
Abstract
Objective:
The purpose of this study is to assess type 2 diabetes mellitus (T2DM) risk factors in grandparent caregivers living in a rural environment.
Methods:
Clinical measures (hemoglobin A1c [HbA1c], blood pressure, and lipids) and self-reported data on social environment factors were attained. Data were analyzed via Pearson’s correlation and regression models.
Results:
By clinical definition of diabetes (HbA1c ≥ 6.5%), 21% were prediabetic and 28% had undiagnosed T2DM. There was an association between the number of individuals in the home and triglycerides (r = −.25), high-density lipoproteins (HDL; r = .43), and body mass index (BMI; r = .39). Guardianship status had a significant association with BMI (r = −.38). There was a significant association between low-density lipoprotein (LDL; r = −.32) and access to community shared resources. In the adjusted linear model, the number of grandchildren in the home had a significant relationship with HDL (β = .012, p = .021) whereas the number of individuals living in the home had a statistically significant relationship with HDL (β = .026, p < .000) and BMI (β = .046, p = .02). In addition, 15% of participants reported being food insecure.
Discussion:
Efforts are needed to identify and screen at-risk populations living in geographically isolated areas. Considerations should be given to leveraging existing community resources for grandparent caregivers via schools, health systems, and government agencies to optimize health and well-being.
Keywords
Introduction
Grandparent-headed households (GHHs) are one of the fastest growing family structures in the United States. The US Census Bureau (2014a) estimates that 5.9 million grandchildren (≤17 years) are being raised by their grandparents. Consequently, approximately 2.7 million grandparents are raising at least one of their grandchildren and about 39% of these grandparent caregivers have cared for their grandchildren for 5 years or more (US Census Bureau, 2014b). The largest number of GHH in the country reside in rural areas. Over 100,000 grandchildren are being raised by their grandparents in rural Appalachia and over half of these households have no parent present (US Census Bureau, 2016). These numbers have continuously increased over the last 25 years (US Census Bureau, 2016).
Skipped generation families are a subset of GHHs, which are formed as a result of crises such as parental incarceration, non-marital births, death, mental illness, and/or substance use disorder (Saxena & Brotherson, 2013; Winokur et al., 2014). This family structure has inherent strengths and challenges to health including mental, physical, and emotional factors for both grandparents and grandchildren (Arpino & Bordone, 2014; Patrick & Tomczewski, 2008; Silverstein, 2007). For instance, grandparents care for grandchildren who may have been otherwise put into foster care and separated from the extended family unit. This separation can result in a separation of the children from a sense of belonging as well as cultural and ethnic traditions (Koh & Testa, 2008). Moreover, grandparents who are the primary caregiver for their grandchildren have reported higher life satisfaction and happiness for keeping their family together (Bullock, 2005). Grandparenting provides a form of daily activity that can stimulate cognitive mechanisms and optimize cognitive aging and may reduce frailty when providing moderate and high amounts of caregiving (Burn & Szoeke, 2015; Chen et al., 2014).
However, potential challenges of GHHs can be significant. These family structures are more likely to live in poverty, have limited resources, suffer from food insecurity, and social isolation (Dunifon et al., 2014). It should be noted that over 60% of GHHs have household income less than 200% of the federal poverty line, with almost 50% of those living below the 100% federal poverty line (Dunifon et al., 2014). Despite this level of poverty, only 12% of these households receive public assistance of any kind and one third of GHHs receive food stamps (Dunifon et al., 2014). Therefore, even though grandparent caregivers are likely to work outside of the home they are more likely to be classified as “working poor” (Baker & Mutchler, 2010) and more likely to experience chronic disease such as type 2 diabetes mellitus (T2DM).
There is a growing body of evidence that suggests that grandparents raising their grandchildren disproportionately suffer from poor health compared with their peers who are not raising their grandchildren. Bachman and Chase-Lansdale (2005) conducted a study in Boston, Chicago, and San Antonio where grandmothers who had legal custody of their grandchildren indicated worse perceived physical health compared with single mothers. Similarly, Bigbee and colleagues (2011) found that rural and urban Ohio grandmothers who are caregivers for their grandchildren may be at risk for mental health concerns and at even higher risk of physical health problems. These findings may suggest that grandparents who are the primary caregiver for their grandchildren may not engage in preventive care or other health behaviors that promote optimal health outcomes.
