
Abstract
Background:
Pandemics uniquely burden family caregivers as they navigate their own health, and that of their care recipients. While the impact of COVID-19 on caregiver well-being is known, there is little information on its impact on caregiver roles and responsibilities, and how caregivers adapted.
Methods:
We used a cross-sectional survey design with a non-probabilistic sample. Our survey anonymously assessed the impact of COVID-19 on caregiving roles, responsibilities, and well-being, and was distributed between April and December 2020. Logistical regression was used to model associations between caregiving experiences and well-being. Free-text fields illustrated quantitative data.
Results:
Respondents (n = 264) were white (80.7%), women (87.1%), and 51.7 years; 72% cared for high-risk conditions. On average, caregivers participated in 8.9 ± 4.5 caregiving tasks and took 4.3 ± 2.0 precautions, especially physical distancing (95.8%) and using protective measures (96.2%). Caregivers worried about not receiving timely help (61.7%), medical attention (55.3%), and medications (41.3%). Caregivers reported increased caregiving responsibilities (61.7%) and time with care recipient (39.4%). The former was associated with higher depression, anxiety, and caregiver burden while the latter was associated with higher caregiver burden.
Conclusions:
These insights from the early days of COVID-19 can help policy makers prepare for future pandemics and other natural disasters.
Introduction
It has been 4 years since the world was transformed by the novel coronavirus COVID-19 when we experienced disruptions due to shelter-in-place requirements, uncertainty from lack of understanding of the virus, and lack of treatment or prophylaxis (Giuntella et al., 2021; Riera et al., 2021; Shepherd & Mohohlwane, 2021). These disruptions especially affected people in caregiving roles. Frontline healthcare workers were providing care to highly infectious and seriously ill patients with a virus that was poorly understood and without a cure; educators and other professionals had to stay home and shift learning and work to virtual platforms overnight; parents of younger children were juggling virtual learning while managing their other personal and professional responsibilities; and adult children were relocating aging parents from long-term care facilities to their homes (American Psychological Association, 2020, 2021; Hossain et al., 2020; Li et al., 2021; Serafini et al., 2020).
The mental health of family caregivers also received attention (Dang et al., 2020; Nesbitt-Ahmed & Subrahmanian, 2020; Rosalynn Carter Institute, 2020). The 53 million adults who provide unpaid care to a family member or friend in the United States have been an unseen workforce that contributes $600 billion with significant psychological cost (National Alliance for Caregiving & AARP, 2020; Reinhard et al., 2019). Pre-pandemic, 75% of older adults relied on family caregivers for at least one independent activity of daily living (Van Houtven et al., 2020). Studies from prior pandemics show that family caregivers have to navigate worsening health of their care recipients’ because of shortages in healthcare personnel and supplies (Loh & Amir, 2019), the risk of exposure if the care recipient requires in-home care (Elizarrarás-Rivas et al., 2010; Giebel et al., 2020), all while juggling childcare, distance learning, and professional responsibilities (Gibson et al., 2018). Early studies during the COVID-19 pandemic confirmed high levels of psychological strain on caregivers. In one study, two-thirds caregivers had an adverse mental or behavioral health issue and a third reported suicidal ideation (Beach et al., 2021; Czeisler et al., 2020; DeAngelis, 2020). Observational studies have since shown that caregivers experienced more psychological strain both compared to non-caregivers (Beach et al., 2021), and compared to caregivers prior to the pandemic (Rodrigues et al., 2021). Caregivers in Germany perceived additional caregiving burden due to caregiver age, excessive caregiving demands, challenges with managing dementia, challenges with implementing COVID-19 protocols, and increase in caregiving responsibilities (Budnick et al., 2021).
While caregiver strain during COVID-19 has been documented, there is limited information on how caregivers adapted to these new challenges. Developing these insights can help develop resource allocation plans for future pandemics and other natural disasters and developing policies to support caregivers as they pivot. The purpose of this current study was twofold. First, we sought to document the caregiver experiences and adaptations the early part of the pandemic. Second, we sought to examine the presence of both positive and negative emotions related to caregiving, and to examine which dimensions of the caregiving experiences were associated with each.
