
Abstract
Body contouring has evolved with technological advancements, improving fat removal and skin tightening. Traditional methods like suction-assisted liposuction (SAL) have limitations, leading to innovations such as powerassisted liposuction (PAL), ultrasound-assisted liposuction (UAL) and radio frequency (RF)-enhanced contouring. This study evaluates the efficacy of PURE Contouring, a novel approach integrating these three techniques. A retrospective analysis was conducted on 1,968 patients who underwent PURE Contouring from September 2021 to December 2024. Procedures involved tumescent infiltration, PAL for efficient fat removal, UAL for targeted fat breakdown and RF for enhanced skin tightening. Patient demographics, procedure details and satisfaction levels were assessed over three to six months, with statistical analysis applied to identify influencing factors. The majority of patients were female (53.20%), and 360-degree liposuction was the most commonly performed procedure (38.61%). The majority of patients fall within the 35-45 years age group (36.03%). No major complications were reported. Satisfaction was measured using a 5-point Likert scale. Overall, 91.51% of patients reported being highly satisfied with their outcomes. This strong positive response suggests that most patients not only achieved their desired aesthetic outcomes but also had a smooth surgical and recovery experience. PURE Contouring effectively enhances body contouring outcomes, offering superior fat removal and skin tightening. High satisfaction rates support its efficacy, highlighting its potential as a preferred technique in aesthetic surgery.
Keywords
Introduction
Body contouring is a surgical procedure that removes excess subcutaneous fat and skin with or without an open surgical method to alter the structure, position or texture of various body parts. 1 It has emerged as one of the most transformative advancements in aesthetic surgery. With technological advancements and an increasing understanding of human anatomy, body contouring has become a preferred choice for individuals seeking to target excess fat, sagging skin and other imperfections that may not be addressed by diet and exercise alone to enhance their appearance and achieve their desired body image. The ultimate goal is to create a harmonious and proportionate silhouette tailored to the individual’s unique aesthetic goals.
The birth of liposuction was a suction technique using a vacuum pump. It involves inserting a cannula connected to a vacuum-assisted aspirator through a stab incision in the natural skin crease and tunnelling through the subcutaneous fat to break it up. 1 This technique came to be known as suction-assisted liposuction (SAL). However, the disadvantage of this technique is surgeon fatigue when larger areas of liposuction are required, thus leading to suboptimal results.
An American surgeon named Charles Gross first introduced power-assisted liposuction (PAL). 2 The cannula tip exhibits a jackhammer-like movement, which aids in breaking up fat and allowing it to be aspirated into the cannula openings, where it is subsequently vacuumed by reciprocating motion. PAL offers the advantages of being superior in fat removal in larger areas, convenient, presenting the most favourable cost–benefit ratio and appearing to be the best option for busy liposuction practices, with less fatigue for the surgeon and least traumatic. 3
The aforementioned procedures did not achieve the desired skin tightening. Consequently, there has been an innovation in the UAL technique known as VASER and radio frequency (RF) skin enhancement. Numerous improvements have been made to the original liposuction technique to obtain optimal results. To address the drawbacks of a single procedure, we introduce a groundbreaking fusion of three advanced methods: PURE contouring. The PURE acronym stands for power-assisted liposuction, ultrasound-assisted liposuction and radio frequency-enhanced contouring. By combining these modalities, we mitigate the limitations of each procedure and deliver the best body contouring results.
Methods
This retrospective study was conducted at an aesthetic surgical centre in New Delhi over a period of three years, from September 2021 to December 2024. A total of 1,968 patients who underwent body contouring procedures were reviewed. Each patient underwent a comprehensive medical history assessment and clinical examination of the concerned body region. Routine blood investigations were performed to assess fitness for general anaesthesia. In cases with suspected hernias or previous abdominal surgeries, additional imaging, such as ultrasound or computed tomography (CT) of the abdomen, was conducted.
On the day of surgery, preoperative skin markings were performed in standing position. Following the induction of anaesthesia, tumescent infiltration was administered using a solution containing 1L of normal saline, 10 mL of 2% lignocaine, one ampoule of adrenaline and one ampoule of tranexamic acid. The solution was evenly distributed using a basket cannula attached to the PAL system. The volume of infiltration was predetermined based on the fat to be aspirated, maintaining a ratio of 1:1 to 1:2. The average amount of fat aspirated is directly influenced by the specific anatomical area being operated upon.