Although the current literature of GHH focuses on the health of grandparents specifically in urban settings, there is a lack of information regarding health challenges of the GHH rural families. A review of the literature on custodial grandparents, Hayslip and Kaminski (2005) highlight the need for more research to understand the complexities of rural GHH. Due to socioeconomic factors associated with being raised in a GHH, grandchildren are often subjected to poor nutrition, have sedentary lifestyles, and may be overweight (Cunningham et al., 2019; Formisano et al., 2014). Because of the unique history of the Appalachian region, the economic changes in the regional industrial base, the rural nature of many Appalachian communities, and the persistent poverty that exists in some areas (Phillips & Alexander-Eitzman, 2016), rural families experience unique challenges in employment, access to health care, availability of health and social services, physical and social environment. The aforementioned characteristics are known determinants of health and health behaviors. For example, in rural Georgia, grandparent caregivers noted how unemployment exacerbates social isolation while access to resources are inhibited by lack of transportation and child care services (King et al., 2009). In addition, rural Appalachian grandparents may possess beliefs and values systems that differ from urban dwellers further impacting their health and health behaviors (Goins et al., 2011).
Moreover, T2DM affects more than 30 million Americans (American Diabetes Association [ADA], 2018) and is a major threat to the health of GHH. The Centers for Disease Control and Prevention (CDC) estimates that one in three children in the United States will develop T2DM in their lifetime and that 50% of the US adult population will have T2DM by 2050 (America’s Health Rankings [AHR], 2019). In addition, an estimated 12.9% of adults in Kentucky have T2DM, which is more than doubled the rate from 2000 (AHR, 2019). More alarming is that 17% of adults in Appalachia have been diagnosed with T2DM (AHR, 2019). Unfortunately, GHHs are likely to experience risk factors that predispose them to the development of T2DM in both grandparents and grandchildren, such as higher levels of stress, depression, and hypertension, limited physical activity, food insecurity, and limited access to health services. A prospective cohort study conducted as part of the Nurses’ Health Study showed higher rates of saturated fat consumption, hypertension, and diabetes among grandmothers caring for their grandchildren than those who were not (Lee et al., 2003). Another study found that caregiving grandmothers were more likely than non-caregivers (32% vs. 19%) to be categorized as depressed (Fuller-Thomson & Minkler, 2000). Given the increasing prevalence of GHHs, their greater vulnerability to T2DM, and the lack of information about the experiences of rural GHHs, we employed a socioecological approach to examine and describe the overall health and T2DM specific risk factors of GHHs.
Design and Method
Participants
For this study, grandparents residing in Appalachia Kentucky who were the primary caretakers for their grandchildren were recruited. The participants resided primarily in one town in a county with a Rural–Urban Commuting Area (RUCA) code of 10, which is an indicator that the County is completely rural (United States Department of Agriculture [USDA], 2010). Using an alpha of .05 and an effect sized of .20, a sample size of 70 (grandparents) was needed for the linear regression F test to have 83% power.
Study Design
This was a cross-sectional study design where data were collected regarding family structure (number of grandchildren being cared for, number of individuals living in the home, and legal custody status of the children); sociodemographic factors (insurance status, ethnicity, employment status, marital status, age, and gender); clinical outcomes to determine chronic disease risk (total cholesterol, triglycerides, blood pressure, hemoglobin A1c [HbA1c], low-density lipoprotein [LDL], high-density lipoprotein [HDL], body mass index [BMI], existing comorbid conditions); and self-reported social support using the Medical Outcomes Study (MOS) Social Support Scale (Sherbourne & Stewart, 1991); and household food insecurity index (USDA, 2012). All clinical outcomes data were collected as a point of care measure during the study visit after participants provided written consent. Prior to all study activities, institutional review board (IRB) approval was obtained via the Office of Research Integrity at the University of Kentucky. The protocol approval number is 14-0311-PIH.
