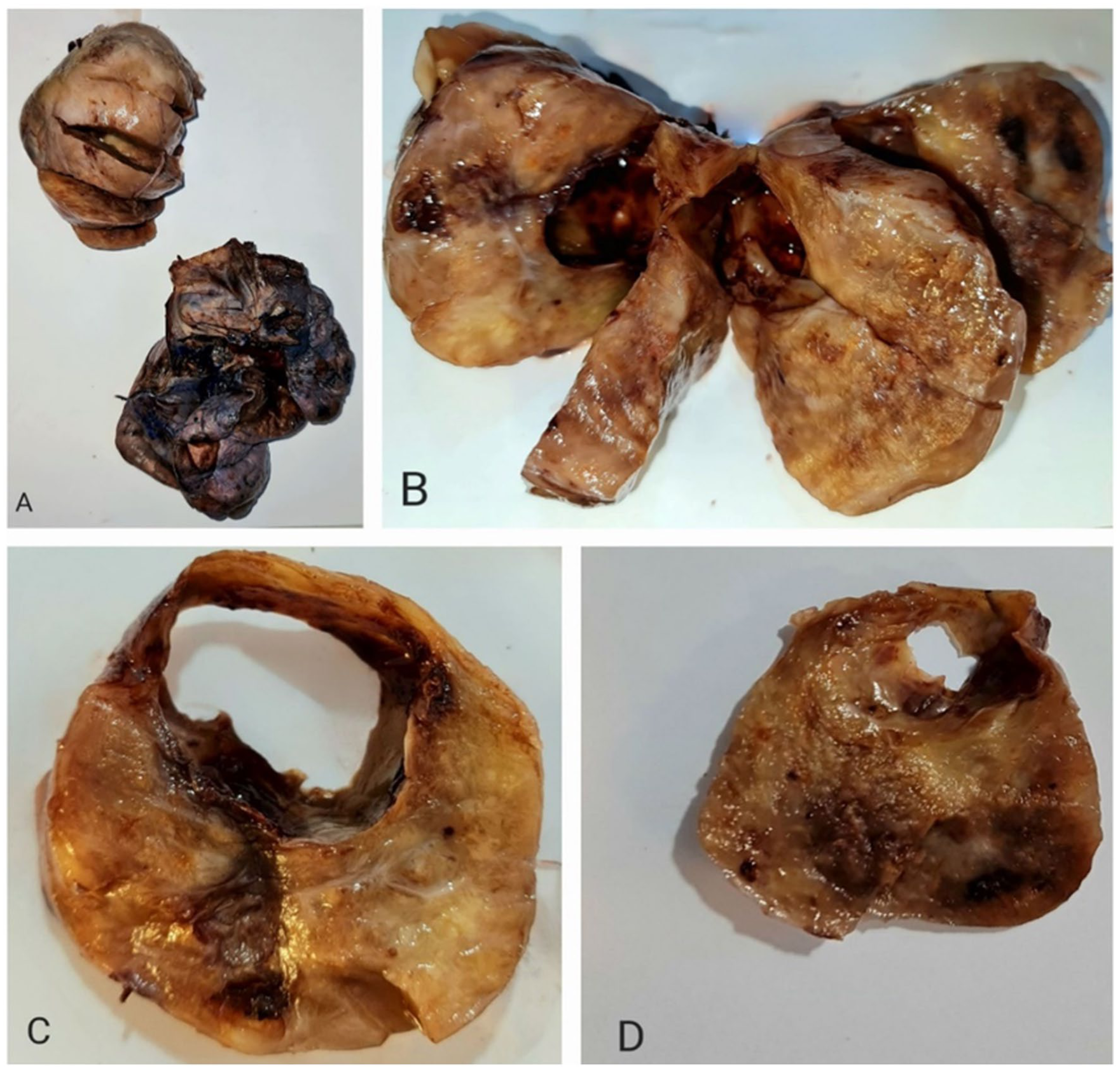
(A) A well-defined, encapsulated mass (left upper) was attached to a lobe of lung that was separated during specimen handling. (B) Cut sections of the mass revealed solid-cystic components. (C, D) Horizontal sections of the mass.
