
Abstract
Objective
Functional appliances are used in orthodontics to bring about correction of mandibular retrognathism by forward positioning and eventually remodeling the condyle- glenoid fossa to retain this new position. Research has shown that these appliances have a significant effect on pharyngeal airway of patients. The aim of this study was to evaluate changes in volume and minimum constriction area in the pharyngeal airway using CBCT imaging after correction of mandibular retrognathism with an Advansync2 Class II corrector.
Methods
This single-center study consisted of 20 Class II patients (mean age 14.8 years) who required correction of mandibular retrognathism. The patients were treated with the Advansync2 Class II corrector for an average of 26 weeks. CBCT records were taken at T0 (beginning of treatment) and T1 (end of functional phase). The airway was segmented into lower nasopharynx, velopharynx and oropharynx and analyzed for changes in partial volume, total volume, and minimum area using a CBCT software [NewTom 3GTM (Newtom- Cefla S.C., Verona, Italy)].
Results
The partial and total volumes were significantly larger at T1 than at T0 (p = .003, .001). In addition, minimum area also improved in each part of the airway (p = .005, .022, .001).
Conclusion
The Advansync2 fixed functional appliance can be used in Class II patients requiring improvement in their airway dimensions. However, additional long-term studies are recommended to confirm these findings.
Introduction
The pharyngeal airway is a vital structure in the human body, essential for multiple physiologic processes such as swallowing, vocalization, and respiration. Variations from the typical respiratory pattern, such as breathing through the mouth rather than the nose, can modify the posture of the head, jaw, and tongue, thus, a normal airway is critical for the healthy growth of craniofacial features. 1
Dr. Edward Angle was the first to conclude that children with skeletal Class II malocclusions had smaller airway dimensions and a higher risk of future respiratory problems such as snoring and obstructive sleep apnea (OSA) syndrome compared with those with skeletal Class I malocclusions. 2 Subsequent research has consistently supported the link between skeletal Class II malocclusion and pharyngeal airway constriction, increasing the risk of snoring and OSA.3–6
Comprehensive orthodontic treatment includes growth modification to improve not only esthetics but also function. 4 Several treatment modalities such as extractions, headgear, and Class II functional appliances can affect upper airway dimensions.7, 8 Previous studies5, 7–10 used cephalometric radiographs to assess the effects of different functional appliances (fixed and removable) on pharyngeal dimensions in growing skeletal Class II patients. However, the advent of cone beam computed tomography (CBCT) imaging has raised questions about the accuracy and usefulness of 2D cephalometrics compared with 3D CBCT imaging. CBCT imaging allows for three-dimensional visualization and analysis of airway structures with lower radiation exposure and greater spatial resolution compared with medical CT.
The AdvanSyncTM appliance, a modification of the Herbst appliance, offers advantages such as early use, no reliance on patient compliance, and improved comfort. However, no previous three-dimensional study has examined the effect of AdvanSyncTM on the pharyngeal airway. Therefore, this study aims to evaluate volumetric and dimensional changes in the pharyngeal airway using CBCT imaging after correcting mandibular retrognathism with an Advansync2 Class II corrector. The study also seeks to identify specific areas of the airway most affected by the appliance, potentially benefiting Class II patients with mandibular retrognathism and reducing the likelihood of future airway and breathing disorders.
Material and Methods
Study Design and Patient Criteria
This study was a single-center, prospective, observational study. Approval for the same was obtained from the Ethical Committee of the Institution (institutional ethics committee approval letter number ACDS/IEC/44/Nov 2019). The patients included in this study were those who reported to the Department of Orthodontics between January 2020 and May 2021, who required skeletal Class II correction by mandibular advancement. Prior informed consent was obtained from all subjects included on the basis of having Angle’s Class II malocclusion with retrognathic mandible (ANB ≥ 4°, overjet ≥ 4 mm), a positive Visual Treatment Objective (VTO), and aged between 10 and 17 years with CVMI (cervical maturity indicator) between C2 and C4. The exclusion criteria consisted of patients with prior orthodontic treatment or orthodontic extractions, functional appliance treatment, or patients with congenital anomalies/history of serious trauma/surgery of orofacial region. No sex differences were taken into account.
Null Hypothesis
“A fixed functional appliance such as the AdvanSync2 Class II corrector cannot increase the airway dimensions of subjects.”
