
Abstract
Introduction:
Burn scars cause cosmetic disfigurement and psychosocial distress. We present two Fitzpatrick phototype (FP) III patients with burn scars successfully treated with combination pulsed dye laser (PDL) and non-ablative fractional lasers (NAFL).
Case 1:
A 30-year-old, FP III woman with a history of a second-degree burn injury to the bilateral arms and legs affecting 30% body surface area (BSA) presented for cosmetic treatment. The patient received three treatments with 595 nm PDL (7 mm, 8 J, 6 ms), six with the 1550 nm erbium:glass laser (30 mJ, 14% density, 4–8 passes) and five with the 1927 nm thulium laser (10 mJ, 30% density, 4–8 passes). Treated burn scars improved significantly in thickness, texture and colour.
Case 2:
A 33-year-old, FP III man with a history of a second-degree burn injury of the left neck and arm affecting 7% BSA presented for cosmetic treatment. The patient received two treatments with 595 nm PDL (5 mm, 7.5 J, 6 ms), four with the 1550 nm erbium:glass laser (30 mJ, 14% density, 4–8 passes) and two with the 1927 nm thulium laser (10 mJ, 30% density, 4–8 passes). The burn scars became thinner, smoother and more normal in pigmentation and appearance.
Discussion:
Our patients’ burn scars were treated with a combination of PDL and NAFL (two wavelengths). The PDL targets scar hypervascularity, the 1550 nm erbium:glass stimulates collagen remodelling and the 1927 nm thulium targets epidermal processes, particularly hyperpigmentation. This combination addresses scar thickness, texture and colour with a low side effect profile and is particularly advantageous in patients at higher risk of post-procedure hyperpigmentation.
Conclusion:
Our cases suggest the combination of 595nm PDL plus NAFL 1550 nm erbium:glass/1927 nm thulium device is effective and well-tolerated for burn scar treatment in skin of colour.
Lay Summary


While all scars can be bothersome, burn scars can be particularly troubling. They can be large, itchy, painful and limit range of motion. Patients with medium and darker skin tones may be more likely to develop dark and discoloured scars due to burns and other scarring injuries. In our case series, we used two types of lasers to treat thick, darkly pigmented burn scars in two patients with medium and darker skin tones. While the pulsed dye laser targets the redness and thickened aspects of scars to restore a more normal appearance, the non-ablative fractional resurfacing laser creates microscopic zones of controlled injury to resurface scars, stimulate new collagen growth, improve texture and lighten excess pigmentation. Treatments were performed once a month for 6–12 months. Using these lasers in combination, our treatment method made our patients’ scars thinner, smoother and more evenly coloured over time, resulting in a more natural appearance. This multi-modal approach was a safe and effective no-downtime method for the improvement of scars in skin of colour patients.
Keywords
Introduction
Burn scars cause significant morbidity due to cosmetic disfigurement, contractures and associated symptoms such as pain and pruritus, and psychosocial distress. 1 Patients with burn scars often have a diminished quality of life, difficulties with social interactions and frequently suffer from anxiety, depression and low self-esteem. 2 While advancements in care have dramatically decreased mortality from burn injuries, the management of burn scars remains quite challenging.3,4 Mainstay treatments for burn scars include silicone gel sheeting, scar massage therapy, compression garments, cryotherapy, corticosteroid injections and surgical interventions, but outcomes are variable. 1
Fractional lasers now play a prominent role in the treatment of burn scars, with ablative fractional lasers being the gold standard. However, ablative lasers are undesirable to many patients due to prolonged downtime and the increased risk of extensive side effects, especially in patients with darker skin tones who are more prone to post-laser hyperpigmentation.5–7 Non-ablative fractional lasers (NAFL) present a viable alternative in treating burn scars in patients who are concerned about potential adverse effects and desire a less aggressive, more gradual treatment approach. 8
Case presentations
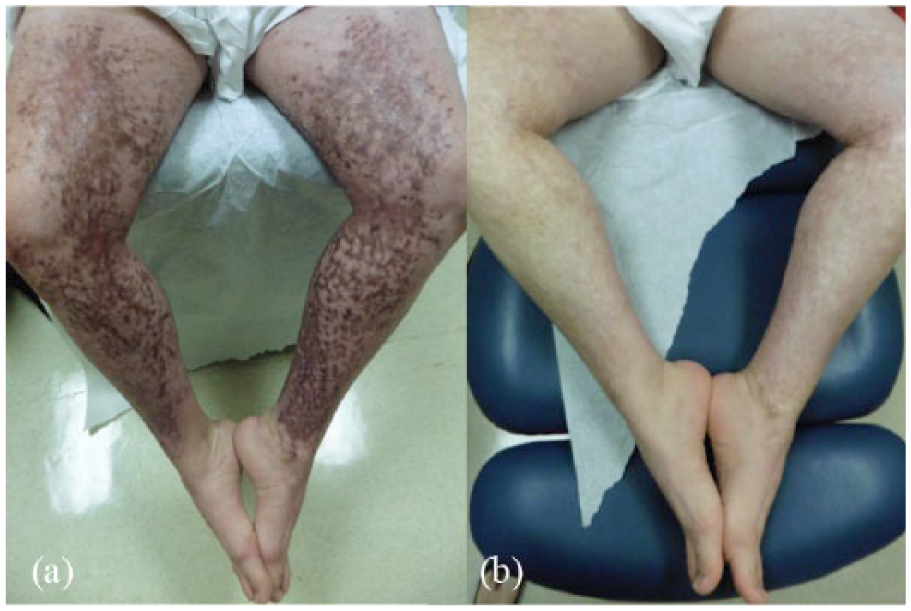
(a) Burn scars on the bilateral lower extremities before treatment. (b) After 12 months.

