
Abstract
Post-implantation management of embolized transcatheter heart valves (THV) remains controversial. The current practice is to leave an embolized THV in the ascending aorta when it is stable, while implementing a second prosthesis for definitive treatment. We present the case of a 75-year-old male who underwent balloon-expandable aortic valve implantation following the migration of a previously placed self-expandable valve. He presented 1 week later with type A aortic dissection, requiring surgical repair. The argument could be made that even with successful implantation of a second valve, surgical explantation of the migrated valve may be considered in selected cases.
Case Presentation
A 75-year-old male known for atrial fibrillation, permanent pacemaker, hypertension, dyslipidemia, and a smoking history presented to the emergency department complaining of symptoms consistent with amaurosis fugax. He had recently undergone transcatheter aortic valve replacement (TAVR) 7 days prior at another institution. He was found to have a significant inter-arm blood pressure discrepancy (right arm: 111/59 mm Hg; left arm: 165/59 mm Hg). Differential diagnosis included transient ischemic attack, aortic dissection, and subclavian artery stenosis or occlusion.
The patient underwent a head CT which ruled out an acute intracranial process. CTA of the head and neck revealed an intimal dissection flap originating from the ascending aorta and extending into the brachiocephalic artery. Thoraco-abdomino-pelvic CT revealed two implanted valves: a balloon-expandable valve positioned in the aortic annulus, and a self-expandable valve in the ascending aorta. Type A aortic dissection was identified, beginning at the distal aspect of the self-expandable valve in the ascending aorta and extending through the brachiocephalic trunk, left common carotid artery, and left subclavian artery (Figure 1). Interestingly, a review of the post-implantation aortography from the patient's recent TAVR demonstrated no evidence of aortic dissection, contrast extravasation, or wall irregularities (Supplemental video 1).
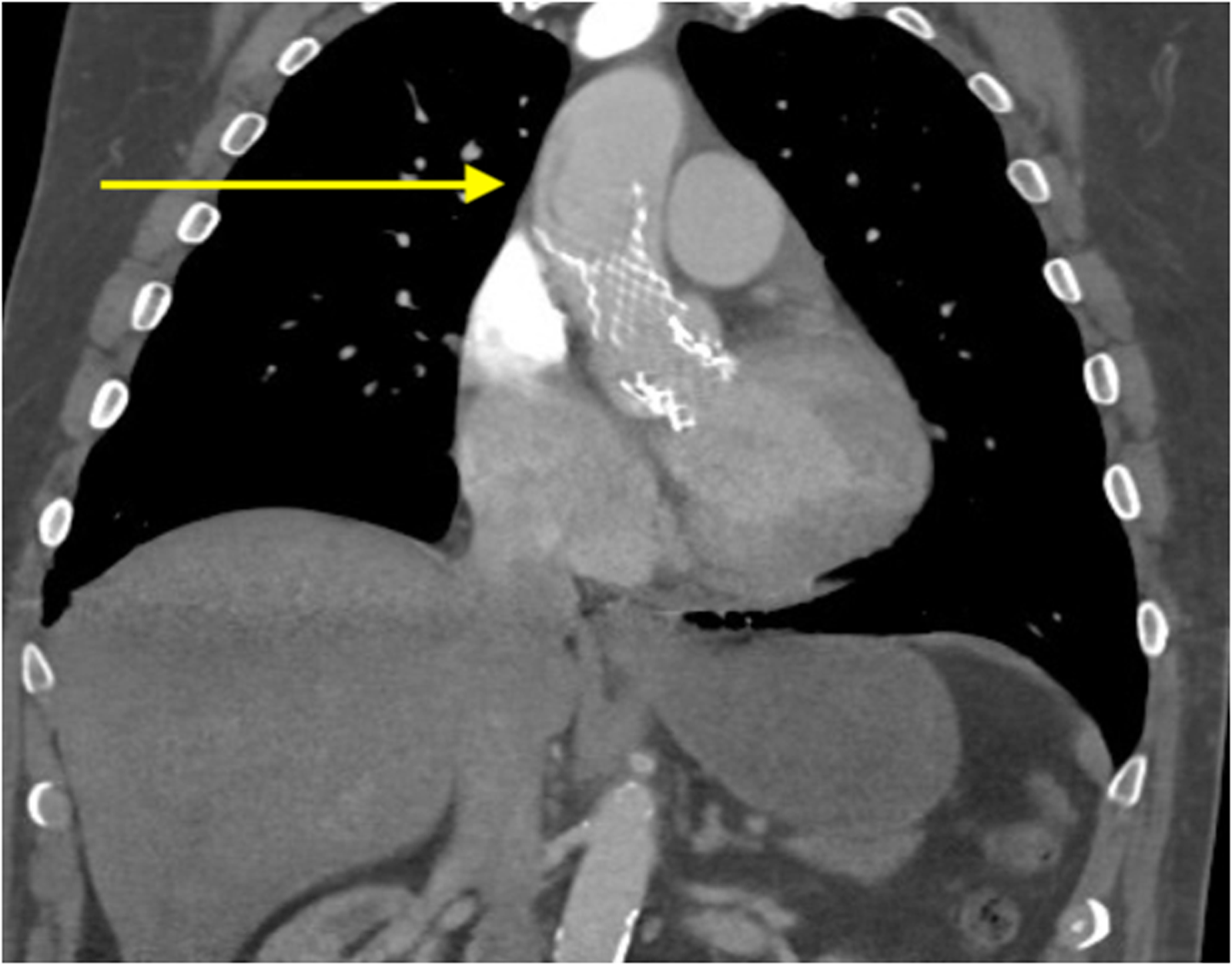
CT Scan of the Chest Showing a Balloon-Expandable Valve Correctly Placed in the Aortic Annulus and a Self-Expandable Valve in the Ascending Aorta. An Aortic Dissection Flap is Also Seen Distal to the Self-Expandable Valve.
