
Abstract
Inflammatory myofibroblastic tumor (IMT) is a very rare lesion of unknown etiology. Cases of IMT involving the appendix are exceptional, and they can mimic malignant appendicular tumors. We present a case of a 65-year-old man who presented to our emergency room on septic shock and acute abdomen secondary to visceral perforation. The patient underwent exploratory laparotomy; massive bowel dilatation was encountered, along with 3 L of purulent intraperitoneal fluid and a perforated appendicular mass of 6 cm. An appendicectomy was performed. Histopathologic examination established the diagnosis of inflammatory pseudotumor with appendiceal perforation. This study constitutes the 14th confirmed case report of an appendicular IMT. It is important to include IMT in differential diagnoses of appendicular masses to avoid excessive resections.
Introduction
Inflammatory myofibroblastic tumor (IMT), also called inflammatory pseudotumor is a rare disease of mesenchymal origin, first described in 1937.1-3 Inflammatory myofibroblastic tumor has distinct clinicopathological entities characterized by a dense inflammatory cell component and amid myofibroblastic proliferation. Its histopathologic nature is benign, but it may not be differentiated from a malignant tumor because of its local invasiveness, aggressive behavior, and its tendency to recur and metastasize.1,4,5 In 2003 was classified as an intermediate neoplasm in the current World Health Organization histologic typing. 6
It was initially described in the lung, which is also the site where it is most commonly presented. 7 Subsequently, it was seen that it can also be presented in soft tissue, the mesentery, the omentum, and retroperitoneum 8 ; thenceforth, it was recognized that any anatomic location can be involved, making IMTs of the gastrointestinal tract extremely rare, being only 13 confirmed cases of appendicular origin.9,10 Most of these reported cases of IMT of the appendix are adolescents or young adult men. 1 Herein, we present a case of a 65-year-old man who presented to our emergency department on septic shock with an acute abdomen secondary to visceral perforation. Surgery was performed finding a perforated appendix with a tumor-like lesion on it. On histological examination, the lesion was identified as an IMT. A review of the literature is also presented.
Presentation of Case
A 65-year-old male patient with family history of diabetes mellitus and medical history of prostatic hyperplasia and a simple umbilical hernia repaired presented to the emergency department. He arrived complaining of a 5-day history of diffuse abdominal pain, nausea, vomiting, and abdominal distension. The patient referred inability to pass flatus or to evacuate for the past 24 hours. On physical examination he was tachycardic and hypotensive. He presented with diffuse abdominal tenderness, suggestive of peritoneal irritation and severe distension. Digital rectal examination revealed an empty rectum, without abnormalities.
Complete blood count confirmed the presence of leukocytosis of 17.9 × 103 with hemoglobin of 18.1 g/dL and platelet count of 207 × 103. Blood chemistry revealed acute renal failure, with a serum creatinine of 3 mg/dL, blood urea nitrogen 60 mg/dL, and urea of 210 mg/dL.
Simple abdominal radiographs displayed dilated loops and no signs of gas in the rectum, suggesting bowel obstruction, and no free air was seen. A noncontrast computed tomography (CT) of the abdomen was ordered, revealing a thick and irregular fibrous capsule at the base of the appendix with central low-attenuation necrotic component. Surrounding inflammatory changes were present with periappendiceal reactive nodal enlargement, pneumoperitoneum, and dilated large bowel. The appendix was enlarged with a perforation at the tip (Figure 1).

(A) Axial abdominal CT shows a thick and irregular fibrous capsule at the base of the appendix with necrotic component (arrow) and surrounding inflammatory changes. (B) Coronal reconstruction of the same patient reveals fibrous capsule and inflammatory changes at the base of the appendix (dotted arrow) and perforation at the tip of the appendix (solid arrow). Distention of the ascending colon is seen.
A preoperative diagnosis of bowel perforation with peritonitis was obtained, on the basis of clinical and radiological findings. The patient’s blood pressure could not be stabilized despite reanimation with crystalloids; therefore, the patient was transferred to the operating room where the attending surgeon and the surgical resident performed an emergency laparotomy. Massive bowel dilatation was encountered and approximately 3 L of purulent intraperitoneal fluid was aspirated. A mass measuring 6 cm × 6 cm was seen at the tip of the appendix with a perforated area of about 1 cm in diameter. The base of the cecum was healthy, and an appendectomy was successfully performed (Figure 2). The patient was transferred to the surgical intensive care unit for 48 hours and had an adequate postoperative outcome, referring only moderate pain during the initial days. Oral intake was reintroduced on the third day, without complications. On the postoperative day 7, the patient was discharged home, with good oral intake and with normal evacuations. The patient was seen in the ambulatory clinic at 1 and 6 months after surgery for a follow-up examination with a satisfactory evolution with normal renal function.

