
Abstract
Background:
Overfilled face syndrome (OFS) is a growing iatrogenic complication of dermal filler use, characterised by unnatural and disharmonious facial appearances. While an anatomical classification of OFS has recently been published, its aetiology extends beyond anatomy alone. This review synthesises the broader drivers of overfilling across three domains: the practitioner, the patient and the product.
Methods:
A narrative review was conducted in accordance with SANRA (Scale for the Assessment of Narrative Review Articles) guidelines. A targeted literature search was conducted using PubMed, Scopus and Web of Science (2018–2025). Aetiological contributors were organised into practitioner-, patient- and product-related factors and contextualised within the framework of the five-type classification of OFS.
Results:
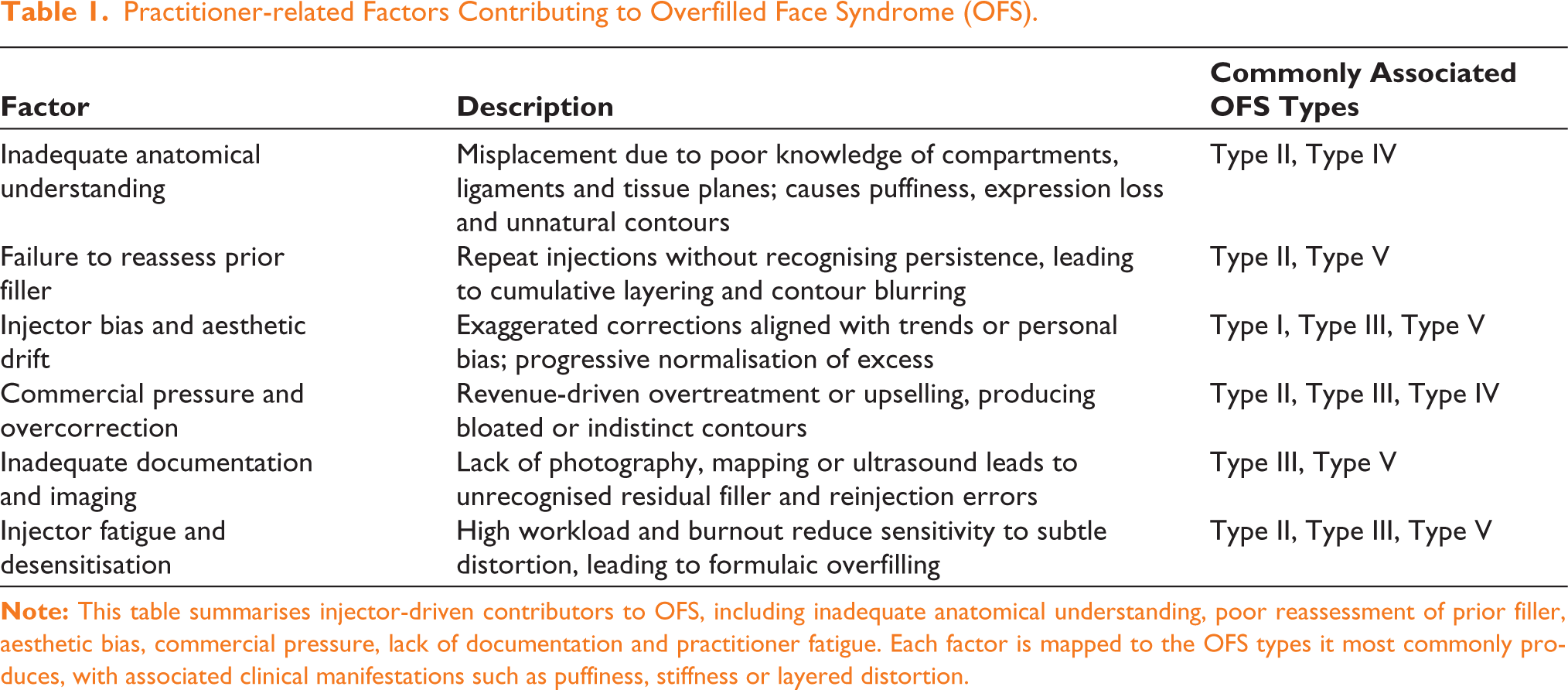
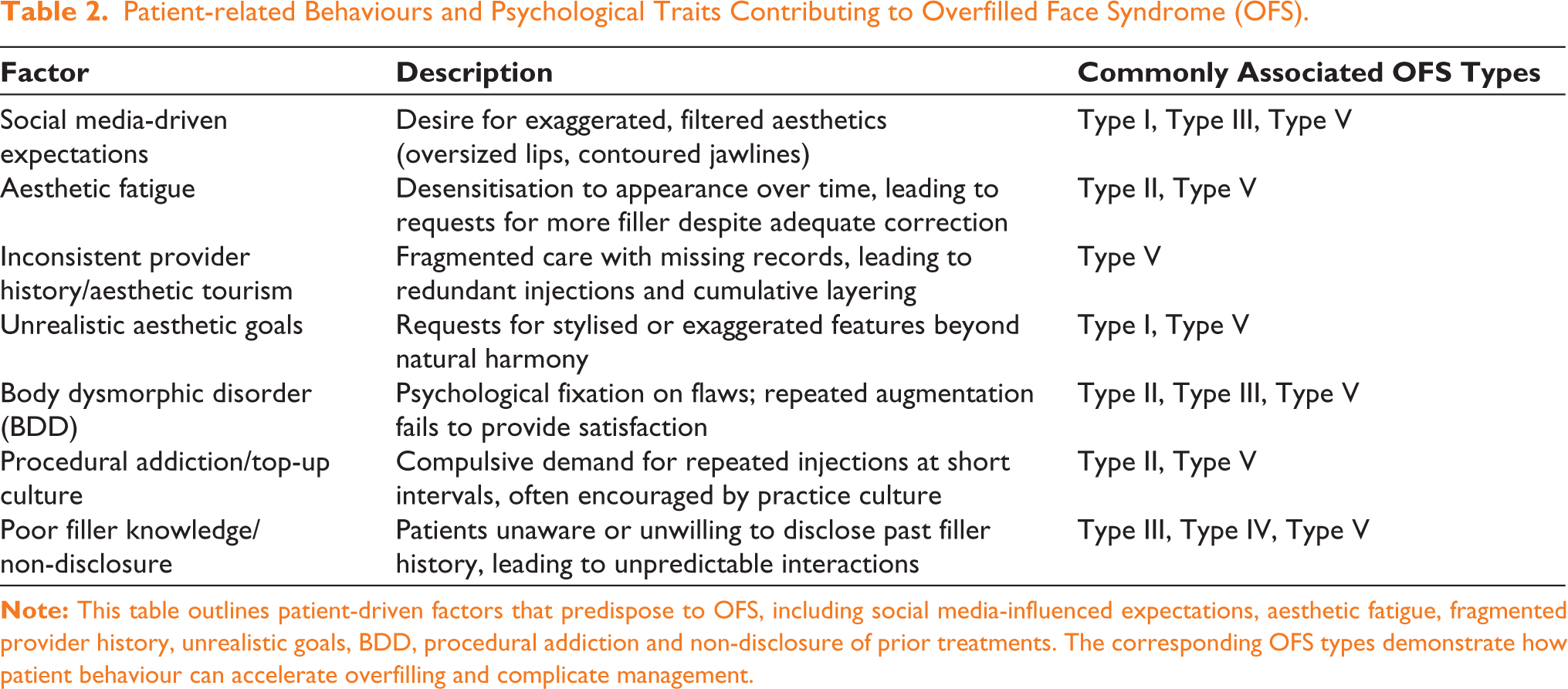
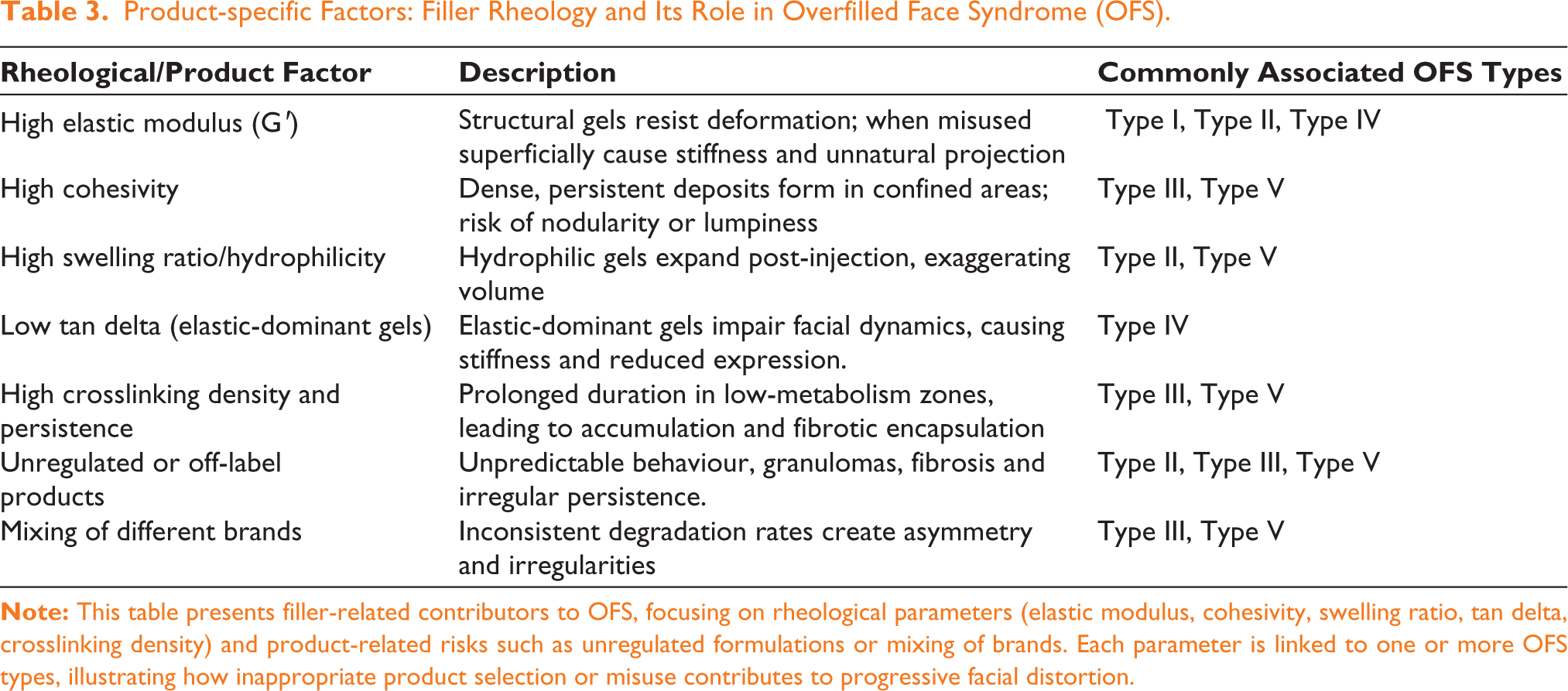
Practitioner-related contributors include inadequate anatomical understanding, repeated injections without reassessment, injector bias, commercial pressures, lack of documentation or imaging, and injector