Aortic Valve Reoperation With The Freestyle Bioprothesis Is Not Associated With Increased Perioperative Risks And Follow-up Mortality: A Single Center Retrospective Study
Authors:Patrick T. Timmermans, Alex Cotovanu, Adriaan Schneider, Mark Hazekamp, Nina Aijmone, Jerry Braun, Robert Klautz, Jesper Hjortnaes
LUMC, Leiden, Netherlands
Abstract Body:
Objective: This study examines the perioperative risks and long-term outcomes of aortic root reoperation compared to primary aortic root replacement using the Freestyle Stentless Bioprosthesis.
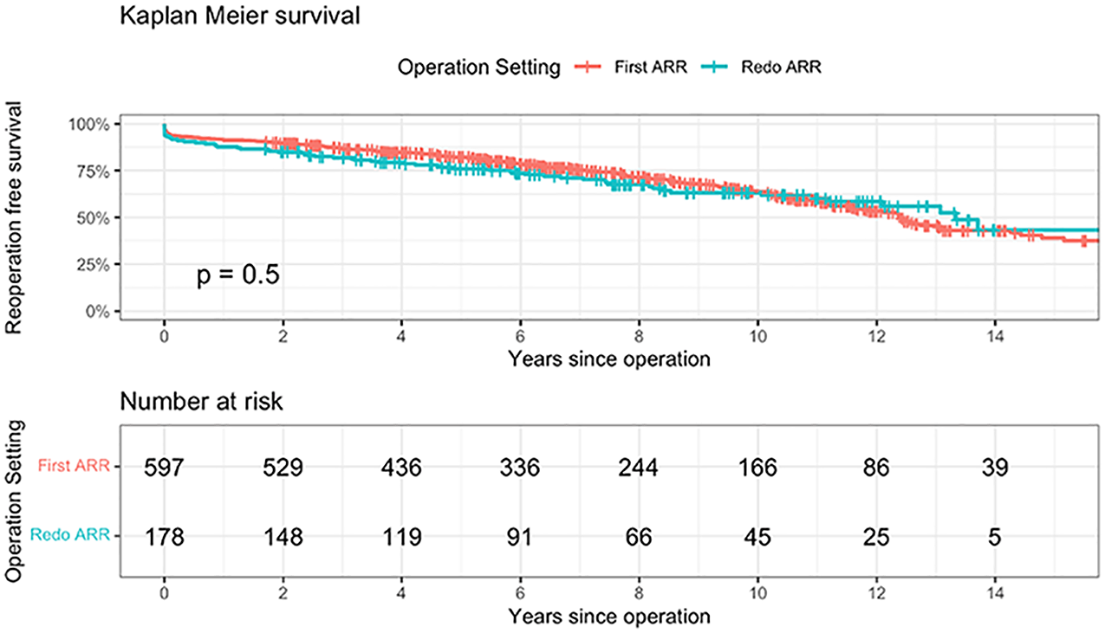
Methods: Data were collected from 775 unselected patients that underwent implantation of the Freestyle Stentless Bioprothesis at the Leiden University Medical Centre between 1993 and 2021 (80% since 2010). 187 (24%) of these patients had previous aortic valve or root replacement (Redo ARR). Perioperative and follow-up data were collected retrospectively. Survival status data was sourced from national registries, while reintervention status was retrieved from hospital medical records. Follow-up was 100% complete (median 7 years), with 234 patients exceeding 10 years. A Kaplan Meier analysis was performed to evaluate the mid- and long-term outcome differences between primary ARR and Redo ARR.
Results: There was no difference in age or sex between the two groups (p=0.95). Redo surgery was more often due to endocarditis (41.4% vs 9.6% in the primary ARR group), but less for acute type A aortic dissection (2.5% vs 16.6% in the primary ARR group, p<0.001). Surgical timing was more often urgent for Redo ARR (39.3% vs. 13.6%, p<0.001). Early mortality did not differ significantly between both groups (5.7% vs 7.3%). 30-day complication rates (including bleedings, CVA and dialysis) were comparable between both groups. The 1-, 5-, 10-, 15-, reintervention free survival for first time ARR was, respectively, 91%, 82%, 64%, 39%, comparable with Redo ARR, respectively, 88%, 76%, 63%, 43%.