Subsequently, UAL was performed, progressing from the superficial to the deeper fat layers to prevent burn injuries. The UAL device settings were adjusted to 80% in C mode for deeper fat targeting and 70% in V mode for superficial fat removal and body contouring. PAL was then utilised to aspirate the fat and smooth out any uneven areas. Superficial liposuction was also performed using the PAL system for enhanced contour definition. PAL was used to aspirate the fat.
Following liposuction, a RF enhancement technique was employed for additional skin tightening and contour refinement. The treatment areas were divided into 10 cm ´ 15 cm grids, designated as treatment zones. A total energy deposition of 6-12 J per treatment zone was administered, with higher energy levels applied to thicker fatty layers and lower energy levels for thinner areas. RF cannulas of varying lengths, diameters and tip configurations were selected based on the targeted anatomical areas.
Post-procedure, the lowermost ports were left open to facilitate fluid drainage, while the remaining ports were closed using Monocryl 3-0 sutures. A compression dressing was then applied.
Data collection included demographic details, types of liposuction procedures performed using the PURE Contouring technique and postoperative patient satisfaction outcomes. Follow-up evaluations were conducted for up to three to six months, with additional assessments scheduled as needed in cases of reported complications (Figures 1–6). Statistical analysis, including chi-squared tests, was conducted to determine associations between patient characteristics and satisfaction levels.
Before and After Six Months Pictures of PURE Contouring of 38-year-old Male Chest and Abdominal Area Showing Good Shape Transformation and Skin Shrinkage.

Before and After Eight Months Pictures of PURE Contouring with High-definition Results of 27-year-old Male Chest and Abdominal Area Showing Good Shape Transformation and Skin Shrinkage.

Before and After Seven Months Pictures of PURE Contouring with High-definition Results of 36-year-old Male Abdominal Area Showing Good Shape Transformation.

Before and After Six Months Pictures of PURE Contouring of 42-year-old Male Chest Area Showing Good Shape Transformation and Skin Shrinkage.

Before and After Six Months Pictures of PURE Contouring with High-definition Results of 26-year-old Female Abdominal Area Showing Good Shape Transformation and Definition.

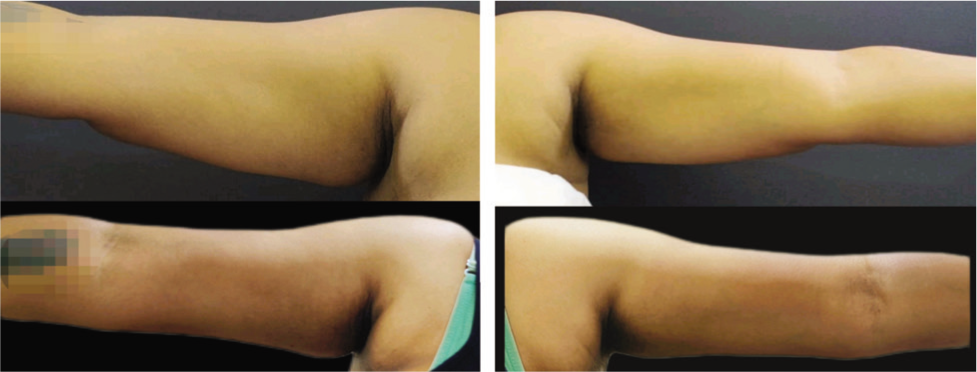
Before and After Ten Months Pictures of PURE Contouring of 42-year-old Female Arm Showing Good Shape Transformation Along with Skin Shrinkage.