Methods
We developed and deployed an anonymous, online survey distributed via social media and networks in May 2020. The survey was developed using a combination of well-validated measures and items adapted specifically for the survey to assess caregiver changes and experiences. Participants were deemed eligible to participate if they reported that they were 18 years of age or older and self-identified as an informal caregiver to a child or adult with mental health or medical conditions. While the survey link remains live, we proactively made two efforts to increase participation, the first in April to June of 2020 and the second one in September to December of 2020. All study procedures and materials were approved by the institutional regulatory board.
Survey Methods
We used non-probability, convenience sampling to capture caregivers’ experiences as early as possible in the pandemic. Though less generalizable than probability sampling, this method is optimal for studies aiming to recruit groups who are hard to identify and reach. (Fielding et al., 2017) The study team distributed the survey link through various methods including social media platforms of the study team (e.g., Facebook, Twitter); mass emails to colleagues, friends, and family; Discussion Boards of professional societies; and through advertisement in the newsletter of the National Alliance of Caregiving. We included a QR code in various presentations led by the first author.
Interested respondents used the link to provide informed consent and were directed to confirm that they were 18 years of age or older, that they were an informal caregiver to a child or adult with health conditions. If deemed eligible, the remaining items in the survey were presented. All respondents were encouraged to share the link with others, even if they were not eligible for this study.
Measures
The survey included five sections and is provided upon request.
Demographics and Health Conditions
Participants self-reported caregiver demographics (e.g., age, gender, race, ethnicity, religious background, years of education, marital status, country/state of residence, number of adults/children under their care) as well as their care recipient’s characteristics (i.e., age, health conditions). Initially, the health conditions were those assessed by the Center for Medicaid Services. We subsequently included other conditions (e.g., childhood autoimmune diseases) based on feedback from initial respondents who found the pandemic challenging while caring for childhood conditions that were relatively rare. We combined health conditions into the following categories: neurological, hematology/oncology, psychological, pain, cardiovascular, metabolic/endocrine, pulmonary, development disorders, COVID-19 high-risk group, and other (see Appendix 1 for details).
Caregiving Tasks
We assessed caregiving responsibilities, including hours spent caregiving per week, caregiving activities including activities of daily living (ADLs; e.g., bathing, toileting) and instrumental activities of daily living (IADL) based on the Lawton and Brody IADL Scale, (Lawton & Brody, 1969) emotional support, and provision of different types of medical care not captured by ADLs or IADLs (e.g., help with medication). We assessed caregivers’ relationship to the care recipient. In April 2020 (1 month after initial deployment), we updated the survey to include items assessing care recipient’s gender, and whether caregivers cohabitated with their care recipient. For analyses, caregiving activities were grouped into ADLs (bathing, dressing, feeding, mobility, toileting, transferring), IADLs (communication/telephone, food preparation, handling finances, housekeeping, laundry, shopping, transport), Medical Activities (injection administration, incontinence care, managing ostomy, care recipient’s medication management, own medication management, oxygen/related equipment, ventilator, wound care) and Emotional Support.
Caregiving Changes due to COVID-19
The following items were developed for the survey: the extent to which caregivers used precautionary measures to mitigate the spread of COVID-19 (e.g., quarantine, cleaning surfaces), fear of contracting COVID-19, changes in spending time with their care recipient, how they compensated for loss of in-person visits (e.g., videoconferencing), whether the caregiver or their care recipient were tested, isolated or quarantined due to COVID-19, and how COVID-19 impacted their caregiving tasks and responsibilities. We also assessed perceived changes in incomes due to COVID-19, and perceived changes in availability of resources and supplies. Caregivers were asked to choose their main caregiving concerns related to COVID-19 (e.g., contracting the disease, not being able to get medical attention, not being able to get groceries). The survey also assessed perceived changes in communication with healthcare providers (e.g., ability to attend outpatient visits, timeliness of electronic communication, and contacting their care recipient’s doctor to discuss COVID-19 risk). For each of these categories, we provided opportunities for narrative responses to allow respondents to add additional context to their responses. For analyses, caregiver precautions were grouped as follows: Physical distancing (isolation, quarantine, social distancing, maintaining six feet), Protective measures (cleaning surfaces, washing hands more, wearing personal protective equipment), and other.