Outcome Measures
BMI
Research personnel performed BMI measurement using standardized procedures. BMI was calculated from height and weight measured with a professional grade stadiometer and a professional grade digital body weight scale. To ensure accuracy, height measurements were taken without shoes and weight measurements were taken with all over-garments (e.g., jackets, sweaters, and vests) removed. BMI was calculated as body weight in kilograms divided by height in meters. A BMI of 26 or greater was considered overweight.
Blood pressure
Following at least 5 min of rest, trained research personnel measured blood pressure using American Heart Association Standards (Pickering et al., 2005) with a validated automated device using appropriate-sized cuffs while participant is in a sitting position. A systolic blood pressure greater than 130 mmHg or diastolic blood pressure greater than 80 mmHg was considered elevated.
Lipids
For each participant, a full fasting lipid profile (i.e., total cholesterol, HDL, LDL, and trigylcerides) were analyzed using the Cholestech® (Cholestech LDX, 2011), a small lightweight analyzer for point of care testing. The process consists of performing a finger stick and placing the sample on the test cassette, loading the cassette into the analyzer, and starting the run process. Accuracy and reproducibility of the Cholestech LDX has been certified by the Cholesterol Reference Method Laboratory Network, demonstrating that this point-of-care lipid profile method is comparable with centralized laboratory testing (Jain et al., 2011; Shemesh et al., 2006). Quality controls checks were performed on the Cholestech LDX analyzer prior to each data collection. For the purposes of this study lipids were considered problematic if LDL >130 mg/dL, HDL <60 mg/dL, total cholesterol >200 mg/dL, and triglycerides >150 mg/dL (US Department of Health and Human Services, 2005).
HbA1c
HbA1c was measured using the Bayer A1CNow + Point of Care A1C (Bayer Healthcare) monitor and disposable test cartridge using a finger stick whole blood sample. The system performs over 25 internal chemical and electronic quality control checks with each test, including checks for potential hardware or software errors, and potential reagent strip errors. An error code is reported in place of a result if any quality check does not pass. The Bayer A1CNow + Point of Care A1C system is annually certified by the National Glycohemoglobin Standardization Program. Accuracy and reproducibility have been demonstrated (Matteucci & Giampietro, 2011). For participants in this study who had an HbA1c between 5.7% and 6.4% was determined be prediabetic and those with an HbA1c ≥6.5% were considered to have T2DM (American Diabetes Association, 2019).
Statistical Analysis
Mean, standard deviation (SD), frequency, and proportions were used to describe the data. Then Pearson’s correlation was used to assess the association between family structure, clinical risk factors, and self-reported social support. Finally, unadjusted and adjusted linear and logistic regression models were conducted to determine whether there was a relationship between family structure, clinical risk factors, and self-reported social support. For these analyses, statistical significance was determined at p < .05.
Results
Table 1 displays a description of the sample population (n = 65) of grandparents. Most grandparents were women (n = 65, 98.5%), non-Hispanic White (n = 65, 98.5%), had at least one chronic condition (n = 49, 74.2%), and were enrolled in government insurance (n = 56, 86.2%). The average age of grandparents was 59.4 (±7.4) years and approximately half (n = 33, 50.8%) were married. Grandparents had a variety of employment statuses where most were unemployed (n = 34, 52.3%) followed by retired (n = 15, 23.1%), employed (n = 9, 13.9%), disabled (n = 5, 7.7%), and two (3%) participants declined to respond. Grandparents reported caring for 2.5 (±1.6) children with the majority having full legal custody of their grandchildren (n = 37, 59.7%). As for clinical risk factors, grandparents fell within the normal range of total cholesterol, triglycerides, LDL, HDL, systolic blood pressure, and HbA1c. However, diastolic blood pressure was higher than normal (90.8 ± 100.5) and BMI (37.3 ± 13.0) for grandparents.
Sample Characteristics.

