
Abstract
Background:
The appearance of well-defined abdominal musculature (‘six-pack abs’) is considered a symbol of male fitness. Traditional liposuction techniques focused on deep fat removal without detailed sculpting. High-definition liposuction (HDL) and abdominal etching have evolved to precisely remove superficial fat and enhance muscular contours using advanced technologies like power-assisted liposuction (PAL) and ultrasound-assisted liposuction (UAL). The aim of this study was to evaluate the safety, effectiveness, and patient satisfaction of PAL- and UAL-assisted HDL with radiofrequency skin tightening for six-pack abs creation in male patients.
Methods:
A retrospective study was conducted at an aesthetic centre in New Delhi between November 2021 and October 2024. Forty-five male patients with a BMI ≤30 underwent HDL for six-pack abs creation. Preoperative assessment included medical history, clinical examination, and imaging when necessary. The surgical technique involved tumescent infiltration, PAL for fat debulking, UAL (VASER) for emulsification, and subdermal sculpting with fine cannulas. Radiofrequency-assisted skin tightening was performed for enhanced definition. Postoperative care included compression garments, lymphatic drainage, and structured follow-ups. A five-point Likert scale was used to assess satisfaction level.
Results:
The mean patient age was 39.5 ± 8 years, with a mean BMI of 26.2 ± 1.75. The average lipoaspirate volume was 2500 mL. At the 6-month follow-up, patient satisfaction was notably high, with 80% reporting being highly satisfied and an additional 15.6% expressing satisfaction. No major complications were observed; however, two patients developed seromas, which were managed conservatively.
Conclusion:
PAL and UAL-assisted HDL combined with radiofrequency skin tightening enable safe and effective six-pack abs creation in male patients. This approach enhances body-contouring precision, expands eligibility beyond lean individuals, and achieves high patient satisfaction with minimal complications.
Keywords
Introduction
The appearance of the topography of the anterior abdominal musculature, or ‘abs’, is considered a symbol of male fitness in contemporary times. 1 With age or compromised fitness, subcutaneous adipose tissue tends to accumulate in the anterior abdominal region, obscuring this topographic anatomy. However, vigorous exercise and a strict diet are not always enough to provide men with the desired appearance of their abdominal muscles. Even with an adequate muscle volume, the muscle outline cannot be visualised if the total body fat is beyond 15%. 2
Early liposuction techniques focused on deep fat layer extraction of the abdomen to reduce volume, and hence were limited to generalised reshaping rather than detailed sculpting. Surgeons avoided any superficial liposuction because it risked significant contour irregularities.
High-definition liposuction (HDL) and abdominal etching developed in the last two decades to address this issue. 3 In addition to removing fat, they enhance the body’s natural contours to create a sculpted, athletic appearance by precisely removing superficial fat and defining muscle structures. These procedures have evolved significantly over the years, incorporating various technologies and techniques to improve outcomes and safety. 4
The aim of the present study is to evaluate the safety, effectiveness, and patient satisfaction of six-pack abs creation in male patients using power-assisted liposuction (PAL) and ultrasound-assisted liposuction (UAL)-assisted HDL combined with radiofrequency skin tightening at our centre over a 3-year period.
History and Evolution
Early liposuction methods remained limited to deep fat layer removal, often resulting in uneven contours and skin laxity. The 1990s saw pioneering work by Gasparotti and Souza Pinto, who demonstrated that superficial fat layer manipulation could enhance contouring precision. 5 However, manual extraction with traditional cannulas posed significant risks—including over-resection, causing skin laxity, mottled skin, and permanent irregularities. Conservative guidelines emerged, advising surgeons to ‘spare 1 cm from the dermis’, which limited artistic potential.
Mark Gilliland first described abdominal etching by liposuction along the Linea semilunaris, Linea alba, and transverse inscriptions of the rectus muscle while preserving the fat over the central muscle body bordered by the muscular inscriptions, to accentuate the appearance of this musculature.6,7
In 2001, Mentz and Ersek introduced ‘abdominal etching’, using differential fat removal to accentuate the rectus abdominis muscles. This technique targeted male bodybuilders with ≤15% body fat, etching horizontal tendinous intersections and vertical Linea alba. 8 While groundbreaking, its applicability was narrow—it ignored surrounding muscle groups and required near-perfect patient physiques.