Results
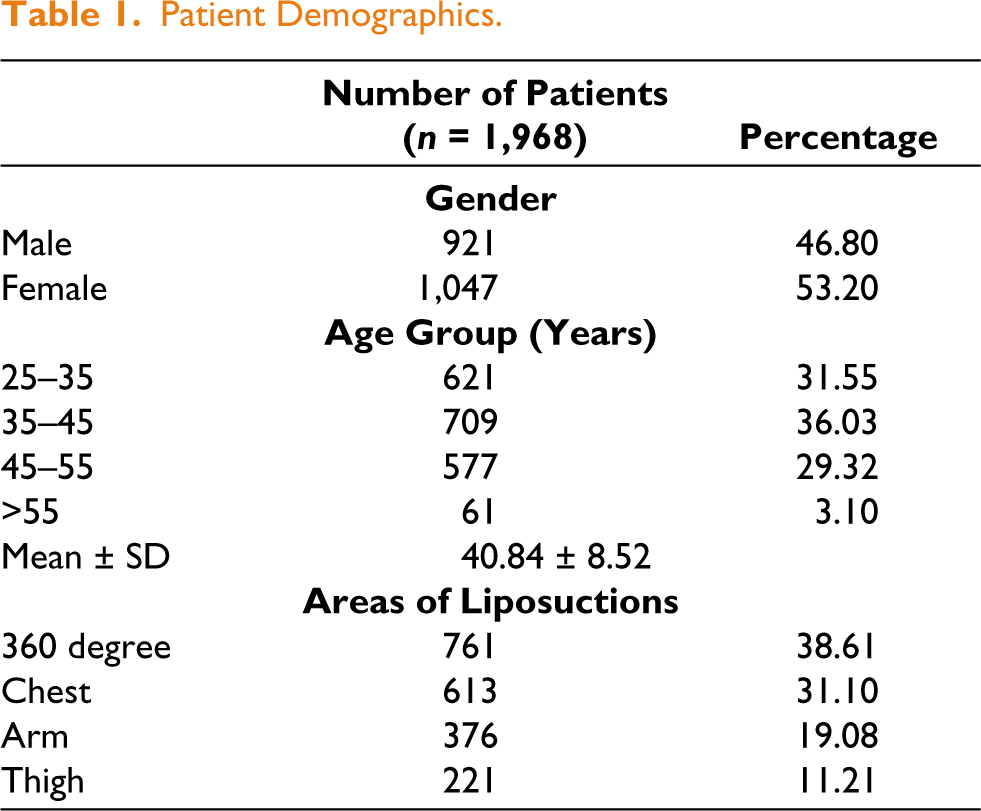
A total of 1,968 patients underwent liposuction procedures, with a slight female predominance (53.2%) compared to males (46.8%). The mean age of the cohort was 40.84 ± 8.52 years, with the majority of patients falling within the 35-45 years age group (36.03%). Among the liposuction procedures performed, 360-degree liposuction was the most common, accounting for 38.61% of cases (Table 1).
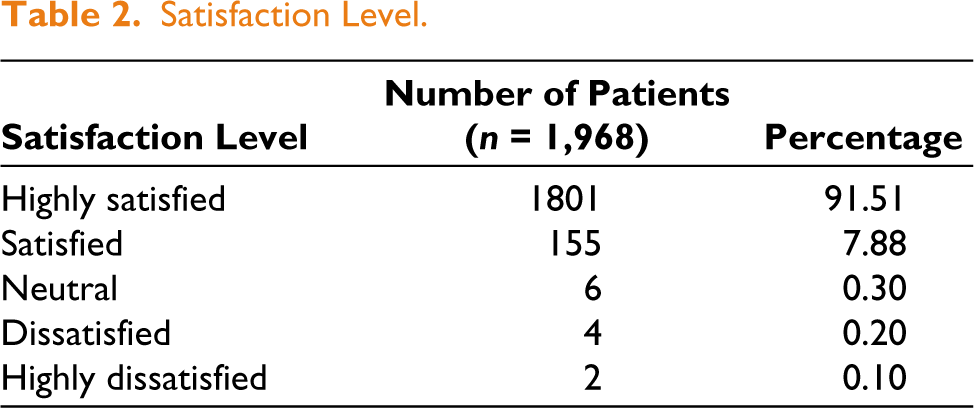
Postoperative satisfaction was notably high, with 91.51% of patients reporting being highly satisfied with their results. Satisfaction was measured using a 5-point Likert scale. No major complications were reported (Table 2).
High patient satisfaction rate underscores the success and effectiveness of the procedures performed. This strong positive response suggests that most patients not only achieved their desired aesthetic outcomes but also had a smooth surgical and recovery experience.
Patient Demographics.
Satisfaction Level.
Discussion
The first attempt to remodel the body silhouette dates back to 1921 when Charles Dujarrier attempted to remove subcutaneous fat by using a uterine curette from the calf and knees of a ballerina. 4 Unfortunately, this ultimately resulted in the amputation of a leg. This unfortunate complication dampened interest and curbed further development in this procedure for many decades. The first surgeons to add suction to facilitate fat extraction in 1974 were father and son gynaecologists Arpad and George Fisher, from Italy.5,6 Since the introduction of liposuction, several modifications have been made to the original concept to make it more effective and to reduce the incidence of complications. Illouz was responsible for monumental advances, the most important contribution being the introduction of blunt instrumentation in 1977, which removed fat while respecting the other surrounding structures. 7 As a result, complications were dramatically reduced and the procedure became reproducible. Pierre-Francois Fournier, in collaboration with Illouz, further improved liposuction techniques. 8 They became known as the pioneers of liposuction as we know it. In 1989, Marco Gasparotti described ‘superficial subdermal liposuction’, which enabled more effective skin retraction and thus further widening the utility of this procedure. 9
SAL is the leading gold-standard method of liposuction, which involves the insertion of a cannula connected to a vacuum-assisted aspirator through a stab incision in the skin and tunnelling through the subcutaneous fat to break it up. 1 To target larger areas tumescent anaesthesia is infused under general anaesthesia. If performed by an inexperienced surgeon, SAL has a greater risk to the skin and its blood supply despite being an inexpensive method of fat removal. Bruising and the possibility of a lengthier recovery are additional dangers to be taken into account while using this procedure. Although SAL is beneficial for a large number of patients, new technologies have produced alternative methods that provide improved accuracy, effectiveness and patient satisfaction.
