
Abstract
This is a visual representation of the abstract.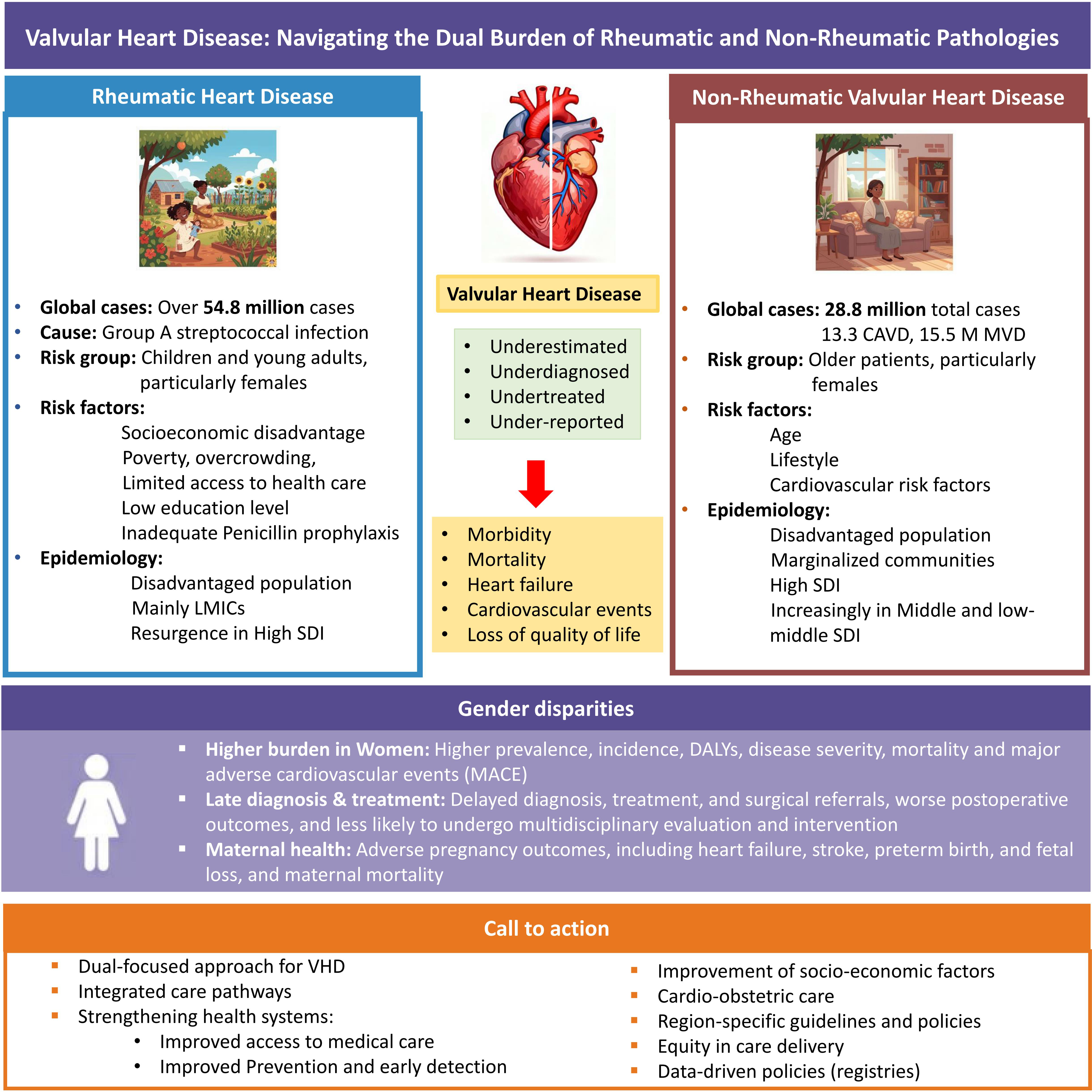
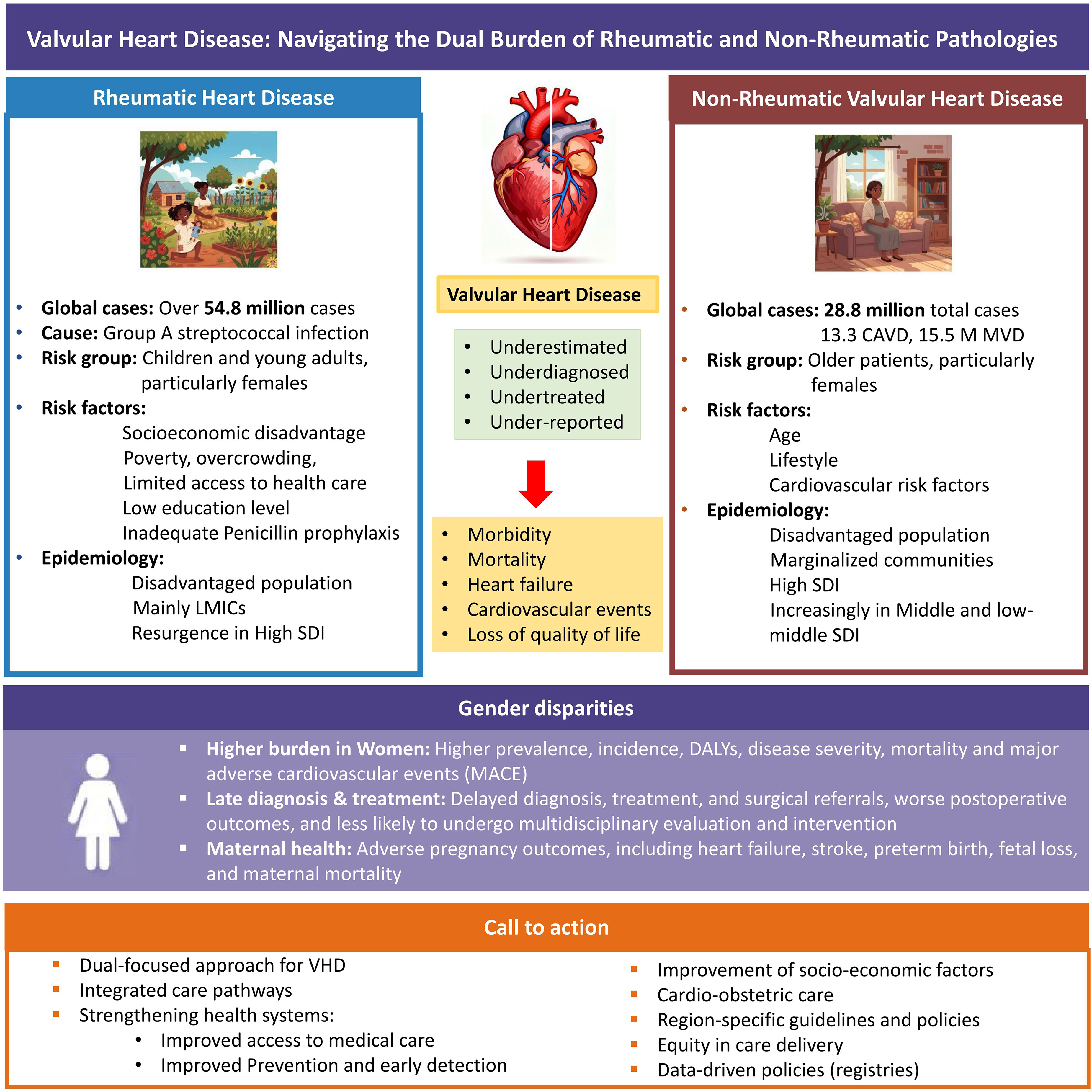
Valvular heart disease (VHD) is a major global public health concern, contributing to a rapid increase in cardiovascular morbidity and mortality globally 1 and posing an evolving challenge for health systems. VHD presents a dual challenge in the form of persistent rheumatic heart disease (RHD) and an escalating prevalence of nonrheumatic valvular heart disease (NRVHD), each showing distinct regional patterns. 1
Worldwide, there are over 54.8 million cases of RHD, 13.3 million of nonrheumatic calcific aortic valve disease (CAVD) cases, and 15.5 million cases of nonrheumatic degenerative mitral valve disease (DMVD). 1 Over the past three decades, the prevalence of RHD and NRVHD has increased 70.5% and 110.0% globally, with an imminent increase expected over the next 20 years. 2
Nonetheless, VHD is often underdiagnosed, detected late, and undertreated despite advancements in diagnostic modalities, including the expansion of the role of echocardiography and multimodality imaging, which facilitate earlier diagnosis, risk stratification, and procedural planning. Inequalities in access to timely diagnosis and treatment in low- and middle-income countries (LMICs) and among marginalized and vulnerable communities, particularly Indigenous populations in wealthier nations, lead to health care disparities. In addition, insufficient resources, financial constraints, and lack of systematic data collection result in further underestimation of the true disease burden in LMICs, which struggle with the dual burden of RHD and NRVHD.
RHD arises from an aberrant immune response to group A streptococcal infection, results in progressive inflammation and scarring of heart valves, and remains one of the most significant yet neglected cardiovascular conditions globally. Despite global efforts, RHD continues to disproportionately affect disadvantaged populations, especially children and young adults in LMICs, revealing a complex and heterogeneous epidemiological landscape. Importantly, a resurgence of RHD has been noticed in developed countries in recent years, mainly due to uneven distribution of medical resources and socioeconomic disadvantage, with the most recent cases of RHD being endemic rather than due to foreign exposure. 3
Socioeconomic determinants 1 such as poverty, overcrowding, poor sanitation, limited access to health care, and low-educational levels, remain key drivers of the ongoing RHD burden. Access to secondary prevention in RHD in the form of benzathine penicillin prophylaxis remains inconsistent amid supply shortages, insufficient awareness, and poor patient adherence. The loss of productive life years, coupled with limited access to secondary prophylaxis and advanced surgical interventions, perpetuates cycles of poverty and health inequity.
