
Abstract
Skeletal class II malocclusion in adult patients with severe gummy smile is challenging for orthodontist and often requires surgical intervention. The difficulty increases when patients refuse orthognathic surgery, and orthodontists have limited treatment alternatives. This report describes the case of a patient with severe dento-skeletal class II malocclusion with excessive gingival display while smiling. The patient was treated with temporary anchorage devices, and an innovative method of lip repositioning was devised to correct the irregularity.
Introduction
The most common reasons for approaching an orthodontist involve malocclusion or other esthetic concerns. Malocclusions can occur owing to dental or skeletal conditions or a combination of both. The class II division I malocclusion not only causes esthetic and functional problems but also results in psychological disturbances. One of the classical features associated with the class II division I malocclusion is excessive gingival display (EGD) while smiling. 1
A “perfect smile” is an interaction among the teeth, lip framework, and gingival scaffold. In an ideal smile esthetic zone, the teeth should be well aligned and gingival margins should be healthy and harmonious. 2
Excessive gingival display, commonly described as “gummy smile,” adversely affects smile esthetics and is, therefore, undesirable. 3 The etiology of EGD can be attributed to diverse causes such as vertical maxillary excess (VME), gingival enlargement, a short upper lip length, or a combination of the mentioned determinants. 4
A short upper lip is one of the primary causes of gummy smile due to neuromuscular anomalies. A lip without dentoalveolar deformity and mobility more than 8 mm is considered hyperactive. 5 The muscles responsible for upper lip elevation include levator labii superioris (LLS), levator labii superioris alaeque nasi, levator anguli oris, zygomaticus major (Zma), zygomaticus minor (Zmi),depressor septi nasi, and andrisorius. Different treatment options, including botulinum toxin type A (BTX-A) injection, hyaluronic injection, lip repositioning, myectomy or combinations of them, which are mainly focused on restricting the movement of muscles, are available.6, 7
Traditionally, dentoalveolar extrusion and VME can be corrected effectively using invasive orthognathic surgery alone. However, temporary anchorage devices (TADs) have widened the spectrum of orthodontics and are also very well accepted by patients. It is necessary to diagnose the etiology associated with gummy smile to prescribe the appropriate treatment modalities. Lip repositioning along with fixed orthodontic therapy offers an excellent alternative to orthognathic surgery.
This report describes the case of a severe dento-skeletal class II malocclusion in a patient with EGD while smiling. The patient was treated using TADs and an innovative method of lip repositioning.
Case Report
A 16-year-old male patient presented with the chief complaint of forward placement of the upper teeth and a gummy smile.
Diagnosis and Etiology