Psychosocial Measures
The survey included validated psychosocial measures of depression, anxiety, caregiver burden, loneliness, and positive aspects of caregiving to assess the psychological impact of COVID-19. We screened for depressive symptoms via the abbreviated Patient Health Questionnaire (PHQ-2) (Kroenke et al., 2003), a two-item measure that assesses the frequency of depressed mood and decreased interest or pleasure in activities. Items are rated on a scale from 0 (not at all) to 3 (nearly every day) and a score of 3+ indicates likely major depressive disorder. We screened for anxiety via the abbreviated Generalized Anxiety Disorder scale (GAD-2) (Kroenke et al., 2007), a two-item measure of the frequency of feeling anxious and uncontrollable worry. Items are rated on a scale from 0 (not at all) to 3 (nearly every day) and a score of 3+ indicates likely generalized anxiety disorder. We screened for caregiver burden via the Zarit Burden Inventory (ZBI-4) (Bédard et al., 2001). The four items relate to perceived stress and meeting non-caregiving responsibilities, strain around relatives, time available for oneself, and uncertainty about caregiving. Items are rated on a scale from 0 (never) to 4 (nearly always) and a score of 4+ indicates likely significant caregiver burden (Higginson et al., 2010). We assessed perceived loneliness using the PROMIS measure, the 5-item UCLA Loneliness Scale (National Institutes of Health, 2016). Participants rate their agreement with items from 1 (never) to 5 (always). A score of 13+ indicates significant loneliness. We assessed the perceived positive aspects of the caregiving experience using the nine-item Positive Aspects of Caregiving scale (PAC-9) (Tarlow et al., 2004). Items are rated on a scale from 1 (disagree a lot) to 5 (agree a lot) with higher scores indicating more positive perceptions of the caregiving experience. Finally, we adapted select items from the Fear of Contracting HIV scale to assess fear of contracting COVID-19 (Holzemer et al., 2007). Participants rated their gut feeling about contracting COVID-19 on a 5-point scale of 1 (extremely unlikely) to 5 (extremely likely). They also rated their worry about contracting COVID-19 on a 5-point scale from 1 (none of the time) to 5 (a lot of the time).
Health Behaviors During COVID-19
The survey included items to assess behavioral changes during COVID-19 related to substance use (e.g., alcohol, tobacco, marijuana use), sleep, exercise, and eating nutritious or unhealthy food.
Statistical Analysis
We conducted univariate analyses with demographic data, caregiving variables, and psychosocial outcome variables. Logistic regression models examined predictors of dichotomized psychosocial outcome variables. These included meeting established clinical cutoffs for depression based on the PHQ-2, anxiety (GAD-2), high caregiver burden (ZBI-4), and loneliness based on the UCLA Loneliness Scale; and having a positive caregiving experience based on being in the top quartile of the PAC scale. Predictors included numbers of health conditions, caregiving activities, precautionary measures for COVID-19, and concerns related to caregiving during COVID-19. We adjusted for caregiver age, gender, marital status, race, and ethnicity. Given the relatively small sample size and rarity of some outcomes, we also conducted sensitivity analyses using Firth’s penalized logistic regressions for all outcomes (Firth, 1993). Analysis was conducted using Stata, version 18 (Stata Statistical Software (Version Release 18), 2023).
