
Abstract
Excessive gingival display (EGD), often termed a “gummy smile,” can negatively impact facial esthetics and patient confidence. Among the various etiologies, hyperactive upper lip movement is frequently encountered in patients with otherwise normal skeletal and dental parameters. While conventional lip repositioning techniques offer a minimally invasive approach to managing EGD, relapse due to persistent elevator muscle activity remains a major limitation. This case report presents a modified lip repositioning technique with modified muscle anchoring sutures to enhance treatment stability and long-term esthetic outcomes. A 32-year-old female patient presented with approximately 5 mm of gingival display upon full smile, attributed to upper lip hypermobility. A partial-thickness epithelial strip was excised from the maxillary vestibular mucosa, extending between the right and left premolar. In addition to standard mucosal advancement, vertical mattress sutures were strategically placed to engage and tack down the levator labii superioris and orbicularis oris muscles. This anchoring limited the upward traction of the upper lip during dynamic movements. The patient was monitored after surgery at 1 week, 1 month, and 6 months. Healing progressed without complications, and the reduction in gingival display remained consistently below 1.5 mm. The patient expressed a high level of satisfaction, experienced minimal discomfort, and showed no evidence of relapse.
Introduction
Excessive gingival display (EGD), commonly known as a gummy smile, is an esthetic concern that affects a notable portion of the population, particularly young adults, impacting self-confidence and social interactions.1, 2 EGD may result from various etiologies, including skeletal discrepancies like vertical maxillary excess, dentoalveolar extrusion, altered passive eruption, or hyperactivity of the upper lip elevator muscles.3, 4 Among these, hypermobile upper lip movement is a frequent soft tissue cause of excessive gingival exposure during smiling. 5
Management of EGD is often challenging due to the multifactorial nature of the condition. While orthognathic surgery remains the definitive treatment for skeletal-related gummy smiles, it is invasive and associated with longer recovery periods, making it less desirable for many patients.6, 7 Conservative approaches such as botulinum toxin injections provide temporary muscle relaxation but require repeated treatments. 8 Traditional lip repositioning surgery offers a less invasive option by limiting the superior movement of the upper lip; however, postoperative relapse due to persistent elevator muscle activity is a significant limitation.9, 10
With the rising demand for minimally invasive, stable, and predictable esthetic interventions, there is an unmet need for techniques that address muscle hyperactivity while maintaining long-term outcomes. 11 This case report presents a novel modification of the lip repositioning procedure that incorporates modified muscle anchoring sutures targeting the levator labii superioris and orbicularis oris muscles. By directly limiting elevator muscle pull, this modification aims to enhance surgical stability and reduce the risk of relapse, providing a practical and patient-friendly alternative for managing gummy smiles caused by upper lip hypermobility.12, 13
Methodology
This case report describes the surgical management of EGD using a modified lip repositioning technique with modified muscle anchoring sutures.
Gingival display was measured clinically using a periodontal probe during both spontaneous and posed full smiles, and the findings were confirmed with standardized frontal smile photographs taken under consistent head positioning. EGD was diagnosed when gingival exposure exceeded 3 mm during a full smile. The severity of gingival display was categorized according to the Garber and Salama classification, with mild (2–4 mm), moderate (4–6 mm), and severe (>6 mm) gingival exposure. 6 Skeletal causes such as vertical maxillary excess were excluded through cephalometric analysis and clinical profile evaluation, while altered passive eruption was ruled out via periodontal probing and assessment of the gingival margin.
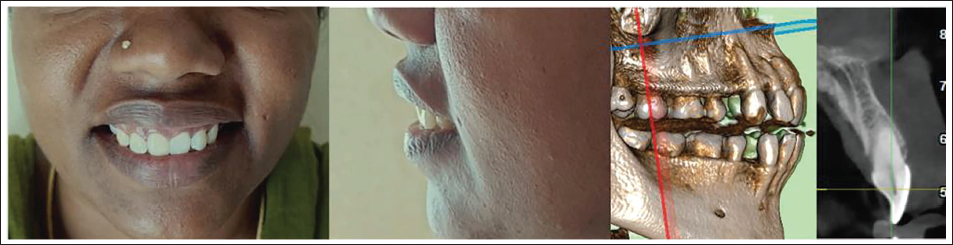
Dynamic smile analysis revealed an upper lip excursion of approximately 5 mm from rest to full smile, confirming hypermobility as the primary etiologic factor. The upper lip length (subnasale to stomion superius) was 20 mm, which falls within the normal female range of 20–22 mm, further supporting that the EGD was primarily due to hypermobility rather than shortened lip length (Figures 1 and 2A).