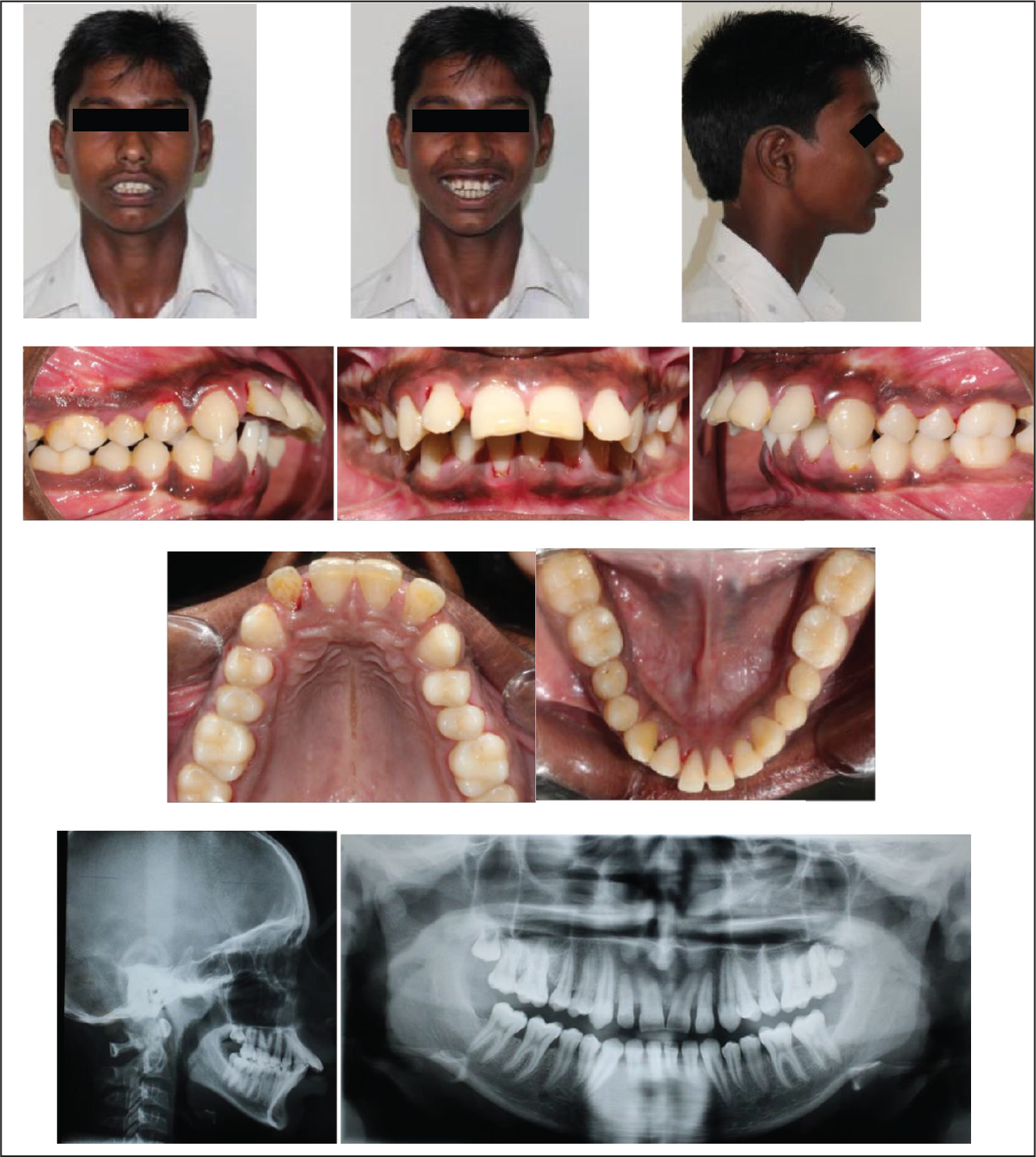
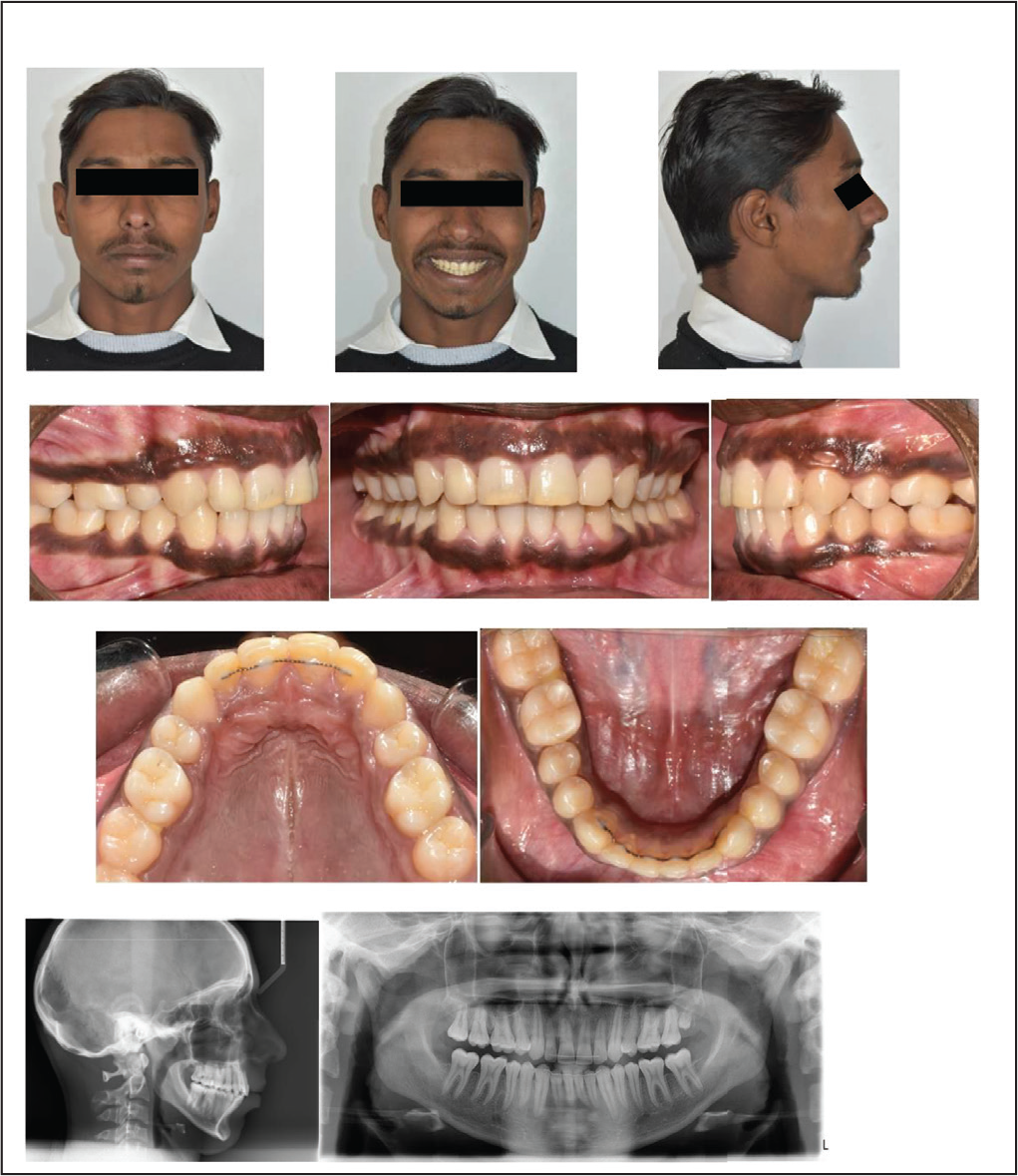
Extraoral examination indicated that the patient had mesocephalic, mesoprosopic, and a convex facial profile with no gross asymmetry. The patient potentially had incompetent lips and increased clinical Frankfort-mandibular plane angle (FMA). A complete exposure of the incisors with an excessive display of gums while smiling was observed. An examination of the temporomandibular joint (TMJ) revealed no clicking sounds. There was no relevant medical or dental history. An intraoral examination revealed that the patient had a class II molar relationship on the right side, End on molar relationship on the left side with spacing between 12, 13, 22, 23, 31, 32, and 41. The upper dental midline shifted 2 mm toward the left with respect to the facial mid-line. The upper incisors were severely proclined with a short upper lip. The maxillary and mandibular arches were U-shaped. Bolton analysis revealed 1.2 mm of the mandibular anterior tooth material excess.
Evaluation of orthopantomograms revealed the presence of all permanent teeth except 38 and 48. TMJ revealed normal size, shape, and position of the condylar heads. The height of the inter-dental crest was normal. Eruption of teeth 18 and 28 were also observed. Examination of the cephalogram indicated an Sella-Nasion-Point A (SNA) of 85°, Sella-Nasion-Point B (SNB) of 76°, and Y-axis of 72°, suggestive of skeletal class II due to maxillary prognathism and mandibular retrognathism with a vertical growth pattern.
