
Abstract
Background:
Overfilled Face Syndrome (OFS) is an emerging aesthetic concern resulting from excessive or inappropriate use of dermal fillers. Despite growing recognition of its clinical and psychological consequences, no universally accepted classification or pathophysiological framework currently exists to guide the diagnosis or management of this condition.
Methods:
This narrative review synthesises current literature on anatomical, procedural and patient-related contributors to OFS. Expert insights, clinical observations and anatomical analysis were incorporated to develop a new classification system based on filler depth, anatomical layer involvement, and etiological mechanisms. The review was structured according to SANRA (Scale for the Assessment of Narrative Review Articles) guidelines to ensure scientific rigour and clarity.
Results:
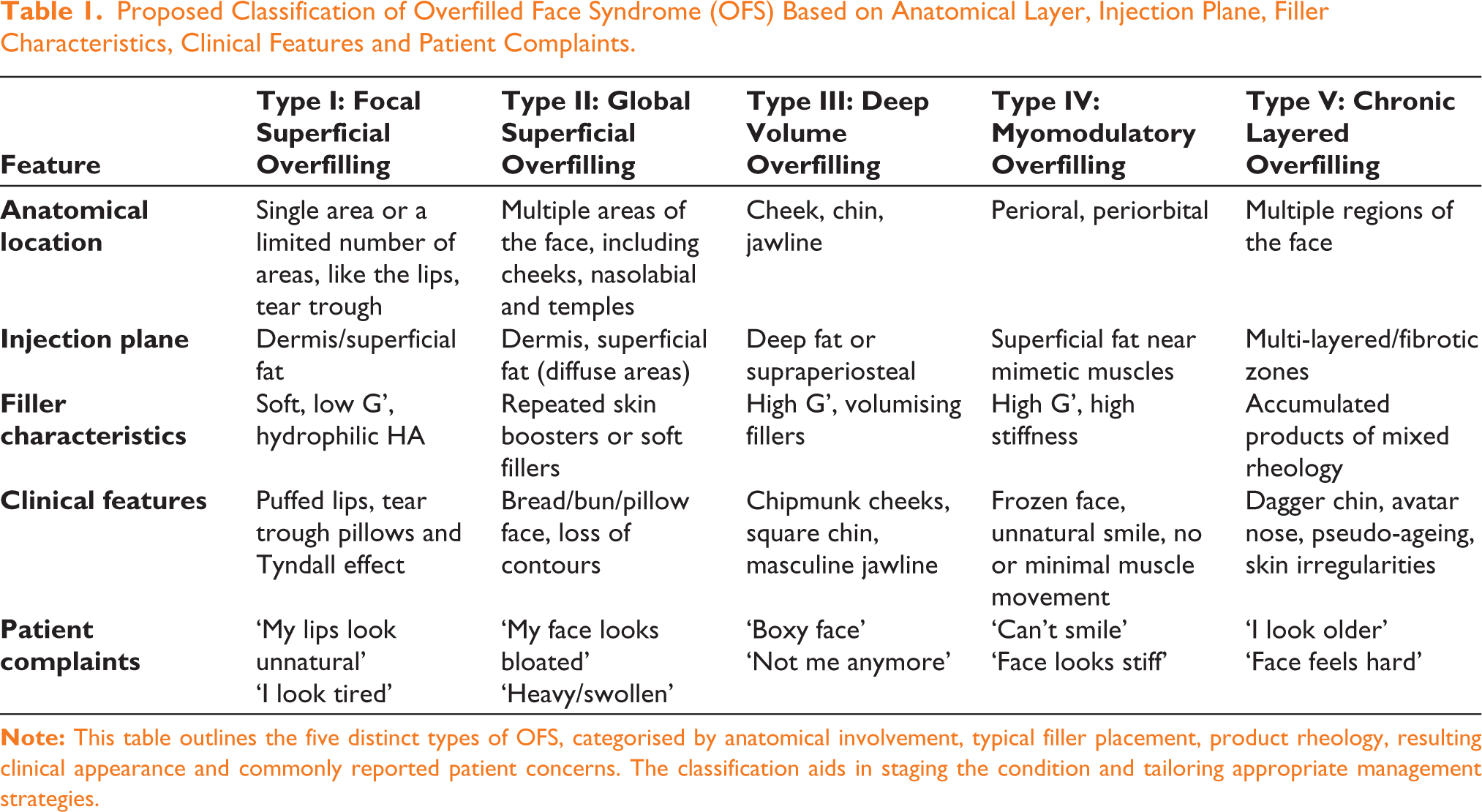
A five-type anatomical classification of OFS is proposed to support clinical recognition and staging. Type I represents focal superficial overfill; Type II involves global superficial overfill; Type III denotes deep volumetric overfill; Type IV describes myomodulatory overfill due to interference with mimetic muscles; and Type V includes chronic layered overfill associated with fibrosis and pseudo-ageing. This anatomy-based, aetiology-driven classification is likely to enhance the understanding of filler-induced facial distortions and support more targeted reversal and prevention strategies.