fatigue. Patient-related drivers span social media-influenced ideals, aesthetic fatigue, fragmented treatment histories, unrealistic goals, undiagnosed body dysmorphic disorder, procedural addiction, and poor filler literacy or disclosure. Product-related risks arise from rheological mismatches, such as high elastic modulus or cohesivity, higher hydrophilicity and swelling factor, low tan delta with elastic-dominant gels, high crosslinking density and long persistence, as well as from unregulated products and brand mixing. These factors rarely act in isolation; instead, they intersect and amplify one another, creating cumulative and progressive overfilling patterns that evolve across OFS types.
Conclusion:
OFS should be understood as a multifactorial spectrum condition shaped by the interplay of practitioner, patient and product factors, rather than being solely attributed to excessive filler volume. Integrating these aetiological domains with the established anatomical classification provides a more holistic framework for prevention and management. Ethical restraint, anatomically precise injection, rheology-informed product selection and longitudinal documentation are critical to safeguarding natural facial identity in contemporary aesthetic practice.
Keywords
Introduction
The widespread adoption of hyaluronic acid (HA) fillers has transformed the field of aesthetic medicine, offering minimally invasive, customisable and reproducible facial rejuvenation options. 1 Yet, with growing demand and the proliferation of undertrained injectors, a new iatrogenic complication has emerged: overfilled face syndrome (OFS). Clinically, OFS is marked by unnatural, disharmonious appearances resulting from excessive, misplaced or cumulatively layered filler injections, often leading to aesthetic dissatisfaction and, in some cases, functional impairment.
Although early writings made reference to concepts such as ‘filler fatigue’ or ‘facial overfilled syndrome’, 2 a structured diagnostic framework was only recently established with the publication of the five-type anatomical classification of OFS. 3 This classification stratifies presentations based on filler depth, anatomical plane and clinical phenotype, providing a systematic way to diagnose and communicate the spectrum of overfilling (Figure 1).
