
Abstract
Background
AdvanSync 2 is one of the most commonly used fixed functional appliances for the management of skeletal Class II malocclusion. However, its bulky design may cause discomfort to patients. The Carriere Motion Appliance (CMA) is a more recently introduced fixed functional appliance that produces treatment outcomes comparable to those of AdvanSync 2. This retrospective study aimed to compare the effectiveness of CMA and AdvanSync 2 in the treatment of Class II malocclusion.
Materials and Methods
The study included 20 patients, who were divided into two equal groups. Ten patients were treated using the AdvanSync 2 appliance, while the remaining 10 received treatment with the CMA. Pre-treatment and post-treatment lateral cephalometric radiographs were obtained for all participants. These radiographs were analyzed to evaluate and compare the skeletal and dentoalveolar changes associated with each appliance.
Results
Both appliances successfully corrected the Class II molar relationship. The AdvanSync 2 group demonstrated statistically significant changes in Sella, Nasion, and Point B (SNB) and A point-Nasion-B point (ANB) angles, indicating notable skeletal improvement. In contrast, the CMA group showed minimal skeletal alterations. As CMA treatment relies on patient cooperation, compliance played an important role in treatment success, whereas AdvanSync 2 functioned independently of patient involvement. Molar distalization was achieved effectively in both groups; however, a greater degree of lower incisor proclination was observed in patients treated with AdvanSync 2.
Conclusion
The CMA appliance is effective in managing dental Class II malocclusions by improving molar and canine relationships, although its skeletal effects are limited, particularly in patients with maxillary prognathism. Successful outcomes with CMA depend largely on patient compliance. In comparison, AdvanSync 2 is a non-compliance-dependent fixed appliance that produces greater skeletal correction through mandibular advancement and restriction of maxillary growth, making it a more suitable option for moderate to severe skeletal Class II malocclusions.
Keywords
Introduction
Class II malocclusion is a significant issue in orthodontics, with studies suggesting that mandibular retrognathism is the main cause. 1 Correction of this discrepancy is ideally achieved by addressing its primary etiological factor, which involves modifying the magnitude or vector of mandibular growth. Functional appliances, either removable or fixed, are commonly employed for this purpose. A wide range of functional appliance designs has been developed to manage Class II skeletal and occlusal discrepancies. The mechanism of neuromuscular adaptation to functional appliances is complex, with theories ranging from isometric muscle contractions to viscoelastic properties. Two general strategies for treatment of Class II malocclusion are to intervene during pre-adolescent years (ages 8–11) with limited goals and to complete the entire correction during adolescence or post-pubertal stage, where fixed functional appliances (FFAs) play a major role. FFAs can be rigid, flexible, or hybrid.
AdvanSync 2 is a rigid FFA designed for Class II correction that operates on a molar-to-molar mechanism and enables the simultaneous achievement of skeletal and dentoalveolar treatment effects. 2 Though the effectiveness and efficiency of the AdvanSync 2 appliance are well established in the literature, but the appliance is bulky, causes patient discomfort during eating and phonation, and frequent de-cementation are its few drawbacks.
The Carriere Motion Appliance (CMA; Figure 1) was introduced in 2004 as a semi-fixed intraoral device for the treatment of Class II malocclusion. 3 It was developed as an alternative approach for maxillary molar distalization and contributes to sagittal correction mainly through controlled mandibular repositioning. The appliance features a slim, low-profile design that improves patient comfort and is intended to promote bodily distal movement of the maxillary molars rather than simple crown tipping. Its ball-and-socket mechanism, located anterior to the molar pad bonded to the maxillary first molars, permits controlled distopalatal rotation around the palatal roots, thereby facilitating effective sagittal molar correction. Figure 2 shows AdvanSync 2 appliance intra orally.
Carriere Motion Appliance (CMA).

AdvanSync 2 Appliance.

However, the use of Class II intermaxillary elastics in combination with the CMA may lead to some degree of anchorage loss. This is most commonly observed as mesial movement of the mandibular dentition and proclination of the lower incisors. These unwanted effects can be reduced by incorporating a mandibular Essix appliance to improve lower arch anchorage. Current literature on the CMA remains limited and has primarily focused on dentoalveolar changes, with relatively few studies evaluating its skeletal effects or comparing it directly with the AdvanSync 2 appliance. Therefore, the present study aimed to assess and compare the skeletal and dental effects of the CMA and AdvanSync 2 in the management of Class II malocclusion.