Results
Sample Characteristics
We focused on the subsample from the United States given the preponderance of responses and the significant heterogeneity in pandemic timing, impact, and responses across the countries that had respondents (Table 1). The mean age of these 264 respondents was 51.7 years (SD = 13.7). Most respondents were women (87%), White (81%), married/partnered (74%), and lived in a suburban area (58%). Nearly one in four had completed a postgraduate degree (24%). Nearly equal numbers of care recipients were significant others (32.6%) and children (34.1%). Per caregivers, care recipients were diagnosed with pain (55%), and cardiovascular (50%), psychological (49%), and metabolic/endocrine (45%) conditions (see Appendix 1 for definitions). Of the 264 total respondents, 143 responded to an updated survey which assessed cohabitation with care recipient and care recipient gender. Ninety-seven of these caregivers (68%) cohabitated with their care recipients and 55% reported that their care recipients were men.
Caregiver and Care Recipient Characteristics as Reported by Caregiver Respondents.
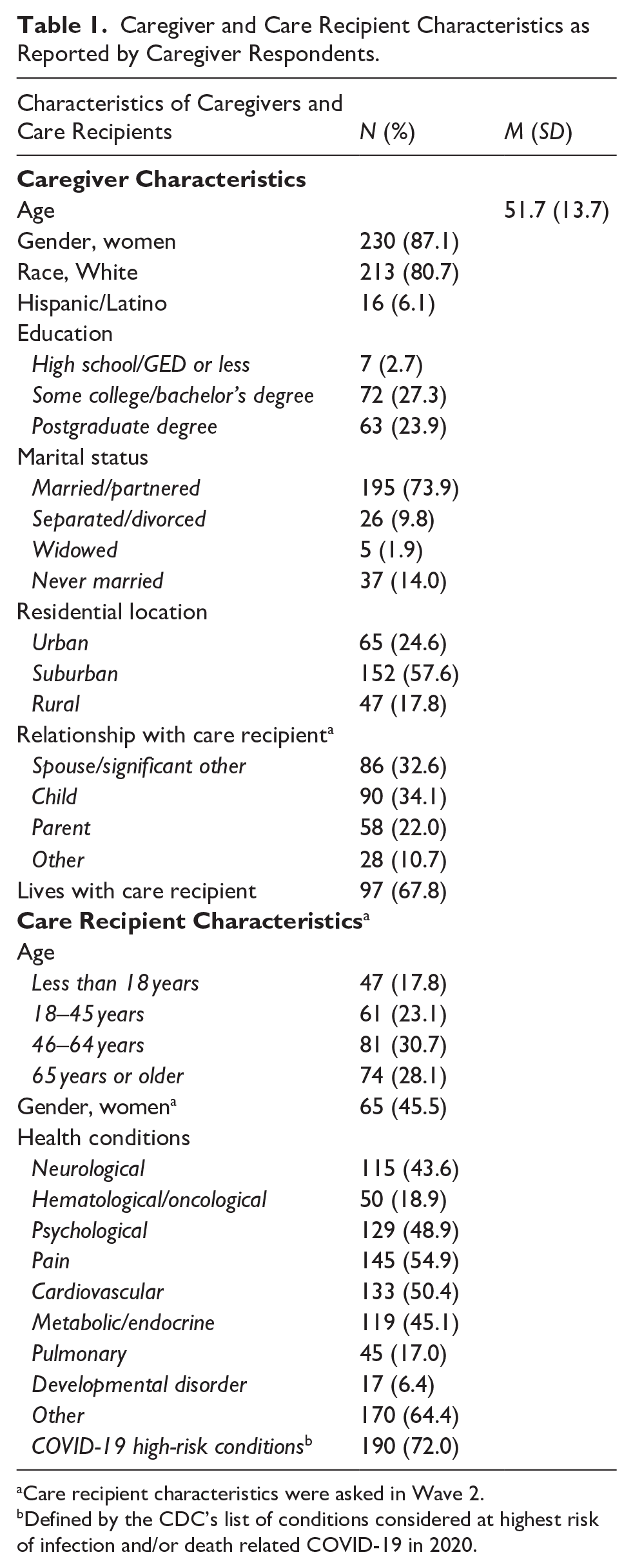
Care recipient characteristics were asked in Wave 2.
Defined by the CDC’s list of conditions considered at highest risk of infection and/or death related COVID-19 in 2020.
