
Abstract
Background:
Carbon dioxide (CO2) lasers have transitioned from niche resurfacing tools to versatile mainstays in aesthetic and reconstructive surgery.
Objectives:
To present 8 years of single-centre clinical outcomes using fractional and surgical CO2 platforms, together with a narrative review of emerging biologic adjuncts.
Methods:
Retrospective analysis of 1,098 patients (650 females, 448 males; aged 4-81 years) treated between August 2017 and May 2025. Indications included acne scars, pigmentary dyschromia, benign cutaneous lesions and post-traumatic/burn scars. Outcomes were measured using clearance rates and patient satisfaction. A narrative review synthesised recent evidence on adjunctive stromal vascular fraction (SVF), platelet-rich plasma (PRP) and exosomes.
Results:
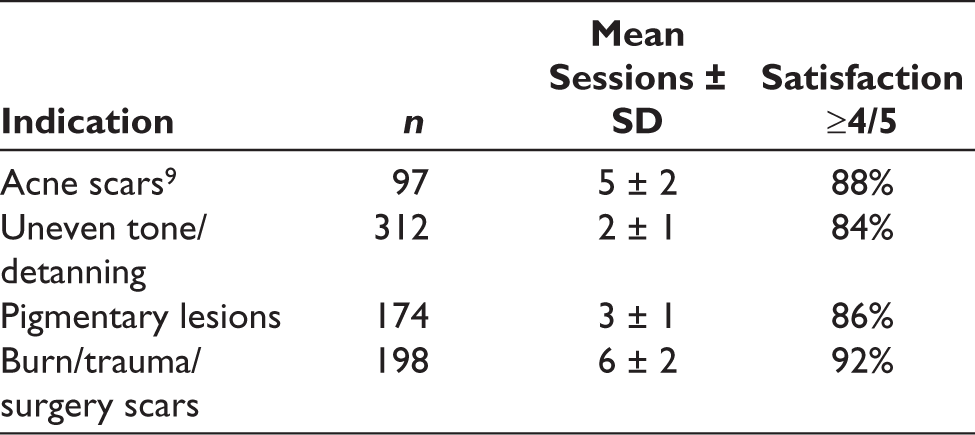
Fractional CO2 achieved 76%-85% mean improvement across texture and pigment indications, with ≥84% patient satisfaction. Surgical mode achieved 95% clearance of benign lesions and ≥50% keloid regression in 86% of cases. Adverse events were limited to transient erythema (47%), post-inflammatory hyperpigmentation (9%) and one delayed hypopigmentation. Literature review suggests biologic adjuncts enhance collagen remodelling, reduce downtime and improve pigmentary safety.
Conclusions:
CO2 lasers remain the gold standard for resurfacing and lesion removal. Biologic adjuncts, particularly SVF, PRP and exosomes, represent promising synergistic strategies. Prospective controlled trials are warranted to define optimal combined protocols.
Introduction
Since the advent of pulsed resurfacing in the 1990s, 1 iterative refinements in scanner optics, pulse modulation and fractional delivery have transformed the CO2 laser into a cornerstone of aesthetic and reconstructive practice.2,3Our centre integrated a dual-mode fractional and surgical CO2 platform in 2017, which has since become integral to treatment protocols for acne scarring, pigmentary disorders and benign cutaneous excisions. Various uses of CO2 lasers include facial rejuvenation, post-acne scars, pigmentation issues, anti-ageing (fine lines), surgical removal of warts, naevi, skin tags and cancer, surgical scars, burn scars, removal of corn foot and vaginal rejuvenation. This study reports our 8-year experience and contextualises outcomes within the contemporary evidence base.
Fractional CO2 Laser Mechanism of Action (Schematic).