Materials and Methods
This retrospective study evaluated 20 adolescent patients with Class II malocclusion, including 10 treated with the CMA and 10 treated with the AdvanSync 2 appliance.
The participants were equally divided into two groups (n = 10 per group). All patients were selected from the outpatient clinic of the Department of Orthodontics and Dentofacial Orthopedics at Rural Dental College, Loni. Group allocation was performed using a randomization procedure to ensure unbiased distribution.
Group I (CMA) consisted of patients aged 11–15 years, with six males and four females.
Group II (AdvanSync 2 appliance) included patients aged 10–15 years, with five males and five females.
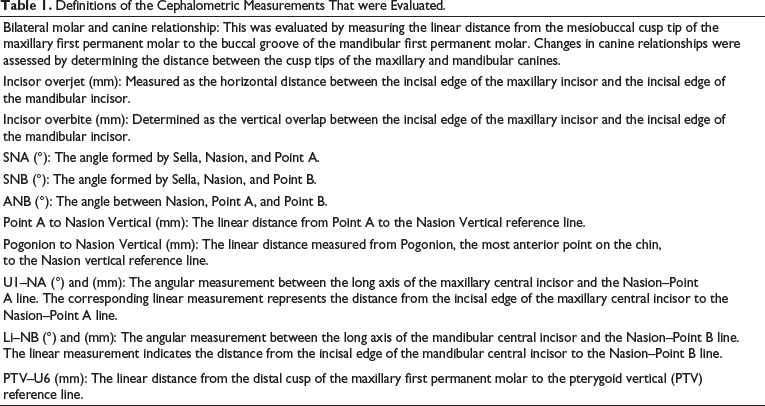
All patients were in the late adolescent growth phase as assessed clinically and from cervical vertebral maturation (CVM) stages recorded in the pre-treatment lateral cephalograms (Table 1).
Definitions of the Cephalometric Measurements That were Evaluated.
Sample Size
The total sample size was 20. The data was coded and entered into Microsoft Excel spreadsheet. Analysis was done using IBM SPSS (SPSS Inc., IBM Corporation, NY, USA) Statistics Version 25 for Windows software program.
Descriptive statistics, including mean and standard deviation, were calculated for all variables.
Within-group comparisons between pre- and post-treatment values were performed using paired t-tests.
Intergroup comparisons were carried out using independent t-tests.
The level of statistical significance was set at p < .05, with 95% confidence intervals.
Method error was assessed by retracing 10 randomly selected lateral cephalograms after a 2-week interval, and intra-observer reliability was evaluated using the intra-class correlation coefficient (ICC).
A comparative analysis was carried out using lateral cephalometric radiographs taken before the initiation of treatment and after completion of the functional phase with either the CMA or AdvanSync 2, at the point when a bilateral Class I molar relationship had been achieved.
Participants were selected based on the following inclusion criteria: (a) presence of late mixed or permanent dentition at the start of treatment; (b) bilateral Class II molar relationship of end-to-end or greater severity; (c) bilateral Class II canine relationship with at least a half-unit discrepancy; and (d) successful completion of treatment with establishment of bilateral Class I molar and canine relationships. Patients with syndromic conditions, skeletal deformities, or those treated with unilateral CMAs were excluded from the study. Ethical approval was obtained from the Institutional Ethics Committee prior to the commencement of the investigation.
The study involved the placement of AdvanSync 2 crowns. The crowns were cemented with glass inomer cement (GIC). Telescopes were attached to the distal casings of the upper crowns, and the lower telescopes were fastened into the mesial casings. After every 6–8 weeks, the patients were recalled to check the correction of mandibular advancement and Class I molar relationship.
In the CMA group, the appliance was placed and activated in accordance with the manufacturer’s recommended protocol. Buccal tubes equipped with elastic hooks were bonded to the mandibular first molars, and additional lower arch anchorage was provided using a 1-mm-thick clear Essix appliance that covered the entire mandibular dentition.