(A) Abdominal cavity with appendicular tumor measuring 6 cm × 6 cm. (B) Resected appendix with the tumor involving the middle and distal third.
Histological examination of the specimen dyed with hematoxylin and eosin, revealed a mass showing fibroblastic proliferation accompanied by a dense inflammatory infiltrate in the mucosa and a clear thickening of the submucosa. A few areas showed myxoid changes with spindle cells, alternating with polyclonal plasma cells and lymphocytes (Figure 3). A perforation was identified in the section from the tip of the appendix lined by fibrinoid exudates. The immunohistochemistry of the paraffin section was positive for vimentin and smooth muscle actin and negative for anaplastic lymphoma kinase (ALK) (Figure 4). Final diagnosis was inflammatory pseudotumor with appendiceal perforation.
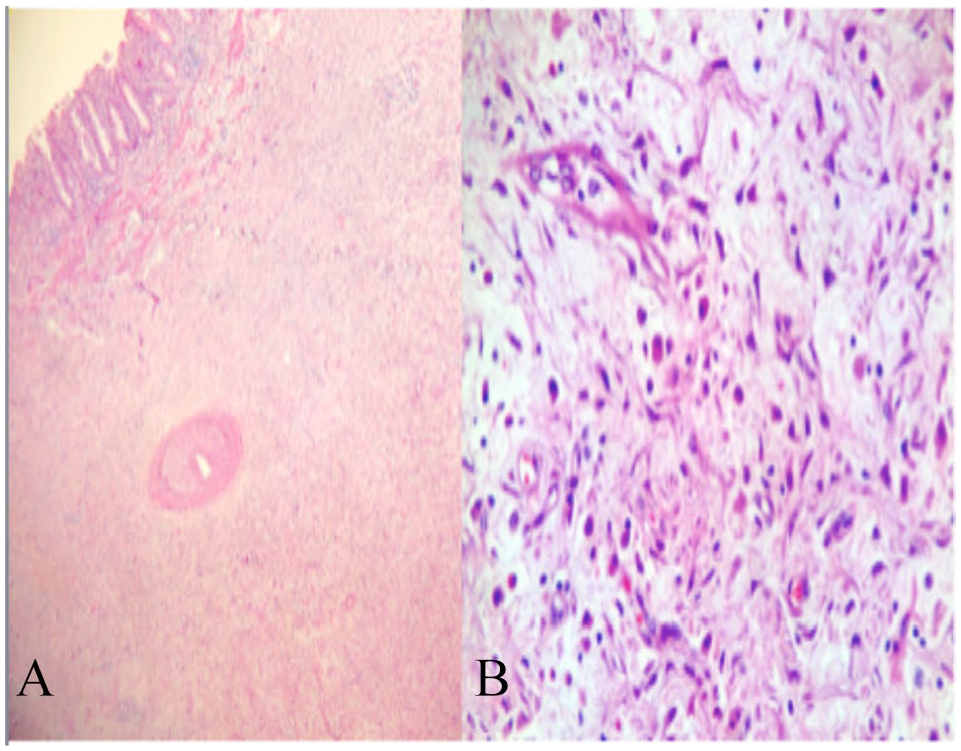
(A) Panoramic view of the appendix. Notice the clear thickening of the submucosa, with the dense inflammatory infiltrate in the mucosa. (B) High-power view of inflammatory myofibroblastic tumor. On a myxoid background with spindle cells, it shows alternating with polyclonal plasma cells and lymphocytes.