MOS = Medical Outcomes Study; LDL = low-density lipoprotein; HDL = high-density lipoprotein; BMI = body mass index.
Government-assisted programs include Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), housing assistance, food stamps, welfare, use of health department (United States Department of Agriculture, 2019).
Community shared resources include gym, pool, school resources, group activities, church, and other.
Table 2 shows the results of Pearson’s correlation. The number of grandchildren in the home did not have a statistically significant association with clinical risk factors, self-reported social support, or presence of one or more chronic conditions. However, there was an association between the total number of individuals living in the home and triglycerides (r = −.25), HDL (r = .43), and BMI (r = .39). Guardianship status also had a statistically significant association with BMI (r = −.38). There was a significant association between LDL (r = −.32) and access to community shared resources (gym, pool, church, and group activities). There were no statistically significant associations between clinical risk factors and food insecurity or access to government assisted programs.
Correlations Assessing the Relationship Between Family Structure Characteristics and Risk-Factors Factors.
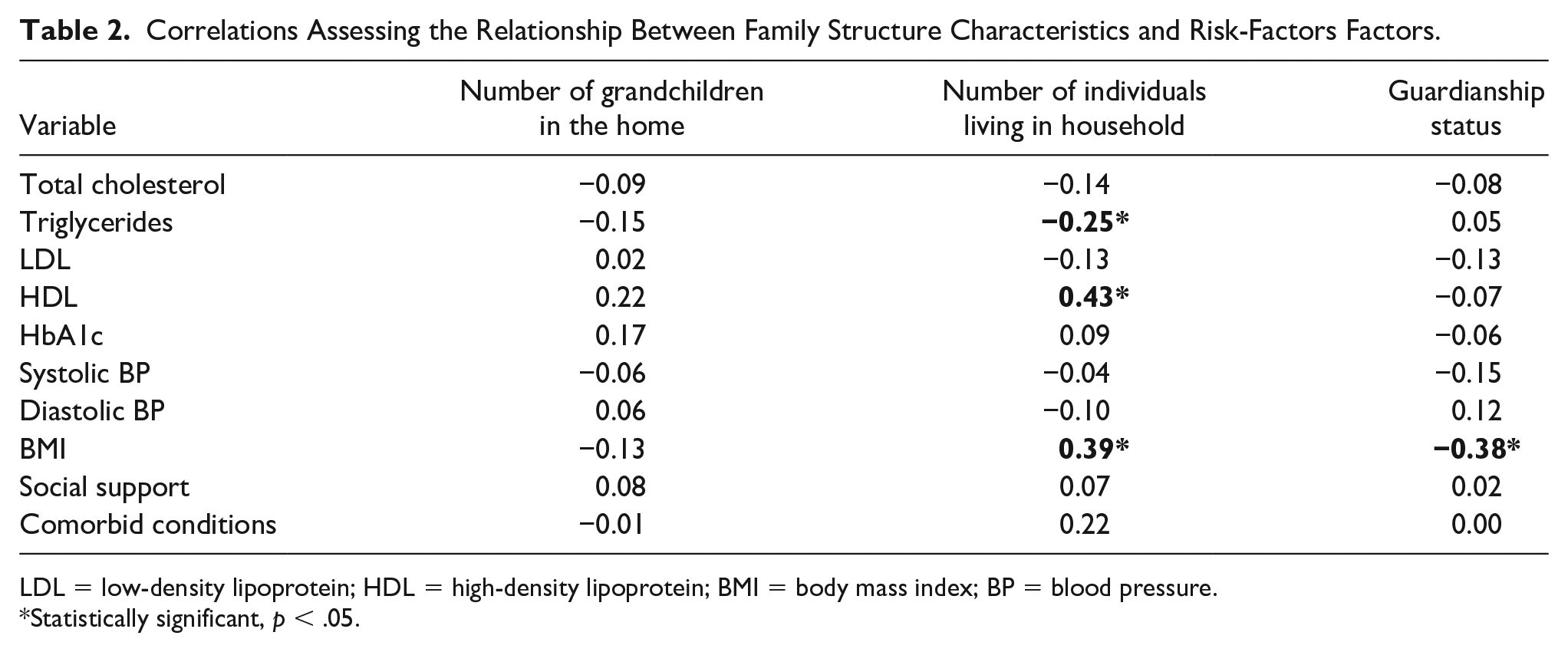
LDL = low-density lipoprotein; HDL = high-density lipoprotein; BMI = body mass index; BP = blood pressure.