Preoperative Assessment of Gummy Smile Using Frontal Photographs and Preoperative Radiographs.
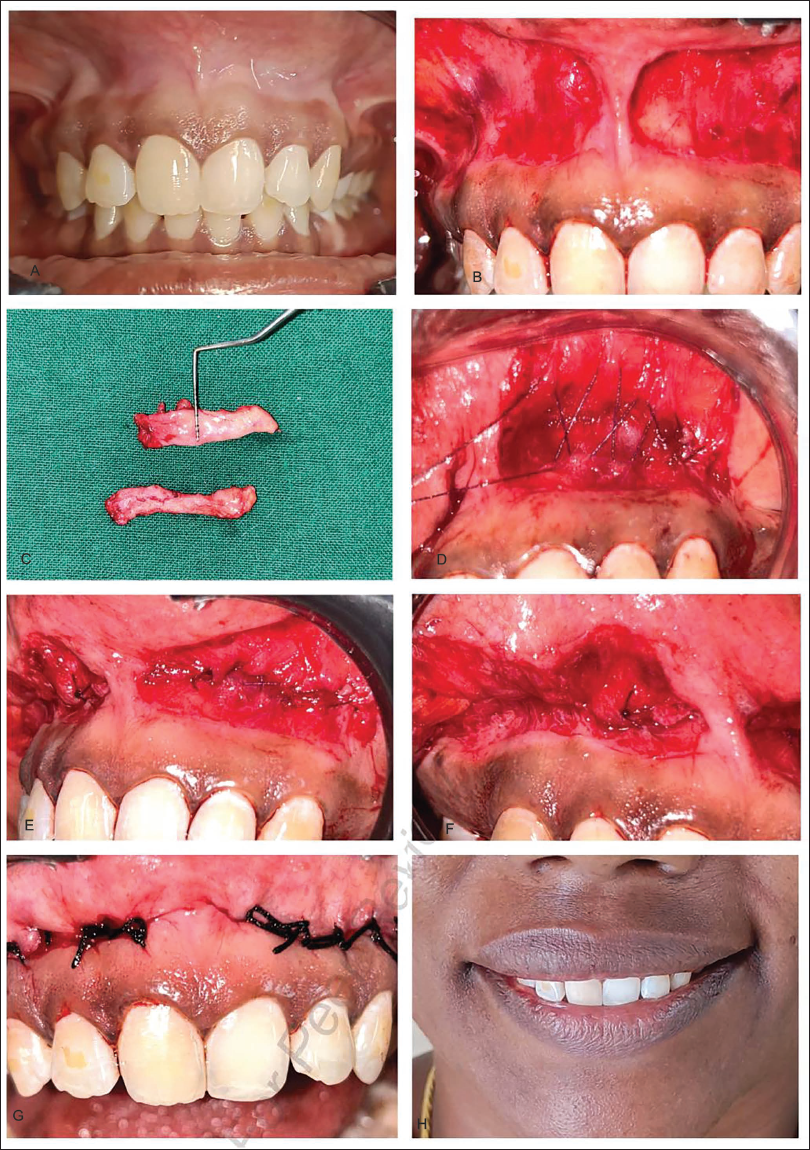
(A) Preoperative Intraoral Picture. (B) Initial Incision. (C) Excised Excessive Tissue. (D–F) Muscle Anchoring Suture Using 5*0 Vicryl. (G) Primary Closure Using 3*0 Silk. (H) Postoperative Image After 14 Days.
The procedure was performed under aseptic conditions with the patient seated in a dental chair and local infiltration anesthesia administered in the maxillary vestibular area from the right first premolar to the left first premolar.
A partial-thickness elliptical strip of mucosa approximately 10–12 mm wide was carefully excised from the labial vestibule, extending horizontally from the distal aspect of tooth #14 to tooth #24 (Figure 2B). The underlying connective tissue and muscles were preserved to maintain vascular supply (Figure 2C).