HDL or liposculpture emerged in the early 2000s as a refined and artistic approach to body contouring by Dr Alfredo Hoyos, a Colombian plastic surgeon. 3 He reimagined body contouring as three-dimensional anatomical art, drawing inspiration from Renaissance sculptors’ mastery of human form. He extended Mentz’s concept beyond isolated muscles to integrate torso, back, and limb anatomy. He refined the technique of superficial fat layer sculpting to enhance underlying muscular definition and introduced dynamic contour analysis based on patient movement and posture.
However, manual HDL was surgically gruelling, with prolonged swelling and inconsistent outcomes due to traumatic extraction methods. The introduction of newer UAL devices addressed this issue. UAL had been initially introduced in the 1990s. 9 However, early UAL devices generated excessive heat, leading to burns, skin necrosis, and prolonged recovery, restricting their use to deep fat layers and delaying superficial applications. 10
Third-generation ultrasound systems like VASER addressed these limitations through pulsed energy delivery and specialised titanium probes. Operating at 25% lower energy than predecessors, VASER enabled safe emulsification of superficial fat while preserving connective tissue. 11 Its pulsed mode further minimised thermal buildup, allowing prolonged use near the dermis—a prerequisite for detailed sculpting. This innovation laid the groundwork for combining ultrasound with artistic anatomy-based techniques. 12
VASER assisted HDL merged Hoyos’ anatomical approach with VASER’s precision, creating a reproducible method for muscular definition.
11
The procedure involves four stages:
Deep debulking: High-power VASER emulsification (80% continuous mode) reduces bulk fat. Superficial sculpting: Pulsed-mode VASER (60% power) prepares subdermal fat for shaping. Transitional blending: Fat layers are smoothed to accentuate muscle borders. Micro-suction: Fine cannulas extract emulsified fat without disrupting vascular networks.
The concept of HDL was further enhanced by Simeon Wall, Jr who introduced SAFE liposuction (separation, aspiration, fat equalisation), which ensures tissue preservation and smooth fat removal, reducing the risk of contour irregularities. 13
Dynamic Definition Liposculpture, a recent concept by Hoyos, integrates fat grafting techniques to enhance muscle contours, making the results appear more natural and proportional.3,14
Methods
Patient Selection
This retrospective study was conducted at an aesthetic centre in New Delhi between November 2021 and October 2024. During that period, 45 male patients underwent HDL with the creation of six-pack abs. Out of these, concomitant gynaecomastia correction was undertaken in 27 patients. Each patient underwent a comprehensive medical history assessment and clinical examination of the concerned body region. Routine blood investigations were performed to assess fitness for general anaesthesia. In cases with suspected hernias or previous abdominal surgeries, additional imaging, such as ultrasound or computed tomography (CT) of the abdomen, was conducted. All patients gave their written consent for surgery.
Markings
Markings were performed with the patient in a standing position. Patients were asked to flex/tone their abdominal musculature before marking. The landmarks marked were the rectus abdominis with its tendinous inscriptions, external oblique, iliac crest, and inguinal ligaments. The medial and lateral edges of the rectus muscle were marked at the Linea alba and Linea semilunaris, respectively. Transverse tendinous inscriptions of the rectus muscle are also marked separately while patients are asked to tone their abdominal muscles. This allows for clear palpation of muscle fibres’ insertion into the dermis. These lines are usually not symmetrical. The highest horizontal intersection roughly follows the downward angle of the thoracic arch. The lowest division is horizontal across the navel and is usually the most visible. Below the belly button, the vertical centreline is not as clear as on the ‘six-pack’. Usually, there is a separation only on the top part of that section, just below the belly button.