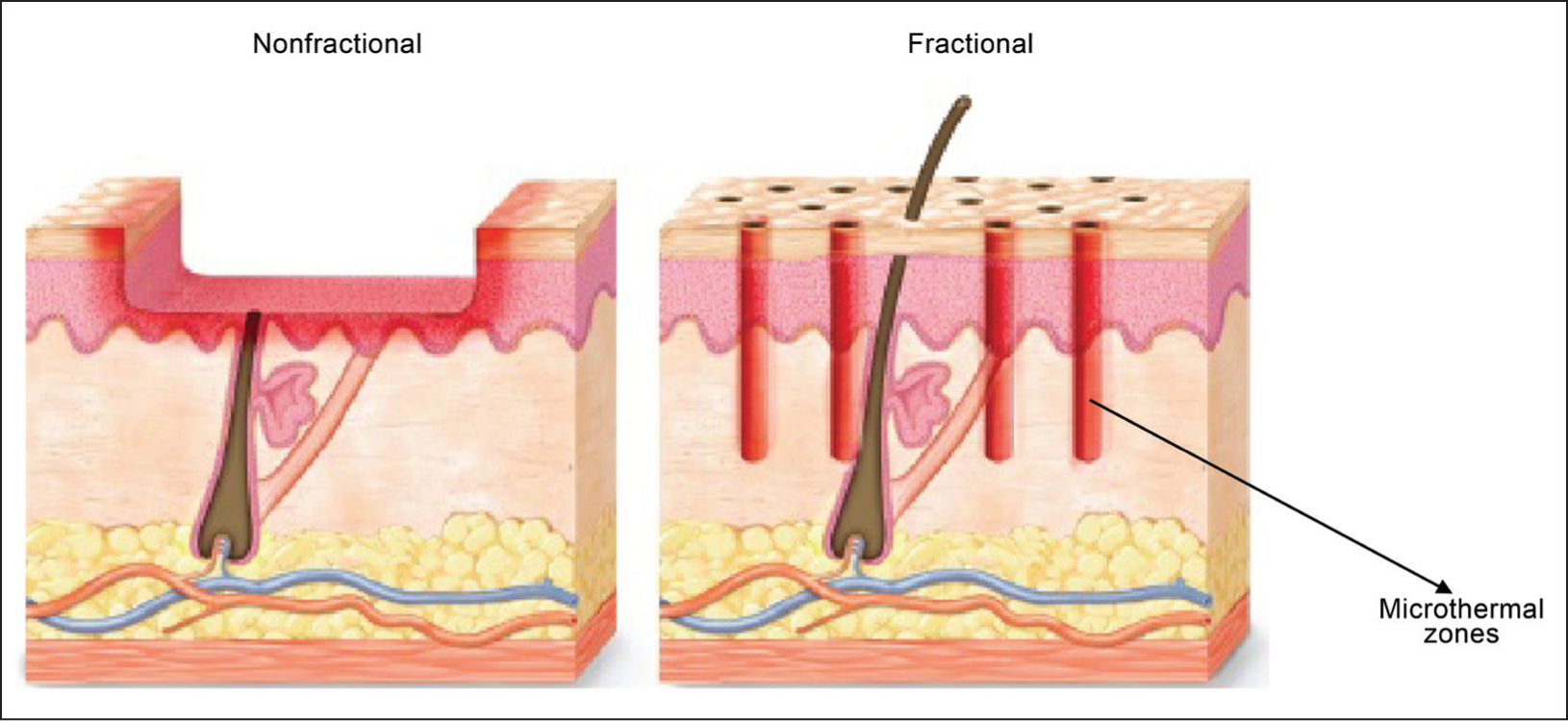
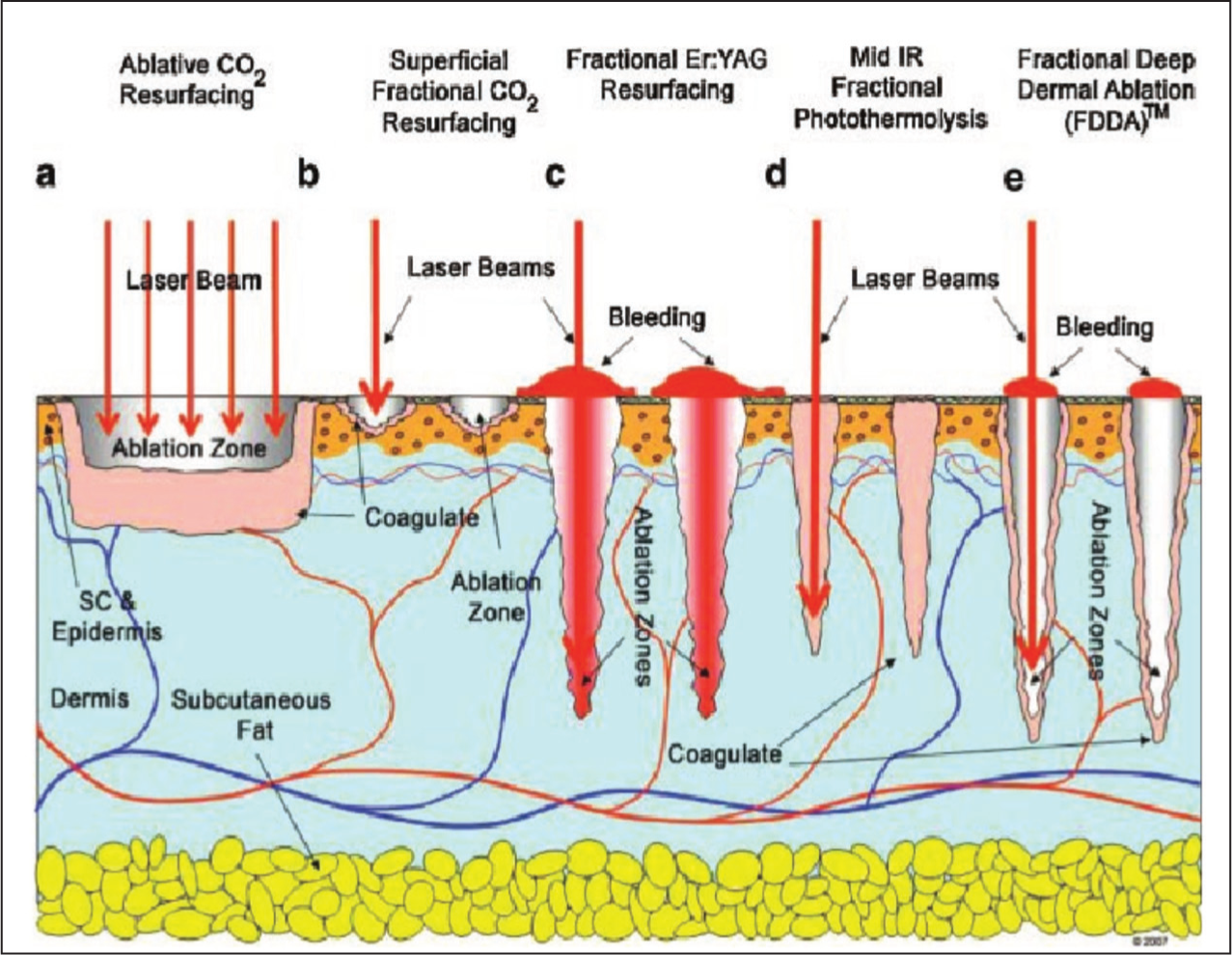
Operating at 10,600 nm, the CO2 laser matches the absorption peak of intracellular water, producing precise vaporisation within ~20 µm and a surrounding 100–200 µm coagulative rim that confers haemostasis. 4 Fractional delivery pixelates the beam, sparing 70%–90% of the epidermis and thereby accelerating re-epithelialisation.5,6 Histologic studies confirm neocollagenesis and elastic fibre reorganisation peaking at 3-6 months (Figure 3).7,8
Our Machine with Fractional and Surgical Probes Mounted Respectively.

Before and After Clinical Example of Acne Scarring Treated with Fractional CO2.

Patients and Methods
Design: Retrospective cohort plus narrative review.
Setting: Single cosmetic surgery centre (Luxor Hospital), Vadodara, Gujarat, India.
Period: August 2017-May 2025.
Participants: 1,098 patients (650 females, 448 males), aged 4-81 years (median 32).
Interventions: Fractional CO2 (scanner density 5%-20%, pulse energy 10-40 mJ) for scars/pigment; surgical CO2 (continuous wave, 4-8 W) for excisions (Figure 2).