Conclusion:
A structured classification of OFS can provide a clinically relevant foundation for diagnosis and management. Recognising OFS as a spectrum disorder allows for a personalised, layer-specific and aetiology-informed corrective approach in aesthetic practice.
Keywords
Introduction
In recent years, the widespread use of hyaluronic acid (HA) fillers and other soft tissue injectables has revolutionised aesthetic facial rejuvenation. These minimally invasive treatments offer patients non-surgical options to restore volume, contour facial features and improve skin quality. 1 However, as the demand for fillers has surged globally, so too has the incidence of complications, both acute and delayed.2,3 Among these, a particularly under-recognised yet increasingly prevalent concern is Overfilled Face Syndrome (OFS).
OFS refers to a spectrum of aesthetic and functional disturbances that result from the excessive, misplaced, or repeated administration of dermal fillers. 4 Patients may present with loss of natural contours, impaired facial expressions, asymmetry, an aged look, and even psychological distress. While once regarded as an artistic error or simply the result of ‘too much filler’, emerging clinical evidence points toward a more complex interplay of anatomical, technical and patient-driven factors.5,6
Despite the growing recognition of OFS, the literature remains fragmented and lacks a standardised nomenclature or classification. Most current discussions rely on anecdotal experience or isolated case reports, and there is little consensus on how to define or categorise this syndrome. Furthermore, the absence of a unified framework hinders research, education and the delivery of consistent clinical care. While various terms have been informally used to describe the consequences of excessive filler use, including ‘Facial Overfilled Syndrome’, 7 there remains no universally accepted nomenclature or diagnostic criteria. In this article, the term OFS is introduced to offer greater anatomical specificity and intuitive clinical relevance. This terminology more precisely reflects the affected region and is consistent with established naming conventions in aesthetic medicine. By formalising OFS as a structured diagnostic entity, this article aims to provide a standardised language for clinical evaluation, communication and academic discourse.
This narrative review aims to bridge this gap by synthesising existing knowledge on the etiological mechanisms of OFS and proposing a novel anatomical classification system. By integrating filler rheology, depth of injection, facial layer involvement and clinical presentation, this article presents a structured approach that supports accurate diagnosis, staging and informed management strategies.
Methodology
This study follows the structure of a narrative review aimed at synthesising current understanding of OFS and proposing a clinically useful classification framework. The methodology aligns with the Scale for the Assessment of Narrative Review Articles (SANRA), a validated tool designed to ensure quality and rigour in narrative reviews.
A literature search was conducted across PubMed, Google Scholar, Scopus and Embase databases for publications that addressed one or more of the following: overfilling, overfilled face, facial overfill, facial overfilled syndrome, anatomical consequences of excessive filler, clinical presentations resembling overfilled face conditions, filler-induced facial distortion. Both peer-reviewed research articles and expert consensus commentaries were considered to ensure a comprehensive synthesis of scientific and clinical perspectives.
Excluded were studies focused exclusively on surgical complications, non-facial filler complications (e.g., hand or body), those involving non-soft tissue fillers (such as silicone or PMMA), and articles that lacked sufficient discussion on the anatomical or aesthetic outcomes of filler use.
In addition to literature synthesis, this review incorporates expert clinical insights derived from the author’s experience in aesthetic and reconstructive medicine, including high-volume injectable practice, anatomical dissections and management of filler complications. Observations from real-world case series, consensus discussions, and multidisciplinary training workshops also influenced the classification system.