In contrast to conventional lip repositioning, where relapse often occurs due to continued elevator muscle pull, this modified approach incorporates modified muscle anchoring sutures. The sutures were placed at a depth engaging the superficial fibers of the levator labii superioris and orbicularis oris and secured to the maxillary periosteum, thereby reducing upward traction. This modification directly addresses the limitation of the traditional technique, where muscle activity is left unaltered.
To enhance stability and minimize relapse, anchoring sutures were placed using 5*0 Vicryl suture to tether the elevator muscles of the upper lip—specifically, the levator labii superioris and orbicularis oris—to the periosteum of the underlying maxilla. These muscle anchoring sutures acted as a physical restraint, limiting excessive lip elevation during smiling (Figure 2D).
Vertical mattress sutures were oriented perpendicular to the direction of muscle pull, engaging superficial fibers of the levator labii superioris and orbicularis oris, and anchored to the maxillary periosteum at a depth of approximately 2–3 mm. This provided effective restraint without compromising vascularity (Figure 2E and 2F).
After the muscle anchoring suture, the lip mucosa was repositioned apically to the mucogingival junction and secured with interrupted non-resorbable sutures (3-0 silk).
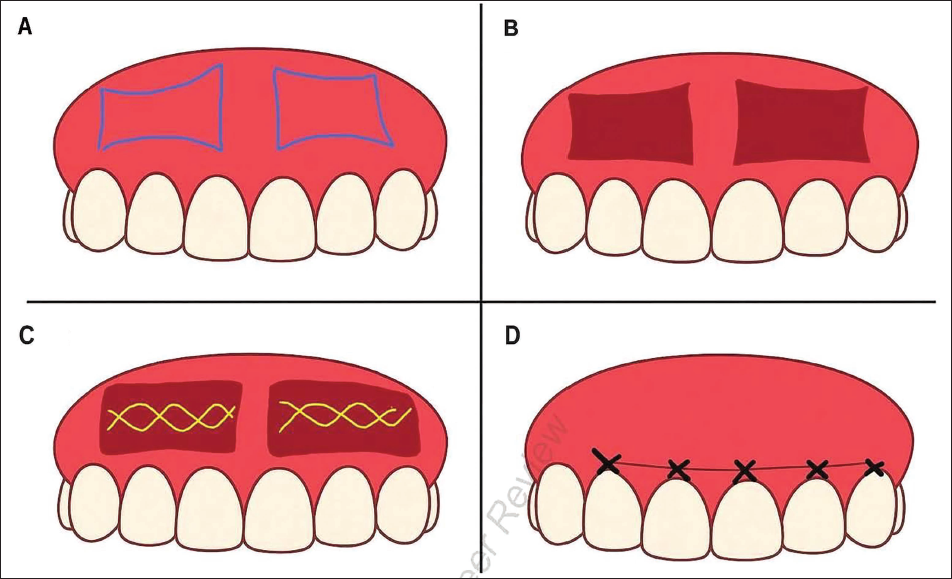
A schematic illustration has been added (Figure 3) to clarify the modified lip repositioning technique with modified muscle anchoring sutures.
Schematic Representation of the Modified Technique. (A) Initial Excessive Gingival Display. (B) Post Removal of Tissues. (C) Modified Muscle Anchoring Suture, Crisscross Type Individual Suture Extending from Premolars. Using 5*0 Vicryl Suture -Yellow Marked. (D) Final Suture for Closure of the Flap Using 3*0 Silk Suture.
Postoperative instructions included limited lip movement and maintenance of oral hygiene with chlorhexidine rinses. The patient was monitored at intervals of 1 week, 1 month, 3 months, and 6 months to assess healing, gingival display, and functional outcomes.
Results
The patient tolerated the surgical procedure well, and immediate postoperative healing was uneventful. Mild edema was observed during the first postoperative week, which subsided without intervention. At 1-week follow-up, the surgical site demonstrated satisfactory healing with no signs of infection or dehiscence.
By 1 month, the mucosa appeared well-adapted, and scar formation was minimal. The gingival display on a full smile was reduced from approximately 5 mm preoperatively to 1.5 mm, representing a stable reduction of nearly 70%.
At 3 months, the gingival display remained within esthetically acceptable limits, and the patient reported no discomfort, functional limitation, or speech alteration. Smile esthetics were subjectively evaluated by the patient as “highly satisfactory.”
