
Abstract
Introduction:
Acne scarring is a very common problem, which can be extensive, and may lead to significant psychosocial morbidity. Multiple types of treatments are used to ameliorate atrophic scars with varying degrees of success. This paper provides an overview of the various energy-based modalities that are commonly employed against acne scarring.
Objectives and methods:
A comprehensive literature search of papers published since 2008 was performed in order to determine the efficacy and adverse reactions of commonly used energy-based treatments against post-acne scarring.
Results:
A total of 59 relevant articles were identified covering a multitude of different devices.
Discussion:
Ablative lasers seem to achieve the highest degree of efficacy, albeit this is associated with significant pain and downtime, and the risk for long-term pigmentary changes. Non-ablative fractional photothermolysis (FP) has a much safer profile but cannot achieve as good cosmetic results. The efficacies of fractional radiofrequency microneedling and radiofrequency are slightly inferior to that of FP but offer an even safer adverse profile. Little evidence is available on the remaining devices, with larger studies required in order to reach more solid conclusions.
Conclusion:
Multiple devices have been used with varying levels of efficacy and very different safety profiles. There is an overall lack of high-quality evidence about the effects of different interventions. Furthermore, no standardised scale is available for acne scarring, leading to variability in evaluation and interpretation of data in different studies.
Introduction
Scarring is the main complication of acne and arises from the disorganised production and deposition of collagen around inflamed follicles, resulting in visibly depressed scars. 1 Such scarring is very common and can lead to impairment in quality of life, as well as being a risk factor for depression and even suicide. Furthermore, it has been linked to poor self-esteem, anxiety and lowered academic performance. 2
Despite the wide array of methods available to improve the appearance of acne scarring, no ‘gold standard’ modality has emerged to date that will clear such scars completely and consistently. Newer treatments and the combination of multiple modalities could therefore be key in achieving consistent results in a large percentage of patients, even in those with severe scarring.
Therapeutic interventions can be generally split into energy- and non-energy-based techniques.
Commonly employed non-energy-based methods include chemical peels, subcision, microneedling, dermabrasion and tissue augmentation with a variety of fillers. These have been covered in part 1 of this literature review. 3
Energy-based modalities can be further divided into light-based modalities, lasers and radiofrequency devices.
Lasers are the commonest employed modality and come in different types. Traditionally, ablative lasers were widely used in the past due to their ability to produce good cosmetic results after only one treatment. 4 Ablative methods work by removing the epidermis and part of the dermis on the affected areas, leading to subsequent neocollagenesis and remodelling; 5 however, the association of the ablative lasers with extended recovery periods and other untoward side effects has led to the increasing use of the safer fractional and non-ablative technologies. 4
Unlike traditional ablative means, fractional ablative lasers utilise regularly spaced arrays over a fraction of the skin surface. These induce thermal ablation in microscopic columns of epidermal and dermal tissue while sparing the remaining skin. This approach leads to significantly faster recovery times when compared to traditional ablative resurfacing. 6
Non-ablative lasers, on the other hand, are able to cause thermal injury in the dermis while preserving the epidermis from any ablation. This process is known as fractional photothermolysis (FP) and limits side effects and recovery time even further. 7
With radiofrequency (RF) devices, electrical current flows through the skin between the electrode-pin rows generating deep dermal heating. This in turn induces skin injury eliciting a healing response and stimulating the remodelling of dermal collagen. 8
The microneedling RF (MRF) method consists of multiple needles that enable the delivery of RF directly to the dermis. The needles are insulated to prevent electrothermal damage from occurring anywhere but at the very tip of the needle and never in the epidermis, which undergoes purely mechanical needling. In contrast to ablative and non-ablative lasers, treatment with MRF can be controlled by varying the depth of the needles, thus allowing for discrete electrothermal coagulation at different levels of the dermis.9,10
Objectives and methods
The aim of this paper is to provide with an overview of the most up-to-date energy-based treatments used in acne scarring.
A comprehensive literature search of papers published since 2008 was performed on PubMed. A search using the keywords [(scar(s), scarring) AND (acne)] was utilised. Only original articles written in English were included. Individual case reports were excluded. Following screening of abstracts, a total of 59 relevant articles were selected.
Results
A total of 59 relevant articles were included in this review. These have been categorised according to research methodology and modality.
Randomised controlled trials
Twenty-three randomised controlled trials (RCTs) were identified (Table 1).