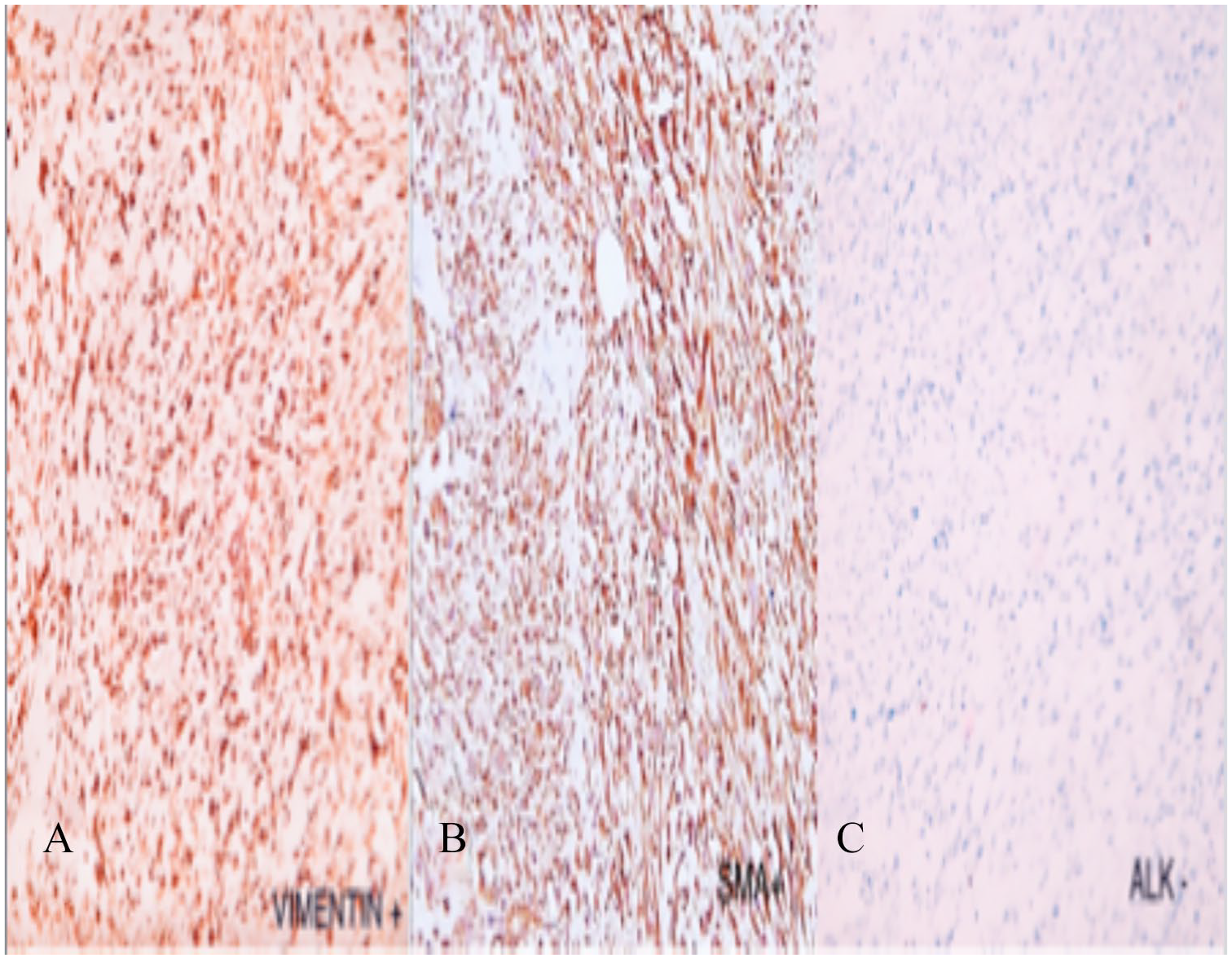
(A) Vimentin stain shows a strong positive stain to cytoplasm with mesenchymal differentiation. (B) Smooth muscle actin shows positive stain to myofibroblast. (C) Anaplastic lymphoma kinase stain results negative to cytoplasmatic and nuclear staining.
Discussion
Inflammatory myofibroblastic tumor is an atypical pseudosarcomatous, inflammatory, and histopathologic entity that most often affects children and young adults. When we performed a comprehensive search of English and Spanish literature, no more than 13 cases reported were found. Of note, most of the reported cases are in pediatric patients and young adult men. 8 The first case report was published in 1984 and describes an 8-year-old boy who presented with symptoms of acute appendicitis, 11 and the most recent report, published in 2018 by Bashir et al, 10 described a 14-year-old boy with the same preoperative diagnosis. Our patient constitutes the oldest patient who has presented with this appendicular tumor, making it the 14th case of this entity and also the first to present with septic shock secondary to perforation. It is most similar to a case reported by Kumar 3 in which the patient was also a male adult who presented with peritonitis.