Elastic wear was initiated with Force 1 elastics (¼-inch, 6 oz) during the first month of treatment. Subsequently, Force 2 elastics (3⁄16-inch, 8 oz) were prescribed and continued until a bilateral Class I molar relationship was achieved. Patients were instructed to wear the elastics full-time, removing them only during meals and oral hygiene procedures. They were also advised to replace the elastics every 24 h to maintain consistent force levels.
Results
The results (Table 2) indicate significant changes induced by the CMA, mainly in the dental variables. Although there were fewer changes in skeletal variables, Sella, Nasion, and Point B (SNB) increased by 2.5°, showing forward mandibular growth. A point-Nasion-B point (ANB) decreased by 2.4°, suggesting improved maxillomandibular relationship (p = .002).
Comparison of Treatment Effects Within the CMA Group (Mean Values).
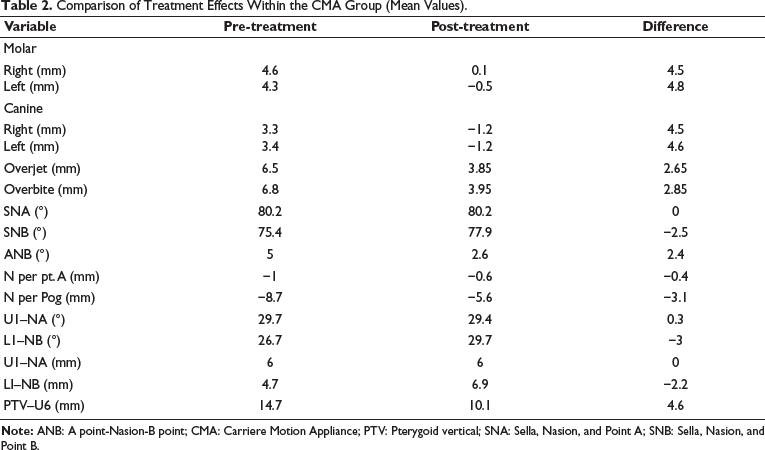
Minor changes in molar positions were observed, with a slight distal shift. Canines moved notably forward (≈1.2 mm bilaterally).
The inclination of the maxillary incisors did not demonstrate any statistically significant change following treatment. In contrast, patients treated with the CMA exhibited proclination and anterior movement of the mandibular incisors, with an increase of approximately 3° in the L1–NB angle and a linear advancement of about 2.2 mm. Additionally, reductions in overjet and overbite of 2.65 and 2.85 mm, respectively, were observed.
Furthermore, an improvement in the anteroposterior relationship between the maxillary and mandibular molars was noted, primarily due to distal movement of the maxillary first molars. The U6–PTV measurement indicated a significant distalization of 4.6 mm (p = .001).
In the soft tissue parameters, Pogonion (N per Pog) advanced 3.1 mm, supporting mandibular advancement.
The results (Table 3) within the AdvanSync 2 group showed a difference in the mandibular skeletal measurements of an increase by 2.9°, suggesting mandibular advancement, while no significant change was observed in the maxilla. There was seen a decrease of 3.9° in ANB, reflecting significant improvement in skeletal Class II relationship (p = .003).
Comparison of Treatment Effects Within the AdvanSync 2 Group (Mean Values).
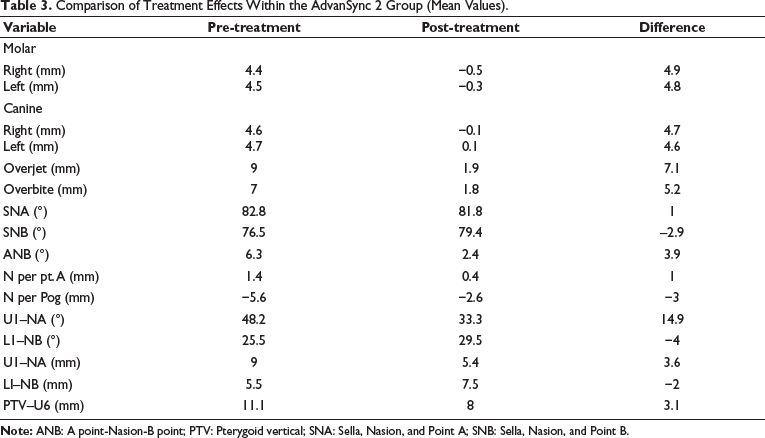
Molars showed minor distalization (right: −0.5 mm, left: −0.3 mm), and canine positions were largely stable, with minimal change (≈0.1 mm).