Clinical Spectrum of Overfilled Face Syndrome (OFS), Types 0–V. (A) Type 0—baseline, natural harmony. (B) Type I—single feature exaggeration. (C) Type II—diffuse puffiness. (D) Type III—deep compartment overfilling. (E) Type IV—stiffness and restricted expression. (F) Type V—multi-planar, global distortion.

However, anatomy alone does not explain why OFS occurs. 4 Clinical practice and emerging literature suggest that its aetiology is broader, arising from the dynamic interplay of practitioner-, patient- and product-related factors. 5 Practitioners contribute through anatomical knowledge gaps, repeated injections without reassessment, aesthetic bias and commercial pressures. Patients drive overfilling through unrealistic expectations, social media-influenced ideals, fragmented treatment histories, psychological vulnerabilities and procedural addiction. Products themselves can amplify risk through rheological mismatches, persistence, swelling potential and the use of poorly regulated or mixed filler brands.
These domains rarely act in isolation. Instead, they intersect and reinforce one another, leading to progressive and sometimes irreversible distortion that evolves across OFS types. 3 By expanding the conversation beyond anatomical misplacement to include the roles of practitioner behaviour, patient psychology and product science, this review aims to provide a comprehensive understanding of OFS aetiology. Such an integrated perspective is essential for developing safer, evidence-informed and ethically grounded practices that preserve natural facial identity in the era of widespread injectables.
Methodology
This review was designed as a narrative review in accordance with the SANRA (Scale for the Assessment of Narrative Review Articles) guidelines, which emphasise clarity of scope, appropriate referencing, justified conclusions and transparent reporting of methodology. The aim was to synthesise existing knowledge on the aetiology of OFS and to place it within the broader ecosystem of practitioner-, patient- and product-related factors.
A targeted literature search was conducted across PubMed, Scopus and Web of Science to identify relevant studies published between January 2018 and September 2025. The search strategy combined free-text terms such as ‘overfilled face syndrome’, ‘facial overfilling’, ‘filler fatigue’, ‘excessive dermal fillers’, ‘filler complications’, ‘facial distortion’, ‘body dysmorphia’, ‘hyaluronic acid’ and ‘filler rheology’, together with MeSH terms including ‘Dermal Fillers’, ‘Hyaluronic Acid’, and ‘Adverse Effects’. Only articles written in English and judged to have clinical relevance to OFS or to the consequences of excessive dermal filler use were considered. Publications focusing exclusively on surgical interventions, animal experiments or non-English sources were excluded.
The initial search yielded 1,104 records. Of these, only eight peer-reviewed publications directly addressed ‘overfilling’ as a defined condition. Due to the limited number of directly relevant sources, supplementary literature was incorporated where it provided indirect but clinically meaningful insights, particularly on filler rheology, long-term product persistence, patient psychology and complications associated with injectables. The selected material was then synthesised into a tripartite framework focusing on practitioner-, patient- and product-related contributors to overfilling. These aetiological domains were subsequently integrated with the published five-type anatomical classification of OFS, providing both a structural and clinical context for the analysis.
Discussion
OFS has emerged as one of the most recognisable iatrogenic outcomes of contemporary aesthetic practice. While the recently published five-type anatomical classification provides a valuable framework for diagnosis, classification alone does not explain why overfilling occurs. 3 The aetiology of OFS is more complex and arises from the interplay of factors related to the practitioner, the patient and the product. Each of these domains contributes independently, yet their influence is most profound when they converge and reinforce one another. 6 Understanding this triad is crucial for clinicians seeking to prevent, recognise and ethically manage the spectrum of OFS.
Practitioner-related Factors
Inadequate Anatomical Understanding
Among the most widely acknowledged contributors to OFS is insufficient anatomical literacy among injectors (Table 1). 7 The face is a layered construct of skin, superficial and deep fat compartments, retaining ligaments, dynamic muscular planes and neurovascular bundles.8,9 Yet many injectors rely only on surface landmarks, leading to misplaced filler. Superficial placement when deeper volumisation is required can cause localised puffiness, or the ‘bread face’ appearance of Type II OFS, where filler blunts natural transitions. Failure to respect superficial fat compartment boundaries predisposes to pooling and migration, further distorting harmony. 4 Such misplacement may also alter mobility when filler is inadvertently placed over active muscles, producing unintended myomodulatory effects and stiffness akin to Type IV OFS. Complication reports consistently suggest that poor anatomical knowledge correlates strongly with aesthetic error, making this the foundation for progression towards OFS.