Microscopically, the tumor showed hypocellular and hypercellular areas with proliferation of elongated wavy cells with spindle-shaped nuclei and cellular palisading (Verocay body) in a myxoid background (Figure 3A–D). There was infiltration of macrophages and vascular hyalinization. No mitotic figures, atypical cells, or necrosis were identified.
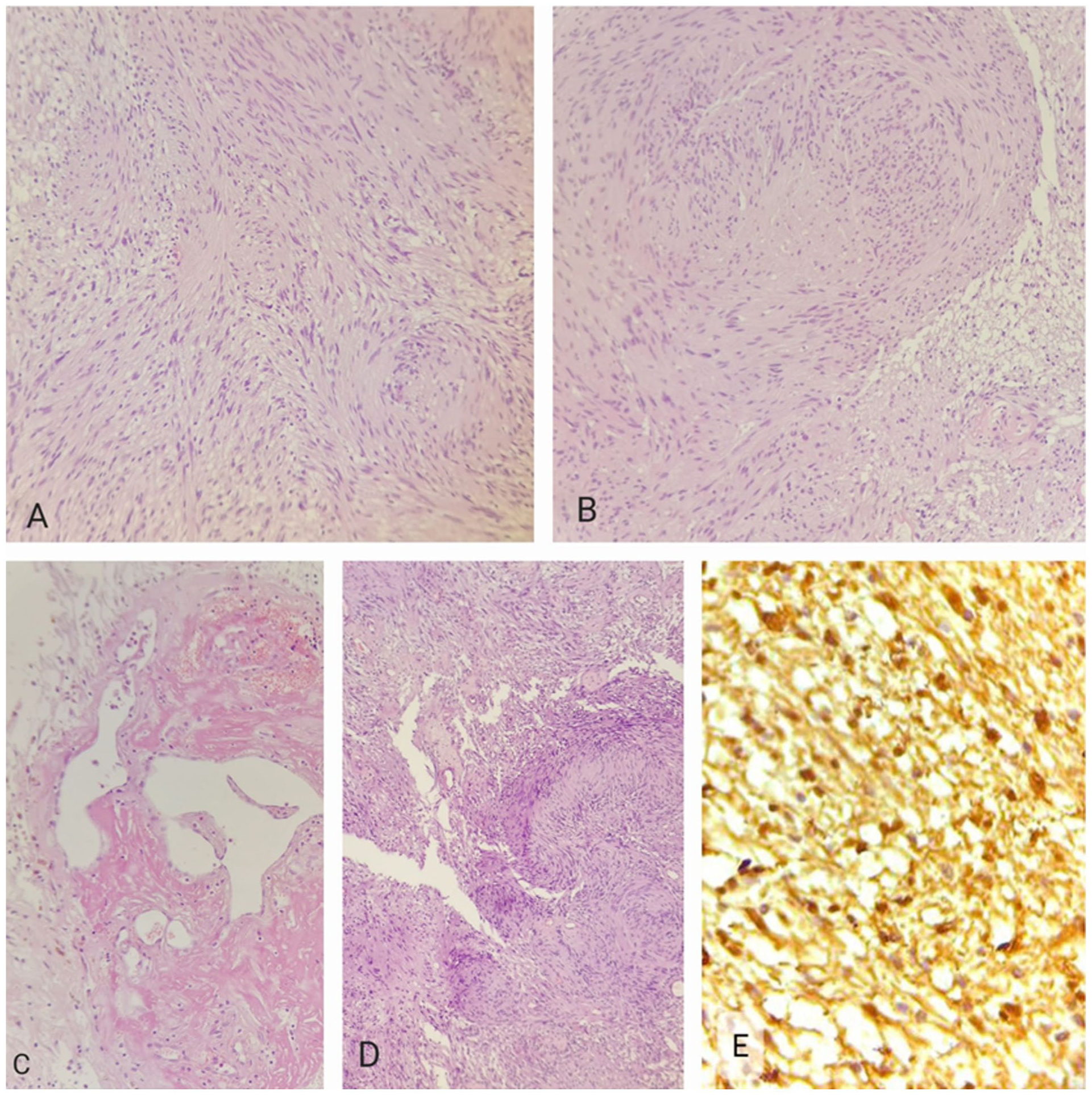
Microscopic view of the mass: (A, B) proliferation of spindle cells (H&E stain, ×20 magnification); (C) hyalinized blood vessels (H&E stain, ×20 magnification); (D) nuclear palisading and Verocay body (H&E stain, ×10 magnification); (E) IHC staining for S-100 (×40 magnification).