At 6 months, the surgical site exhibited normal mucosal color and contour, with no fibrosis or scarring evident clinically. Gingival display remained stable at ≤1.5 mm, and no recurrence of excessive display was observed. Lip mobility during smiling and speaking was preserved, with no restriction in function.
Overall, the modified lip repositioning technique with muscle anchoring resulted in stable esthetic improvement, uneventful healing, and high patient satisfaction over the 6-month observation period.
Discussion
EGD due to hyperactive upper lip muscles presents a unique challenge in esthetic dentistry. Traditional lip repositioning surgeries have been widely accepted as a conservative approach, offering a simple and minimally invasive method to reduce gingival exposure by limiting lip elevation. 14 However, one of the major drawbacks of this technique is postoperative relapse, commonly caused by the persistent pull of the elevator muscles, such as the levator labii superioris and orbicularis oris. 15
The primary drawback of conventional lip repositioning is postoperative relapse caused by persistent elevator muscle activity. By introducing muscle anchoring, this modification reduces the chance of recurrence by biomechanically restraining the lip elevator pull. Thus, while traditional surgery offers temporary esthetic benefit, the modified technique enhances long-term stability.
The modified lip repositioning technique described in this case addresses this limitation by incorporating modified muscle anchoring sutures. These sutures effectively tack down the hyperactive muscles, thereby reducing their upward traction on the lip during smiling and speaking. This approach leverages the biomechanical principle of muscle restraint to enhance the stability of surgical outcomes. 16
Compared to other treatment modalities such as botulinum toxin injections, which require repeated applications and may have variable efficacy, or orthognathic surgery, which is invasive and associated with longer recovery times, this technique offers a balanced alternative that is both minimally invasive and long-lasting.17, 18 The use of resorbable sutures for muscle anchoring avoids the need for secondary procedures and reduces patient morbidity. 19
In the present case, the patient exhibited a significant and stable reduction in gingival display over a 6-month follow-up period with high satisfaction and no evidence of relapse or functional impairment. This supports the hypothesis that muscle anchoring can effectively mitigate one of the primary causes of relapse in lip repositioning surgery. 20
Healing was uneventful, with resolution of edema by the first postoperative week and satisfactory mucosal adaptation noted at one month. By three months, the mucosa appeared well-integrated, with no fibrosis, scar contracture, or impaired mobility. The surgical site remained stable with harmonious smile esthetics throughout the six-month follow-up. Recurrence was specifically evaluated up to 6 months postoperatively, and no signs of relapse were observed during this follow-up period.
Potential complications of this approach include fibrosis, excessive scarring, restricted smile dynamics, or speech alteration. Although not observed in the present case, these possibilities should be considered, particularly in patients with high muscle activity or thin mucosa.
The modified lip repositioning technique with muscle anchoring sutures offers a novel, minimally invasive, and effective approach to managing EGD due to hyperactive upper lip muscles. By directly limiting the elevator muscle pull, this method enhances the stability of the surgical outcome, reducing the risk of relapse commonly seen with traditional procedures.12, 13 The positive clinical results and patient satisfaction observed in this case highlight its potential as a practical alternative to more invasive or temporary treatments. Further studies with larger sample sizes and longer follow-up are warranted to validate these findings and establish standardized protocols.19, 20
Shortcomings of the Modified Lip Repositioning Technique with Muscle Anchoring Sutures
Despite the favorable short-term outcomes observed, this modified approach carries certain shortcomings. The risk of relapse cannot be completely eliminated, particularly after resorption of sutures if fibrotic stabilization is inadequate. Over-anchoring of muscles may restrict natural smile dynamics, and in patients with thin mucosa, fibrosis or scarring may be more pronounced. The technique is operator-sensitive, requiring accurate placement of anchoring sutures to avoid asymmetry or functional restriction. Moreover, the present report is limited to a single case with a 6-month follow-up; larger clinical trials with longer observation periods are necessary to establish the long-term predictability and generalizability of this method. Finally, this technique may not be suitable for EGD of skeletal or dentoalveolar origin, where orthognathic or restorative approaches remain essential.
Conclusion
The modified lip repositioning with muscle anchoring sutures achieved a stable reduction in gingival display over 6 months with high patient satisfaction. While the technique may carry risks such as scarring or altered mobility, none were encountered in this case. This modification represents a minimally invasive and predictable approach to managing gummy smiles caused by upper lip hypermobility.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The institutional review board exempted the study from ethical approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written consent form obtained from the patient.