Practitioner-related Factors Contributing to Overfilled Face Syndrome (OFS).
Failure to Reassess Prior Filler
A second driver of OFS is inadequate reassessment of existing filler before reinjection. HA products are often assumed to degrade within 6–12 months; however, magnetic resonance imaging (MRI) and ultrasound studies repeatedly demonstrate their persistence for years. 10 In practice, fading correction is equated with resorption, leading injectors to add more product to areas still containing filler. 11 Without baseline photography or imaging, these remnants remain undetected. 12 Over time, repeated ‘top-ups’ cause cumulative layering: superficially, this creates Type II puffiness, while deeper persistence manifests as Type V nodularity or irregular contour. Patients often acclimate to gradual changes and fail to notice distortion until it is advanced, while injectors misinterpret dissatisfaction as undercorrection. This cycle emphasises the importance of longitudinal assessment with photographic audits or ultrasound mapping before reinjection. 13
Injector Bias and Aesthetic Drift
Practitioners’ aesthetic biases also shape the development of OFS. Aesthetic drift occurs when an injector’s perception of beauty shifts towards exaggerated or stylised ideals, influenced by prevailing social media trends such as sharply angular jawlines or highly projected lips. 14 Treatments then overshoot the natural balance, producing disharmony even in well-proportioned faces. This drift frequently aligns with Type I OFS, where a single feature is over-augmented; Type III OFS, where deep compartments are overfilled; or Type V, where distortion spreads across multiple planes. Cultural and regional preferences can reinforce this drift, as practitioners cater to demand and normalise excess. Over time, both injector and patient adapt to progressively exaggerated outcomes, blurring the line between enhancement and caricature. 15 Peer review, continuing education and reliance on proportional, evidence-based standards are necessary safeguards against this subtle yet powerful influence.16,17
Commercial Pressure and Overcorrection
The commercial framework of aesthetic practice exerts another strong influence on overfilling. Clinics often operate within revenue-driven models, incentivising upselling, bundled packages or frequent touch-ups. 15 While financially advantageous, such models risk overshadowing clinical restraint, especially in inexperienced injectors who equate more volume with better results. Patients with balanced features may thus be persuaded into additional augmentation, producing distortion rather than refinement. Such overtreatment typically manifests as Type II diffuse swelling, Type III deep accumulations or Type IV myomodulatory overfill. The ethical implications are significant: when business priorities outweigh clinical prudence, iatrogenic harm escalates. 18 Some authors recommend structured consultation protocols that emphasise proportion, informed consent and precise documentation of conservative treatment plans. Such frameworks allow practitioners to counterbalance financial pressures with ethical responsibility.
Inadequate Documentation and Imaging
Longitudinal safety in filler practice depends on robust documentation and imaging,19,20 yet both are frequently neglected. Many clinics lack standardised photography, injection maps or volumetric records, leaving practitioners reliant on memory or patient recall. This approach is unreliable given the persistence and cumulative effects of fillers. Imaging studies consistently show residual HA deposits in areas previously thought to be resorbed, highlighting the limitations of visual assessment. 11 Without records or ultrasound, reinjections risk targeting already corrected zones, accelerating progression to Type III or Type V OFS. Beyond prevention, imaging and documentation are also crucial once distortion arises, guiding reversal or hyaluronidase use. 13 From a medico-legal standpoint, thorough records protect practitioners in disputes. Thus, neglecting these tools undermines both safety and accountability, directly contributing to the burden of OFS.
Injector Fatigue and Desensitisation
Finally, practitioner fatigue and desensitisation represent underrecognised contributors.21,22 High-volume practice, repetitive procedures and long hours can dull sensitivity to subtle overfilling. Burnout fosters formulaic approaches and recalibrates perception, making exaggerated corrections appear normal. This phenomenon mirrors patterns in other medical fields where fatigue increases error rates. In aesthetics, the incremental nature of filler treatments compounds this risk: small, unnoticed excesses accumulate until the patient presents with Type II, III or V OFS. Fatigue also intersects with commercial pressures, where speed and throughput are rewarded over reflection. Addressing this requires systemic interventions, including workload management, reflective practice and continuing education to restore critical judgement.23,24 Recognising fatigue not as an occupational nuisance but as a risk factor reframes it as a genuine contributor to OFS.