The maxillary incisors exhibited a statistically significant decrease in inclination, with an average retroclination of 14.90° and a mean retraction of 3.6 mm. In the mandibular arch, the incisors demonstrated a proclination of approximately 4°, along with a forward movement of 2 mm.
A significant reduction in both overjet and overbite was recorded, with mean decreases of 7.1 and 5.2 mm, respectively. In addition, a marked improvement was noted in the anteroposterior molar relationship, reflecting distal correction of the maxillary molars relative to the mandibular molars.
This was supported by the U6–PTV measurement, which indicated significant distal movement of the maxillary first molars, with a mean distalization of 3.1 mm (p = .001).
In the soft tissue parameters, Pogonion (N per Pog) advanced by 3 mm, supporting mandibular advancement.
Skeletal Effects
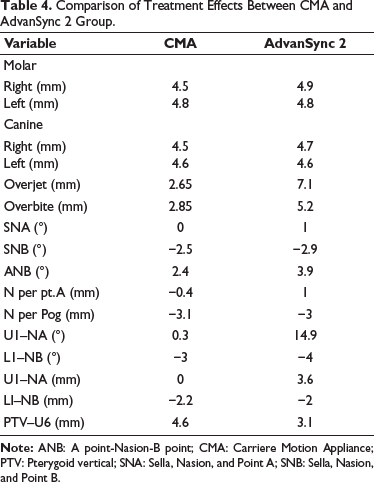
At the pre-treatment stage, both groups demonstrated skeletal Class II patterns, as presented in Table 4. Following treatment, no statistically significant difference was observed between the groups with respect to maxillary position or dimensions. In contrast, mandibular adaptations showed a significant intergroup variation in SNB values, with increases of 2.5° in the CMA group and 2.9° in the AdvanSync 2 group. Both groups exhibited a reduction in ANB angle, reflecting an improvement in sagittal jaw relationship. This reduction was more marked in the AdvanSync 2 group. Specifically, the CMA group demonstrated a decrease of 2.4°, whereas a greater reduction of 3.9° was recorded in the AdvanSync 2 group.
Comparison of Treatment Effects Between CMA and AdvanSync 2 Group.
Dental Effects
Both treatment modalities resulted in mild retrusion of the maxillary incisors, accompanied by proclination and forward displacement of the mandibular incisors (CMA: 3° and 2.2 mm; AdvanSync 2: 4° and 2 mm). A reduction in overjet and overbite was observed in both groups, with relatively greater improvement noted in the AdvanSync 2 group. Enhancement of the anteroposterior molar relationship was achieved with both appliances; however, significantly greater molar distalization was recorded in the CMA group (p = .001).
Soft Tissue Effects
The most notable soft tissue change in both groups was forward positioning of the mandible, with comparable advancement observed between the two treatment modalities.
Both appliances improved Class II malocclusion, but AdvanSync 2 produced more pronounced skeletal and dental corrections, especially in overjet reduction, ANB improvement, and upper incisor control. CMA provided greater molar distalization but less impact on incisor and other skeletal parameters.