Conclusions: Redo aortic root replacement using the Freestyle Stentless Bioprosthesis does not come with a higher perioperative risk compared to primary root replacement. In addition, long- term survival did not differ between groups and reoperation rates during follow-up were comparable.
Control Number: 24-A-57-HVS
Presentation Number: A3
Early Structural Valvular Deterioration of Bovine Pericardial Aortic Bioprosthesis
Authors:Kang Min Kim, MD, Joon Chul Jung, MD,PhD, Hyoung Woo Chang, MD,PhD, Jae Hang Lee, MD,PhD, Dong Jung Kim, MD,PhD, Jun Sung Kim, MD,PhD, Cheong Lim, MD,PhD, Kay-Hyun Park, MD,PhD
Seoul National University Bundang Hospital, Seongnam-si, Republic of Korea
Abstract Body:
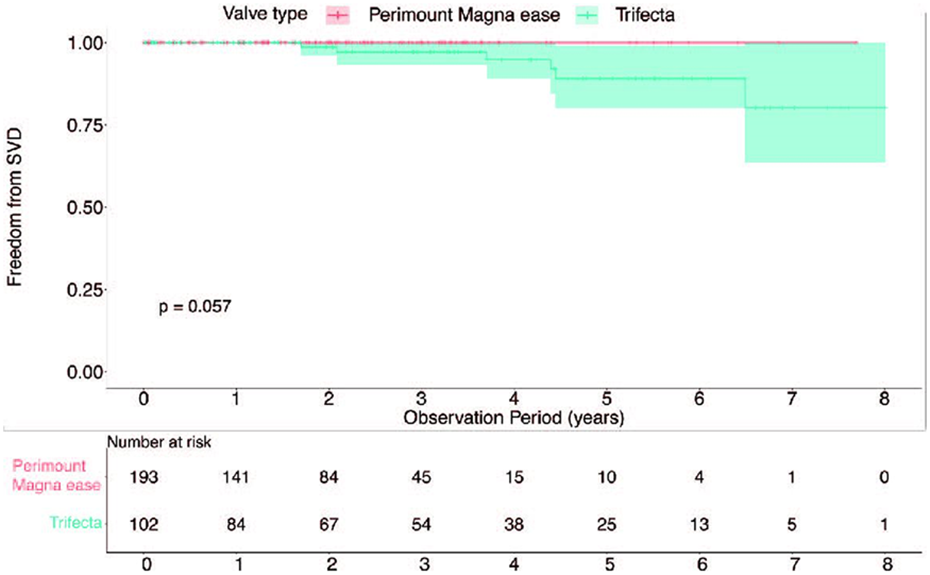
Objective: We aim to analyze the early structural valvular deterioration (SVD) rate occurring within 5 years after aortic valve replacement (AVR) using the Abbott Trifecta (TF) valve.
Methods: From 2015 to 2022, 641 patients underwent AVR. We analyzed the early SVD rate and hemodynamics in patients who underwent AVR using bovine pericardial valve with the Perimount Magna (PM) valve (n = 193) and the TF (n = 102) valve.
Results: There were 6 (5.9%) cases of SVD in the TF cohort, while there were 0 (0.0%) cases of SVD in the PM cohort during observational period. Out of the 6 cases, 5 were early SVD with a median interval of 4.0 [2.1; 4.4] years. The 5-year freedom from SVD for the TF cohort was 0.891 (95% CI: 0.800 to 0.991), whereas for the PM cohort, it was 1.000 (95% CI: 1.000 to 1.000) with a p-value from log-rank test of 0.057. Immediate postoperative mean systolic pressure gradient (MSPG) in the TF cohort was 8.9 ± 3.9 mmHg, which was significantly lower than the PM cohort's MSPG of 14.2 ± 5.1 mmHg (p < 0.001). This trend was consistent even when comparing the cohorts based on the size of the replaced valve.
Conclusions: TF valve exhibits more favorable hemodynamics compared to the PM valve. However, TF valve has a higher probability of experiencing early SVD within the first five years. Multi-center study is necessary to establish the early SVD rate of TF valve.