PAL is also known as vibroliposuction. The major technological advancement era in the development of PAL was in 1990, introduced by Malak and Rebelo. 10 The manufacturers created a sophisticated device which produces oscillating reciprocal to-and-fro movements of the cannula tip with a 2 to 3-mm stroke and 2,000 to 4,000 cycles per minute vibration range generated by the motorised handpiece to aspirate fat. 11 The vibration facilitates easy penetration of even fibrous fat while generating less thermal energy, thereby reducing the risk of cutaneous burns and necrosis. While primitive PAL systems were powered by compressed gas, modern devices utilise a motorised or pneumatic unit. The oscillating movement mimics the surgeon’s technique during SAL, and the speed of the cannula movement can be adjusted according to the surgeon’s preference. This results in less strain on the surgeon and simplifies fat extraction, particularly in cases involving more fibrous fat. In our study, we used this modality after emulsification of the fat through UAL, which further reduces the work of a surgeon. Numerous studies comparing PAL and SAL have documented that PAL is superior in terms of ease, speed of fat extraction, faster healing and recovery times for patients, shorter procedure durations, reduced surgeon fatigue and a lower incidence of the need for secondary procedure. 12
UAL was initially developed in the late 1980s. 13 The driving force behind the improvement and evolution was mainly the nonuniformity to treat difficult fibrous areas via traditional SAL. 14 UAL utilises ultrasonic energy to break down fat and facilitate suction-assisted removal. Its mechanism of action is primarily mechanical and cavitation, along with some thermal effects, which provide skin retraction owing to ‘stimulation’ of the subdermal collagen of the treated areas. With this technique, there is a selective destruction of the connective tissue in between the fatty cells since UAL can target only tissue with low density and low molecular cohesion. Vessels, nerves, elastic fibres and connective tissue fibres of the subcutaneous structures are preserved. SAL, on the other hand, is an unselective methodology and is unable to target only the adiposity, while all the anatomical components are attacked and destroyed, such as vessels and elastic fibres. This explains why UAL is accomplished with low blood loss, and the haematocrit drop after surgery is considerably reduced. SAL leads to a 1% decrease in haematocrit with 450 mL of fat removal, whereas UAL results in a 1% drop in haematocrit with 1,050 mL of aspiration. This is the reason why more fat can be removed without great blood loss using UAL.
We employed ultrasound technology, utilising solid, small-diameter, multiringed probes that deliver energy in pulsed mode at the necessary level for targeting and disrupting fatty tissues at 36 kHz. 15 This was the initial step we took immediately after infiltration to emulsify the fat. However, the degree of skin contraction achieved by this method is insufficient, as we focused the procedure solely on the emulsification of fat and hence employed it for less duration of time. Instead of using ultrasound energy for 1 minute per 100 mL of fluid infiltration, we used it only for 25 to 30 seconds per 100 mL infiltration. This much energy is enough to emulsify the fat but not enough for skin shrinkage/ heating. The benefits of UAL we believe include reduced surgeon fatigue, improved outcomes with less blood loss in fibrous areas and in secondary procedures, more uniform treatment of fat layers and enhanced contour with less need for revisions. Disadvantages involve an increase in surgical time (40% longer), the cost of the equipment, a steep learning curve, larger incisions and the risk of thermal skin injury from unregulated heat. To counter this, we implemented RF as a method for achieving desired skin tightening.