The proposed classification framework was developed by analysing common patterns in anatomical distortion, filler behaviour across tissue planes, and patient-reported outcomes. Emphasis was placed on anatomical layer involvement, filler rheology and the mechanism of overfill (e.g., accumulation, myomodulation, fibrosis). The resulting five-type classification aims to be both descriptive and functional, supporting clinical staging and individualised treatment planning.
Image Generation and Ethical Considerations
To visually support the proposed classification framework, we created a set of illustrative images using publicly available generative AI tools from OpenAI. The baseline image was digitally synthesised to represent a 32-year-old Asian woman with no prior filler treatment. This reference image was then algorithmically modified to simulate the visual characteristics of each OFS subtype. These images do not represent real individuals and were generated solely for educational and illustrative purposes. No patient photographs were used, and no identifiable human subjects were involved, thereby exempting the study from ethical review or consent requirements. The use of AI-generated images aligns with current ethical guidelines for synthetic medical illustrations, thereby avoiding issues related to patient confidentiality and the misuse of real clinical photographs.
Results
To address the growing need for standardised terminology in diagnosing filler-induced distortions, this article proposes Kapoor’s Classification of OFS. Based on a comprehensive review of the literature, clinical experience, and anatomical analysis, this classification categorises patients into five types based on anatomical patterns and clinical severity. This classification will enable clinicians to stage the severity of OFS, understand its origin, and plan targeted reversal strategies.
To enhance understanding and standardisation, Table 1 provides a comprehensive summary of each classification type, outlining their anatomical location, injection plane, filler characteristics, clinical features and common patient complaints. In addition, a reference image of a 32-year-old Asian woman with no prior filler treatment was generated using OpenAI tools (Figure 1). This base image was subsequently modified to visually illustrate the defining features of each OFS type, providing a consistent and educational visual representation of the classification.
Proposed Classification of Overfilled Face Syndrome (OFS) Based on Anatomical Layer, Injection Plane, Filler Characteristics, Clinical Features and Patient Complaints.
Baseline Reference Image: Frontal View of a Digitally Generated Image of a 32-year-old Asian Woman with No Prior Filler Treatment. This Image, Created Using OpenAI tools, Serves as the Anatomical Reference for Subsequent Illustrations of ‘Overfilled Face Syndrome’ Types.

Type I: Focal superficial overfilling is characterised by excess filler localised to specific zones such as the lips, tear troughs, nasolabial folds, or marionette lines. Anatomically, it involves the dermis and/or superficial fat compartment (Figure 2). This form of OFS typically results from excessive or improperly placed superficial filler, often compounded by repeated touch-ups before the prior filler has fully degraded. Clinically, it presents as visible lumps, surface irregularities, or a bluish hue from the Tyndall effect, particularly in the tear trough. The lips may appear unnaturally voluminous (‘duck lips’), and the nasolabial region may appear overfilled. Patients often present with exaggerated contours, such as ‘duck lips’ or ‘pillow under eyes’, and report unnatural appearance in photographs.
Type I—Focal Superficial Overfilling: Illustration of OFS Type I, Showing Localised Overcorrection of Superficial Soft Tissues in Areas Such as the Lips and Tear Troughs. The Image Demonstrates Unnatural Lip Volume Resulting from the Overfilling of Superficial Hyaluronic Acid Fillers (AI-generated Image Using OpenAI Tools).

Type II: Global superficial overfilling affects the superficial fat layer across multiple facial zones, including the midface, lateral cheeks, jawline, temples and sometimes the forehead (Figure 3). It is commonly the result of frequent superficial injections using ‘skin boosters’ or hydrating fillers without adequate volumetric reassessment. This type is often seen in patients undergoing repeated fillers or ‘hydration’ protocols. Clinically, the face appears diffusely puffy or swollen, with loss of anatomical definition and a generalised oedematous look often described in Asian contexts as ‘bun face’. Overlying tissue appears tight, glossy and swollen—described by patients as ‘bloated’ or ‘bread-face’. Despite the fullness, youthful contours are lost. The facial skin may also show reduced elasticity and overexpansion in later stages.
Type II—Global Superficial Overfilling: Representation of Type II OFS, Characterised by Diffuse Puffiness of the Cheeks, Nasolabial Folds and Temples. The Face Appears Bloated and Heavy, Reflecting Repeated Superficial Filler Treatments (AI-generated Image Using OpenAI Tools).