Statistically significant, p < .05.
The results of the unadjusted linear and logistic regression models are displayed in Table 3. In the linear regression model for the relationship between the number of grandchildren in the home and outcomes of interest, there was a statistically significant relationship with HDL (β = .012, p = .021). Whereas the unadjusted linear regression model for the number of individuals living in the home, HDL (β = .028, p < .000) and BMI (β = .052, p = .003) showed significant relationships. Finally, the unadjusted logistic model assessing guardianship status, there was a significant relationship with BMI (odds ratio [OR] = 0.795, p = .002).
Unadjusted Regression Models Assessing the Relationship Between Family Structure Characteristics and Risk-Factors Factors.
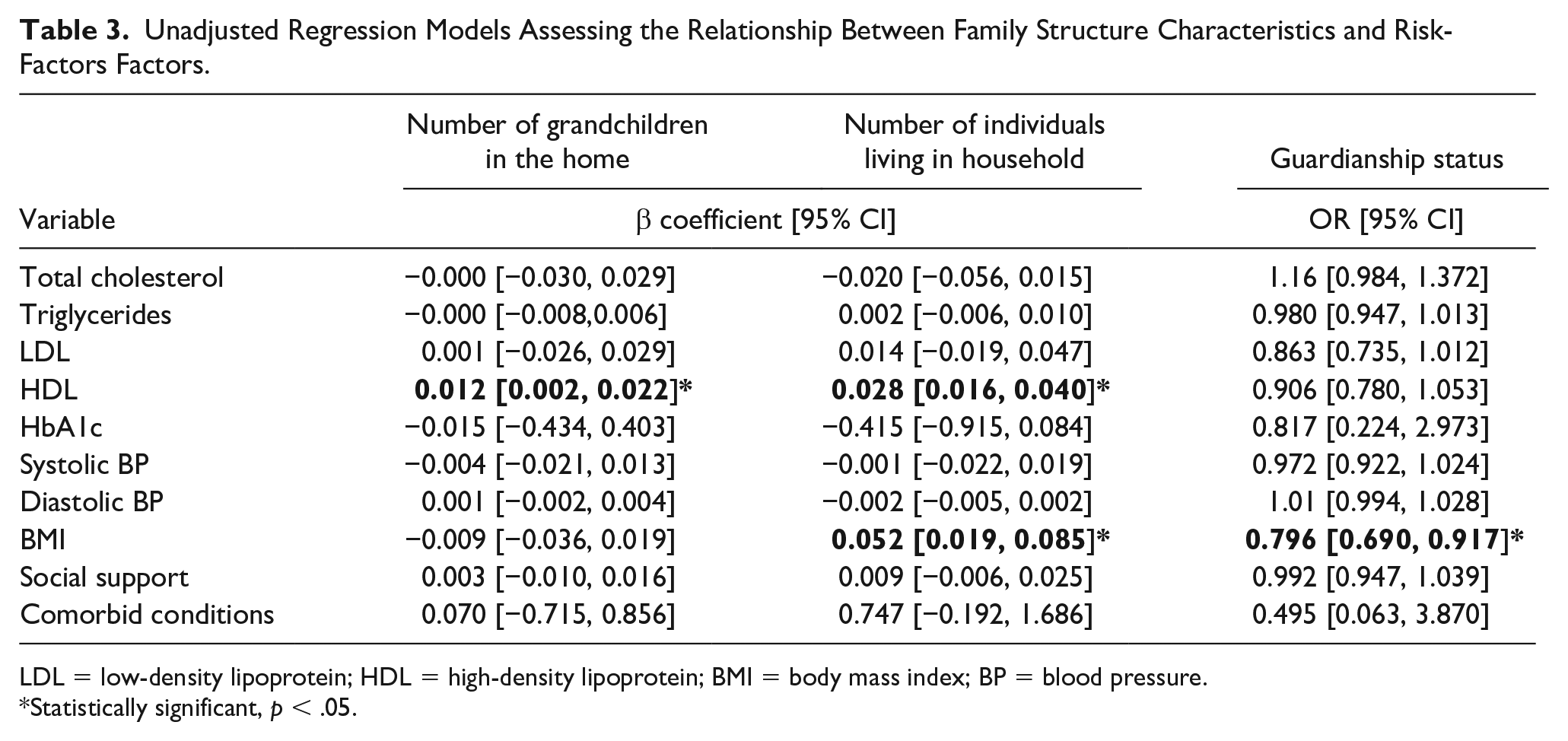
LDL = low-density lipoprotein; HDL = high-density lipoprotein; BMI = body mass index; BP = blood pressure.