Intervention
All enrolled patients were strapped up with 0.022” ×0.028” slot Damon Q™ or Damon 3MX™ (Ormco, Glendora, USA). An AdvanSyncTM2 Class II corrector (Ormco, Glendora, USA) was inserted in each patient after the initial leveling and alignment phase. The appliance consists of pre-fabricated crowns, which are cemented on the upper and lower first molars, which are then connected with the help of telescopic rods from upper to lower crowns. Wherever required, reactivation of the appliance was carried out to obtain the desired molar relation/overjet. The appliance was retained for a period of 6–8 months depending upon the severity of the malocclusion.
CBCT Image Acquisition and Data Collection
All CBCT images were taken using a NewTom 3GTM (Newtom- Cefla S.C., Verona, Italy) scanner in an erect posture, with teeth in maximum intercuspation and tongue in resting position. The images were then opened in the Newtom NNT software (Newtom- Cefla S.C., Verona, Italy) for assessment of pharyngeal airway dimensions such as volume of the segmented pharyngeal airway spaces, minimum area, etc.
Airway Segmentation and Analysis
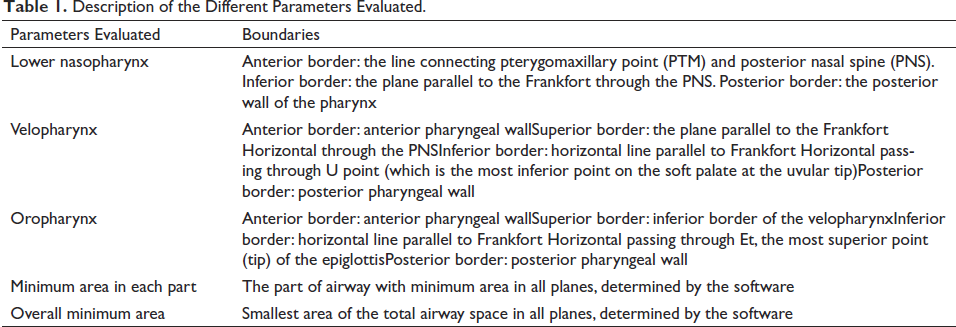
In their book titled “Cone Beam Computed Tomography in Orthodontics: Indications, Insights, and Innovations,” Kapila et al. described a method of airway segmentation into five distinct parts using six sagittal linear landmarks which we have followed. 11 These parts are lower nasopharynx, upper velopharynx, lower velopharynx, upper oropharynx, and lower oropharynx. We evaluated the pretreatment and post-functional CBCT images of each subject to derive information of volumetric change and minimum area of three parts (after combining upper and lower velopharynx and upper and lower oropharynx) as previously described by Isidor et al. 12 Details of the boundaries of the various parts of the airway are mentioned in Table 1 and Figure 1.
Description of the Different Parameters Evaluated.
Airway Segmentation into (a) Lower Nasopharynx; (b) Velopharynx; (c) Oropharynx.
Method Error and Statistical Analysis
The sample size was determined using GPower software. Effect size was calculated from data obtained from a previous study conducted by Entrenas et al. 13 The sample size derived from the calculations was 20. Statistical Package for Social Sciences (SPSS) software for Windows, Version 22.0 was used to perform the statistical analyses. Prior to assessing changes in pharyngeal airspaces pre and post treatment, airway segmentation was done twice by the same examiner 10 days apart and the measurements were subject to intra-examiner method error testing using the Dahlberg’s reliability test to assess for reproducibility of study measurements. Comparison of airway volumes and minimum area before and after treatment were analyzed using the paired t-test. Overall minimum constriction area and changes before and after treatment were determined using the independent t-test. The level of significance was set at p < .05.
Results
A total of 20 patients were included in the study after shortlisting potential patients for the relevant eligibility criteria. Since no sex differences were taken into account while setting the eligibility criteria, gender-based evaluation of subjects was not undertaken. The mean age of patients was 14.8 years with an average treatment time of 26 weeks.
Intra-operator Method Error
The calculation of the error of the method revealed that errors were small for all measurements. The coefficient of reliability was excellent for all measurements and no systematic error in measuring was detected.