A synopsis of all randomised controlled trials.

Joanna Briggs Institute classification.
CO2 laser
Ten papers focused on the efficacy of the CO2 laser. In the largest RCT in this group (42 patients), Faghihi et al. compared treatment with punch elevation alongside fractional CO2 laser resurfacing (21.4% minimal response, 42.9% moderate, 35.7% good) against that of isolated CO2 laser resurfacing (26.2% minimal response, 42.9% moderate, 31% good). 11
In other large trials, Zhang et al. (33 patients) compared fractional microplasma radiofrequency (RF) (56.4% mean improvement) to the fractional ablative CO2 laser (59.2%). 12
Gawdat et al. (30 patients) assessed the efficacy of the fractional ablative CO2 laser combined with either saline (excellent improvement in 26.7%), intradermal platelet rich plasma (PRP) (excellent improvement in 66.7%) or topical PRP (excellent improvement in 60%). 13
Ahmed et al. (28 patients) found the efficacy of CO2 laser pinpoint irradiation to be superior to that of chemical peeling (trichloroacetic acid chemical reconstruction of skin scars – TCA CROSS technique). 14
One study (16 patients) studied the effects of the ablative fractional CO2 laser either in isolation (31.2% little or no response, 68.8% fair or good response) or alongside with intradermal PRP (12.5% little or no response, 87.5% fair or good response). 15 Another study (12 patients) achieved good improvement in scar texture and atrophy with the ablative fractional CO2 laser. 7 Compared to the non-ablative fractional Er-Glass laser, Cho et al. (eight patients) achieved slightly superior results with the ablative fractional CO2 laser. 16
Kim et al. (20 patients) assessed the response of high-energy (two patients had 30–49% improvement and eight had 50–69% improvement) and low-energy (seven patients had 10–39% improvement and three had 40–59% improvement) ablative fractional CO2 laser resurfacing as well as that of fractional ablative CO2 laser resurfacing combined with non-ablative Nd:YAG resurfacing (one patient had 40–49% improvement, seven had 50–59% improvement, nine had 50–69% improvement and three had 60–69%). 17
Yuan et al. (20 patients) reviewed the effects of three different energy and density settings of the fractional CO2 laser (20mJ, 10% vs. 20mJ, 20% vs. 10mJ, 10%). Results were comparable across all three groups, but with somewhat efficacy in the higher-energy higher-density group. 18
Finally, Bjørn et al. (11 patients) assessed the response of acne scars to treatment with the fractional CO2 laser at either one- or three-month intervals. 19 Results were significant in efficacy and comparable across both groups.
Er:Glass fractional photothermolysis
Seven RCTs were included in this category.
Cachafeiro et al. (42 patients) compared Er:Glass laser to microneedling (mean improvement of 3.41% and 4.05%, respectively), 2 and Ronsgaard et al. (20 patients) compared Er:Glass to bipolar RF (mean improvement of 2.86% ± 0.42 and 2.70% ± 0.37, respectively). 8
Another study (40 patients) reported moderate but slightly superior results with the Er:Glass against those achieved with fractional radiofrequency microneedling (FRM). 1
One study (39 patients) compared isolated Er:Glass FP (59.79% improvement) to that of FP plus percutaneous collagen induction (PCI) (61.83% improvement) and also against PCI plus 20% TCA (78.27% improvement). 20
Kim et al. (18 patients) compared the Er:Glass laser to the TCA CROSS method (average improvement of 2.51% and 2.44%, respectively) 21 and Yang et al. (30 patients) compared it to asiaticoside cream (mean improvement of 5.65% ± 4.34 and 1.23% ± 3.41, respectively). 22
The final study in this category (seven patients) reported significant and comparable improvement in appearance, with both high- and low-energy levels of Er:Glass photothermolysis. 23
Er:YAG fractional photothermolysis
Three studies utilised this modality.
Min et al. (24 patients) displayed superior efficacy with the Er:YAG laser (50% mean improvement) compared to the combination of bipolar RF and the non-ablative infrared diode laser (25% mean improvement). 24
Mahmoud et al. (15 patients) attained mild improvement with both 10-mJ and 40-mJ energy settings of the Er:YAG laser. 25 Wanitphakdeedecha et al. (24 patients), on the other hand, found that 72.7% of patients achieved > 50% improvement with the 300-ms wavelength, whereas only 63.6% achieved > 50% improvement with the 1500-ms wavelength. 26
Other modalities
The remaining RCTs studied a mixture of energy devices.