Immunohistochemical staining showed strong nuclear positivity for S-100, confirming diagnosis of Schwannoma (Figure 3E).
The patient was discharged 5 days after surgery and there were no complications associated with the surgery. Follow-up serial chest X-ray remained unremarkable. Adjuvant chemotherapy or radiation treatment was not essential due to the benign nature of the tumor. The patient has no complication after 6 months of his surgery.
Discussion
Schwannoma is a benign, well-circumscribed, and encapsulated peripheral nerve sheath tumor that arises from Schwann cells that cover the axons of nerves of periphery, cranium, and the autonomic nervous system. 1 They are often mistaken for more common malignant tumors due to their radiologic appearance, which frequently prompts further investigation and leads to a definitive diagnosis only after histological examination. This highlights the importance of considering schwannoma in the differential diagnosis of pulmonary masses, as seen in the present case. 2 Most cases are sporadic; however, some are associated with neurofibromatosis 2 (NF2), Schwannomatosis, or Carney’s complex, and they may rarely occur following radiation. 3
Intrapulmonary schwannomas are uncommon benign lung tumors that typically appear as solitary masses. They may be found in either the central or peripheral areas of the lung and have a low risk of malignant transformation.4,5 Their most common presentations include thoracic pain, dorsal or intercostal neuralgia, respiratory symptoms such as cough and dyspnea, and Horner’s syndrome. 6 Our patient’s tumor was discovered by chance during a post-trauma assessment, as it was not causing any symptoms.
Thoracic schwannomas are typically well-defined, spherical, and lobulated, though they may also present as dumbbell-shaped paraspinal masses. 7 They may exhibit a smooth, nodular outline, and occasionally the nerve origin is visible. On the cut surface, they appear tan or yellow in color, often with areas of hemorrhage and cystic changes. 8
The microscopic morphology of the resected mass in our case lacked mitotic figure, atypia, and necrosis, similar to the typical microscopic appearance and included Verocay bodies, which are characterized by the parallel alignment of cellular nuclei. 9 Since nuclear palisading is not exclusive to schwannomas and can be observed in other tumors as well, immunohistochemical techniques assist in diagnosis by detecting markers like S-100, Calretinin, CD34, CD56, Desmin, and EMA, especially when the diagnosis is difficult due to atypical clinical presentation or the unusual location of the mass. 9
A study reports a benign pulmonary schwannoma that remained asymptomatic for 4 years until it compressed intrathoracic structures, leading to symptoms like upper limb or lower limb edema, chronic venous stasis, increased right ventricular systolic pressure, and a mildly enlarged inferior vena cava. 10 A rare extrapulmonary schwannoma near the right paratracheal region was reported, presenting with symptoms resembling those of intraparenchymal and endobronchial tumors, including persistent cough and shortness of breath. 2 An incidental pulmonary nodule was diagnosed as a schwannoma in a patient with a subtle history of blood-tinged sputum. 11 The severity of symptoms depends on the size and location of the mass. 6 Most patients with peripheral intra-pulmonary schwannoma are asymptomatic. 12
In a case series of 5 patients, intrapulmonary schwannomas typically appeared as well-defined masses with varying levels of enhancement on CT and MRI. 9 These masses tend to be neurogenic in origin and are sometimes mistaken for more common tumors. Each case had a different presentation (ranging from mass lesions to suspected Pancoast tumors) showing how varied and deceptive these tumors can be.