Based on the clinical findings and cephalometric values, the patient’s condition was diagnosed as skeletal class II malocclusion, hyperdivergent growth pattern, convex soft tissue facial profile, and a short upper lip with severe gummy smile (Figure 1; Table 1).
Pretreatment Records.
Pretreatment, Posttreatment, and 1-Year Follow-up Cephalometric Values.
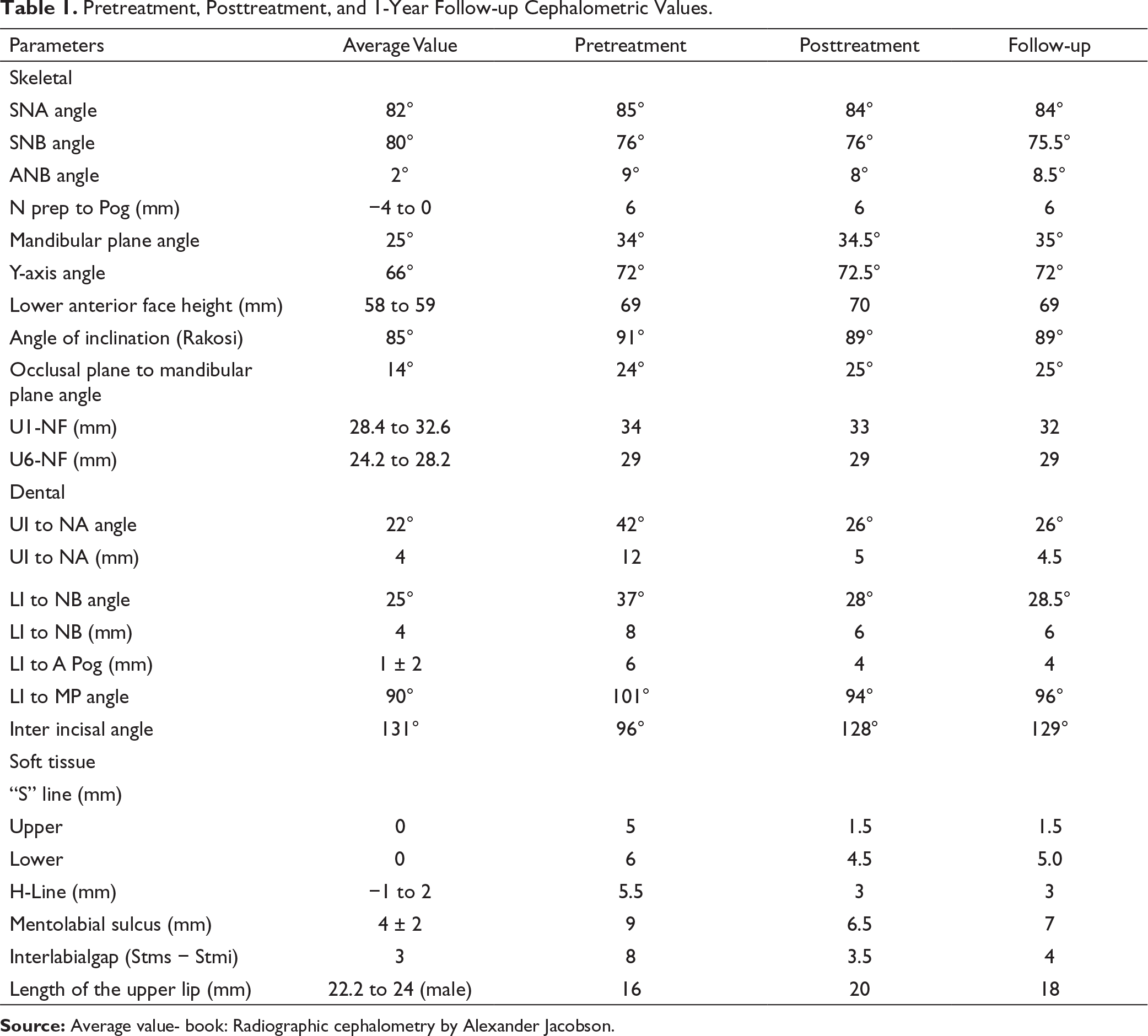
Source: Average value- book: Radiographic cephalometry by Alexander Jacobson.