(a) Burn scars on the dorsal hand before treatment. (b) After 12 months.
The patient was treated with both the 595-nm pulsed dye laser (PDL) (Vbeam Perfecta, Syneron Candela, Wayland, MA, USA) and a NAFL dual wavelength device (Fraxel DUAL, Solta Medical, Hayward, CA, USA). Topical EMLA cream was applied to the treatment areas under occlusion 1 h before each procedure. She received three treatments with the PDL (7 mm spot size, energy 8 J, pulse duration 6 ms, 30:20 dynamic cooling), six treatments with the 1550 nm erbium:glass laser (energy 30 mJ,14% density, 4–8 passes) and five treatments with the 1927 nm thulium laser (energy 10 mJ, 30% density, 4–8 passes) to the bilateral upper and lower extremities. Treatments were spaced approximately one month apart. Immediate post-treatment care included application of triamcinolone 0.1% cream twice daily for three to four days and broad-spectrum sunscreen. Adjuvant therapy included a one-time 1 mL of triamcinolone acetonide (20 mg/mL) injected intralesionally to a symptomatic hypertrophic scar on the left hand. Tacrolimus 0.1% ointment was applied twice daily to hyperpigmented scars on the legs throughout the course of treatment. Treated burn scars became softer, thinner and more normal in texture and pigmentation with significant overall cosmetic improvement (Figures 1b and 2b). The laser treatments were very well-tolerated with no downtime, with minor pain during the procedure being the only adverse effect. The patient also reported improved mood and decreased pain and pruritus associated with her scars and was able to discontinue gabapentin therapy.

(a) Burn scars on the left upper extremity before treatment. (b) After six months.

(a) Non-scarring alopecic patch on the left postauricular scalp. (b) After four monthly sessions of intralesional triamcinolone acetonide injections.
The patient was treated with a 595 nm PDL and the NAFL dual wavelength device. He received two treatments with the PDL (5 mm spot size, energy 7.5 J, pulse duration 6 ms, 30:20 dynamic cooling), four treatments with the 1550 nm erbium:glass laser (energy 30 mJ, 14% density, 4–8 passes) and two treatments with the 1927 nm thulium laser (energy 10 mJ, 30% density, 4–8 passes). All treatments targeted the left upper extremities and neck. Topical EMLA cream was applied under occlusion to the treatment area 1 h before the procedure. At two of his sessions, both non-ablative lasers (1550 and 1927 wavelengths) were used sequentially over the affected areas. Treatments were spaced approximately one month apart and were well-tolerated. Post-treatment care included application of triamcinolone 0.1% cream twice daily for three days and broad-spectrum sun protection. Adjuvant therapy included continued scar massage. There was vast improvement in the appearance of the scars with regard to both texture and skin colour (Figure 3b). His alopecia areata resolved with four monthly sessions of intralesional triamcinolone acetonide injections (concentration 10 mg/mL, volume 0.5–2.5 mL) (Figure 4b).