Descriptive Statistics for Volume and Area
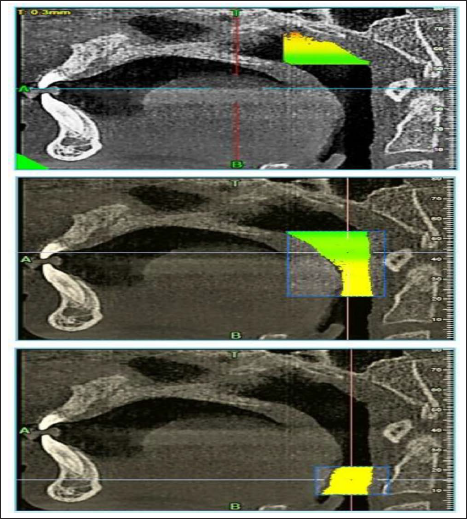
Mean volume of lower nasopharynx before and after treatment was 5.52 and 5.90 cm3, respectively, that of velopharynx was 6.42 and 7.45 cm3, and that of oropharynx was 6.38 and 7.25 cm3. Mean total volume before and after treatment was 18.32 and 20.6 cm3, respectively.
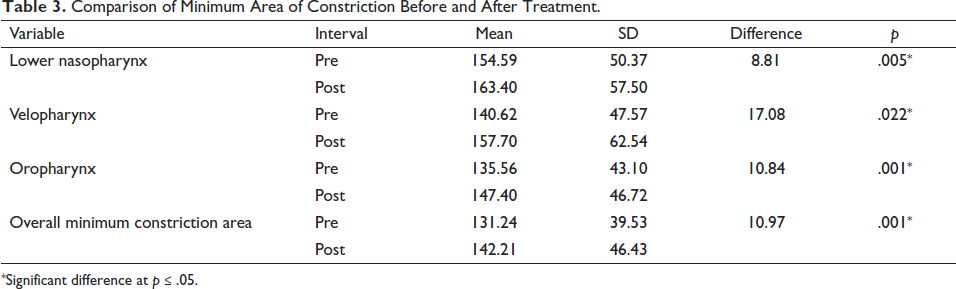
Average minimum area of lower nasopharynx before and after treatment was 154.59 and 163.40 mm2. Average minimum area of velopharynx before and after treatment was 140.62 and 157.70 mm2. Average minimum area of oropharynx before and after treatment was 135.56 and 147.40 mm2. Overall minimum constriction area before and after treatment was 131.24 and 142.21 mm2, respectively.
Comparison of Volume Before and After Treatment
Differences in volume in the lower nasopharynx before and after treatment were statistically significant (p = .003). Difference in volume in the velopharynx before and after treatment was also statistically significant (p = .003), as was difference in volume in the oropharynx before and after treatment (p = .001). Difference in total volume before and after treatment was found to be statistically significant as well (p = .001) (Table 2, Figure 2).
Comparison of Volume Before and After Treatment.
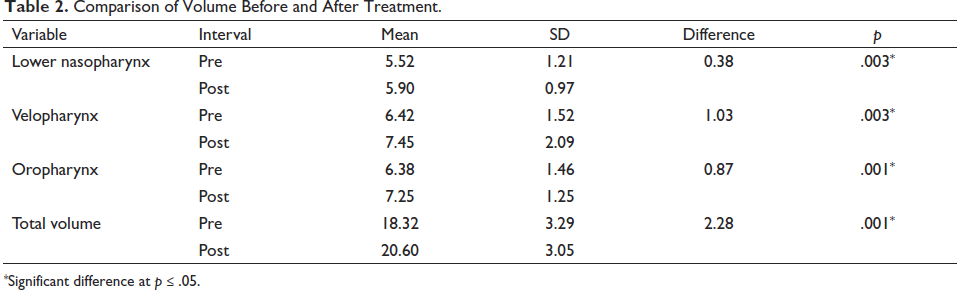
Box Plot Indicating the Change in Volume in Each Segment of Airway Before and After Treatment. LNP, Lower Nasopharynx; OP, Oropharynx; VP, Velopharynx.
