
Abstract
Changes in body habitus and age-related soft tissue descent can alter the body’s centre of mass, thus centre of gravity and loading patterns, contributing to postural maladaptations and myofascial dysfunction. Previous studies have demonstrated postural improvement and reduction in back pain after abdominoplasty and rectus plication; however, to our knowledge, no reports have described comprehensive body contouring as a functional intervention to reat Gluteus Medius Syndrome. A 61-year-old female with a history of L4 fracture managed conservatively presented with progressive buttock pain and ambulatory limitation consistent with Gluteus Medius Syndrome. She underwent a combined single-session procedure: abdominoplasty with rectus plication (preserving infra-umbilical Scarpa’s fascia), 360° waist liposuction, liposuction of the lateral thighs, buttock lift with autologous adipo-dermal pedicled auto-augmentation cranial adipo-dermal paddle rotation). Total aspirate/excised volumes were 6 L of fat and 4.3 kg of skin flaps. The postoperative course was uncomplicated. By 8 months post-op, the patient reported complete resolution of buttock pain and returned to habitual ambulation, now walking ~5 km daily beyond routine activities. Photographs at 8 months show improved trunk posture. Comprehensive body contouring that includes abdominal wall tightening and circumferential lift procedures may alter the body’s centre of gravity and spinal loading sufficiently to produce clinically meaningful improvements in posture and function. This single case suggests a potential functional role for plastic surgical body contouring beyond aesthetic benefit. Prospective studies using objective postural and gait metrics are needed to conclusively recommend this approach broadly.
Keywords
Level of Evidence
Level V (Case report).
Introduction
Mobility and ambulation are fundamental determinants of quality and longevity of life, and their decline is associated with increased morbidity in older adults. 1 Age-related soft tissue descent (abdominal laxity, diastasis recti, sagging gluteal tissues) combined with altered fat distribution can shift the body’s centre of mass, thus centre of gravity anteriorly, increasing strain on antigravity musculature and potentially precipitating myofascial and tendinous disorders. Prior work has demonstrated that abdominoplasty with rectus plication and targeted trunk contouring can lead to measurable postural improvements and reductions in back pain,2,3 likely through restoration of trunk stability and modification of load distribution.