Treatment Objectives
To maintain class II molar relationship.
To achieve class I canine relationship.
To achieve ideal overjet and overbite.
To improve smile and lip competency.
To achieve an esthetic soft tissue profile.
Treatment Options and Plan
The treatment plan offered to the patient included the following:
LeFort I osteotomy followed by superior repositioning of the maxilla and bilateral sagittal split osteotomy for advancement of the mandible with genioplasty after dental decompensation. As the patient had a minimal curve of Spee without crowding in the lower arch, we decided to camouflage the skeletal discrepancy by extracting teeth 14 and 24 along with a lip lengthening surgery to address the patient’s chief concern of gummy smile.
The patient refused the first treatment modality owing to the involvement of an invasive surgical procedure.
Treatment Progress
A preadjusted edgewise appliance with McLaughlin-Bennett-Trevesi (MBT) prescription metal brackets (0.022 × 0.028-inchslot 3M UnitekTM Gemini Metal, USA) was placed following extraction of teeth 14 and 24. An initial 0.014-inch nickel–titanium (3M Unitek Nitinol Super Elastic, USA) arch wire was placed for leveling and aligning the upper and lower arches. The lower arch was bonded 3 months later. Alignment and leveling were achieved with the use of the continuous archwire in the following sequence: 0.014” NiTi, 0.016” NiTi, 0.017” × 0.025” NiTi. Eventually, a thicker gauge wire (0.017” × 0.025”) of stainless steel was employed in the upper and lower arches over a period of 9 months. The elastomeric chain (intermediate linked) was used in the upper anterior region to close the spacing between 12, 13, 22, and 23, and it was replaced every month. All anterior spacings were closed within a time span of 3 months.
As treatment progressed, a heavier arch wire (0.019″ × 0.025″) of stainless steel with a crimpable power arm (8 mm) was placed between the lateral incisor and the canine in the upper arch. Since the anchorage requirement was Group A (≥75% of the extraction space needed for anterior retraction) in the upper arch, self-drilling stainless steel mini implants (1.5 × 8 mm; SK Surgical, Pune, Maharashtra, India) were placed bilaterally. Implants were loaded immediately using an elastomeric chain with an appropriate force of 150 g on each side to retract the anterior segment. The elastomeric chain was changed every 5 weeks until the extraction spaces were closed completely. After 18 months of active treatment (Figure 2), the patient was referred to the Department of Periodontology for the lip lengthening procedure (Figure 3).
Mid-treatment Records.