Discussion
The CMA reflects a shift toward a minimally invasive, “sagittal-first” approach in orthodontics. This prefabricated appliance is anchored to the maxillary canine and first molar and works by producing molar distalization and derotation, while simultaneously encouraging mandibular advancement through interarch elastics. 3 In this study, CMA treatment resulted in notable dentoalveolar corrections, particularly distal molar rotation. These rotational changes are clinically significant, as mesially rotated maxillary molars occupy more arch space and worsen Class II anteroposterior discrepancies. Their distal rotation not only improves occlusal interdigitation but also facilitates further molar distalization. 4 Improvement in canine relationships was also significant, consistent with earlier studies that highlight CMA’s efficiency in early occlusal correction. Reductions in overjet and overbite were observed as well, most likely due to lower molar mesialization and mandibular anterior repositioning. However, the skeletal changes associated with CMA were relatively modest. The proclination of lower incisors was also moderate. These findings were also confirmed in previous studies by Kim-Berman et al., 5 Clermont et al., 6 and Luca et al. 7
By contrast, AdvanSync 2 is a fixed, rigid appliance that exerts greater skeletal influence, designed specifically for moderate-to-severe skeletal Class II discrepancies. Its non-compliant design, supported by bilateral telescopic mechanisms, ensures consistent forward posturing of the mandible, independent of patient cooperation. Over a 6-month observation period, AdvanSync 2 achieved significant orthopedic correction, demonstrated by reductions in ANB angle and increases in SNB, indicating forward mandibular displacement and improved jaw symmetry. These skeletal corrections were accompanied by visible facial profile improvements, such as reduced mentolabial sulcus depth and better chin projection, underlining its effectiveness in addressing skeletal imbalances during growth.
The present study assessed and compared the skeletal, dentoalveolar, and soft tissue changes produced by the CMA and AdvanSync 2. 8 At the pre-treatment stage, both groups exhibited dentoalveolar features of Class II malocclusion along with underlying skeletal Class II characteristics. In view of the increasing clinical use of the CMA in recent years, an evaluation of its biomechanical effects was considered necessary. Both appliances demonstrated effective treatment outcomes by producing measurable improvements in occlusal and skeletal relationships and a statistically significant improvement in the anteroposterior molar relationship.
In the CMA group, the molar relationship is improved by a mean value of approximately 4.5 mm. This correction appeared to be multifactorial, involving distal movement of the maxillary molars, mesial shift of the mandibular molars secondary to skeletal mandibular changes, and rotational adjustment of the maxillary first molars. While precise assessment of molar derotation is limited to two-dimensional cephalometric records, indirect evaluation can be performed by analyzing positional changes at the mesial and distal aspects of the maxillary first molars. Comparable multidirectional mechanisms contributing to molar correction with the CMA have been documented in earlier studies.9–11 The observations of the present investigation align with previously published findings5, 12 with slight discrepancies that may be attributed to variations in study design and methodological approach.
The limited skeletal influence of CMA on the maxilla observed in this study is in agreement with existing literature.9–12 Likewise, AdvanSync 2 demonstrated only minimal restraint of maxillary sagittal growth. 5 The mandibular skeletal changes associated with CMA were comparable to, or smaller than, those reported in previous studies.5, 10, 11 Furthermore, the significant reduction in ANB angle observed in the CMA group corresponds with findings previously reported in the literature. 13
Upper incisor retroclination was significantly greater in the AdvanSync 2 group than in the CMA group, explained by a headgear effect. 14 The change in upper incisor inclination seen with CMA is noteworthy, as this appliance does not apply direct force to them. This could be beneficial for patients with a high risk of root resorption 11 and aligns with existing literature.12, 15 Some reports, however, have described CMA causing upper incisor proclination in certain clinical scenarios, with decreased overjet and lower incisor proclination.12, 15
Both groups showed lower incisor protrusion, though it was significantly lower with CMA compared to AdvanSync 2. The smaller anchorage loss in mandibular incisors with CMA is consistent with, or even smaller than, findings from previous studies.5, 12, 15–18 In contrast, other treatment modalities such as FFAs or Class II intermaxillary elastics are frequently associated with pronounced anterior dental movement and increased incisor proclination. The relatively minimal anchorage loss observed with the CMA in the present study may be attributed to limited maxillary incisor retraction, reduced duration of elastic wear, and the adjunctive use of a mandibular Essix appliance to reinforce anchorage. 19
Both treatment modalities resulted in significant reductions in overjet and overbite. However, the magnitude of overjet correction achieved with the CMA was comparatively lower than that reported for other Class II correction strategies, including the Forsus appliance or mini-screw-assisted distalization systems, whose outcomes more closely resemble those observed with AdvanSync 2. In the AdvanSync 2 group, the reduction in overjet and overbite was achieved through a combination of skeletal and dentoalveolar adaptations. Conversely, the improvements in the CMA group were largely attributable to dentoalveolar changes, with comparatively limited skeletal contribution. 20
Although dentoalveolar modifications are inherent to Class II correction, AdvanSync 2 appears to provide a more balanced distribution of skeletal and dental effects. This proportional response may enhance long-term stability and potentially reduce the likelihood of relapse.
