
Abstract

The advent of transcatheter aortic valve replacement (TAVR) has been one of the greatest achievements in cardiology since the turn of the 21st century. TAVR was initially developed in Europe 1 and quickly spread to other Western countries and then globally. The intensive and rapid refinement of TAVR devices has been largely based on their adjustment to valve anatomy, with the aim of avoiding complications, mainly through the availability of different valve sizes or designs.
Most TAVR trials and registries have historically been performed in Western countries and Caucasian populations, and data remain scarce for some other regions and ethnicities. It is widely acknowledged that some Asian populations have smaller annular anatomies. Thus, several registries have already analyzed aortic root anatomies in some Asian populations,2–4 and new TAVR devices have been developed both in China and India. However, even though South Asia accounts for one of the largest populations worldwide, aortic valve studies in South Asian populations are very limited.
In this context, the elegant and insightful article by Hakeem et al in the present issue of Journal of the Heart Valve Society comes to address a major unmet need for detailed anatomical valve data in such patients. The authors report a retrospective analysis comparing aortic root dimensions in a Pakistani population undergoing TAVR with those in other ethnic–racial groups, using data from cohorts reported in the literature. Their main findings include a higher incidence of smaller sinus of Valsalva (SOV) dimensions and of lower coronary heights compared to a European cohort. More specifically, although no tests of statistical significance are reported, a SOV <28 mm is documented in 66.7%, 22.8% and 14% of patients from Japanese, Pakistani, and European cohorts, respectively. Left main height is shown to be <10.7 mm in 18.7% and right coronary artery height is <12.7 mm in 14% of Pakistanis, with both percentages being higher than those reported in Japanese and European cohorts. Additionally, the authors report a high frequency of bicuspid valves. They also highlight the absence of TAVR devices tailored to these markedly different anatomies and suggest potential strategies to overcome such anatomical challenges (see Figure 1).
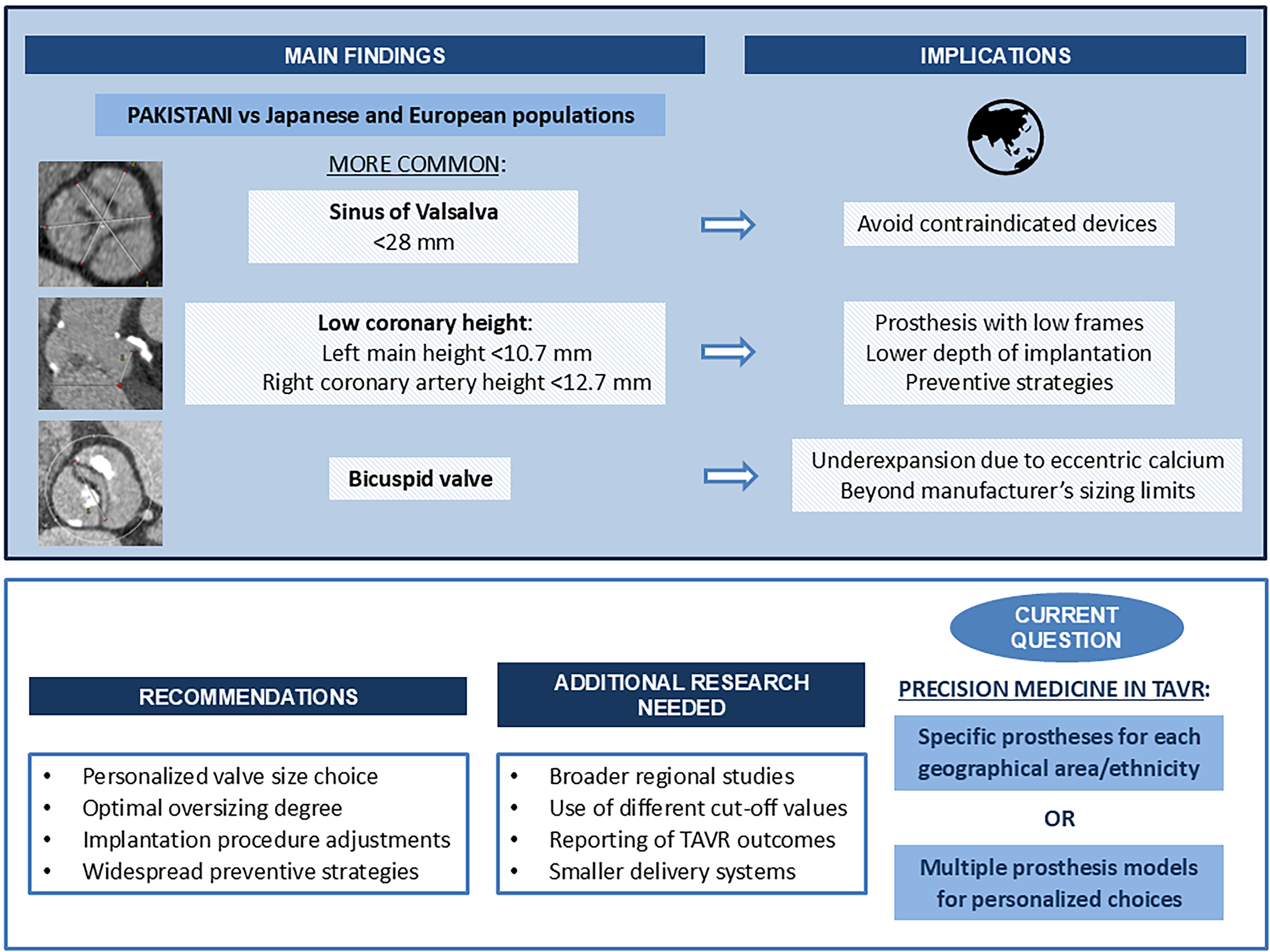
Geographical Differences in Anatomy and TAVR: Main Messages and Implications.