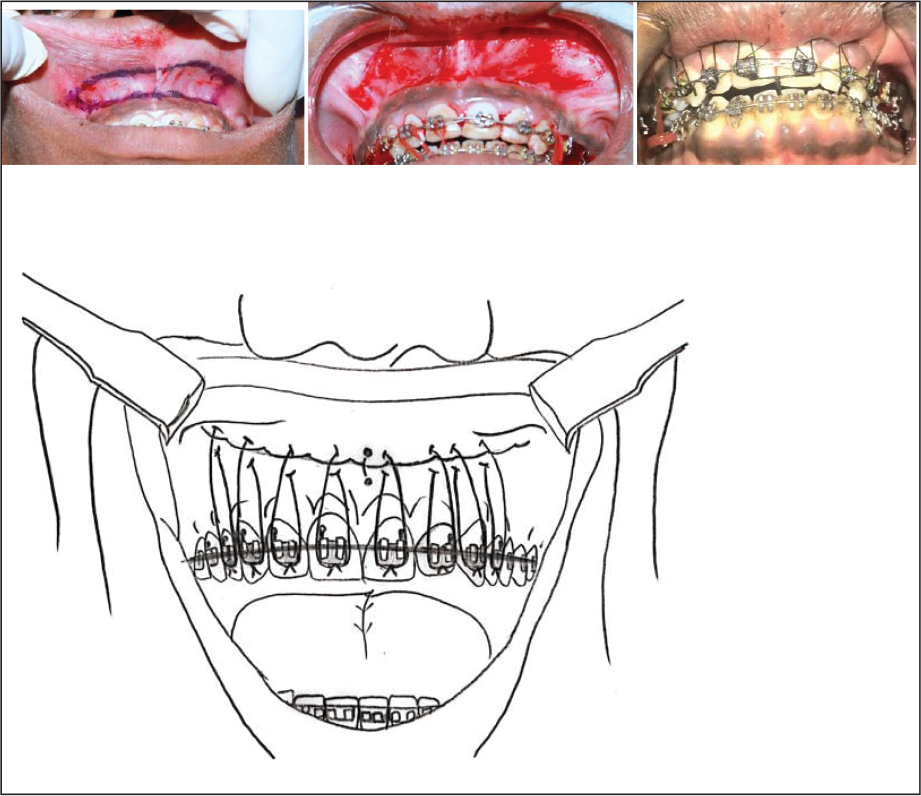
Lip Repositioning Surgery.
After the lip lengthening procedure and 3 months of finishing and detailing, a bilateral class I canine relationship and an ideal overjet and overbite with pleasing soft tissue profile were achieved. Fixed retainers were employed on the upper and the lower arches along with the Begg retainer for retention. The total treatment time was 23 months (Figure 4).
Innovative Surgery for Lip Lengthening
The area to be removed was first marked using a surgical marking pencil in the vestibular region of the alveolar mucosa in an elliptical form extending from the mucogingival junction to 12 mm apically and expanding to the distal end of the first premolar region. This step was performed prior to the administration of local anesthesia, as these points provide correct realignment of the area to be excised. Under local anesthesia (lignocaine 2% with epinephrine 1:80,000), a partial thickness incision was made in the previously marked areas, exposing the underlying connective tissue. The apical mucosa was first approximated at the midline to reduce the vestibular depth and then sutured at the mucogingival junction using 6-0 sutures. Suturing was first performed by penetrating through the mucogingival junction, and then anchorage was taken from the respective brackets to ensure minimal relapse during the healing phase. The sutures were placed in all areas where incisions were made, finally closing the incisions. The patient received nonsteroidal anti-inflammatory drugs (NSAIDs) for 7 days along with antimicrobial rinses. Postoperative care was explained to the patient with suggestions on minimizing lip movement for 4 weeks. Follow-up evaluations were conducted 10 days, 1 month, 6 months, and 1 year after the treatment.
This modification helped retain the upper lip position during the healing period and enabled enhanced vertical control over conventional methods (Figure 3).