Comparison of Minimum Area of Constriction Before and After Treatment
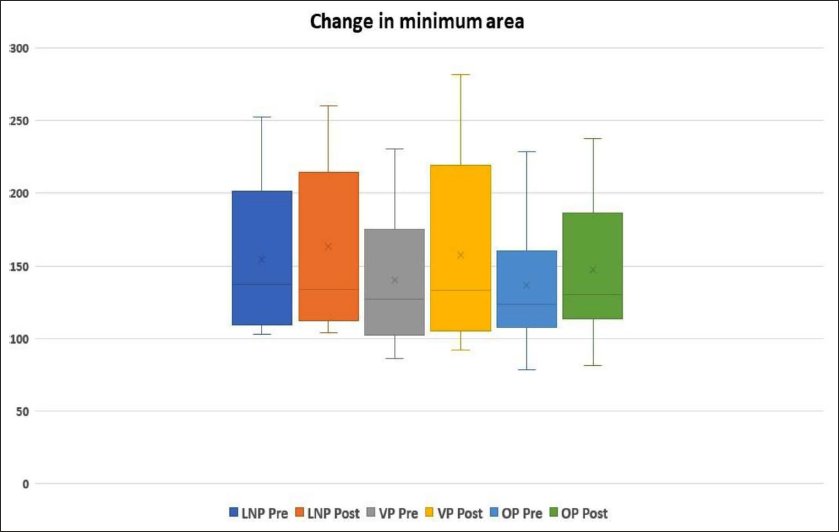
Difference in minimum area in lower nasopharynx before and after treatment was statistically significant (p = .005). Difference in minimum area in velopharynx before and after treatment was statistically significant (p = .022). The difference between minimum constriction area of the oropharynx before and after treatment was statistically significant (p = .001). Difference in overall minimum constriction area before and after treatment was statistically significant (p = .001) (Table 3, Figure 3).
Comparison of Minimum Area of Constriction Before and After Treatment.
Box Plot Indicating the Change in Minimum Area in Each Segment of Airway Before and After Treatment. LNP, Lower Nasopharynx; OP, Oropharynx; VP, Velopharynx.
Overall minimum constriction area before treatment in oropharynx and velopharynx was 149.12 and 113.37, respectively, and the difference between the two groups was significant (p = .039). Overall minimum constriction area after treatment in oropharynx and velopharynx was 162.46 and 121.96, respectively, and the difference between the two groups was significant (p = .048). Difference in overall minimum constriction area in oropharynx before and after treatment was 13.35 and difference in overall minimum constriction area in velopharynx before and after treatment was 8.59; however, difference between the two groups (oropharynx and velopharynx) was nonsignificant (p = .321) (Table 4).
Comparison of Total Minimum Constriction Area Between Oropharynx and Velopharynx.
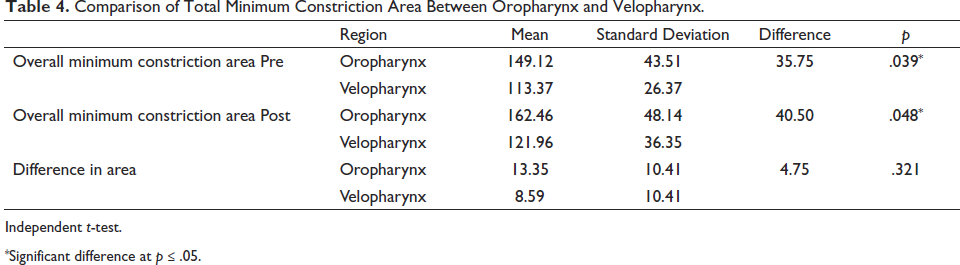
Independent t-test.