Caregiving Activities During COVID-19
As seen in Table 2, forty percent of caregivers provided 40 hr or more care per week. Nearly all caregivers (97%) assisted with IADLs, and 75% assisted with food preparation and housekeeping. Eighty percent of all caregivers supported medical activities, especially managing multiple medications (63%). Nearly two-thirds of caregivers provided ADL support (62%), commonly assisting with mobility (44%) and bathing (33%); a similar number (64%) provided emotional support to care recipients. Caregivers supported 8.9 (SD = 4.5) activities, used 4.3 (SD = 2.0) precautions, and had 3.0 (SD = 1.7) COVID-19 specific concerns. Nearly all reported taking physical distancing precautions (96%) and protective measures (97%). Approximately half (48%) practiced five or more precautionary measures. Forty-five percent worried about leaving their house because they may become infected with COVID-19 or infect their care recipient (47%). Concerns regarding their care recipients’ care were high and further illustrated by free text responses. One respondent noted, “If I become sick, who will care for my mother, since others in my family would be exposed to the virus?” Nearly two-thirds (62%) expressed concerns about obtaining help (e.g., “I have been trying to find someone to care for my husband if I get COVID. There are no good answers during this”), 55% expressed concern that their care recipient would not receive timely medical attention (e.g., “I am worried about healthcare rationing”), and 34% expressed concerns about obtaining medications. Caregivers were concerned about seeking non-COVID care, for instance, “My mother has COPD, and I know that she can’t go to the hospital if it flares up. She’s too high a risk.” Respondents poignantly stated concerns around, as in, “I am concerned about dying alone in the hospital without my family, who will then be left to take care of themselves [sic] without me?” while another noted, “I am concerned about not having the ability to have a funeral if [my partner] dies.”
Caregiver Activities During COVID-19.

PPE = personal protective equipment (e.g., gloves, masks, gowns).
Nearly two-thirds of caregivers (N = 163, 62%) reported an increase in their caregiving responsibilities, and changes in time spent with their care recipient since the pandemic (62%) of these, 39% reported spending more time than before. This was reflected in statements such as, “I am concerned about not being able to see my Dad: he’s in an independent living apartment in lockdown/isolation due to the virus outbreak. Also, that he’ll contract the virus and I cannot see/help him.” Of the 59 caregivers who spent less time with their care recipient, 80% used phone calls (N = 47) and 47% used video conferencing (N = 28) to compensate. Caregivers described strategies to maintain their connection to care recipients during shelter-in-place mandates, making socially distanced visits (e.g., “I talk through the window,” “I wave/dance in front of the driveway. My care recipient is hard of hearing, so using the phone isn’t good.”); getting more informal help (e.g., “I ask others to help that live closer to my care recipient”); getting more paid help (e.g., “I liaise daily with carers and housekeepers”); and finding alternate communications (e.g., “I send lovely cards”). Caregivers of those in assisted living facilities and other institutions found shelter-in-place particularly challenging. Respondents noted, “I am concerned about not being able to provide emotional support as my mother has been quarantined after a stroke at a rehab facility”, while another stated “I got a temporary custodial job at his assisted living facility and spend breaks in his room.”
Despite the high education and employment levels, more than half of all respondents reported some concern about their financial situation since the pandemic began (N = 137; 52%), stating that, “I am concerned about being laid off with no health insurance/mental health supports.” Amongst caregivers who were asked behavioral questions (Wave 2; N = 126), 67 caregivers reported exercising less (53%) and 77 caregivers reported sleeping worse (61%) during the pandemic. Almost two-thirds of these caregivers (61%) endorsed alcohol, marijuana and/or tobacco use. More than two in five reported consuming alcohol a few times a week or daily (N = 54, 43%).