The study fully achieves the aim of raising awareness of the issue, and the reported data are very useful, as a needed first step. This Pakistani cohort included 494 patients and was compared with previously reported 90 East Asian and 181 European patients. Considering the potential variations in the overall populations of such regions and the way measurements are obtained in different places, broader regional studies will be required to validate these findings, with a sample size that allows significant conclusions to be drawn. Additional analyses will need to be performed with different cut-off values for SOV and coronary heights, since much of the literature has used the thresholds of 30 mm and 10 or 12 mm,5,6 respectively, instead of the values used in this study. Furthermore, future data will need to be presented alongside TAVR outcomes, since recent Asian registries do not appear to show results that differ greatly from European registries. It is unclear whether this is due to a low actual effect of anatomical differences or to a selection bias for less difficult cases.
While we await additional valve designs adjusted to different Asian populations, interventionists practicing in regions that are underrepresented in clinical trials should pay particular attention to the factors they can influence. These include: a personalized valve size choice and optimal oversizing degree depending on specific anatomical features, adjustments of the implantation procedure, and promoting a more widespread use of preventive strategies of potentially dreadful complications in selected patients with unfavorable anatomies.
In patients with low coronary height, balloon-expandable prostheses with short frames can be advantageous compared to self-expanding supra-annular devices because their frame may extend further up toward the coronary ostia. While a Sapien (Edwards Lifesciences) prosthesis may be the standard choice at present, the recently introduced Myval (Meril Lifesciences), a short frame prosthesis offering more sizing options, could be a promising valve for patients with low coronary heights. Further options to overcome this issue are aiming at an intentionally lower depth of implantation, or using preventive strategies (eg, BASILICA, CHIMNEY stenting, and coronary wire protection techniques), even though some of these are technically challenging.
The SOV diameter also plays an important role. In fact, some prosthesis types, such as the Evolut (Medtronic) valves, are contraindicated if the SOV is too small, according to the manufacturer's reference chart. The risk of coronary obstruction increases further when there is a combination of both low coronary height and small SOV, as reported by Ribeiro et al. 7 Thus, future studies in a South Asian population should probably focus on this subgroup of very high-risk patients.
The high prevalence of bicuspid valves in the Pakistani population is not surprising, since this has been well-reported in other Asian populations. 8 For a proper interpretation of these data, it should be noted that the median age of the population was only 71 years, since patients at a higher age (eg, 80–90) may rather have a pure degenerative stenosis. With such a high proportion of patients with bicuspid valves, in the future, it will probably be necessary to analyze their anatomical measurements separately from those of other patients. TAVR procedures in bicuspid valves are challenging. As mentioned in the study, this can be due to anatomical factors such as eccentric calcium and elliptical shape that can cause an underexpansion of the device, resulting in a higher frequency of paravalvular leak. Other factors can be the usually larger dimensions with an annular size lying beyond the limits of the manufacturer's sizing charts of currently available prostheses, or more frequent concomitant coronary anomalies and horizontal aorta, causing an increased procedural complexity. 9
Although not explored in this study, smaller vascular access dimensions have also been reported in Asian patients, with both iliac and common femoral artery luminal diameters being smaller than in Western populations. 10 Future development of smaller delivery systems will be needed alongside smaller valve designs.
As is the case with any good research study, the article by Hakeem et al answers some questions and it also raises some new ones: Based on these ethnic differences in aortic root anatomy, should we aim to have specific prostheses for each geographical area or for each ethnicity? Or, with the increasing multiethnicity in some world regions, should we have multiple prosthesis models that allow for personalized choices based on exhaustive anatomical measurements for each individual patient? Both approaches would pave the way for precision medicine in the field of TAVR.