Discussion
The shape and dimensions of the pharyngeal airway vary with age, the condition of surrounding structures, and the position of the tongue. Scammon’s growth curve demonstrates that the lymphoid tissue grows to 200% of normal adult size around 10.45 years. 14 All subjects included in the current study were of a similar age range, with the mean age being 14.8 years with CVMI stage C4. This indicates relative stability of the airway and remaining growth potential for a fixed functional appliance to affect the advancement of the mandible. 15
Functional appliances are a time-tested and efficient method for correcting Class II malocclusion. They can be used for mandibular advancement in moderate and even some severe cases, reducing the need for orthognathic surgical procedures. Their effect on the maxilla and mandible has been widely studied in literature.16, 17 Regardless of their effect on skeletal structures, most studies assessing functional appliance effects on the airway concluded that there was a positive change, showing that indeed, functional appliances such as twin block, activator, MARA, and Forsus could help increase the airway space.12, 18–21
The goal of this CBCT study was to identify any increased airway benefit obtained from the use of an AdvanSync2 in the treatment of subjects with skeletal Class II malocclusions due to mandibular retrognathism. We selected an AdvanSync2 appliance, as it is widely used at present and has advantages over other fixed functional appliances such as superior design, concomitant use with fixed appliances from the beginning of the treatment, and better patient comfort. The idea behind the present investigation was that advancing the mandible using a functional appliance such as an AdvanSync2 could potentially increase the pharyngeal airway volume. By positioning the mandible or mandibular dento-alveolar structures forward, the associated musculature and soft tissue would be shifted forward as well, thus increasing the airway volume. With our results, the null hypothesis of the present investigation was rejected. Not only was the volume of the airway increased, but even the most constricted part of the airway also changed positively.
The lower nasopharynx, theoretically, is associated with structures such as the nose and maxilla. In several previous studies, this part of the airway has not been included for investigation with the reasoning that it is not influenced much by functional appliances.21–23 However, our results found positive changes in the lower nasopharynx not only in volume but also in minimum area. This creates scope for further investigation to strengthen the evidence that mandibular advancement can affect even the upper part of the pharyngeal airway.
The AdvanSync2 caused a statistically significant increase in volume for all three parts of the airway, with the maximum increase being in the velopharynx and the minimum increase in the lower nasopharynx. This was as per previous CBCT studies using the Herbst, 9 Forsus, 21 and other functional appliances. 12 One reason for increased airway volume after treatment with these appliances could be that the dentoalveolar modifications occurring after functional appliance therapy guided the tongue to a more forward position, indirectly enlarging the posterior airway space. A commonly employed surgical strategy for the treatment of OSA is the forward displacement of the tongue, which strengthens this particular line of reasoning. 12
We studied the area of minimum constriction in each part of the airway and the overall airway space, both of which increased post-treatment with the appliance. 3D assessment of the effect of a functional appliance on this parameter has only been investigated once before, to the best of our knowledge. 20 Previously, minimum area changes have been evaluated only in the sagittal dimension using lateral cephalometric radiography. This is a particularly important finding for subjects with constricted airways since an improvement in a restrictive point in the airway could hold greater significance than an overall increase in volume.
Strengths and Weaknesses
There is limited evidence describing the effects of the AdvanSync2 Class II corrector in literature.23, 24 Among the few published articles, none have discussed the effects of the appliance on the pharyngeal airway. The findings in our study are similar to the airway change findings in other investigations with other fixed functional appliances.
An increase in airway dimensions may not necessarily mean that it can cure OSA. OSA is studied in patients who are asleep and in a supine position, whereas our patients were awake and upright during the CBCT scanning. Apart from this, sleep apnea is a multifactorial disorder, largely related to BMI (body mass index) and neck circumference, 25 none of which was assessed in the present study.
Treatment effects in growing patients can be evaluated by comparing treatment outcomes with a matched control group. 26 However, having an age-matched control group could raise ethical concerns, as many skeletal Class II subjects would be left untreated for a long time and exposed to ionizing radiation.12, 27 Therefore, there were no control groups and no scope for randomization in the present study. This can be addressed in future studies.
Another limitation of our study is that only short-term effects of the appliance were studied. Systematic reviews claim that the effects of fixed functional appliances on dento-skeletal structures are not stable in the long term, which may affect the pharyngeal airway space as well.28–30 To verify if our study findings remain stable with time, investigations with a long-term follow-up may be considered in the future.
Conclusion
The most constricted pre-treatment area lies in the oropharynx.
Volume of the lower nasopharynx, velopharynx, and oropharynx increases upon correction of mandibular retrognathism using an AdvanSync2 Class II corrector. This may aid in prevention/treatment of OSA and other respiratory problems.
Along with volume, areas of minimum constriction in each part of the pharyngeal airway also increase in dimension, indicating a change in shape of the pharyngeal airway.
The maximum effect of the appliance with regard to an increase in constriction area is on the velopharynx, followed by the oropharynx.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval was obtained from Institutional Ethics Committee (letter number ACDS/IEC/44/Nov 2019).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.