In summary, our results support that CMA’s main effects are dentoalveolar. Importantly, we were able to highlight the multidirectional molar movements and the critical role of molar derotation in Class II correction, even when assessed with 2D cephalometrics alone. Limitations of the study include (a) its retrospective design, (b) lack of data on patient compliance, (c) restriction to the initial treatment phase without follow-up of later corrections, and (d) reliance on 2D cephalometric imaging, which may involve distortion and anatomical overlap.
From a clinical standpoint, both appliances have distinct advantages:
CMA: Lightweight, esthetic, and effective for early sagittal correction before comprehensive treatment. Best suited for mild-to-moderate Class II cases where compliance is expected, and skeletal discrepancies are not severe. AdvanSync 2: More suitable for non-compliant patients or those with pronounced skeletal discrepancies, especially during peak growth periods when orthopedic effects can be maximized.
Growth as a Confounding Factor
One of the important considerations in interpreting the findings of this study is the influence of growth. Although all patients were categorized as being in the late adolescent growth phase based on CVM stages, individual variations in growth potential cannot be entirely eliminated. Previous longitudinal studies have demonstrated that mandibular growth continues variably into late adolescence, which may augment the apparent skeletal effects of functional appliances.
Therefore, the skeletal changes observed in the AdvanSync group cannot be attributed solely to appliance therapy. The contribution of residual growth must be acknowledged, particularly in retrospective studies where growth modulation cannot be controlled prospectively. This limitation underscores the importance of cautious interpretation of skeletal outcomes and supports the need for long-term follow-up studies to differentiate treatment effects from growth-related changes.
Comparison with Existing Literature
The findings of the present study are in agreement with earlier reports comparing functional appliances and compliance-dependent systems. Studies evaluating FFAs have consistently demonstrated greater improvements in skeletal parameters, particularly SNB angle, when compared to elastic-based systems. Conversely, CMA-focused studies have emphasized its effectiveness in achieving rapid dentoalveolar correction with limited skeletal change.
Differences in reported outcomes across studies may be attributed to variations in patient age, growth status, treatment duration, appliance design, and methodological approaches. The present study adds to the existing literature by providing a direct cephalometric comparison between the CMA and the AdvanSync 2 appliance, highlighting their distinct modes of action in Class II correction.
Limitations
The limitations of this study include its retrospective design, relatively small sample size, and lack of long-term follow-up. Additionally, the influence of growth could not be isolated from appliance effects. Future prospective studies with larger sample sizes, matched growth stages, and long-term evaluations are recommended to further elucidate the skeletal and dentoalveolar contributions of these appliances.
Conclusion
While both appliances contribute effectively to Class II correction, their clinical indications and biomechanical impacts differ:
CMA is most suitable for mild-to-moderate Class II malocclusions with cooperative patients, offering rapid changes in molar relationships, attributed to both linear and rotational changes. AdvanSync 2 is preferred for growing patients with skeletal discrepancies, yielding more significant changes in jaw positioning and facial esthetics. CMA minimizes the lower incisor proclination and prevents anchorage loss, which is rather more evident in the case of AdvanSync 2. A significant amount of distalization is caused by CMA as compared to that of AdvanSync 2. Both appliances produced a statistically significant reduction in overjet and overbite. Further studies with larger sample sizes are required to confirm and strengthen the findings of the present investigation.
Footnotes
Acknowledgment
The authors would like to thank the statistician for providing us with the statistical analysis report.
Authors’ Contribution
All authors have read and agreed to the published version of the manuscript.
Data Availability Statement
The data presented in this study are available on request from the corresponding author (to accurately indicate status).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval Institutional Statement
This study was approved by the Institutional Ethics Committee and Review Board.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
All study participants had provided informed written consent prior to enrollment.