Given the critical nature of the findings, the patient was brought to the operating room emergently for explantation of the migrated valve and type A aortic dissection repair. The surgery was performed via median sternotomy. Standard central cannulation was employed, with venous access in the right atrium and aortic cannulation in the distal ascending aorta. Transesophageal echocardiogram confirmed the presence of an aortic tear associated to the distal struts of the self-expandable valve (Figure 2, Supplemental video 2). Upon opening the ascending aorta, the self-expandable valve was found to have caused a tear in the aortic wall, creating a false lumen. The distal struts of the valve were protruding into the false lumen through a longitudinal tear in the aorta. The valve was explanted easily without complication (Figure 3). The entry tear was resected. The ascending aorta and hemi-arch were then replaced using a Dacron graft, and the patient was successfully weaned off cardiopulmonary bypass. The balloon-expandable valve was inspected and determined to be working properly. Myocardial and systemic ischemia time were 75 and 37 min, respectively. Antegrade cerebral perfusion time was 34 min; 3 min without perfusion, while patient was at 28 °C. Cardiopulmonary bypass time was 135 min.
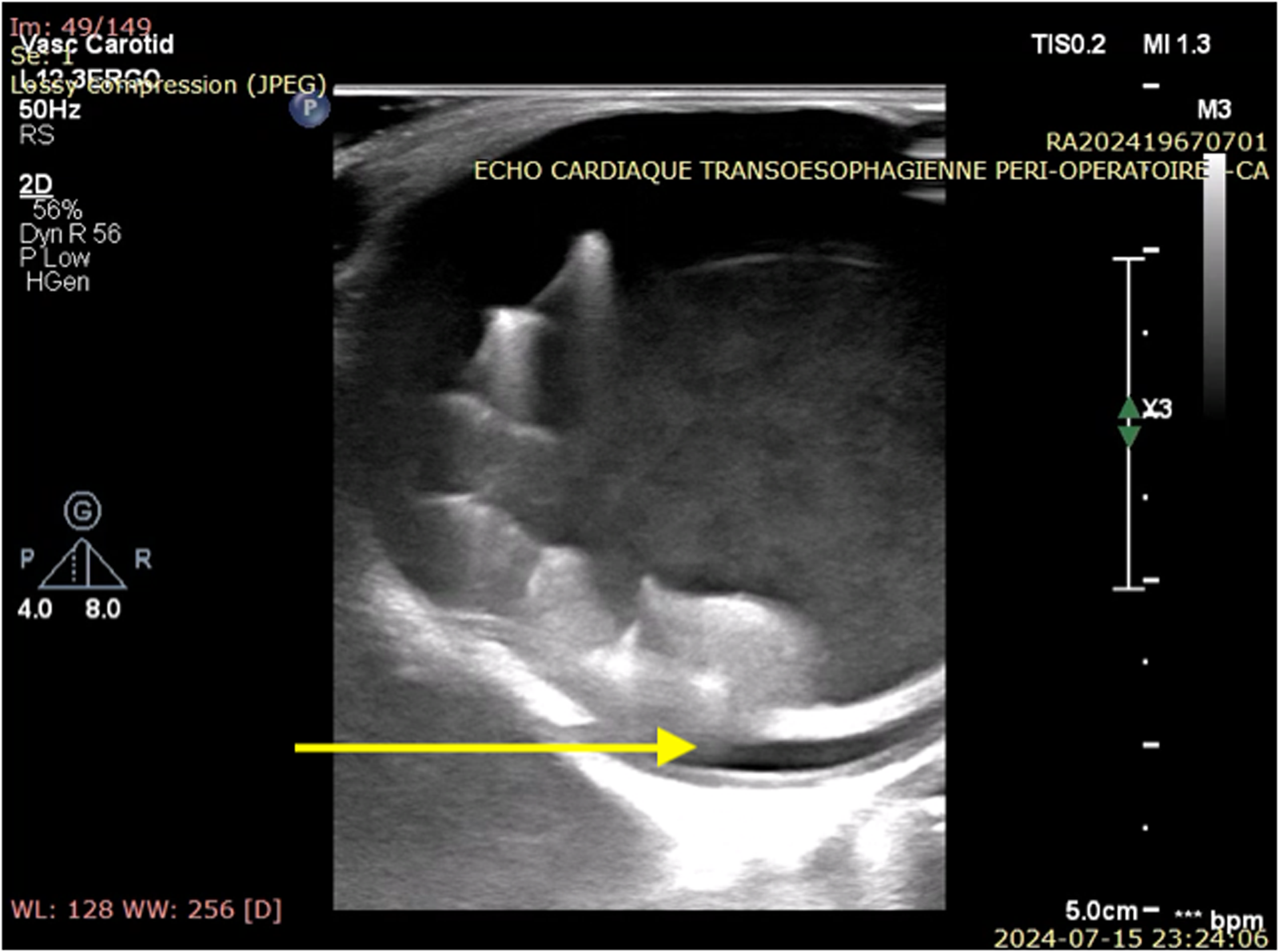
Intra-Operative Transesophageal Echocardiogram Showing the Migrated Valve Encompassed Into the Dissection Flap.