Gluteus Medius Syndrome—a clinical spectrum encompassing tendinopathy, partial tears, and myofascial dysfunction of the hip abductors—commonly manifests with lateral buttock pain and gait disturbance, and is typically managed conservatively or with targeted tendon repair when indicated. 4 We present a novel case in which a comprehensive body contouring strategy was applied with the explicit functional intent to realign the centre of gravity, resulting in resolution of symptomatic Gluteus Medius Syndrome and restoration of ambulatory capacity.
Case Presentation
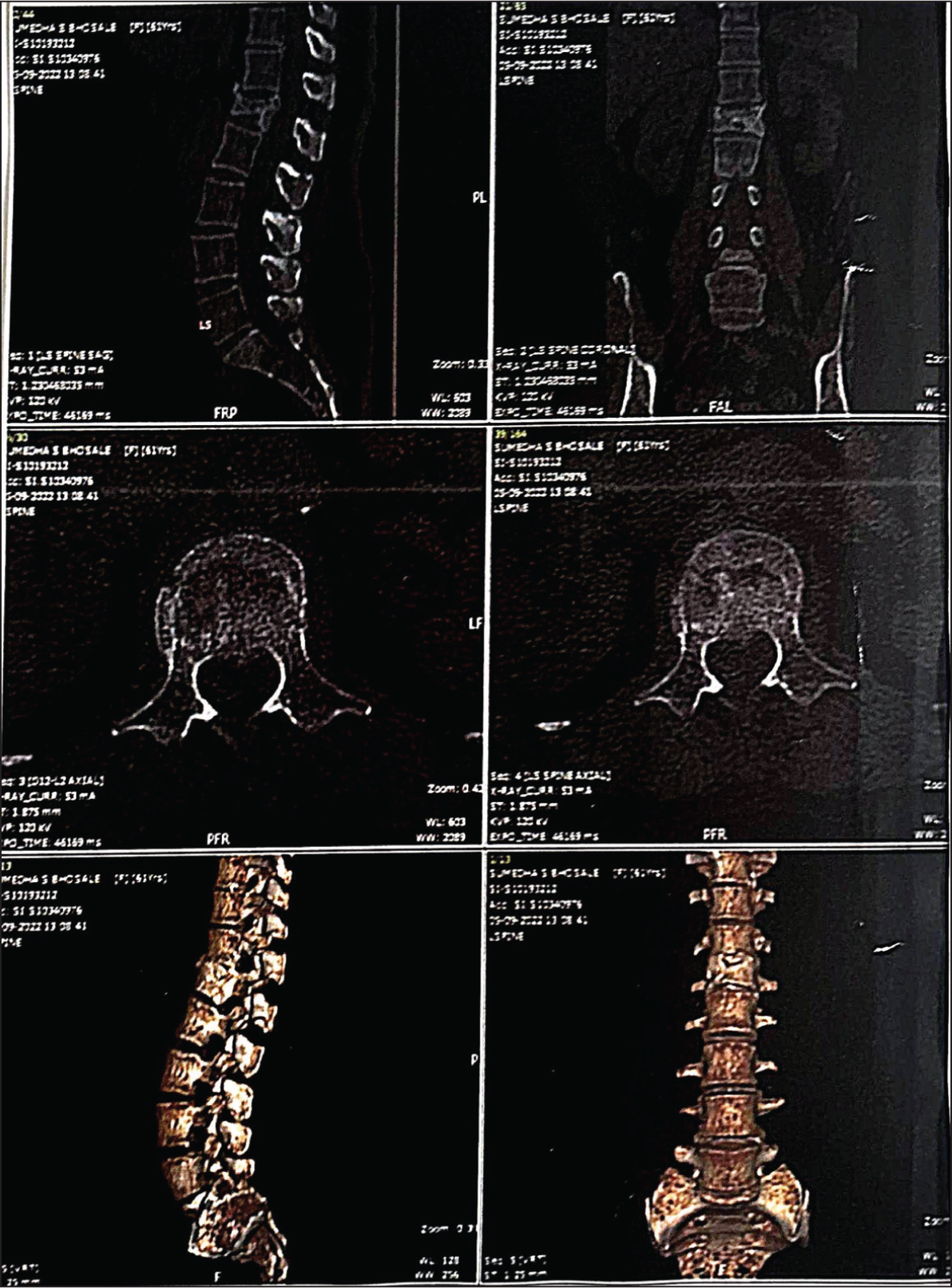
A 61-year-old woman (height 162.6 cm, weight 70.5 kg, BMI ~26.7 kg/m²) sustained an L4 vertebral fracture in a motor vehicle collision two years earlier (Figure 1). The fracture was managed conservatively with extended bed rest and a lumbar support brace; subsequent healing was documented radiographically, and she received calcium supplementation. Following resumption of activities, she developed progressive, activity-related pain in the buttock and reduced walking tolerance; she was assessed by an orthopaedic specialist and given a diagnosis of Gluteus Medius Syndrome. Conservative measures, including physiotherapy and activity restriction, were undertaken, and she was advised to limit ambulation to <2 km/day. Previously an active walker (≈6 km/day), the functional limitation had a significant negative impact on her quality of life.
Two years after the index injury, she presented to our clinic seeking both functional recovery and aesthetic body renewal. After routine preoperative evaluation and clearance for anaesthesia, we offered a combined, single-session operation consisting of:
Abdominoplasty with midline rectus plication, preserving infra-umbilical Scarpa’s fascia; 360° waist liposuction (manual technique) for torso contouring; Buttock lift with pedicled autologous adipo-dermal paddle auto-augmentation (cranial adipo-dermal paddle lifted on its pedicle and rotated caudally to augment the gluteal contour); Manual liposuction of lateral upper thighs to improve hip and thigh silhouette.
The combined procedure lasted approximately eight hours under general anaesthesia. Total aspirate/excision: ~6 L of fat removed; 4.3 kg skin flaps excised. There were no intraoperative complications. The patient began routine ambulation on postoperative Day 1; sutures were removed at two weeks. A compression garment was worn continuously for six weeks, then intermittently up to six months.