The lateral abdominal wall marking centres on the external oblique muscle complex. The marking ensures the surgeon can delineate the muscle prominence while ensuring minimal debulking to maintain the characteristic masculine bulk appearance
Inferiorly, the marking begins with identification of the inguinal crease. The lateral extensions of this marking must consider the natural skin tension lines and the patient’s desired aesthetic outcome while avoiding distortion of infra crease anatomy
Superiorly, no markings were done at the chest apart from patients who underwent simultaneous gynaecomastia correction, in whom relevant markings for gynaecomastia correction were done.
Surgical Technique (Video 1)
Antibiotic prophylaxis was performed with Injection Ceftriaxone 1 g and Injection Amikacin 500 mg as per hospital infection control policy
Back Liposuction
Following the induction of anaesthesia, the patient is initially placed in a prone position for Liposuction of the back areas. Tumescent infiltration was administered using a solution containing 1 L of normal saline, 10 mL of 2% lignocaine, one ampule of adrenaline, and one ampule of tranexamic acid. It is done from deep to superficial layers. The solution was evenly distributed using a basket cannula attached to the PAL system (Microaire Inc., Charlottesville, VA). The volume of infiltration was predetermined based on the fat to be aspirated, maintaining a ratio of 1:1 to 1:2.
Subsequently, UAL (VASER, SoltaMedical, Bothell) was performed, progressing from the superficial to the deeper fat layers. The UAL device settings were adjusted to 80% in C mode for deeper fat targeting and 70% in V mode for superficial fat removal. PAL was then utilised to aspirate the fat. This is done from deep to superficial layers. Then, fat equalisation is done using PAL without suction to smooth out any uneven areas.
Post-procedure, the lowermost ports were left open to facilitate fluid drainage. A compression dressing was then applied. Then the patient’s position is changed to the Supine position.
Six-pack Abs Creation
Stab incisions of 3 mm were made at the level of the pubis area at the lateral edge of the rectus. A stealth umbilical puncture was used for access to the Linea alba and the lowest and middle rectus inscriptions. Tumescent infiltration is done starting from the deep to the superficial layers. Next, VASER liposuction is performed from superficial to deep layers. This sequence helps to dissipate ultrasound energy and reduces the chances of thermal injury to skin. Then PAL debulking was performed, starting from the deep to the superficial layers.
Finally, subdermal liposuction is carried out along definition lines with fine 2- or 3-mm cannulas. We apply gentle pressure by pressing the skin along the movement of the cannula below the linear marking. This gives the surgeon control while also ensuring safety during finer sculpting.
Our sequence of subdermal liposuction is as follows. First, subdermal liposuction is done along the marked straight line of the Linea alba and slightly curved Linea semilunaris through the lower stab incisions. Next, using another single stab incision at the junction of the Linea semilunaris and the upper tendinous inscription of the rectus on the right side, the upper tendinous inscription is carved out on both sides. Finally, through the umbilical incision, the lower two transverse intersections were created using fine straight and bent cannulae. A bent cannula facilitates precise access to the lateral aspects of markings and prevents entry into the wrong plane. The fat between the tendinous intersections was retained or, when a thick fat layer was present, reduced to a 1-cm fat layer from the dermis.
Radiofrequency-assisted skin tightening using the EmbarceRF Body Tite (Inmode, Yokne’am Illit, Israel) system is done in all cases along the definition lines of the Linea alba, Linea semilunaris and tendinous inscriptions. Suction drains were placed through the two lower stab incisions. Gauze pieces were folded as linear bands and placed along linear depressions, which were then secured in place using an adhesive bandage. A compression dressing is done over this layer using Dynaplast adhesive bandage.
Post OP Protocol
Patients are mobilised on the same day in the evening. Patients typically stay in the hospital overnight and are discharged the next morning after dressing. Before discharge, the initial dressing was removed, and the suction drains were removed. Folded gauze pieces were replaced with linear foam pads to enhance the definition of lines. A compression garment is worn over it, and this is continued for 6–8 weeks to support healing and reduce swelling.
Five days of oral antibiotics and pain medications are prescribed to manage discomfort and prevent infection as per the hospital infection control policy. Patients are advised to stay hydrated and gradually return to a high-protein diet after two weeks. Lymphatic drainage massages are advised after 72 hours, and this is continued for at least 8–10 weeks.