Results
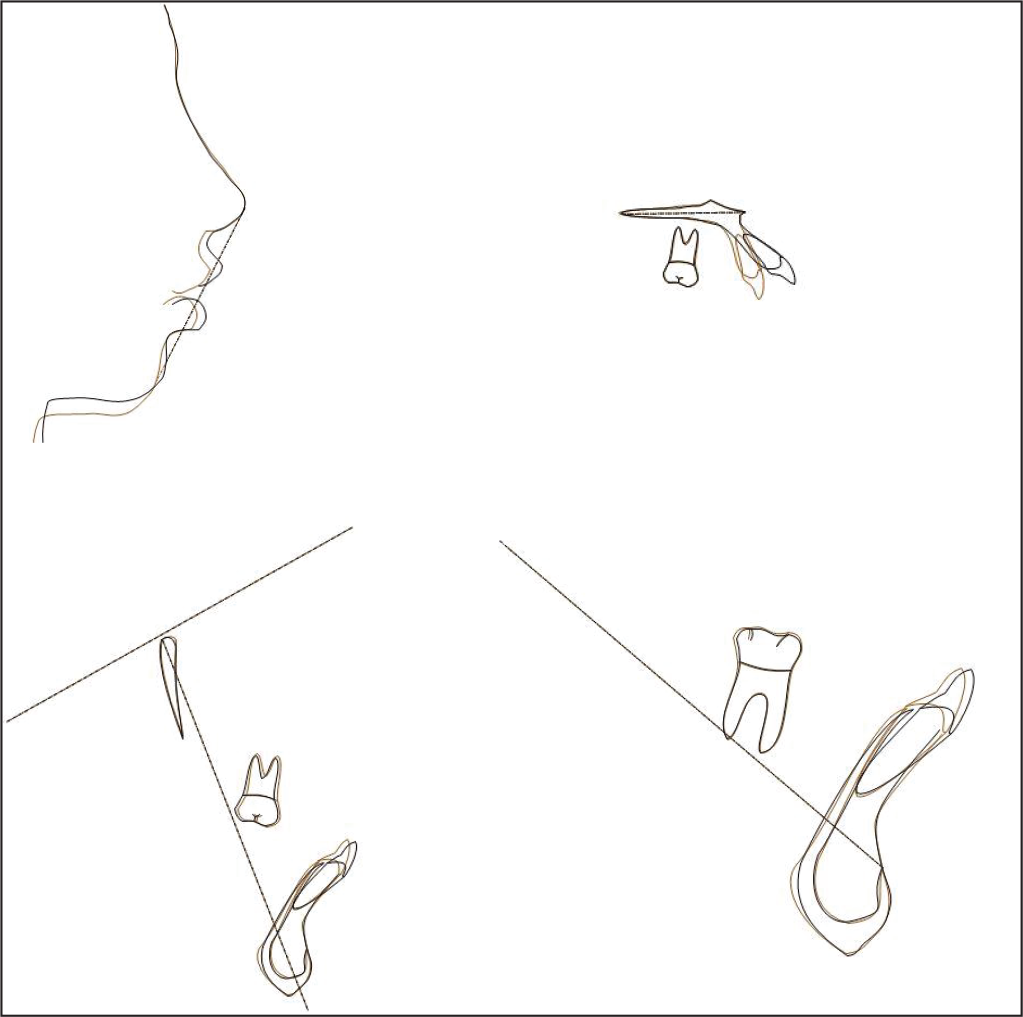
The treatment protocol resulted in a remarkable improvement in gummy smile, soft tissue facial profile, and upper lip length. The patient had competent lips with 3 to 4 mm of gingival exposure while smiling. A consonant smile was obtained at the end of the treatment. A bilateral class I canine relationship was achieved with optimal overjet and overbite. Posttreatment cephalometric tracing revealed significant improvement in the inclination of the maxillary and mandibular incisors (upper incisor to NA angle, pretreatment 42° and posttreatment 26°; IMPA, pretreatment 101° and posttreatment 94°; Table 1). The panoramic radiograph showed good root parallelism. Clinical examination of the masticatory muscles and TMJs did not show any pathological signs or symptoms upon completion of the treatment. Superimposition also showed that maxillary and mandibular incisor retraction with improvement in the soft tissue facial profile (Figure 5).
Posttreatment Records.

A 1-year follow-up record after lip lengthening surgery showed stable inter–arch relationships with a pleasing smile (Figure 6).
Discussion
Orthognathic surgery is the ideal treatment against severe skeletal discrepancy in adult patients. However, in many societies, surgery is only pursued when there is a life threatening condition and is generally not favored for esthetic or functional reasons. 8 In the context of dental problems, an auxiliary option to surgery includes camouflage with extraction of all first premolars or 2 maxillary premolars.