Control Number: 24-A-44-HVS
Presentation Number: A4
Early Outcomes of Aortic Valve Replacement Using a New Stented Pericardial Bioprostesis
Authors:Maria cannoletta, Ryan Mohamed, Anthony De Souza
Royal brompton hospital, london, United Kingdom
Abstract Body:
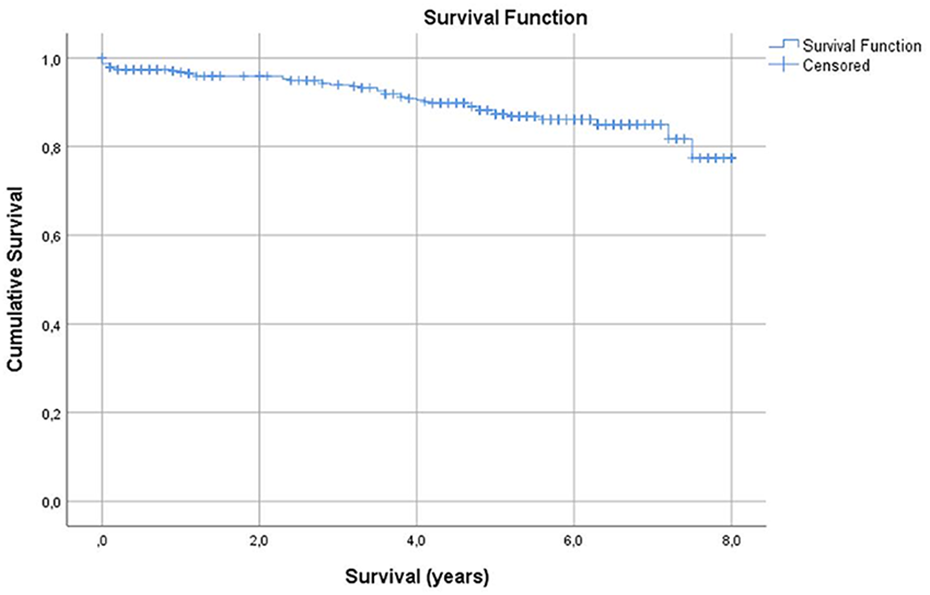
Objective: Development of stented bioprosthesis has been evolving through several decades to improve performance and durability. A new pericardial bovine valve has been recently approved and released. This was introduced in our institution in December 2018. We report our single institution early results in 164 patients.
Methods: The hospital cardiac surgery database (PATS & EPR) was retrospectively reviewed. Characteristics and outcomes, including mortality, post-operative complications together with echocardiographic findings are reported.
Results: Between December 2018 and July 2023 n=164 patients underwent aortic valve replacements and had an Avalus tissue valve implanted. Average Euroscore was 3.58, ventricular function was good in n=138 patients, moderate in n=21 patients, poor in n=5 patients. 4 over 164 patients underwent redo surgery. 87 patients had isolated AVR, the rest had concomitant procedures: n=37 CABG, n=4 mitral valve surgery, n=5 ascending aorta replacement, n=15 AF ablation. Size of valve sizes were: n=1 19mm, n=13 21mm, n=55 23mm, n=66 25mm, n=29 27mm, n=1 29mm. We had 4 in-hospital mortality not valve related, one case of re-exploration for bleeding and no valve related complications (thromboembolism, thrombosis, significant paravalvular leak, endocarditis, hemolysis, structural valve deterioration). All the patients had a pre-discharge echocardiogram which showed a mean gradient =11.2mmHg
Conclusions: Our short term experience with Avalus bioprosthesis demonstrated it to be a safe, with low mortality or valve related complications and good haemodynamic performance.
Control Number: 24-A-95-HVS
Presentation Number: A6
A Single-center Experience in Minimally Invasive Aortic Valve Surgery in Brazil
Authors:Elinthon Veronese, Carlos Manuel A. Brandão, Pablo Maria A. Pomerantzeff, Fabricio Dinato, Marcelo Luis C. Vieira, Flavio Tarasoutschi, Fabio B. Jatene
Heart Institute - University of São Paulo Medical School, São Paulo, Brazil
Abstract Body:
Objective: describe the experience in minimally aortic valve surgery in a cardiology specialized hospital.
Methods: between 2016 and 2023 we performed 62 minimally invasive aortic surgery by ministernotomy (MS) or minithoracotomy (MT) approach. Inclusion criteria was low-risk adult patients with indication of elective isolated aortic valve surgery. Exclusion criteria were: urgency/emergency status, severe left ventricular dysfunction (<30%), redo procedures, previous atrial fibrillation and anatomic abnormalities of the chest. A preoperative chest computed tomography was used to the definition of surgical approach, according to the dextroposition and depth of the aorta.