Patient-related Factors
Social Media-driven Expectations
The influence of social media has reshaped beauty ideals and is a major driver of OFS (Table 2). Platforms such as Instagram and TikTok promote filtered or enhanced features— oversized lips, sharp jawlines or elevated brows—as normal, creating unrealistic standards that patients expect to be replicated.25,26 The demand for exaggerated corrections frequently produces Type I OFS, where single features dominate facial balance. Younger patients are especially vulnerable, as algorithm-driven feeds normalise homogenised aesthetics. 27 Practitioners may reinforce this cycle, either to satisfy requests or due to shared exposure, leading to progressive distortion that evolves into more severe or global forms, such as OFS Type III or Type V, if unchecked.
Patient-related Behaviours and Psychological Traits Contributing to Overfilled Face Syndrome (OFS).
Aesthetic Fatigue
Patients often become desensitised to their improved appearance, a phenomenon described as aesthetic fatigue. 28 Over time, post-treatment results are perceived as baseline, and the return of natural features is misinterpreted as regression. This prompts repeated ‘top-ups’ in already treated zones, resulting in cumulative layering. 29 The outcome is typically Type II OFS, with diffuse puffiness and contour blunting, particularly in the midface and periorbital areas. Similar to tolerance in addiction, escalating volumes are needed to meet shifting expectations, locking both patient and injector into a cycle of reinforcement until obvious distortion like Type V OFS emerges. 30
Inconsistent Provider History and Aesthetic Tourism
Fragmented care and aesthetic tourism can further predispose patients to complications. 31 Patients often move between providers or clinics abroad, with poor continuity and limited record-keeping of product type, volume or plane of injection.32,33 Subsequent practitioners, unaware of residual filler, may unknowingly reinject into saturated areas. This results in progressive layering, particularly in deep compartments, culminating in Type V OFS, characterised by chronic, multi-planar distortion. Such cases are not only aesthetically challenging but also complex to reverse when product identity is unknown, complicating hyaluronidase use and overfilling management.
Unrealistic Aesthetic Goals
Many patients pursue stylised ideals—‘snatched’ jawlines, ‘foxy’ eyes or hyper-voluminous lips—driven by transient trends rather than harmony. 34 These requests pressure practitioners into exceeding natural proportions. 35 Conservative correction is often rejected as inadequate, prompting either compliance or doctor-hopping until demands are met. 15 This pattern produces Type I OFS, where one feature is exaggerated, and contributes to Type V when multiple areas are altered over time. Literature emphasises the practitioner’s ethical duty to decline unrealistic requests, using structured consultations to realign goals with achievable, natural outcomes.
Undiagnosed Body Dysmorphic Disorder (BDD)
BDD is a critical but underrecognised driver of OFS. Patients with BDD are preoccupied with minor or imagined flaws and seek repeated interventions, though no amount of treatment relieves their distress. 36 In practice, BDD often leads to excessive augmentation in already corrected regions, producing Type II puffiness or Type III deep accumulations. Advanced cases evolve into Type V OFS, with global disproportion. Patients with BDD are often dissatisfied despite extensive correction and may pose legal or reputational risks. 37 Screening with validated tools and referral pathways is essential to prevent such outcomes.36,38
Procedural Addiction and Top-up Culture
Distinct from BDD, procedural addiction—or ‘top-up culture’—is characterised by compulsive requests for frequent injections, reinforced by the psychological gratification of undergoing procedures. 39 This behaviour is sometimes enabled by practitioners offering short-interval ‘maintenance’ schedules, encouraging the idea that frequent touch-ups are necessary. Over time, cumulative layering in superficial planes results in Type II OFS, with diffuse swelling. If generalised across regions, Type V OFS ensues. Conceptually similar to substance dependence, procedural addiction thrives in the absence of standardised protocols, highlighting the need for clinical restraint and patient education.40,41
Poor Filler Knowledge or Non-disclosure
Patient non-disclosure and poor literacy further contribute to OFS. Many are unaware of the type, volume or anatomical placement of past fillers, especially when treated by multiple providers. 33 Others underestimate persistence, assuming fillers are temporary. 10 Without accurate disclosure, practitioners may unknowingly mix brands or inject into areas with residual product, resulting in irregular degradation, migration or clumping. These patterns typically manifest as Type III deep overfilling, Type IV myomodulatory overfilling or Type V chronic distortion. Improved patient education, combined with standardised documentation systems, is crucial in addressing this silent yet potent risk factor.