Superimposition of Pre- and Posttreatment Lateral Cephalogram (Pre—Black; Post—Red).
One year Follow-up of Lip Lengthening Procedure and 6-Month Post Debonding.
In this case, the patient was subjected to camouflage with extraction of teeth 14 and 24 and minimally invasive surgical procedures. Lip lengthening was performed with an innovative approach to prevent relapse.
The correct evaluation of the etiology of EGD is important for determining treatment recommendations. The lip lengthening technique to decrease gummy smile is a simple surgical procedure and was designed to be less aggressive and to have fewer postoperative complications than orthognathic surgery. 9
The lip repositioning procedure was first described in 1973 by Rubinstein and Kostianovsky as part of a plastic surgery. Later, it was introduced in dentistry, after being modified in 2006 by Rosenblatt and Simon. The etiology of EGD is variable, including extraoral or oral components. 10
Conventional lip repositioning surgery is a safe technique with minimal side effects. Following this procedure, several modifications have been suggested with myotomy by various authors.11, 12 Litton and Fournier advocated this procedure for the correction of EGD in the presence of a short upper lip by detaching the muscles from the bony structures to the coronal position of the upper lip, and no complications were reported. Miskinyar described a technique in which he performed a myectomy and partial amputation of the LLS muscle. Alammar et al reported that the modified technique utilized in treating gummy smile results in less relapse and shows excellent esthetics than the conventional technique. In addition, modified lip repositioning with myotomy or myectomy is a more aggressive procedure and has been shown to cause irreversible morbidity in some patients postoperatively (paresthesia).13-15
In this case, a modification of the conventional lip lengthening technique was performed with placement of sutures using the respective brackets as anchorages to ensure minimal relapse during healing. The advantages of this innovative procedure are as follows:
Less aggressive than the conventional technique; more conducive to the patient; less pain; and fewer chances of relapse owing to the continuous pull being exerted by the fixed brackets during the healing process.
The disadvantages of this innovative procedure are as follows:
Patient might experience slight discomfort due to the constant pull. The maintenance of oral hygiene is a challenge, as the patient would have orthodontic brackets, which could be overcome by judicious use of interdental brushes and mouthwashes.
Earlier studies reported that relapse could occur after various lip lengthening procedures within 6 months. It could also lead to a complete relapse of the procedure.16-18 In this case, minimal relapse was observed during the 1-year follow-up investigation, and the patient maintained lip competency (Table 1). The fewer chances of relapse were owing to the continuous pull being exerted by the fixed brackets during the healing process, and the procedure being less aggressive than the conventional technique.
The treatment of gummy smile can also be performed with crown lengthening procedures (gingivectomy). The length of the clinical crown was adequate, with no gingival enlargement. However, owing to the presence of a short upper lip, the lip lengthening procedure was considered instead of crown lengthening.19-21
Necessary care was taken to attain an ideal dental relationship. Anchorage control is a key factor in orthodontic treatment. Although extraoral anchorage could be used to supplement tooth borne anchorage, lack of cooperation with extraoral appliances could result in anchor loss and poor treatment results. As a substitute for endosseous implants, miniplates, miniimplants, and screws were used as orthodontic anchorages. The advantages of using TADs were as follows:
Provide absolute anchorage to retract maxillary anterior segment and enable simultaneous retraction and intrusion.
Conclusion
Correct diagnosis is very important for patients with gummy smile to decide on the appropriate treatment plan.
Temporary anchorage devices have widened the scope of camouflage treatment in severe skeletal cases.
The modified lip lengthening procedure enables greater vertical control over conventional methods and helps retain the lip in the desired position. A randomized clinical trial is needed in this direction to determine the efficacy of this innovative technique.
Statement of Informed Consent:Written informed consent was obtained from the subject for the use of photographs
for publication.