Results: mean age was 40.8 years and 72.6% of patients were male. Aortic stenosis and mixed disease consisted of 54.8% valvular lesions. Congenital (40.3%) and Rheumatic (37.1%) were the main etiology. About 54.8% of patients were in NYHA functional class I-II. Mean EuroSCORE2 was 0.71 and STS Score 0.65. MS was the approach in 55 patients (88.7%). Mean surgery time was 310 minutes, cardiopulmonary bypass time was 110 minutes and aortic cross clamp time was 75 minutes. Bioprosthesis was the choice in 77.4%. Intraoperative blood loss was 348mL and 24h drainage was 210mL. Requirements of blood transfusion was 9.7% during hospitalization. One patient (1.6%) required reoperation for bleeding. One patient (1.6%) died because of vasoplegic syndrome. No neurologic or vascular complications were observed. Using numeric scale, mean incision pain was 3.7 in the first postoperative day and 1.4 at the discharge. Mean ICU and hospital length of stay was 67.4 hours and 8.6 days, respectively.
Conclusions: in our experience, even in rheumatic etiology and advanced NYHA functional class, minimally invasive aortic surgery in low risk patients is safe with low incidence of postoperative complications and/or requirement of blood transfusion.
Control Number: 24-A-49-HVS
Presentation Number: A7
Early and Midterm Outcomes of Three-dimensional Virtual Reality Evaluation of the Aortic Root Configuration in Aortic Valve Leaflet Reconstruction with Three Same-sized Autologous Pericardial Leaflets
Objective: Aortic valve leaflet reconstruction with autologous pericardium is an option for aortic valve surgery. We have performed a unique technique of aortic valve leaflet reconstruction using three same-sized autologous pericardium leaflets (ATLAS). We had introduced a three dimensional-virtual reality (3D-VR) workstation to clarify physio-anatomical details of the aortic root to enhance reproducibility of this technique. We evaluated early and midterm outcomes of ATLAS procedure with 3D-VR image analysis as well as echocardiogram.
Methods: Basic technique; 1) autologous pericardium treated by 0.6 % are tailored to a template referred by the STJ diameter, 2) new commissures and nadirs were confirmed, 3) tailored leaflets are sutured to the annulus by continuous stitching, 4) commissure coaptation stitches between each leaflet were placed, 5) STJ is fixed by pericardial stripe. Enrolled patients underwent ECG-triggered cardiac CT to obtain 3D-VR image of the aortic root configuration. We evaluated trans-thoracic echocardiography results one month and six months, then in every year
Results: In 2016, ATLAS were performed in 42 patients (AS=19, AR=18, active IE=5). In 14 patients, 3D-VR analysis revealed unbalanced aortic annuls, which required additional procedures. Postoperative analysis showed appropriate correction of the aortic root. One patient died by sepsis of preoperative active IE. One redo AVR was required due to perforation of one leaflet. Echocardiographic evaluation revealed no aortic leaflet problem with minimum pressure gradient in maximum follow-up of 6.5 years.
Conclusions: ATLAS can provide a simple and reproducible procedure that allows anatomical physiologic correction of the aortic valve. Early and midterm outcomes were acceptable for aortic valve surgery, although further strict follow up should be necessary.
Control Number: 24-A-92-HVS
Presentation Number: A8
8-year Single Center Experience with a Rapid Deployment Bioprosthesis in Bicuspid and Tricuspid Aortic Valve Pathology: Follow-up in 383 Patients
Authors:Romy R. Hegeman1, Idserd Klop1, Geoffrey Kloppenburg1, Bart van Putte1, Patrick Klein2
1St. Antonius Hospital, Nieuwegein, Netherlands, 2Amsterdam UMC, Amsterdam, Netherlands
Abstract Body:
Objective: Rapid deployment bioprostheses (RDBP) enable faster valve implantation in surgical aortic valve replacement (SAVR), but are associated with increased pacemaker risk and can be challenging to implant in pure bicuspid aortic valves (BAV). We aimed to evaluate the outcome of RDBP in bicuspid and tricuspid aortic valves.
Methods: Between May 2015 and May 2023, all consecutive patients who underwent isolated or combined SAVR with an RDBP were retrospectively included. Early and late outcomes were assessed.