Min et al. (20 patients) assessed the efficacy of FRM against that of bipolar RF and found FMR to be superior, especially against ice-pick and boxcar scars. 27
In a different paper, Min et al. (19 patients) studied the effects of treatment with the long-pulse Nd:YAG laser either in isolation (27% improvement) or in combination to the PDL laser (32.3% improvement). 28 Both modalities were found to be effective at treating superficial rolling and boxcar scars but ineffective at treating deep and ice-pick scars.
Finally, one study (30 patients) compared high- to moderate-energy bipolar fractional RF. 29 Scar appearance was significantly reduced in both groups but high-energy settings demonstrated superior efficacy.
Non-randomised controlled trials
Two non-RCTs were identified (Table 2).
A synopsis of all non-RCTs.
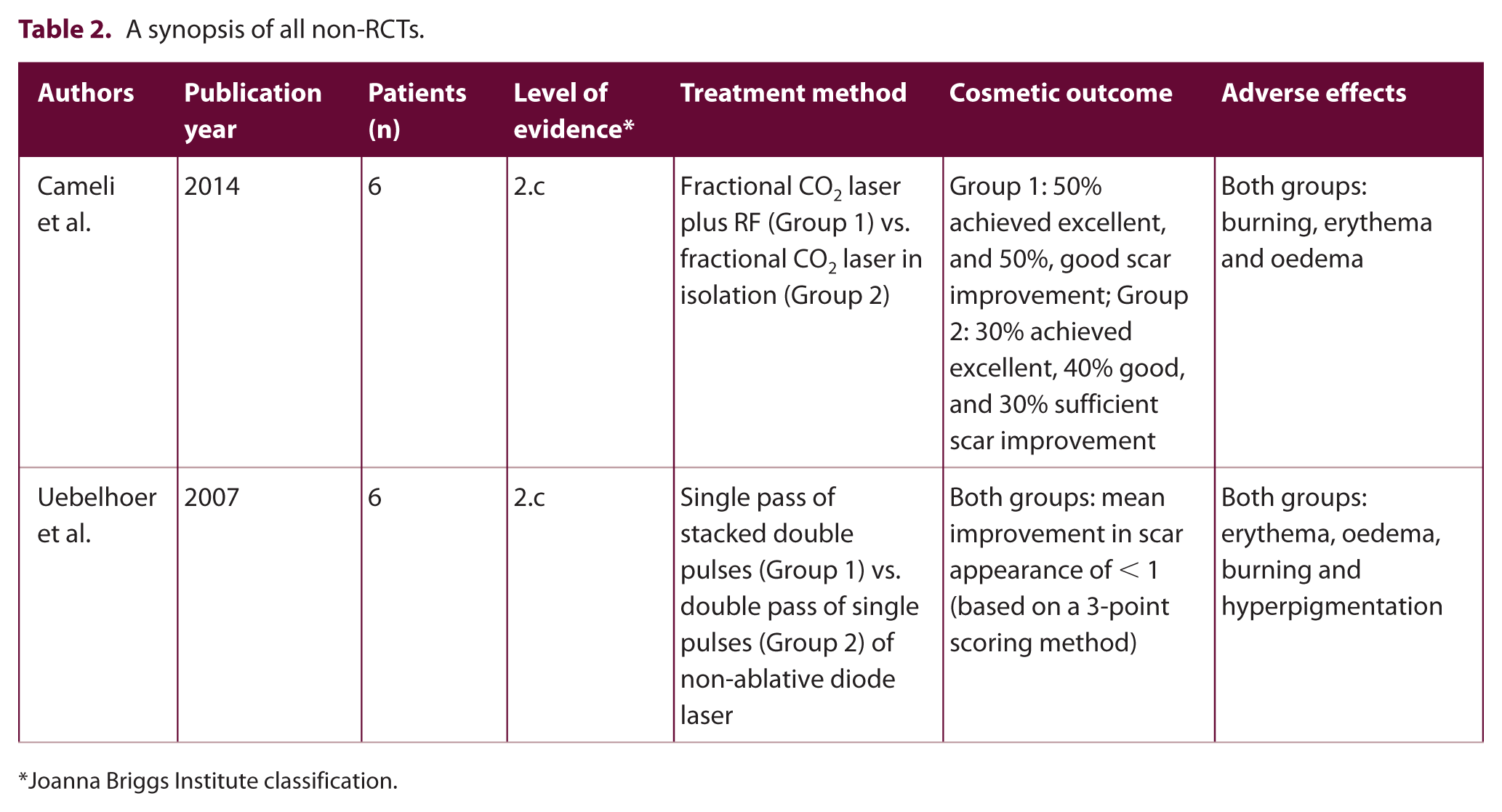
Joanna Briggs Institute classification.