How we select the patients and how we do the laser: A patient consults us for their various problems like acne scars, pigmentation, uneven skin tone, keloids or various skin lesions such as moles, warts and other macular localised lesions. We classify them as to whether they will need a fractional CO2 laser or surgical CO2 laser and explain the whole process to them. Next, we apply Prilox cream to the concerned areas for topical anaesthesia and wait for around 25–30 min. For various localised skin lesions, we inject local anaesthesia too, just before proceeding with surgical CO2 so that the procedure is completely painless. Now the laser procedure is done, which takes around 15 to 20 min for fractional CO2 (if for the whole face) or around 5 min for surgical CO2 (if for a few skin lesions). Then the patient washes their face, ice application is done, and a healing cream (like Hydroheal Nova) is applied all over. Post-procedure instructions are given, like not to expose the lasered area to any form of heat for 4–5 days, use a sunscreen and moisturiser regularly and to review with us after 1 week. For cases of uneven skin tone, we generally need two to three sittings of fractional CO2 laser, which is around three to four sittings for pigmentary lesions, around five to seven sittings for acne scars, and around six to eight sittings for burn/trauma scars to improve. Surgical CO2 laser gives results in a maximum of one to two sittings for various localised skin lesions to be treated. We do regular followups and make sure that our patients do not get hyper/hypopigmented and put them on various topical agents accordingly.
Outcomes: Lesion clearance, patient satisfaction (Likert scale).
Results
Fractional Mode
Surgical Mode
Benign lesions: 95% one-session clearance; <2% hypertrophic scars (Figures 3–6).
Uneven Skin Tone Treated with Fractional CO2.

Post-surgical (Outside Operated) Scar Correction by Fractional CO2.

Skin Tags/Mole Removal Using Surgical CO2.

Viral warts: 89% cure at 3 months (Figure 7).
Viral Wart and Skin Lesion Surgical CO2 Correction.

Comparison of Traditional versus Fractional Resurfacing Depth.
Keloids: Debulking + intralesional triamcinolone achieved ≥50% regression in 86%.
Adverse effects: Mild erythema (47%, which gets healed by healing creams), post-inflammatory hyperpigmentation (PIH) (5%-6%, mostly Fitzpatrick IV-V), one delayed hypopigmentation.
Discussion
CO2 as the Gold Standard
Water absorption properties make CO2 ideal for both superficial resurfacing and scalpel-like excision.
10
Our outcomes align with prior series reporting >80% acne scar improvement.4,6 The various advantages and caveats are as follows: CO2 provides precision and haemostasis, facilitating periocular and cosmetically sensitive procedures.11-16 Fractional delivery reduces downtime; however, PIH remains a concern in darker phototypes. Pre-treatment with hydroquinone or tranexamic acid mitigates this risk. The various technological trends are:
AI-driven scanners with real-time density titration.
17
Hybrid CO2 + 1570 nm systems enabling deeper dermal thermolysis. Adjunctive biologic therapies (written below).
The various adjunctive therapies are as follows:
Recent studies suggest synergy between CO2 lasers and biologics.
Stromal vascular fraction (SVF): Meta-analysis shows CO2 + SVF outperforms CO2 alone in hypertrophic scar outcomes.8,18,19
Exosomes: Split-face RCT showed greater acne scar reduction with less erythema and shorter downtime.8,18,19
Platelet-rich plasma (PRP): Enhances acne scar improvement when combined with CO2 versus laser alone. 20
Limitations and Future Work
Retrospective design and single-centre scope limit generalisability.
Future priorities:
Prospective RCTs in Asian skin comparing CO2, Er:YAG and picosecond platforms. Controlled trials of CO2 combined with SVF, PRP, exosomes and stem cells. Standardisation of adjunct protocols and long-term durability studies.
Conclusion
CO2 lasers remain a cornerstone of aesthetic and minor surgical practice/dermatology. Our 8-year data confirm their versatility, safety and predictability across diverse indications. Adjunctive biologic therapies—SVF, PRP, exosomes and stem cells—represent a promising frontier. AI-guided systems and combination regimens are poised to extend the clinical primacy of CO2 in cutaneous laser surgery.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Patient Consent
All procedures were conducted in accordance with the ethical standards of institutional practice. Patient confidentiality was maintained, and informed consent was obtained for treatment and for the use of anonymised data/images for academic and publication purposes.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.