Results: A total of 383 patients (mean age 72±6 years; 55% male) who underwent SAVR with the use of an RDBP were included. Overall survival was 89% at 8 years. Minimally invasive SAVR was associated with significantly lower in-hospital mortality (p=0.011), while there was no difference in overall survival up to 8 years (p=0.838). Twelve patients (3%) had to undergo a reintervention of the aortic valve (9 (75%) for PVL closure, 2 (17%) for endocarditis and 1 (9%) for structural valve deterioration respectively), of whom 8 patients (67%) had BAV pathology (p=0.008). Significantly less patient prosthesis mismatch (PPM) occurred in patients with BAV compared to patients with a tricuspid valve (p< 0.001). Type of BAV pathology did not influence the incidence PPM (p=0.907). Both calculated moderate and severe PPM did not influence survival (p=0.834 and p=0.414 respectively) and neither did small valve size (p=0.751). Permanent pacemaker implantation occurred in 8.4%, but was not influenced by the presence of BAV (p=0.847).
Conclusions: The use of an RDBP in SAVR is associated with excellent long-term survival and freedom from reinterventions. It especially facilitates minimally invasive SAVR approaches, without compromising early risk or late outcome. Although BAV pathology is a risk factor for reintervention, it is also associated with less PPM and equal risk of permanent pacemaker implantation.
Control Number: 24-A-63-HVS
Presentation Number: A9
In-hospital and 1-year Outcomes of Transcatheter Aortic Valve Replacement Patients Requiring Emergent Conversion to Cardiac Surgery
Authors:Mohiuddin Cheema, Raymond Mckay, Eduardo Perez
Hartford Hospital, Glastonbury, CT, USA
Abstract Body:
Objective: Despite increasing operator experience, improved imaging and advanced device technology resulting in an improved safety profile for transcatheter aortic valve replacement (TAVR), a small percentage of patients require emergent conversion to cardiac surgery to treat life-threatening intraprocedural complications. We sought to determine the incidence, etiology and clinical impact of surgical bailout in a high-volume TAVR program
Methods: From a total cohort of 2,931 TAVR patients treated since 2012, we compared in-hospital and 1-year clinical outcomes in 23 patients requiring emergent conversion to open heart surgery (OHS group) versus 2,908 patients not requiring surgical bailout (non-OHS group). All procedures were performed with either balloon-expandable or self-expanding TAVR valves in a hybrid operating with immediate cardiac surgery availability
Results: OHS and non-OHS patients were well matched with respect to baseline demographics, cardiac risk factors, comorbidities, pre-TAVR cardiac catheterization and echocardiographic testing, and STS Risk Score (10.4 ± 7.1 vs 9.2 ± 7.3, p=0.458). OHS procedures more commonly required non-femoral alternative access (30%% vs 12%, p=0<0.001) with general anesthesia (48% vs 35%, p=0.001), and more commonly employed balloon-expandable as opposed to self-expanding TAVR valves (78% vs 61%, p=0.032). OHS (n=23) and Non-OHS (n=2908) p Value for In-Hospital Outcomes: Procedural Cardiac Arrest 5 (21.7%) versus 29 (1.0%) (p<0.001), Mortality 11 (47.8%) versus 33 (1.1%) (p<0.001), Ischemic Stroke 2(8.7%) versus 42 (1.4%) (p=0.004). 1-Year Outcomes: Mortality 8 (34.8%) versus 397 (13.7%) (p=0.009), and Hospital Readmission 0 (0.0%) versus 117 (4.0%) (p=1.000).
Conclusions: The need for TAVR surgical bail-out is infrequent, but is associated with high rate of in-hospital mortality and stroke and poor 1-year survival.
Control Number: 24-A-113-HVS
Presentation Number: A10
In-hospital and Long-term Outcomes of Transcatheter Aortic Valve Replacement in Patients with Peripheral Arterial Disease
Authors:Mohiuddin Cheema, Eduardo Perez, Jawad Haider, Raymond Mckay, Sabet Hashim
Hartford Hospital, Hartford, CT, USA
Abstract Body:
Objective: Peripheral arterial disease (PAD) is common in patients treated with transcatheter aortic valve replacement (TAVR) and is a marker for increased in-hospital and intermediate adverse outcomes. We sought to determine the long-term follow-up of TAVR PAD patients.