In a study of six patients, Cameli et al. compared treatment with fractional CO2 laser plus RF (50% achieved excellent and 50% good scar improvement) against that of fractional CO2 laser in isolation (30% achieved excellent, 40% good and 30% sufficient scar improvement). 30
Uebelhoer et al. treated six patients with the non-ablative diode laser, either with a single pass of stacked double pulses or with a double pass of single pulses. 31 In both groups, mean improvement in scar appearance was minimal.
Retrospective studies
Four papers were included in this category (Table 3).
A synopsis of all retrospective studies.

Joanna Briggs Institute classification.
Alajlan et al. compared the efficacy of the non-ablative Er-doped fractional laser (77% attained > 25% improvement and 35% attained > 50% improvement) against that of fractional ablative CO2 laser (70% attained > 25% improvement and 37% attained > 50% improvement). 34
Chan et al. assessed the effects of the non-ablative fractional Er-doped fibre laser by comparing full (mild improvement in 23.1%, moderate in 7.7%, good in 15.4%, excellent in 53.8%) against mini resurfacing (mild improvement in 0%, moderate in 13.3%, good in 40%, excellent in 46.7%). 33
Using the fractional ablative CO2 laser, Kim et al. achieved moderate improvement in appearance across the vast majority of patients, 34 whereas with the use of the non-ablative Nd:YAG laser Badawi et al. achieved moderate results. 35
Observational studies
A total of 30 observational studies have been included in this review article, which are summarised in Table 4.9,10,36 –63
A synopsis of all observational studies.

Joanna Briggs Institute classification.
Discussion
The ablative fractional CO2 laser was identified as the modality with the most available evidence (20 studies), followed by the Er:Glass laser and RF (18 and 13 studies, respectively). Interestingly, no studies in this review were found to have used fully ablative, non-fractional CO2 lasers.
A critical review of the existing studies shows that CO2 ablative fractional resurfacing (AFR) achieved improvement in appearance that ranged from modest to excellent in most of the studies. Rolling and boxcar scars were found to respond the best while ice-pick scars responded the least. 48 Interestingly, combining the CO2 laser with punch elevation was found to be beneficial against such deeper scars. 11
The efficacy of the CO2 laser was synergistic to treatment with the Nd:YAG laser. 17 However, complementary use of platelet rich plasma (PRP) yielded contradictory results across different studies.13,15
In direct comparison, CO2 laser AFR was found to be superior to both Er:Glass FP and TCA CROSS.14,16
The risk of developing hyperpigmentation was heavily influenced by treatment parameters, with more aggressive regimes causing hyperpigmentation in as high as 55–100% of patients. 18 This risk can, however, be brought down further by employing a number of different interventions. These include using lower treatment densities and pulsed energies, avoiding sun exposure and using broad-spectrum sunblock, and utilising pre-treatment bleaching agents. 18 Lengthening the treatment interval was theorised to lead to fewer adverse effects; however, this was not demonstrated in practice. 19
Er:Glass FP is commonly employed for multiple cosmetic purposes, including the treatment of rhytides, stretch marks and melasma. 36 It is also widely used against acne scarring with moderate efficacy. More specifically, much better results can be achieved against boxcar and rolling scars, than against ice-pick scars. 54 Even though comparison FP and the TCA CROSS method achieved similar outcomes, closer scrutiny reveals that FP is more effective against rolling scars, whereas the CROSS method has a better effect against ice-pick scars.20,21 This is likely due to the fact that ice pick scars are deep and the thermal effect of FP cannot reach their base in order to induce stimulation of the dermis and lead to collagen remodelling. 21
Overall, results were comparable to those achieved by RF. However, FP is associated with higher levels of procedural discomfort. 8 Other adverse reactions are mild and of short duration and can be further reduced by employing lower energy densities. 33
RF energy, unlike lasers, is not absorbed by melanin, making this modality potentially safer in individuals with dark skin.30,55
In general, RF achieved moderate results and was found to be more effective against ice-pick than other types of scars. 53 However, treatment was particularly effective when combined with certain other modalities such as acoustic pressure ultrasound, Er:YAG, diode and CO2 lasers.8,24,30
Overall, the main advantage of the RF modalities is their low profile of side effects, especially that of hyperpigmentation, and the low downtime associated with their use.51,53