Caregivers’ Psychosocial Outcomes
At the time of the survey, 85 (32%) met clinical cutoffs for depression, 100 caregivers (38%) met clinical cutoffs for anxiety, 150 (57%) met clinical cutoffs for caregiver burden on the ZBI-4, and 48 (18%) caregivers met criteria for loneliness (Table 3). One hundred eighty-eight (71%) caregivers met clinical criteria for at least one of the four psychosocial measures of anxiety, depressive symptoms, caregiver burden, and loneliness, with 40% meeting clinical criteria for two or more, and 25% meeting criteria for at least three. Interestingly, 66 caregivers (25%) scored in the top quartile on the PAC-9 scale. Notably, all caregivers in the top quartile of the PAC-9 also met clinical criteria for at least one other psychosocial measure.
Descriptive Analyses of Validated Psychosocial Measures. a

PHQ-2 = Patient Health Questionnaire 2 items, cutoff = 3+.
GAD-2 = Generalized Anxiety Disorder questionnaire, cutoff = 3+.
ZBI-4 = Zarit Burden Inventory, cutoff = 8+.
PROMIS loneliness measure, cutoff = 13+.
PAC-9 = Positive Aspects of Caregiving questionnaire, top quartile cutoff = 35+ (higher scores indicate more positive).
Compared to caregivers reporting no changes, changes in caregiving responsibilities was significantly related to depression, anxiety, and caregiver burden. Uncertainty of finding necessary resources for the care recipient was significantly associated with anxiety (p < .01), caregiver burden (p < .01), loneliness (p < .05), but also with positive aspects of caregiving (p < .05). Respondents who noted that COVID-19 had impacted their communication with care providers were also more likely to report depression (p < .01), caregiver burden (p < .01) and loneliness (p < .05). Reporting three or more concerns related to COVID-19 was significantly related to depression (p < .01), anxiety (p < .01), caregiver burden (p < .01) and loneliness (p < .05).
Caregivers reported greater caregiver burden if they assisted the care recipient with two or more activities (p < .05), and if they spent more time with the care recipient during the pandemic (p < .01). Compared to caregivers who spent < 20 hr per week in caregiving tasks, those who spent 20 or more hours per week caregiving reported greater loneliness (p < .05) but also positive aspects of caregiving (p < .01). Worry about leaving the house was significantly associated with anxiety scores (p < .05). Being told to quarantine or self-isolate was significantly associated with loneliness (p < .05).
Regression analyses (Table 4) showed that a higher number of concerns about caregiving during COVID-19 was associated with a higher likelihood of meeting the cutoff for anxiety (p < .001). A higher number of caregiving activities was associated with higher likelihood of meeting the clinical cutoff for caregiver burden (p < .001) and for loneliness (p < .001). Firth’s penalized logistic regressions yielded similar results with respect to coefficient magnitude and significance (Appendix 2) (Firth, 1993).
Odds Ratios and 95% Confidence Intervals from Logistic Regression Analyses Showing Association Between Caregiving Characteristics and Psychosocial Measures.

Depression measured by PHQ-2 = Patient Health Questionnaire 2 items, cutoff = 3+.
Anxiety measured by GAD-2 = Generalized Anxiety Disorder questionnaire, cutoff = 3+.
Caregiver Burden measured by ZBI-4 = Zarit Burden Inventory, cutoff = 8+.
Loneliness measured by PROMIS loneliness measure, cutoff = 13+.
Positive aspects of caregiving measured by PAC-9 = Positive Aspects of Caregiving 9 item questionnaire, top quartile cutoff = 35+ (higher scores indicate more positive experiences).
Discussion
Our first goal was to document caregiver experiences during the early part of the pandemic. Results indicated that caregivers adopted new strategies to manage care and maintain connections with their care recipients and were taking multiple precautions to mitigate infection risk. For many caregivers, these were undertaken to care for more individuals and more intensive care than before the pandemic-related shelter-in-place mandates. Nearly all care recipients required IADL support. As the pandemic hit, caregivers worried about receiving necessary help, medications, or timely care for their care recipients.