Discussion
There is increasing demand for better non-surgical options in scar management. The use of fractional laser devices represents a major advancement in the treatment of scars. Fractional resurfacing lasers insert hundreds of evenly distributed columns of thermal injury, referred to as microscopic treatment zones (MTZ), into the dermis.1,9 Untreated skin between MTZs promotes rapid post-procedure healing and collagen remodelling. Fractional resurfacing lasers have shown efficacy in improving thickness, pliability, pigmentary changes and textural abnormalities in both early and mature scars. 5
NAFL is a type of fractional laser that produces a more superficial injury to the dermis while sparing the overlying epidermis compared to ablative fractional lasers (AFL) that cause injury to both the epidermis and dermis.10,11 AFLs are more effective at treating thicker, hypertrophic or contracted scars because they stimulates a more vigorous remodelling response, while NAFLs are more beneficial in treating scar dyschromia.5,9 However, NAFLs are associated with less post-procedural downtime and have a significantly lower risk of producing undesirable side effects.6,12, Potential adverse effects of fractional resurfacing lasers include prolonged erythema, swelling, blistering, post-inflammatory hyperpigmentation (PIH) and pain.6,7
Our patients’ burn scars achieved significant clinical improvement with a NAFL device containing two lasers, the 1550 nm erbium:glass and 1927 nm thulium, and the 595nm PDL device. The 1550 nm wavelength injures the dermis to stimulate collagen remodelling while the 1927 nm wavelength targets dyspigmentation by shuttling melanin into collections of microscopic epidermal necrotic debris just above the MTZs which are subsequently shed after one to two weeks.10,11 This laser combination of two wavelengths addresses scar thickness, texture and hyperpigmentation with a low side effect profile. This device may be especially advantageous in patients with skin of colour who tend to develop more pigmented burn scars and are at an increased risk of developing PIH after resurfacing treatments, a side effect that may last several years.6,13–16 Treatment factors reported to reduce the likelihood of PIH and other post-treatment adverse events include using lower fluences, reduced treatment densities and fewer treatment passes.5,6,17 Additionally, strict sun avoidance pre- and post-procedure for at least one to two weeks before and after a NAFL treatment must be emphasised. 7 The NAFL combination device has also been shown to improve range of motion limited by scar contracture in a report by Finney et al. 18 The PDL was added to address mainly erythema, pruritis and scar thickness by preventing excessive collagen accumulation and promoting collagen remodelling via selective photothermolysis of scar vasculature resulting in scar tissue hypoxia.4,9,10,19
The darkly pigmented scars on the lower extremities of our first case improved dramatically using the thulium laser. Previous literature has discussed the utilisation of the 1927 nm thulium laser in treating many different hyperpigmentation disorders. The thulium laser is frequently used to treat melasma with minimal side effects; however, many patients had experienced some recurrence and required repeat sessions.20–23 Lee et al successfully treated a patient with truncal PIH related to cupping using the thulium laser over four sessions. Another study found that acquired facial hyperpigmentation can be managed using a combination of topical anti-inflammatory agents and the thulium laser. 24 Additionally, several reports have studied the laser’s efficacy in treating photo-damage induced pigmentation and found that the thulium fractional laser can dramatically improve the appearance of dyspigmentation, ephelides, lentigines and keratosis.25–28 In all of these applications, most of the data are only pertinent to patients with a FP of less than V. To our knowledge, our case series is the first report using the 1927 nm thulium laser to as part of a multimodal approach to specifically address burn scar hyperpigmentation.
In our first case, tacrolimus ointment was used in conjunction with the laser treatments to address hyperpigmentation and reduce scarring in the bilateral lower extremities. Tacrolimus is a calcineurin inhibitor that prevents the activation of T-cells. 29 Its topical form is most commonly used to treat atopic dermatitis but has many off-label indications such as scarring due to its immunomodulating effects that may reduce inflammation and low side-effect profile. 30 There is limited evidence that suggests tacrolimus may ameliorate scarring by modulating collagen pathways and synthesis.31,32 However, the exact mechanism is not known and further studies are needed to define its role in managing scars. Kim et al report of a keloid that resolved after application of topical tacrolimus, possibly due to its ability to inhibit gli-1 signal transduction, which is overexpressed in keloids. 33 A few studies have utilised topical tacrolimus to successfully treat pigmentation conditions including acquired facial hyperpigmentation and erythema dyschromicum perstans.28,34
Conclusion
Our cases suggest the NAFL 1550 nm erbium:glass/1927 nm thulium device is effective and well-tolerated for burn scar treatment in darker skin types and can be used in combination with the 595-nm PDL and topical tacrolimus. The thulium laser specifically addresses hyperpigmentation, which is advantageous in patients with skin of colour who are more prone to developing PIH. Further studies are needed to optimise settings and establish treatment guidelines.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
The authors confirm that the necessary written, informed consent was obtained from patients for this article.