Even though no direct comparison with FRM is available, efficacy seems to be better against rolling and boxcar type scars. 9 Results seem to be inferior to those achieved by ablative resurfacing, and comparable but slightly inferior to those achieved by FP. 1
Combined treatment with FRM and sublative fractional radiofrequency lead to excellent outcomes with apparent synergistic effects between the two modalities, while maintaining a safe profile. 10
Because FRM affects a smaller fraction of the epidermis than most lasers (5% in FRM vs. 10–70% in FP), it was also associated with milder pain, lesser frequency and extent of hyperpigmentation, and shorter downtime. 1 Therefore, FRM may be a good option in patients who are sensitive to pain, those at risk of hyperpigmentation (darker skin phototypes or prior history of post-procedural hyperpigmentation) or those who prefer a shorter downtime.1,9
The long-pulsed Nd:YAG achieved moderate efficacy against atrophic acne scars, mainly superficial boxcar and rolling scars, with measurable and statistically significant increase in the number of collagen fibres.28,35,46 Combination treatment with the Nd:YAG and PDL lasers leads to synergistic effects. 28
The picosecond laser is a promising modality in this field. Unfortunately, small numbers of patients were treated with this laser as only one study utilised a 755-nm picosecond laser with a diffractive lens array. Results showed a 25–50% improvement against rolling type scars with minimal pain, little downtime and no pigmentary changes. 37
The efficacy of the non-ablative diode in isolation has been found to be low against acne scars while also leading to significant discomfort (especially in those with darker skin).24,31
Even though the efficacy improved when treatment was combined with RF, it is unclear whether any synergistic effects were manifested.24,55,62
The ablative YSGG laser achieved excellent improvement in appearance, in the range of 40–90%. However, given the small numbers of patients treated with this device, it is hard to judge the place of this modality in the overall treatment pathway of acne scars. Further studies are required to reach more conclusive results.
The plasma skin regeneration system (PRS) has been advocated as an alternative to ablative and fractional resurfacing lasers. It utilises RF in order to convert nitrogen gas into plasma. The plasma is then directed onto the skin via a hand-piece, delivering thermal energy in a precise manner. 43 Efficacy against acne scars was found to be moderate.
Benefits of this device include a lower cost, better safety and shorter downtime than ablative devices, and less training required for the operator. 43 It is also worth noting that significant discomfort and hyperpigmentation are potential drawbacks to its use. 43
One of the main problems of reviews in this field lies in the difficulty of comparing outcomes. Although several different grading systems have been proposed to standardise acne scar classification and evaluation, there is no universal accepted scale. Similarly, there is no widely accepted device for measuring acne scar improvement in a reproducible and objective fashion. The lack of such standardisation has led to great variability in evaluation and interpretation of data across different studies.37,54
Another important drawback lies in failing to identify the type of atrophic scar being treated. The depth of penetration of most lasers seems appropriate to ameliorate most superficial and some deeper scars (rolling and boxcar scars); however, ice-pick scars extend vertically to the deep dermis or subcutaneous tissue and are likely deeper than the depth that can be reached with conventional lasers. 54 Because acne scars are usually a mix of ice-pick, boxcar and rolling scars, the final effect of fractional lasers would likely depend more on the predominant scars than on the fractional laser being used. 54
Conclusions
Multiple devices have been used with varying levels of efficacy and very different safety profiles.
There is an overall lack of high-quality evidence about the effects of different interventions because of poor methodology, underpowered studies and different scarring subtypes being assessed. Furthermore, no standardised scale is available for acne scarring, leading to variability in evaluation and interpretation of data in different studies.
Ablative lasers seem to achieve the highest degree of efficacy among all devices tested, albeit this is associated with significant pain and downtime, and the risk for long-term pigmentary changes. Non-ablative FP has a much safer profile but does not achieve as good cosmetic results. The efficacy of FRM and RF is slightly inferior to that of FP but offers an even safer adverse profile. Little evidence is available on the remaining devices, with larger studies required to reach more solid conclusions.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.