RF is an exceptional modality for treating soft tissue laxity such as sagging abdomen, upper limbs and thighs. It provides aesthetically appealing results and high patient satisfaction, regardless of the degree of lipodystrophy and skin ptosis. Radio frequency-assisted liposuction (RFAL) of the BodyTite system makes use of a novel technology wherein a bipolar device is used to deliver a regulated energy resulting in fat liquefaction, improved haemostasis and skin tightening via skin contraction. 16
The BodyTite handpiece features two significant safety mechanisms that reduce the risk of indirect thermal injuries. The primary safety mechanism restricts the delivery of RF energy to the lax tissue treated between the two electrode probes. The secondary safety mechanism enables the superior external electrodes to function as a thermostat. At the predetermined temperature range of 38-42°C, this feature automatically shuts off. Both of these safety features facilitate safer use of the device. The effective and prolonged heating of the procedure promotes thermal stimulation of the subdermal layer, which encompasses the complete matrix of adipose tissue along with the vertical and oblique fibrous septa. 17 This leads to a strong three-dimensional retraction and contraction of the entire soft tissue envelope in a controlled manner. Thus, by using this modality, we can achieve the desired skin contraction while avoiding thermal burns, which are often caused by UAL. Additionally, the peri-umbilical contraction and improvement in its shape further enhance the aesthetic outcome, contributing to a more defined and harmonious abdominal contour.
We combined the advantages of the aforementioned technologies in our study to create an innovative merger known as PURE, which stands for PAL, UAL and RF-enhanced contouring (Figure 7).

2. PAL→ by MicroAire. 3. VASER→ Ultrasonic Systems. 4. Bodytite, Radiofrequency Assisted Lipolysis (RFAL).
With the introduction of PAL, surgeon strain is significantly reduced, particularly when targeting more fibrous areas. This is a crucial consideration in large volume liposuction, as surgeon fatigue can lead to suboptimal outcomes. In PAL, the reciprocating power cannula operates at tissue level, mirroring the manual movements executed in SAL on an extremely microcosmic scale. The lateral movement is minimised, thereby reducing trauma to the surrounding tissue. Katz et al. proposed a study in which power liposuction was performed on one side of the body, while traditional liposuction was conducted on the corresponding contralateral side. 19 The time taken to perform powered liposuction was 35% less, and intraoperative pain was 45% less compared to traditional liposuction. Postoperative pain, ecchymoses and oedema were observed to be between 32% and 38% less on the side of the body that underwent powered liposuction. 18 The advantage experienced by us in our study was less effort applied by the surgeon as most of the fat was emulsified with the UAL and the motorised handpiece with suction helped in aspiration and equalisation of the fat.
Zocchi reported 1 point of haematocrit drop per 1,400 mL of aspirated fat by UAL compared to 1 point drop of haematocrit per 300 mL of aspirate in SAL and 40% more skin retraction than other methods. 19 In 2000, Howard and Rohrich studied cell rupture after liposuction using creatinine kinase as a marker and their results were as follows: 70%-90% cell rupture in internal ultrasound compared to 5%-20% in SAL. The cell rupture was 30% higher in UAL than in SAL resulting in faster fat lysis. 20 Another interesting factor was formation of free H2O2 in treated areas that acts as a bactericidal, reducing the chances of infection. 21 UAL proves to be a novel modality wherein it breaks down fibrous septa and fat cells preserving the vessels and nerves, giving a smooth contour and skin retraction that is better than traditional liposuction techniques where irregularities in final outcome are not uncommon. By setting the time of UAL to emulsification of fat, we encountered no chances of skin burn or necrosis in our study. And to counteract the minimal contraction caused by UAL, we used RF to achieve desired results of skin tightening.
Another advantage of RF is that it also helps in collagen remodelling. Blugerman et al. demonstrated 8%-15% linear tightening at the end of the surgery on the operating table, which further increased dramatically during the first week of follow-up when most of the swelling was reduced. The maximum contraction was noted by them at the follow-up visit of 24 weeks after the treatment which varied from 12.7% up to 47% depending on the patient and treatment variables. 17
Thus, we could achieve the intermingling of art and science, enabling individuals to transform their bodies and enhance their self-image. These procedures offer a pathway to achieving desired contours and addressing areas of concern that may not respond to traditional methods. All patients opting for body contouring are likely to benefit from this procedure for more defined and aesthetically pleasing outcomes.
Conclusion
Currently, liposuction is one of the most accomplished aesthetic interventions to redefine a patient’s body profile. In this study, we performed PURE by performing UAL where fat emulsification occurs, allowing it to be suctioned out using PAL, providing better definition to contour different body areas, followed by skin tightening using RF.
With our innovative merger technique of PURE, an overwhelming 91.51% of patients reported high satisfaction with their outcomes, reflecting the efficacy of the procedures and the quality of care provided. These findings underscore the safety, effectiveness, feasibility and acceptance of PURE as a key body contouring procedure. With careful execution, this combined PURE modality can be a powerful tool for achieving aesthetic transformation in patients with realistic expectations.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr. Adarsh Keshari from Team APAR health for medical writing assistance and data analysis (CARE PROGRAM).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.