Women bear a disproportionate burden of RHD, with higher age-standardized disability-adjusted life years (DALYs), mortality, and prevalence rates, 4 a disparity rooted in both biological and sociocultural factors leading to more severe valvular damage and faster disease progression. RHD is a leading cause of maternal morbidity and mortality in many endemic regions, contributing significantly to adverse pregnancy outcomes, including heart failure (HF), stroke, preterm birth, and fetal loss. The complex interaction of cardiac pathology and pregnancy physiology necessitates specialized multidisciplinary care spanning preconception counseling, antenatal monitoring, and long-term postpartum follow-up. Unfortunately, routine cardiac assessment remains inaccessible or unavailable to most patients with RHD in LMICs, underscoring an urgent gap in service delivery.
In addition, NRVHDs have emerged as significant contributors to the overall burden of VHD in high-income countries and increasingly in LMICs. 5 Globally, the incidence of NRVHDs has been steadily increasing 5 in all regions, 2 especially in industrialized nations, driven by aging populations, lifestyle, and cardiovascular risk factors. 1 However, the most substantial increases in age-standardized prevalence of CAVD and DMVD were noted in the middle and low-middle Sociodemographic index (SDI) regions. 1 Moreover, NRVHD-related mortality has increased by 110.6% over the past three decades, with a further increase expected in the coming decades. 2
Importantly, there has been a marked increase in the global incidence of NRVHDs among women, 6 showing notable gender differences in the disease burden, 7 with women exhibiting higher incidence, mortality, DALYs, 5 and occurrence of major adverse cardiovascular events (MACE). 6 In addition, long-term disease outcomes and risk factors are unique to women. 6 The underlying mechanisms remain uncertain, and further investigation into the biological and sociodemographic factors contributing to these disparities is warranted. 6 Women are also consistently diagnosed at later stages of disease, receive delayed surgical referrals, exhibit worse postoperative outcomes, and are less likely to undergo multidisciplinary evaluation and intervention than men. 8 Delayed diagnosis and treatment might be the result of differences in presentation, but are more strongly linked to the historical underrepresentation of women in studies that form the basis of current guidelines for assessing disease severity, staging, and surgical timing.
HF remains one of the most severe complications of VHD, leading to high disability and mortality. The incidence of NRVHD-related HF continues to rise annually, with women consistently exhibiting higher burden and age-standardized prevalence rates (ASPRs) for NRVHD-related HF in all regions. 7
The geographical differences in global prevalence of RHD and NRVHD reflect an evolving epidemiological landscape shaped by socioeconomic factors, demographic transitions, and inequity in medical care. The coexistence of RHD and NRVHD places additional demands on already constrained health systems, especially in LMICs, urging integrated care pathways, adaptable to local contexts, that can address the required comprehensive strategies encompassing prevention, early detection, and access to medical and surgical treatment. In-depth assessment of VHD burden and trends globally, with region-specific insights, especially from LMICs, including the recent shifts in VHD epidemiology and burden across socioeconomic conditions and health care, is crucial but still insufficient.
The article “Epidemiological Trends in Rheumatic and Nonrheumatic Valvular Heart Disease in Low- and Middle-Income Countries from 1990–2019” by Gerbier et al sheds light on the patterns of VHD in LMICs, showing a marked shift in epidemiology with persistently high incidence of RHD and rising incidence and prevalence of NRVHD, resulting in dual burden in resource-limited settings. In addition, the study notes that RHD-related DALYs have decreased significantly in countries with higher SDI levels.
This emphasizes the critical need to improve of socioeconomic factors, reduce financial risks and barriers, and enhance disease prevention and access to health care. The prevention and management of VHD should be integrated into existing national primary health care systems, alongside improvement of awareness and training of health care providers.
Understanding and addressing the intricate interplay of factors involved in VHD is essential to address disparities, guide targeted public health initiatives and tailor health care policies to support equitable resource allocation for prevention, management, and treatment. This calls for region-specific data on demographics and disease characteristics through robust registries at the global, national, and hospital levels. Enhanced efforts for early diagnosis and timely treatment are vital to improve disease outcomes. Furthermore, long-term studies, with adequate female representation are necessary to identify clinical predictors, determine the disease prognosis, and elucidate critical points of action.
The global challenge of VHD (Figure 1) demands a nuanced, dual-focused approach that simultaneously addresses the enduring scourge of RHD and the rising tide of NRVHD, especially in LMICs. This underscores the urgent necessity of strengthening health systems, expanding access to both preventive measures, advanced therapies, and specialized cardiac care, with equity in care delivery. Prioritizing women's cardiovascular health, including a multidisciplinary focus on cardio-obstetric care, is essential to address existing gender disparities. Region-specific guidelines and policies must be developed to address these diverse challenges. A clear evidence-based roadmap 9 should guide the prevention and management of VHD, aiming to improve outcomes globally.
Valvular Heart Disease: Navigating the Dual Burden of Rheumatic and Non-Rheumatic Pathologies.