Our second goal was to understand the psychological effects of the pandemic on caregivers, and to determine which dimensions of the caregiver experience were related to the psychological effects. Given that decades of literature have emphasized the connection between caregiver intensity and psychological strain, (Ge & Mordiffi, 2017; van der Lee et al., 2014; Zhu & Jiang, 2018) it was not surprising to note that caregivers frequently met the clinical cutoffs for depressive symptoms, caregiver burden, and/or anxiety. Our results also showed that the additional burden of managing vulnerable care recipients during a pandemic led to additional strain due to greater intensity of caregiving, changes in caregiving responsibilities, and worry about receiving timely care.
Yet, one in four caregivers also reported positive dimensions of caregiving, especially if they were caring for people with more health conditions. There is limited literature on documenting positive emotions of caregiving during the pandemic, and our study makes an important contribution in this area. A qualitative study of caregivers of persons living with dementia noted that the pandemic strengthened their connections with their care recipient, and deeper reflections on their values and purpose (Tulloch et al., 2022). Another qualitative study noted that caregivers who had higher concerns about the pandemic and less support from family and friends experienced higher role stress than those who had more positive appraisal of the pandemic (Savla et al., 2021). More rigorous and generalizable research is needed to understand the sources and role of positive emotions among caregivers, and to determine if these could be enhanced during current and future public health crises.
A recent study of caregiver experiences during the pandemic described three sources of stressors: primary, such as obtaining care for their care recipient; secondary, such as increased financial difficulties, and stress appraisal (Beach et al., 2021). Our study extends these in three ways: by providing further nuance to the caregiving experience; by showcasing strategies that caregivers used to navigate both the pandemic and the shelter-in-place mandates; and by highlighting challenges in implementing these strategies. This provides an important direction to support caregivers during pandemics and other disasters, especially during the acute phases. First, caregivers should be provided necessary resources such as PPE that would both mitigate infection risk and reduce their worry about infections. Second, technology should be made readily available for individuals in inpatient facilities such as hospitals and nursing homes, so that caregivers and care recipients can maintain their connections where physical distancing is mandated. Third, health care providers should use their virtual care visits to engage with caregivers, assess their concerns about the care recipient, and assess caregivers’ wellness.
The strengths of our study include the rapid deployment of a survey in the acute phases of the COVID-19 pandemic, the combination of validated instruments and COVID-19 specific items to assess psychosocial well-being, the focus on caregiver experiences and behaviors, the use of social media to increase reach, and allowing participants to share their experiences to deepen our understanding of our quantitative results. Our study has several limitations. First, because we did not seek a representative sample of caregivers to participate in our survey, our results do not reflect population-average effects. Second, our sample was predominantly White, well-educated participants who were not facing financial challenges. Studies have revealed that individuals from racial and ethnic minority groups disproportionately felt the negative effects of the pandemic (Garcia et al., 2021; Tai et al., 2021), and it is likely that caregivers within these communities also faced greater challenges (Longacre et al., 2021; Moon et al., 2022). However, we also note that even our highly educated, financially stable caregivers experienced significant challenges which would be only amplified in more vulnerable groups. Third, we note the small sample size for some demographic groups (e.g., Hispanic respondents, n = 16). While we controlled for these characteristics to reduce selection bias given the use of convenience sampling, we cannot draw any conclusions about the association between demographic characteristics and our outcomes. Fourth, the cross-sectional design precluded any causal inferences of the effects of the pandemic on psychosocial outcomes. It is possible that caregivers were experiencing psychological strain before the pandemic which remained unchanged. Because of these limitations, these findings should be considered exploratory and hypothesis generating for rigorously designed quantitative surveys focused on the caregiver experience during future public health emergencies.
Conclusions
Our study highlights how the pandemic affected caregivers both positively and negatively, the practical strategies they used to navigate the shelter-in-place requirements, and the profound lengths to which they went to support their care recipients. These insights should be used to develop policies and plans to address their needs in future public health emergencies that may be caused by infectious diseases, natural disasters, and climate change.