Statistically significant, p < .05.
Table 4 shows the results for the adjusted linear and logistic regressions. There was no statistically significant relationship between the number of grandchildren in the home or guardianship status and the outcomes of interest. However, the number of individuals living in the home had a statistically significant relationship with HDL (β = .026, p < .000) and BMI (β = .046, p = .02).
Regression Models Assessing the Relationship Between Family Structure Characteristics and Risk-Factors Factors Adjusting for Covariates.

LDL = low-density lipoprotein; HDL = high-density lipoprotein; BMI = body mass index; BP = blood pressure.
Statistically significant, p < .05; covariates: age, marital status, employment status, age, insurance status, age of grandchildren.
Discussion
GHHs are one of the fastest growing family constellations in the United States. This study supports the use of evidence-based interventions designed for these grandparent caregivers (Chan et al., 2019). This is one of the first studies to look exclusively at the health of this vulnerable and growing population, despite our knowledge of their unique relationship and the implied risks to their health as a result. Moreover, the growing prevalence of these family constellations are of great concern in rural communities where disease prevalence is higher.
It is critical to consider the demographics of the sample and the population to be sure that interventions are appropriately tailored. This sample is representative of rural grandparents in the United States and were predominantly White women, married, and unemployed (Ahmed et al., 2019). However, importantly this sample was below 60 years old and not eligible for older adult services, such as social security or retirement services (Hatcher et al., 2018; Holben & Pheley, 2006). Grandparents in rural Appalachia may not only be younger than national averages but also dependent on government health care coverage (i.e., Medicaid) to treat more than one comorbid chronic disease. This has economic implication given that these grandparents already have limited resources, with an average of 2.5 kids in the house and most grandparents having legal custody, grandparents may need financial support to care adequately for their grandchildren. Biological and sociocultural risk factors for T2DM such as obesity, HDL, LDL, household food insecurity, and poverty have been well established in populations of rural Appalachia (Holben & Pheley, 2006).
An additional important finding from this study that will help with tailoring interventions is the health status of the grandparents. This is one of only a few studies that actually examines HbA1c in this important group, allowing a glimpse into the prevalence of diabetes and their risks. Almost one third of the participants in this study were prediabetic putting these grandparents at high risk for T2DM, which is higher than the estimated prevalence of prediabetes ranging from 9.3% to 14.6% in rural Kentucky or the state prevalence of 10.2% (Kentucky Cabinet for Health and Family Services, 2019). Moreover, in the United States, nearly 34% of the population has prediabetes, but less than 12% have been diagnosed by their health care provider. Although not every individual with prediabetes will develop T2DM, up to 65% of these individuals will progress to T2DM within 6 years if left untreated (CDC, 2017). Understanding the prevalence of prediabetes for this group will allow tailored interventions to include important information and appropriate activities that might prevent the progression to T2DM, including connections to local resources such as community centers and programs to promote exercise and other community-based resources.