Type III: Deep compartment overfilling involves excessive augmentation of deep facial fat pads (e.g., DMCF, SOOF, ROOF) and supraperiosteal regions such as the cheeks, chin, pyriform fossa, or jawline (Figure 4). This condition typically results from large bolus injections of high G′ fillers intended for structural enhancement, without considering their long-term persistence. Patients present with exaggerated midface or jawline projection, leading to a ‘ball face’ appearance. Clinical features include ‘chipmunk cheeks’, ‘square jawline’, and masculinised facial contours, often inconsistent with the patient’s baseline anatomy. There may be adjacent hollowing due to pressure on surrounding tissues. The distortion of normal contours disrupts natural light reflection, making the face appear overfilled and heavy at specific places.
Type III—Deep Volume Overfilling: Depiction of Type III OFS Showing Exaggerated Projection in the Cheeks, Chin and Jawline Due to Overfilling of Deep Anatomical Compartments. The Resulting Appearance Is Boxy and Masculinised (AI-generated Image Using OpenAI Tools).

Type IV: Myomodulatory overfilling targets the superficial fat layer overlying mimetic muscles, especially in the periorbital and perioral zones (Figure 5). In this form, fillers with high elasticity or large-volume fillers are placed over facial muscles, intentionally or inadvertently, to mimic the functional effects of neuromodulatory agents, such as those seen with botulinum toxin.:8–10 This leads to a characteristic ‘frozen face’ presentation where expressions appear blunted despite the absence of neuromodulators. Patients show reduced animation, a ‘frozen smile’, and struggle to express emotions. Patients may complain of restricted smiles, flat expressions, or a mask-like appearance.
Type IV—Myomodulatory Overfilling: Illustration of Type IV OFS Demonstrating Filler-induced Restriction of Mimetic Muscles, Especially in the Perioral and Periorbital Areas. Despite an Attempt to Smile, the Face Appears Frozen and Expressionless (AI-generated Image Using OpenAI Tools).

Type V: Chronic layered overfilling represents the most advanced and structurally complex form of OFS. It involves the dermis, as well as the superficial and deep fat compartments, often progressing to fibrotic changes due to long-term filler accumulation, product migration, and low-grade inflammation (Figure 6). These cases are often seen in patients with a history of layered treatments over many years without proper reassessment. Clinically, the face may develop firm, immobile areas with distorted contours and asymmetries that persist even after hyaluronidase use. Hollowing, tethering, or irregular texture may emerge after filler dissolution, revealing pre-existing fibrosis or volume loss. The result is an irregular, pseudo-aged appearance, characterised by features such as a ‘dagger chin’, ‘avatar nose’, dermal bumps and skin dullness. Patients frequently complain of looking older or ‘not like themselves’.
Type V—Chronic Layered Overfilling: Image Showing Advanced, Multi-layer Filler Accumulation with Fibrosis, Typical of Type V OFS. Notable Features Include a Dagger-shaped Chin, Widened Nasal Bridge (‘avatar nose’) and Facial Contour Irregularities (AI-generated Image Using OpenAI Tools).

This five-type classification captures the layered nature and evolving severity of OFS. It enables clinical staging, facilitates the identification of the pathophysiological mechanism of overfill, and could help in treatment decisions ranging from conservative management to staged reversal with hyaluronidase or surgical correction.
Discussion
OFS is now widely recognised because of the rising use and misuse of dermal fillers in aesthetic practice. It is no longer rare to encounter patients with facial distortion due to excessive volume, inappropriate product selection, poor injection technique, or repeated treatments without adequate reassessment.11,12 The aesthetic and psychological consequences of OFS are substantial, often leading to dissatisfaction, loss of self-image, and requests for corrective procedures. Despite its increasing frequency, there has been a lack of standardised nomenclature or classification to describe the condition. This article introduces a five-type classification system for OFS grounded in anatomical layers, injection depth, and underlying etiological mechanisms, which aims to provide a more structured approach to its diagnosis and management.