Methods: We compared in-hospital and late outcomes of 650 PAD patients versus 2,271 no-PAD patients undergoing TAVR since 2012
Results: In comparison to the No-PAD cohort, PAD patients were more likely male (61% vs 52%, p=0.001), had more cardiovascular risk factors including hypertension (93% vs 89%, p=0.002), diabetes (39% vs 33%, p=0.002), and tobacco use (27% vs 20%, p=0.001), and had more comorbidities including prior myocardial infarction (36% vs 20%, p=0.001), prior stroke (16% vs 9%, p=0.001), COPD (48% vs 36%, p=0.001) and ESRD requiring dialysis (4% vs 2%, p=0.007). These clinical characteristics translated into a higher STS Risk Score for PAD patients (11.1±7.5% vs 8.7±7.1%, p<0.001).
PAD patients require higher use of non-femoral alternative access (36% vs 5%, p=0.001) with greater use of general anesthesia (57% vs 29%), p=0.001). There was similar use of balloon-expandable TAVR valves (59% vs 60%) and newer generation valves (69% vs 71%) in the two cohorts.
The PAD cohort had a higher incidence of death (2.5% vs 1.2%, p=0.025), major vascular complications (3.6% vs 1.5%, p=0.001), post-TAVR TIA (0.6% vs 0.04%, p=0.002), and post-TAVR atrial fibrillation (2.6% vs 1.2%, p=0.018), with no differences regarding stroke or need for permanent pacemaker. PAD patients had a longer post-TAVR hospital length of stay (4.0±5.9 vs 2.5±3.4 days, p<0.001).
Kaplan-Meier survival curves for the two cohorts demonstrated that all-cause mortality for the PAD cohort was significantly worse with an overall mean (95% CI) survival time of 70.2 (64.3-76.1) months, p=0.005.
Conclusions: TAVR patients with PAD represent a high-risk patient subgroup with increased in-hospital mortality and morbidity, and worse long-term surviva
Control Number: 24-A-75-HVS
Presentation Number: AA1
Can Perceval Sutureless Aortic Valve Help Closing the Gender Gap in Aortic Valve Replacement?
Authors:Delphine Szecel, Marie Lamberigts, Peter Verbrugghe, Christophe Dubois, Bart Meuris
UZ Leuven, Leuven, Belgium
Abstract Body:
Objective: Poorer outcomes after surgical aortic valve replacement (SAVR) in females have been described when compared to males. High risk profile, small aortic annulus, higher gradient and delayed referral seems to influence outcomes. On contrary, a survival advantage in females has been described after TAVR. We aimed to look at the potential benefits of Perceval sutureless prosthesis in SAVR in female patients.
Methods: Our cohort includes 349 patients of whom 217 females who underwent an isolated SAVR using a Perceval sutureless valve between 2007 and 2019. We performed a retrospective analysis comparing perioperative factors and outcomes according to the patient gender. Standard T-tests, Chi-square and Fisher exact testing were used.
Results: The mean age was 78.52 years (± 5.8). Demographics data did not differ between the two groups except for body surface area (BSA) (1.98 in males versus 1.77 in females, p < 0.001), smoking history (48% in males versus 9% in females, p < 0.001) and preoperative kidney impairment (1.27% in males versus 1.03% in females, p < 0.001). The mean Euroscore II was 3.79% (± 3.5) and was not significantly different. Mean cross clamp time and cardiopulmonary bypass were respectively 40.38 (± 15.97) and 65.26 minutes (± 24.55). Patient prosthesis mismatch (moderate or severe) was not different (49.5% versus 55.3%, p = 0.334) nor were the in-hospital mortality (1.51% versus 1.38%, p = 1) and the 1-year survival (94.7 versus 93.6, p = 0.662).
Conclusions: In conclusion, poor outcomes in females after SAVR is not a fate. We observed low in-hospital mortality in males as well as in females. No difference was found in patient prosthesis mismatch. SAVR using Perceval sutureless aortic valve is a safe option in women. Minimal invasive surgery availability might lower the threshold to surgery for women. Gender bias should be taken into account in prospective studies.