Footnotes
Appendix
Odds Ratios and 95% Confidence Intervals from Penalized Logistic Regression Analyses Showing Association Between Caregiving Characteristics and Psychosocial Measures. a

| Depression b | Anxiety c | Caregiver burden d | Loneliness e | Positive aspects of caregiving f | |
|---|---|---|---|---|---|
| Caregiver demographic characteristics | |||||
| Age | 0.95 [0.37, 2.41] | 0.96 [0.94, 0.99] | 1.01 [0.99, 1.03] | 0.99 [0.96, 1.02] | 1.00 [0.97, 1.02] |
| Gender | 0.93 [0.48, 1.78] | 1.85 [0.68, 5.03] | 2.1 [0.86, 5.1] | 2.07 [0.5, 8.61] | 0.83 [0.33, 2.07] |
| Marital status | 2.09 [0.58, 7.49] | 0.85 [0.44, 1.63] | 0.82 [0.43, 1.55] | 0.5 [0.23, 1.1] | 1.22 [0.6, 2.47] |
| Race | 1.68 [0.68, 4.13] | 2.36 [0.59, 9.35] | 4.17 [0.89, 19.44] | 2.38 [0.5, 11.24] | 0.95 [0.24, 3.81] |
| Ethnicity | 1.07 [0.98, 1.15] | 3.32 [1.27, 8.66] | 1.78 [0.77, 4.09] | 2.62 [0.7, 9.81] | 0.79 [0.34, 1.83] |
| Caregiving characteristics | |||||
| Number of health conditions | 1.05 [0.99, 1.13] | 1.04 [0.96, 1.13] | 0.97 [0.9, 1.05] | 1.02 [0.92, 1.12] | 0.95 [0.87, 1.04] |
| Number of caregiving activities | 0.96 [0.83, 1.11] | 1.01 [0.95, 1.08] | 1.15 [1.07, 1.23] | 1.16 [1.06, 1.26] | 0.97 [0.91, 1.05] |
| COVID-19 Precautions | 1.14 [0.97, 1.34] | 0.87 [0.75, 1.01] | 1 [0.86, 1.16] | 0.91 [0.75, 1.1] | 1 [0.85, 1.17] |
| Concerns specific to COVID-19 | 0.95 [0.37, 2.41] | 1.31 [1.11, 1.55] | 1.17 [0.99, 1.37] | 1.08 [0.88, 1.31] | 0.84 [0.70, 1.01] |
| N | 243 | 243 | 241 | 242 | 239 |
Firth’s penalized logistic regression used to address bias due to small sample sizes and rare events.
Depression measured by PHQ-2 = Patient Health Questionnaire 2 items, cutoff = 3+.
Anxiety measured by GAD-2 = Generalized Anxiety Disorder questionnaire, cutoff = 3+.
Caregiver Burden measured by ZBI-4 = Zarit Burden Inventory, cutoff = 8+.
Loneliness measured by PROMIS loneliness measure, cutoff = 13+.
Positive aspects of caregiving measured by PAC-9 = Positive Aspects of Caregiving 9 item questionnaire, top quartile cutoff = 35+ (higher scores indicate more positive experiences).
Acknowledgements
We thank the study participants for their willingness to share their experiences. This work was supported by resources provided by Stanford University and the Department of Veterans Affairs, including VA Office of Academic Affiliations Advanced Fellowship in Health Services Research (Dr. Blair Humber), and a Health Services Research Career Development Award (Dr. Josephine Jacobs). The views herein represent those of the authors and do not necessarily reflect the views of the Department of Veterans Affairs.
Ethical Considerations and Informed Consent
All study procedures and materials were approved by the institutional regulatory board. Waiver of consent was approved because of the anonymous nature of the survey
Author Contributions
RT, MS and RR conceived the project and developed the survey. RT, MS, MBH, and RR participated in data collection. RT, MS, JJ, SCT and TL conducted analyses and interpretation of the data. RT and MS prepared the manuscript and all authors reviewed and approved the final version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The PI is an investigator at the VA Palo Alto Health Care System. Dr. Humber was supported by a VA Advanced Fellowship in Health Services Research. Dr. Jacobs was supported by a VA HSR&D Career Development Award (CDA-19-120). The views expressed here are those of the authors and do not necessarily reflect those of the Department of Veterans Affairs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available by contacting the corresponding author.