Product-related Factors
High Elastic Modulus (G')
Fillers with a high elastic modulus (G′) resist deformation and provide structural support in areas such as the chin or jawline (Table 3). 42 However, when used superficially or in dynamic regions, they produce visible stiffness, exaggerated contours and palpable firmness. Such misuse often results in Type I OFS, where a feature is disproportionately augmented, or Type II, where transitions blur into puffiness. Because high G′ gels resist compression, they may also diminish facial expressivity, overlapping with Type IV OFS. These outcomes highlight the need for rheology-aware product selection and precise placement. 43
Product-specific Factors: Filler Rheology and Its Role in Overfilled Face Syndrome (OFS).
High Cohesivity
Cohesivity determines whether a filler disperses or stays in one mass.43,44 Highly cohesive gels are effective for deep projection but problematic in confined areas if injected in excess. Misplaced or repeatedly layered cohesive fillers tend to form dense deposits, particularly in well-defined deep fat compartments. Clinically, this produces Type III OFS. Their resistance to enzymatic breakdown prolongs the problem, and repeated injections across multiple regions may culminate in Type V, with widespread contour disruption.
High Swelling Ratio/Hydrophilicity
Hydrophilic fillers attract water and swell post-injection.43,45,46 While this can enhance correction in deflated areas, it often exaggerates volume beyond what was injected. When swelling subsides, patients and practitioners may perceive ‘filler loss’, prompting reinjections and cumulative overfilling. This cycle drives Type II OFS, especially in the midface and periorbital regions, and contributes to the classic ‘pillow face’. In chronic cases, diffuse puffiness may evolve towards Type V. Awareness of a filler’s swelling profile is critical to avoiding this reinforcement loop.
Low Tan Delta (Elastic-dominant Gels)
Tan delta expresses the ratio of viscous to elastic properties in a filler. 47 A low tan delta indicates an elastic-dominant gel that resists deformation but adapts poorly to movement. 48 When used in expressive zones like the lips or perioral area, these fillers can cause unintended myomodulation, restricting animation and leading to Type IV OFS, where stiffness dominates. While low tan delta gels are valuable for structural correction, their misuse in mobile areas compromises both aesthetics and social expressivity.
High Crosslinking Density and Persistence
Crosslinking prolongs filler duration; however, highly crosslinked products often persist for years,49,50 particularly in low-metabolism zones, such as the infraorbital hollow or temple. Reinjections into such areas can result in cumulative buildup, producing Type III deep overfilling or Type V multi-planar distortion. Persistent products may also encapsulate, complicating reversal with hyaluronidase. Longevity, marketed as a benefit, becomes a liability when not matched to the treatment site.
Unregulated or Off-label Products
The global filler market encompasses numerous unregulated or off-label products that lack reliable rheological data or predictable degradation.51,52 In vivo, they may swell, migrate or persist unpredictably, increasing risks of granuloma, fibrosis or chronic inflammation. Clinically, these cases resemble Type II, Type III or Type V OFS. The problem is amplified in patients undergoing aesthetic tourism, where the identity of the injected product is often unknown, hindering safe management or reversal. 32
Mixing Different Brands
Different filler brands vary in rheology and degradation kinetics.53,54 When mixed in the same zone, they may behave inconsistently: one product dissipating while another persists, creating asymmetry, irregularities or migration. Such outcomes typically present as Type III or Type V OFS, where disharmony stems from incompatible product behaviour. Case reports increasingly highlight the risks of reinjecting without knowledge of prior filler type, underscoring the importance of documentation and disclosure.
Interplay of Factors and OFS Progression
OFS rarely results from a single factor; it emerges from the interaction between practitioner behaviour, patient expectations and filler properties. 3 These domains amplify one another—patient demand encourages overtreatment, practitioner bias or fatigue normalises excess, and product persistence ensures that distortion accumulates. OFS is thus not an abrupt complication, but a progressive syndrome that evolves over years of repeated treatments.14,55
In early stages, Type I and Type II OFS often develop when social media-driven requests intersect with injector bias or commercial pressure and the misuse of structural gels. For example, exaggerated lips treated with a high G′ filler superficially, followed by top-ups with hydrophilic gels, may lead to diffuse puffiness. Type III arises when fragmented care or poor disclosure allows cohesive or crosslinked fillers to build up unnoticed in deep planes. Type IV develops when elastic-dominant gels blunt expression in mobile zones. Ultimately, Type V OFS represents the convergence of all three domains—doctor-hopping patients, practitioners under commercial or social pressures and long-lasting fillers compounding across sessions.