A variety of substitutes have been attributed to these lesions, such plasma cell granuloma, mast cell granuloma, histiocytoma, xanthomatous pseudotumor, fibroxanthoma, fibromyxomatous tumor, pseudosarcomatous myofibroblastic proliferation, inflammatory fibrosarcoma, pseudosarcomatous fibromyxomatous tumor, and reactive pseudosarcomatous response.3,7 The etiology of IMT remains unclear, and in most cases no causative agent is evident. Its development has been described after trauma, neoplasia, and surgery. 9 There are reports of an association with Castleman disease, Hodgkin disease, peptic ulceration, Behçet disease, and chronic infections (Campylobacter jejuni, Helicobacter pylori, Escherichia coli, Epstein-Barr virus, Coxiella burnetii, Klebsiella pneumoniae).3,5,8 We do not know the exact origin of our patient’s appendiceal pseudotumor; however, we do not consider acute appendicitis to be an etiological factor for developing this entity. Nonetheless, we believe that appendicitis occurred secondary to obliteration of the appendiceal lumen by the tumor, leading to perforation. Another rare presentation of this tumor was described by Majumdar et al 8 describing a case with concomitant mucosal dysplasia, first impression of which was pseudomyxoma peritonei.
Surgery remains the most effective treatment for this pseudotumor1,3; however, it must be noted that IMTs present with inconstant biological behavior that ranges from benign lesions (most frequent) to more aggressive variations. Whether complete surgical resection can be achieved depends on several factors such as the location of the tumor, multinodularity, and proximity to neighbor structures.3,4 For multiple and invasive lesions, chemotherapy with cisplatin, doxorubicin, and methotrexate may be considered, as well as radiotherapy for local recurrence or incomplete removal of the tumor.1,3
The clinical presentation of IMT varies markedly, depending on the site at which the tumors originated. Most of the patients with appendiceal IMT presented with abdominal pain in the right lower quadrant, nausea, and vomiting, mimicking acute appendicitis.7,8,10,12 In some patients, imaging studies were ordered suspecting this last diagnosis, thus revealing an appendicular mass.1,5,9,13,14 Despite detection during preoperative screening methods, its radiological appearance is nonspecific and insufficient to make a specific diagnosis. Therefore, the final diagnosis is made by histopathologic examination. 7
In our case, our patient had abdominal tenderness to palpation and presented with septic shock. We therefore ordered a CT of the abdomen preoperatively, which reported changes consistent with complicated appendicitis and bowel obstruction, leading to an emergent laparotomy.
The microscopic descriptions of IMT are relatively uniform. In general, these tumors are composed of a dominant-spindle cell proliferation with inflammatory polyclonal mononuclear infiltrates, including plasma cells, lymphocytes, and histiocytes, arranged in a collagenous and slightly myxoid background. Our patient’s tumor presented these histologic changes. Three histological patterns are described: fibromyxoid or vascular, proliferating, and sclerosing. Immunostains on spindle cells have often been found positive for vimentin, smooth muscle actin, muscle-specific actin, desmin, and focally for cytokeratins in most of the cases. Specific immunostaining techniques can help differentiate these tumors, with a favorable prognosis.5,7,10 The expression of ALK, may be a specific marker for IMT. Immunostaining for ALK produced fibrillary or granular cytoplasmic staining in the neoplastic cells, sometimes with cell membrane accentuation. This marker is implicated selectively in younger patients and is generally associated with a favorable outcome. 15
Because of the presence of spindle cells in bundles, soft-tissue sarcomas such as malignant fibrous histiocytoma, rhabdomysarcoma, and fibrosarcoma should be kept in mind in the differential diagnosis of IMT; nonetheless, these tumors will express mitotic activity. 3 Final diagnosis of our case was diagnosed as benign IMT because there was eosinophilic infiltration, with no mitotic activity, and because of the occurrence of dense inflammatory cells and fibroblasts with reactive swollen nuclei.
The incidence of local recurrence has been reported to be 15% to 37% in a large series of children presenting with IMT of mesentery and retroperitoneum; furthermore, infrequent distant metastases also have been suggested to occur. 4 Predictors of a potentially malignant behavior include cellular atypia, ganglion-like cells, necrosis, nucleolar prominence, atypical or increased mitotic figures, expression of p53, and DNA aneuploidy. However, a unique and consistent chromosomal abnormality has not been identified.7,8 Nonetheless, none of the 13 appendicular IMT reported cases had an aggressive behavior. They are summarized and detailed in Table 1.
Reported appendiceal inflammatory myofibroblastic tumors.