Control Number: 24-A-31-HVS
Presentation Number: AA2
The First Experience of Using a "sutureless" Perceval S Prosthesis in a Combined, Hybrid Operation: Aortic Valve Replacement, with Coronary Bypass Grafting Through Mini-thoracotomy Access and Coronary Artery Stenting
RSSPMCS named after Academician V. Vakhidov, Tashkent, Uzbekistan
Abstract Body:
Objective: The aim of the study is to present a clinical case of using a "sutureless" prosthesis Perceval S in a simultaneous, hybrid operation: aortic valve replacement, with coronary bypass grafting through mini-thoracotomy access and coronary artery stenting.
Methods: Patient O. aged 53, with a diagnosis of combined aortic defect with a predominance of stenosis. Competing diagnosis: IHD. Angina pectoris FC III. Complication: CHF stage II B, NYHA FC IV. Mitral valve insufficiency II grade. According to the EuroScore II scale the risk is 11.2%. Echocardiography: EDV 184 ml, EF 30%, AV - severe fibrosis and calcification. The diameter of the annulus fibrous of AV is 1.9 cm. Systolic pressure gradient 85 mmHg. AR I grade. MR II grade. According to CAG: RCA occlusion of the proximal third. LAD - 70% stenosis of the middle third. LCX was unchanged. The right dominant coronary blood supply.
Results: An infusion of levosimendan was given preoperatively, the day before surgery. First, a distal anastomosis of the vein graft with the RCA imposed. Then biological AV prosthesis Perceval S №21 was implanted. EC time - 43 min, aortic cross-clamping time - 24 min, total operation time 240 min. After that, the patient transported to the angiographic laboratory, where direct LAD stenting was performed. The patient extubated after 18 hours, and the time spent in the ICU was 42 hours. The course of the postoperative period proceeded relatively smoothly. On the control, Echocardiography (7th-day p/o): EDV - 123 ml, EF - 45%, peak gradient of AV was 12 mm Hg. MR I grade. The patient discharged on the 9th day after the operation.
Conclusions: The chosen method made it possible to reduce the time of surgical intervention, and reduce the volume of surgical trauma, which in turn significantly reduces the risk of fatal complications.
Control Number: 24-A-13-HVS
Presentation Number: AA3
Comparison of Hemodynamic Performance Under Stress Echocardiography Between Stentless Solo Smart and Sutureless Perceval S
Authors:María Sol Siliato Robles, José Carlos Sureda Barbosa, Neiser Eduardo Palmer Camino, Remedios Ríos Barrera, Miguel Ángel Castro Alba, Mehrdad Moradi Kolbolandi, Carlota Vigil-Escalera López, Mario Contreras Godoy, Mohamed Cherif Traore Kone, Marta Magaly Paguay Fernandez, Rafael Rodríguez Lecoq
Vall d'Hebron Hospital, Barcelon, Spain
Abstract Body:
Objective: Hemodynamic performance of prosthesis after aortic valve replacement can determine a small effective orifice area and this can produce a continuity of aortic stenosis symptoms. We compare the hemodynamic profile between two different bioprosthesis.
Methods: From February 2018 until March 2021, we have randomized 48 female patients over 70 years old, with aortic valve replacement. We have created two groups, one (group S) received a Sorin Solo Smart stentless valve while the other (group P) received a sutureless Sorin Perceval S valve. We have performed rest echocardiography prior to hospital discharge and rest and exercise stress echocardiography in a mean follow-up time of 9.8 months. The main endpoint of this study was to compare the hemodynamics of both prosthesis while exercise.
Results: Patients in both groups presented similar sociodemographic characteristics. The sutureless bioprosthesis Sorin Perceval S was confirmed to have a faster implantation with shorter cardio-pulmonary bypass and cross clamp times (p< 0.001). The patients in the Sorin Perceval S group received smaller bioprosthesis (P<0.01). Sorin Solo Smart presented better mean transvalvular gradient in the postoperative period and also in the mid-term follow up at rest and stress echocardiography (p<0.05).
Conclusions: This single-center prospective randomized study demonstrated that Sorin Solo Smart has better hemodynamic performance than Sorin Perceval S in this selected group of patients in a mid-term follow up. However, Sorin Perceval S is faster to implant. The decision of implanting one or other bioprosthesis should be made taking into account patients’ comorbidities and the need of concomitant surgery.