Each proposed type of OFS is defined by a combination of anatomical involvement 13 and clinical presentation. Type I, or focal superficial overfill, is typically caused by excessive filler in localised regions such as the lips or tear trough, often from repeated top-ups with soft or hydrophilic products. Type II, or global superficial overfill, occurs when skin boosters or soft fillers are overused in multiple superficial fat compartments, resulting in a uniformly swollen or ‘pillow face’ appearance with loss of natural contour. Type III represents deep volumetric overfill, where high G′ fillers are placed in deep fat or supraperiosteal planes, leading to exaggerated skeletal features such as ‘chipmunk cheeks’ or a square, masculinised jawline. Type IV, or myomodulatory overfill, involves filler placed near mimetic muscles—particularly around the mouth and eyes—that reduces natural movement and results in an expressionless or stiff face. Type V, chronic layered overfill, represents the culmination of years of over-treatment, filler accumulation 14 and layering across multiple planes and filler types, often with the development of fibrosis, nodularity and signs of pseudo-ageing and features of chronic overfilling such as a dagger-like chin or widened nasal bridge.
Although these types can exist independently, clinical overlap is common, and understanding the differences between similar presentations is critical. Types II and III may both involve the midface but differ in depth and texture—Type II is characterised by superficial puffiness with soft, doughy skin, while Type III presents as sharply contoured and rigid due to deep structural augmentation. In contrast, Types II and IV can appear similar in facial volume, but the key distinction lies in facial expression. Patients with Type II retain dynamic function to some extent, whereas Type IV individuals appear frozen due to the interference of fillers with muscle motion. Differentiating Type II from Type V is equally important. While both may involve generalised volume, Type V patients often have irregular contours, visible lumps and harder tissue due to fibrosis and product accumulation. Likewise, although both Types III and V involve deep filler placement, Type V exhibits architectural distortion and chronic changes that are not typically seen in Type III. Finally, Types IV and V may both appear expressionless, but Type IV results from direct muscle interference, whereas Type V stiffness is often due to fibrosis and layered scarring.
This classification has practical clinical implications. By recognising the type of OFS, practitioners can tailor treatment strategies to the underlying mechanism. For example, early intervention with hyaluronidase may be effective in Types I and II, while more complex, layered reversal strategies may be needed for Type V. Similarly, understanding that Type IV involves muscle movement alteration can prevent unnecessary dissolving or surgical correction. From a preventive perspective, the classification emphasises the importance of respecting anatomical boundaries, avoiding frequent reinjections without reassessment, and selecting appropriate filler types for each facial layer. It also highlights the role of patient education and the need to temper expectations regarding long-term volume maintenance.
While the proposed five-type classification of OFS provides a structured framework for diagnosis and staging, it is important to recognise that these categories are not rigid or mutually exclusive. OFS often exists as a continuum, where patients may evolve from one type to another over time due to cumulative filler exposure, anatomical changes and fibrotic remodelling. For instance, Type I (focal superficial overfill) may progress to Type II (global superficial overfill) with repeated skin booster or filler treatments, or eventually transition into Type V (chronic layered overfill) in the presence of multiple filler layers, poor degradation, or tissue scarring. Similarly, Types II and III may co-exist in patients who receive both superficial and deep volumising injections without adequate contour evaluation.
This overlapping nature underscores the need for longitudinal assessment and layer-specific mapping during both filler planning and reversal. A spectrum-based view of OFS helps clinicians better understand the complexity of overfilling and guides more nuanced, patient-specific management strategies. Understanding these distinctions supports not only accurate diagnosis but also patient counselling and shared decision-making.
Limitations
This narrative review is based on existing literature, clinical experience, and expert observations rather than prospective cohort data or systematic meta-analysis. The spectrum nature of OFS may result in overlap between categories, which could introduce subjectivity in classification, particularly in mixed-type presentations. The use of AI-generated visual references—while helpful for illustrative purposes—may not fully capture the diversity of facial morphology across populations. Furthermore, although the images were digitally generated to simulate anatomical changes associated with OFS, they do not replace the need for photographic validation from real clinical cases. Ethical considerations in the use of AI imagery were addressed by ensuring that no real patient data or likenesses were used.
Conclusions
OFS is an increasingly recognised complication of aesthetic filler treatments. This review proposes a five-type classification framework grounded in anatomical depth, filler characteristics and etiological mechanisms. By conceptualising OFS as a layered and spectrum-based disorder, the classification aids clinicians in diagnosis, communication and treatment planning. It emphasises the importance of individualised assessment and reinforces the need for judicious filler use. Future validation through clinical studies and integration of objective imaging will help refine this framework and enhance patient safety.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The author received no financial support for the research, authorship and/or publication of this article.