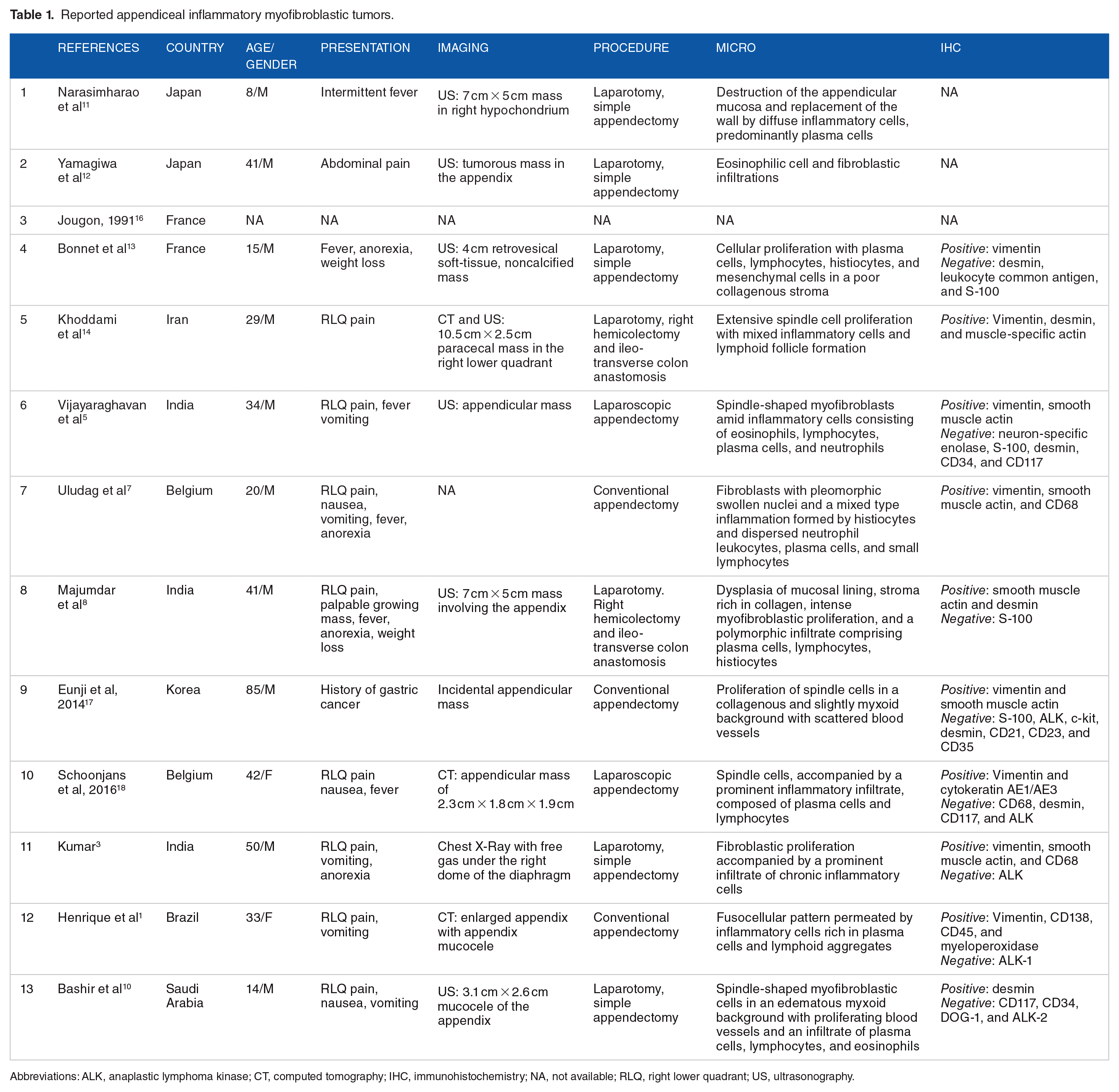
Abbreviations: ALK, anaplastic lymphoma kinase; CT, computed tomography; IHC, immunohistochemistry; NA, not available; RLQ, right lower quadrant; US, ultrasonography.
Conclusions
This study constitutes the 14th confirmed case report of an appendicular IMT. It is important to include IMT in differential diagnoses of appendicular masses to avoid excessive resections; however, appendectomy should be sufficient for this relatively indolent lesion. Although IMT is a benign tumor, which rarely presents malignant behavior, long-term clinical and radiological follow-up is recommended due to the lack of scientific data of this particular tumor at this specific anatomical site.
Footnotes
Author Contributions
MGU: Conceptualization, data curation, writing original draft
ARD: Data curation, formal analysis, investigation
SEK: Project administration, supervision
RGR: Supervision and editing
GG: Validation, Writing-review & editing.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of Tecnologico de Monterrey ethics committee and institutional review board number 122 and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Informed Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.