Patients were followed up with a rigorous follow-up protocol. Follow-up was scheduled at Day 3, 1 week, 3 weeks, 6 weeks, 3 months, and 6 months after surgery (Figures 1–4). Patient satisfaction was assessed after 6 months using the Likert scale. Complications were also noted. Statistical analysis included profiling of subjects according to age, BMI, and satisfaction level, according to a Likert scale.
Pre- and Postoperative (8 Months) Photographs Showing High-definition Liposuction Results in a 27-year-old Male.

Pre- and Postoperative (7 Months) Photographs Showing High-definition Liposuction with Six-pack Abs Creation in a 36-year-old Male.

Pre- and Postoperative (6 Months) Photographs Showing High-definition Liposuction of the Chest and Abdomen in a 42-year-old Male.

Devices Used in High-definition Liposuction (HDL): (1) Vibrasat Pro (PAL), (2) MicroAire (PAL), (3) VASER (UAL) and (4) BodyTite (RF).

Results
Between November 2021 and October 2024, 45 male patients underwent HDL with six-pack abs creation. Concomitant gynaecomastia correction was performed in 27 of the 45 patients (60%).
The mean age of the patients in our study was 39.5 ± 8 years. All patients in the study group had a BMI of 30 or less. The mean BMI was 26.2 ± 1.75. The amount of lipoaspirate in each patient ranged from 1,500 to 3,500 mL, with a mean of 2,500 mL (2.5 L).
Most patients had no significant postoperative complications except swelling and bruising, and no adverse events were reported. However, two patients developed seromas, which were managed with aspiration and compression dressing. Both patients were also advised to undergo an extended course of lymphatic massages.
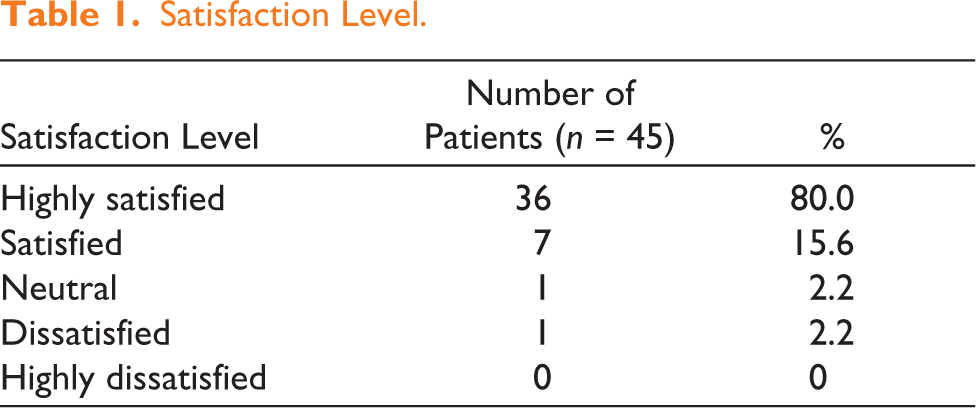
The majority of patients were satisfied or highly satisfied with their results at the 6-month follow-up. Patients rated their appearance using a 5-point Likert scale, as shown in the table below (Table 1). One patient, who rated their result as ‘dissatisfied’, had developed a postoperative seroma and required three sessions of aspiration for management.
Satisfaction Level.
Discussion
The development of PAL, UAL and RF-assisted body tightening technologies has enabled surgeons to perform large volume liposuctions together with precise superficial contouring.