Clinical course and outcomes: The patient’s postoperative recovery was uneventful. She progressively increased activity and was encouraged to resume full activities at six weeks. At eight months postoperatively, she reported complete resolution of lateral buttock pain and restoration of pre-injury ambulatory levels; she currently walks ~5 km daily beyond routine ambulation. Objectively, weight decreased to 64 kg and standing height measured 161.5 cm. Photographs (anterior and lateral views) taken at 8 months demonstrate improved trunk posture with less forward lean and a more posterior torso alignment (Figures 2 and 3). The patient provided written informed consent for surgery and publication of clinical data and images.


Discussion
This case illustrates a potentially under-recognised functional benefit of comprehensive body contouring in older adults: altering trunk mass distribution and augmenting posterior soft tissues may realign the body’s centre of gravity 5 and improve ergonomic loading of the spine and myofascial system, thereby relieving symptoms originating from abductor pathology.
Existing literature supports the concept that abdominal wall correction can affect posture and functional symptoms.2,3 Objective studies have documented changes in centre-of-pressure and trunk orientation after abdominoplasty and rectus plication, and series have reported improvement in chronic back pain following abdominoplasty—effects attributed to both tissue resection (mass redistribution) and abdominal wall strengthening. These prior reports provide physiological plausibility for our hypothesis: reduction of anterior trunk mass and restoration of abdominal support shifts the centre of gravity posteriorly and reduces compensatory forward trunk lean, thereby altering load transfer to the hip abductor complex.
To our knowledge, there are no prior published reports specifically documenting the resolution of Gluteus Medius Syndrome following a targeted programme of body contouring. The case, therefore, appears to expand the functional narrative of body contouring surgery from purely aesthetic to potentially therapeutic in select patients with posture-dependent myofascial syndromes.
Important limitations merit emphasis. This is a single-patient report without objective kinematic or biomechanical measurements (force plate analysis, centre-of-mass modelling, gait lab data) and thus cannot establish causality. The preoperative diagnosis of Gluteus Medius Syndrome was made by an orthopaedic colleague, but we do not have EMG or MRI evidence of tendon tear vs tendinopathy; baseline quantitative gait/posture metrics were not recorded. The observed improvement may reflect a combination of factors, including surgical restoration of trunk stability, rehabilitation progression, weight loss, and improved confidence and activity levels following aesthetic enhancement.
Future direction: The promising outcome in this patient justifies a structured investigation. Prospective studies with objective biomechanical endpoints (3-D posture analysis, centre-of-pressure/force plate testing, validated pain and function scales), control groups (physiotherapy alone, abdominoplasty alone), and longer follow-up are required to determine which patients might benefit, the durability of effect, and safety considerations in older populations. If confirmed, plastic surgeons could collaborate with orthopaedics and rehabilitation specialists to define selection criteria, perioperative protocols, and outcome measures. Postural improvement and the gait stability achieved, resulting in improved quality of life, could potentially be a driver in adopting extensive body contouring procedures as a routine practice for the high-functioning individuals of the geriatric population.
Conclusion
Comprehensive body contouring, which may combine any or all of breast reduction, abdominal wall tightening, circumferential torso liposuction, back lift, belt lipectomy, buttock auto-augmentation, thighplasty, liposuction of thighs, may shift trunk mass distribution and realign the centre of gravity, producing clinically meaningful improvements in posture and load distribution. Thereby producing an improvement in function and thus quality of life. In this case, such an approach was associated with complete resolution of symptomatic Gluteus Medius Syndrome and restoration of ambulatory capacity at eight months. While encouraging, this single case cannot justify broad clinical recommendations. We advocate for prospective, controlled studies with objective biomechanical measures before recommending body contouring procedures as routine functional therapy for geriatric individuals.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Statement
Written informed consent for surgery and publication was obtained from the patient. This is a single case report; no institutional review board approval was sought.
Funding
The author received no financial support for the research, authorship and/or publication of this article.