There are a number of environmental factors in this community that underpin the prevalence of prediabetes and also illuminate areas where interventions might concentrate, including long term poverty, environmental factors, and limited access to health care. Evidence shows that dietary and lifestyle changes are the cornerstone of T2DM prevention. For example, diets that incorporate whole grains, fruits, vegetables, legumes, nuts, and moderate alcohol consumption, limits red/processed meats, processed foods, and sugar-sweetened drinks have demonstrated reduced risk of developing T2DM (Ley et al., 2014). Also, the U.S. Diabetes Prevention Program (DPP) proposed a minimum of 7% weight loss/weight maintenance and a minimum of 150 min of physical activity for diabetes prevention (Diabetes Prevention Program Research Group, 2002). However, the physical environment in rural communities such as those found in the study setting is often not supportive of regular physical activities. Unlike cities, rural areas tend not to have the sidewalks, easily accessible parks, commercial and public recreational facilities, and various organized recreational leisure (Swanson et al., 2013). In addition, grandparents in our study may not have time and resources to undergo physical activities due to their caregiving responsibilities.
Other important risk factors for diabetes also emerged in this population, including the average BMI among participants being 37.3 (±13.0), with the majority of the participants being obese. This may be closely tied to the physical inactivity and food insecurity noted in this sample. About 15% (n = 10) of this sample reported household food insecurity. The Appalachian mountainous terrain has resulted in isolated pockets of settlements, causing many individuals to have limited access to supermarkets, thus limited access to vegetables, fruits, and other whole foods. Food insecurity is associated with higher rates of chronic diseases, obesity, poor management of health conditions and depression (Gundersen & Ziliak, 2015; Laraia, 2013).
Despite the growing evidence of T2DM in the Appalachian region, there remains a lack of awareness of prediabetes and available data concerning prediabetes prevalence in this region. In accordance with the American Diabetes Association Standards of Medical Care for Diabetes this study concluded that 31% of caregiving grandparents had prediabetes and 66% were obese (data not shown), further exacerbating the risk of T2DM in this older population. These staggering results further elucidate the importance of prediabetes and obesity surveillance among caregiving grandparents in rural Appalachia. Furthermore, findings from this study can advance the purpose of the Appalachian Diabetes Control and Translation Project by promoting the implementation of local diabetes prevention and control policies to alleviate the burden of this disease among the aging caregiving population of this region.
Limitations
Despite the strengths in our study, we need to acknowledge some limitations. First, we had a small sample size, so the results are not generalizable to all rural Appalachian Kentucky grandparents. Second, due to the cross-sectional nature of the study, we cannot determine causal relationships between health status and grandparents’ caregiving status. Third, our study had only one grandfather, future studies should oversample grandfathers caring for their grandchildren to extend understanding of gender difference in caregiving. Finally, we did not collect information about how often grandchildren saw their biological mother or father, we acknowledge that this would have skewed our results on physical activity, what they ate, food insecurity, stress, and interaction with biological parents.
Implications
The findings from this study have implications for research, policy, and practice. The study provides a nascent view of the health of grandparents who are primary caretakers for one or more grandchildren. This growing family constellation is at risk for a variety of poor outcomes including T2DM. The study provides a solid foundation from which to tailor evidence-based interventions to meet the needs of the vulnerable population and reduce their risk for T2DM as well as reducing caregiver burden. It also provides a launching point for further research to examine further the sociocultural impact of unexpectedly raising grandchildren as caretakers. In addition, it allows communities, including providers, health care systems, schools, churches, and community members to better understand the needs of this important community group. This increased illumination of the needs of this group should be the basis for policy changes that has the potential to significantly improve the life of both the grandparents and the grandchildren, such as policies that address issues related to access to care and nutritious and affordable foods.
Footnotes
Acknowledgements
The content is solely of the authors and does not necessarily represent the official views of the University of Arizona Cancer Center or the Office of Community Outreach and Engagement.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute of Diabetes and Digestive and Kidney Disease (PI: J.H., R03DK101705). This publication was supported by the University of Arizona Cancer Center Office of Community Outreach and Engagement DREAM Center.