Viewed this way, OFS is a spectrum disorder shaped by cumulative interactions rather than an isolated misstep. 2 Recognising this interplay reframes OFS as the predictable outcome of systemic vulnerabilities in aesthetic practice, emphasising the need for prevention strategies that extend beyond technique to include patient education, psychological screening, product science and longitudinal monitoring
Prevention and Clinical Implications
Ethical Restraint and Consultation
The most powerful preventive tool lies in ethics. Practitioners must resist pressures that normalise overcorrection. 56 Structured consultations should emphasise proportion over volume, reframing success as harmony rather than exaggeration. Using the OFS classification in consultations can help patients understand how overfilling progresses across Type I through Type V. Ethical restraint is thus not about saying ‘no’, but about reframing treatment goals and objectives. 18
Anatomical Precision and Reassessment
Technical skill remains central. Anatomical precision and awareness of layers, compartments and ligaments reduce misplacement, while reassessment prevents cumulative layering. 57 Imaging studies confirm fillers often persist for years despite apparent fading. 11 Periodic ultrasound and photographic documentation provide baselines, minimising unrecognised buildup. 58 Reassessment intervals based on actual need, rather than routine ‘maintenance’, align treatment with safety.
Rheology-informed Product Selection
Product choice must match anatomy. Parameters such as G′, cohesivity, tan delta, swelling ratio and crosslinking density directly influence filler behaviour.59,60 Misalignments—such as structural gels used superficially or highly crosslinked gels in low-metabolism zones—predispose to OFS. Prevention requires plane-specific selection and transparency in rheology data. Training should emphasise filler science alongside technique.
Patient Screening and Psychological Assessment
Psychological contributors must not be overlooked. Unrealistic goals, procedural addiction, and BDD increase risk. Routine screening and careful history-taking can identify high-risk patients, while referral to mental health professionals should be normalised.61,62 Educating patients about filler persistence and cumulative risks is essential, correcting the misconception that fillers are harmless and short-lived.
Longitudinal Documentation and Collaborative Care
Preventing OFS requires system-level change. Standardised treatment records, photography and imaging preserve continuity of care and prevent inadvertent layering, especially in patients seeking care across providers or abroad. Professional societies could establish minimum standards for record-keeping, while collaboration between specialities ensures both technical and psychological risks are addressed. 63
Preventing OFS requires more than technical correction; it calls for a cultural shift in aesthetic medicine. Practitioners must balance demand with restraint, align products with anatomy and adopt longitudinal monitoring. Patients must be educated to value natural outcomes. By integrating ethics, anatomical precision, product science, psychological screening and robust documentation, the field can reduce OFS and preserve the principle that beauty is enhancement, not distortion.
Limitations
This review has inherent constraints. As a narrative rather than a systematic review, it is susceptible to selection bias and cannot claim comprehensive coverage of all relevant literature. Evidence specific to OFS is limited, with most insights derived from expert opinion, small imaging studies or case reports, restricting generalisability. Psychological contributors such as BDD and procedural addiction remain underrecognised in aesthetic practice, likely leading to underestimation of their true impact. In discussing rheology and product persistence, much of the analysis is extrapolated from laboratory or preclinical data rather than large prospective trials. Integration of Kapoor’s OFS classification into the aetiological discussion is interpretive and requires further validation. Finally, the filler industry continues to evolve rapidly, with the introduction of new products, advancements in crosslinking technologies and global regulatory variations, meaning conclusions must be revisited as higher-level evidence and long-term clinical data become available.
Conclusions
OFS is best understood as a progressive, multifactorial condition resulting from the interplay of practitioner, patient and product factors. Distortion arises not from isolated errors but from cumulative dynamics: anatomical misjudgement, commercial or aesthetic bias, unrealistic expectations, psychological vulnerabilities and rheological mismatches. The five-type OFS classification provides a framework to contextualise these mechanisms. Preventing OFS requires more than technical skill; it demands ethical restraint, patient education, psychological screening, longitudinal reassessment, rheology-informed filler choice and systematic documentation. Equally important is a cultural shift that prioritises proportion and harmony over exaggerated correction, reframing fillers as tools for subtle enhancement rather than unlimited augmentation. Future research should validate classification systems, clarify long-term persistence through imaging and establish standardised screening protocols. By embedding evidence, ethics and interdisciplinary collaboration, aesthetic medicine can reduce OFS incidence and preserve both facial integrity and patient trust.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Statement
This article is a narrative review and does not involve human participants, animals or patient data. All illustrative images are AI-generated and not derived from real individuals. Ethical approval and patient consent were therefore not required.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.