Introduction of PAL significantly reduced surgeon strain during liposuction, particularly when targeting more fibrous areas. This is a crucial consideration in large-volume liposuction, as surgeon fatigue can lead to suboptimal outcomes. In PAL, the reciprocating power cannula operates at the tissue level, mirroring the manual movements executed in SAL on a minute scale. The lateral movement is minimised, thereby reducing trauma to the surrounding tissue.15,16
Mechanism of action of UAL is primarily mechanical and cavitation, along with some thermal effects, which provide skin retraction owing to ‘stimulation’ of the dermis of the treated areas.17,18 With this technique, there is a selective destruction of the connective tissue in between the fatty cells since UAL can target only tissue with low density and low molecular cohesion. Vessels, nerves, elastic fibres, and connective tissue fibres of the subcutaneous structures are preserved. This explains why UAL is accomplished with low blood loss, and the haematocrit drop after surgery is considerably reduced.11,12 Disadvantages involve an increase in surgical time (40% longer), the cost of the equipment, a steep learning curve, and the risk of thermal skin injury from unregulated heat. Also, the degree of skin contraction achieved by this method is insufficient for precise superficial contouring. 11
To counter this, we implemented RF as a method for achieving desired skin tightening. Embrace RF Body Tite system is a bipolar device used to deliver a regulated energy to skin and subcutaneous tissue, resulting in fat liquefaction, improved haemostasis, and skin tightening via skin contraction and collagen remodelling.
It was generally believed that patients should have good skin elasticity and a relatively low body fat percentage for optimal results after HDL. However, HDL using VASER and PAL has expanded eligibility up to patients with a BMI of 30. All patients in our study group had a BMI of 30 or less. The mean BMI was 26.2 (range: 23.1–30), which falls in the pre-obese to Obese I category according to the Indian standard classification. This was similar to studies by Hussain et al., Boeni et al. and Saad et al.19-21 The advent of these newer technologies has allowed these patients to achieve their desired look sooner than they otherwise would achieve with lifestyle changes and later surgery.14,22
All our patients underwent 360° Liposuction along with abdominal etching because this leads to better circumferential skin draping and allows for better overall shape and patient satisfaction.
We used a basket cannula for infiltration using a power-assisted method. This helps in the easier and even dissipation of fluid in tissue planes and also facilitates easier liposuction later. This concept of fluid infiltration is similar to the Expansion, Vibration and Lipofilling concept described for large volume lipofilling by Del Vecchio et al. 23 and improves on the concept of SAFE liposuction given by SH Wall Jr. 13
We carried out subdermal liposuction along the definition lines with fine 2 mm cannulas. In our technique, we apply gentle pressure by pressing the skin along the movement of the cannula below the linear marking of definition lines. This gives the surgeon control while also ensuring safety during finer sculpting. The usual method of pinching the skin and doing suction risks uneven liposuction, especially in the superficial plane. Also, the bent cannulas, which we used to sculpt the lateral aspect of tendinous inscriptions, help to avoid additional puncture incisions.
Potential risks and complications in HDL include postoperative swelling and bruising, temporary numbness or skin sensitivity, and the risk of over-sculpting, leading to unnatural results.10,24,25 In our study, most patients had no significant postoperative complications. There were two cases of seromas in two patients. Both these patients were conservatively managed with aspiration and compression dressing. Both were also advised to take a longer course of lymphatic massages. Most seromas can be managed conservatively on an OPD basis. 10 No major complications were noted in the study group.
The majority of the patients were satisfied or highly satisfied with the result achieved at 6 months. The satisfaction rates were similar to those of other studies conducted by Hussain, Boedi and Saad in recent times.19,21 However, patients should follow healthy lifestyle habits, including diet and exercise, to maintain the results for a long time, as with the results of any body-contouring procedure.
Conclusion
With the growing demand for male aesthetic procedures—particularly body sculpting—HDL utilising UAL, PAL, and RF-assisted skin tightening has proven to be a safe and effective technique. It consistently delivers natural-looking, reproducible results, with high patient satisfaction, minimal complications, and a relatively short, manageable recovery period.
This article introduces a surgical abdominal etching technique designed to guide plastic surgeons interested in adopting this procedure. While abdominal etching challenges certain traditional plastic surgery principles—such as performing liposuction in the superficial layer—our study demonstrates that HDL can be safely and effectively executed, yielding aesthetically desirable outcomes.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr Adarsh Keshari from APAR Health for medical writing assistance (CARE PROGRAMME).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.