In order to identify and carefully evaluate all reported cases and their impact on clinical presentation, we conducted a comprehensive literature review covering the last 10 years. Table 1 presents 24 reported cases of intrapulmonary schwannoma published over the last decade, including the current case. The patients’ ages ranged from 19 to 69 years, with a relatively even distribution between males and females. Tumor sizes varied significantly, from small nodules measuring 2 cm to large masses exceeding 20 cm in diameter. The majority of tumors were discovered incidentally, while others presented with non-specific respiratory symptoms such as chronic cough, chest pain, dyspnea, or signs of pneumonia. The lesions were most commonly located in the upper and lower lobes of the lungs, with a slight predominance in the right lung. The current case of a 50-year-old man with a large asymptomatic lung mass highlights the potential for significant tumor growth and the need to consider schwannoma in the differential diagnosis of pulmonary lesions.
Case Reports of Intrapulmonary Schwannoma in the Last 10 Years.

A key insight from our literature review is the almost universal absence of molecular genetic profiling in reported cases of intrapulmonary schwannoma. While none of the cases in our series, including the 23 from the literature, documented NF2 gene sequencing or other molecular tests, a majority provided clinical follow-up regarding syndromic association. In these instances, the tumors were consistently reported as sporadic, with no personal or family history of NF2 or schwannomatosis.9,11,13,14,16,18,19,21 -23,26,28 This strongly suggests that solitary intrapulmonary schwannomas are predominantly sporadic events. Nevertheless, the potential for a syndromic origin, though seemingly rare in this location, warrants a basic clinical evaluation for features of NF2, such as hearing loss, vestibular schwannomas, or other nervous system tumors, particularly in younger patients. The definitive role of NF2 gene inactivation in the pathogenesis of these pulmonary tumors remains an open question. Future reports would be greatly enhanced by incorporating basic molecular techniques, such as immunohistochemistry for Merlin protein loss or genetic analysis, to confirm the sporadic nature and further elucidate the driver mutations involved.
Several treatment options are available for managing intrapulmonary schwannomas, including surgical removal, endoscopic intrabronchial excision, and yttrium aluminum garnet (YAG) laser resection. 9 The choice between lobectomy and enucleation depends on tumor size, location, and adherence to adjacent structures. In our case, lobectomy was necessitated by the tumor’s large dimensions and mediastinal adhesions. However, literature supports enucleation for smaller, encapsulated lesions,13,21 with equivalent oncologic outcomes and superior functional preservation. Preoperative biopsy and advanced imaging may aid in selecting conservative approaches when feasible. Future studies should evaluate long-term pulmonary function after parenchymal-sparing.
Conclusion
In conclusion, intrapulmonary schwannomas are rare, benign nerve sheath tumors that may mimic other pulmonary masses. Although typically asymptomatic, their size and location can vary significantly. Accurate diagnosis relies heavily on radiologic study, histopathological examination, and immunohistochemical staining may further support the diagnosis in ambiguous cases. Early surgical resection remains the mainstay of treatment with favorable outcomes.
Footnotes
Ethical Considerations
This is an observational study. The Bioethics Committee of the Medical University of Shiraz Research Ethics Committee has confirmed that no ethical approval is required.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent for Publication
A consent was obtained from the patient whose case is being reported in this manuscript. In addition, the case report is anonymized in order to protect the identity of the patient in the study. It is not possible to identify the patient with certainty from the information presented in this case report. The patient authorized the research team to release information regarding his diagnosis, treatment, in any format including multimedia files for educational and publication purposes. The consent document detailing the health information that would be used for publication purposes was provided to the patient. In addition, their content was discussed with the patient orally. All their questions were answered, and the patient provided orals as well as a written consent.
Author Contributions
All authors contributed to the study’s conception and design. EEA, MJ, PM, ZB, BG material preparation, data collection, and analysis were performed. EEA written the first draft of the manuscript. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data generated for this study are available upon reasonable request from the corresponding author.