Explantation of the Self-Expandable Valve Causing Type A Dissection in the Ascending Aorta.
The patient had an uncomplicated post-operative course. He spent 4 days in the ICU and was discharged 8 days post-operatively. He was asymptomatic during follow-up, 1 month post-operatively.
Discussion
TAVR has transformed the interventional management of aortic stenosis, providing a minimally invasive alternative to surgical aortic valve replacement. However, valve migration remains a notable complication, with an incidence of approximately 1%. 1 Both balloon-expandable and self-expandable valves tend to embolize toward the left ventricle in cases of insufficient anchoring or toward the aorta if rapid pacing is interrupted during deployment.1,2 Common causes of embolization include mispositioning, manipulation errors, sizing inaccuracies, and rapid pacing failure. Additional risk factors include a larger sinus of Valsalva diameter, the use of self-expanding devices, the presence of a horizontal aorta, and repeated attempts at valve implantation.1,3,4
Type A aortic dissection is a rare complication post-TAVR. Its incidence is <0.5%, and it usually occurs during the TAVR procedure itself. While some case reports of delayed aortic dissection following TAVR have previously been described,5,6 this report is, to our knowledge, one of the first to describe a case of embolized transcatheter heart valve (THV) treated with deployment of a second valve that was complicated by type A aortic dissection. DeRoo et al describe a similar case in a 76-year-old woman who was found to have type A aortic dissection 4 days after implantation of a second valve. She underwent hemi-arch repair and aortic valve replacement. 7
Three primary approaches for managing THV embolization include repositioning, multiple valve implantation, and conversion to surgery. 8 Repositioning carries a heightened risk of aortic injury, especially when the valve's final position is distal to the left subclavian artery. 1 The implantation of a second prosthesis, such as in our patient, is a frequently used strategy, as it demonstrates high technical success rates and favorable outcomes.1,9 Valve-in-valve therapy has also been described with good hemodynamic outcomes, especially as a bail-out strategy for ventricular embolization, although associated with increased 30-day and 1-year mortality rates. 9
The current practice is to leave an embolized THV in the ascending aorta when it is stable.1-4,9,10 Indeed, reports have shown no further migration or complications in these cases at mid-term follow-up.11,12 Yet, a notable limitation in this series is the absence of immediate post-procedural CT for comparison with follow-up imaging. In terms of embolized THV devices in the aortic arch or the thoracic descending aorta, studies have shown that these tend to remain stable without migration, strut fractures, aortic complications, or thrombosis. However, some valves display leaflet degeneration.13,14 Conversely, some have found higher incidences of cardiac death and stroke associated with embolization at the 30-day mark. 9
The argument could be made that even with successful implantation of a second valve, surgical intervention to retrieve the migrated valve may be considered in selected cases, although further data are needed to support this approach. It is important to note that surgical retrieval of THV can be complicated by penetration into the aorta or annulus. Submerging a self-expandable valve into ice-cold saline has been shown to cause shrinkage of the metallic valve skeleton, facilitating extraction. 15
Conclusion
There remains a lack of consensus regarding the management of embolized THV and their surgical extraction when positioned non-anatomically within the aorta. Additional studies are needed to further evaluate the pertinence of surgical intervention for embolized THV in ectopic aortic positions to mitigate the risk of life-threatening aortic dissection.
Supplemental Material
Supplemental Material
Footnotes
Author's Statement
Patient consent for publication of this case report and its associated media was obtained.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.