Control Number: 24-A-43-HVS
Presentation Number: AA4
Totally Endoscopic Aortic Valve Replacement in Patients Rejected for Transcatheter Aortic Valve Implantation
Authors:Silke Van Genechten, Loren Packlé, Jade Claessens, Alaaddin Yilmaz
Jessa Hospital, Hasselt, Belgium
Abstract Body:
Objective: Transcatheter aortic valve implantation (TAVI) is a valuable technique to replace a severely stenotic aortic valve in high-risk and inoperable patients. Still, some patients are rejected for TAVI because of their comorbidities, frailty, or technical non-suitability, leaving them with no other treatment options. Due to its low invasiveness, totally endoscopic aortic valve replacement surgery (TEAVR), might form a serious alternative for this subset of patients. Therefore, the aim of this study is to investigate the clinical feasibility of TEAVR in patients who were deemed unsuitable for TAVI.
Methods: This single-center retrospective study included 30 patients who were considered ineligible for TAVI, undergoing isolated TEAVR from January 2020 until June 2023. All procedures were performed totally endoscopically using three 5 mm trocars and a 2 cm working port.The primary endpoints consisted of parameters for surgical success: i.e. postoperative paravalvular leakage and permanent pacemaker implantation. Secondary endpoints included peri-operative parameters, including aortic cross-clamping and cardiopulmonary bypass times and bleeding.
Results: A permanent pacemaker was implanted in two (6.67%) patients, while paravalvular leakage was not seen during echocardiographic follow-up. One (3.33%) patient suffered a cardiac death and two (6.67%) patients suffered from a stroke. Cardiopulmonary bypass and aortic clamping times consisted of 85 [67;96] and 56 [41;64] minutes, respectively. Patients were ventilated for a median of 3.5 [2;14.6] hours. Peri-procedural blood loss was only 300 [236.5;665.8] mL, while postoperative blood loss for 24 hours was 212.5 [100;390] mL. Moreover, patients remained at the intensive care unit and hospital for a median of 67.5 [23.88;109.23] hours and 7 [5;9.75] days, respectively.
Conclusions: In conclusion, TEAVR appears to be a feasible technique for patients who were rejected for TAVI, showing permanent pacemaker implantation- and paravalvular leakage rates comparable to open surgery. More research is necessary to extrapolate our TEAVR results to general practice.
Control Number: 24-A-80-HVS
Presentation Number: AA5
Partial Sternotomy as the Possible New Gold Standard for Aortic Valve Surgery
Authors:Ali Shadmanian, Antal Szabó-Bicók, István Gecse, Csenge P. Csanádi, Szilárd Szűcs, Márkó Kovacev, Miklós Bitay
University of Szeged, Szeged, Hungary
Abstract Body:
Objective: In this retrospective study, we aim to report our results on aortic valve and major aortic surgery performed through partial sternotomy, compared with a matched group of patients operated through full sternotomy.
Methods: Between 2013 and 2016, 163 consecutive patients (group A) operated through partial sternotomy were compared with 315 propensity matched patients operated through full sternotomy (B). The patients’ mean age was 68 and 67 years, respectively. The mean ejection fraction was above 50% in both groups and the incidence of comorbidities was also similar. In group A, 79% of the procedures were aortic valve replacements (AVR) and 21% were major aortic interventions (modified Bentall , ascending aorta replacement, valve sparing root replacement, aortic valve repair, homograft implantation, Ross procedure). The partial sternotomy was either “J” (25%), or “arrow” (75%) shaped, to the 3rd intercostal space. In group B, 79% were AVR operations, 21% were major aortic interventions.
Results: The 30 day mortality in group A was lower than in group B (0.6% vs. 2.9%, P=0.19), as well as the incidence of postoperative neurological complications (1.2% vs. 3.2%, P=0.32) and the incidence of postoperative dialysis (1.8% vs. 3.8%, P=0.37), but the differences were statistically not significant. There were significant differences between cardiopulmonary bypass time (A: 94.24 min vs. B: 105.82 min, P=0.013) and cross-clamping time (A: 61.53 min vs. B: 76.08 min, P=0.0001)
Conclusions: The partial sternotomy approach offers the possibility of safely performing all types of interventions involving the aortic valve, root, and ascending aorta. These aspects, coroborated with publications on the non-inferiority of the partial sternotomy approach compared to the full sternotomy, makes us consider the partial sternotomy as the new gold-standard approach for aortic valve surgery.
Control Number: 24-A-78-HVS
Presentation Number: AA6
Risk Factors Associated with Adverse Outcomes for Sternal Re-entry for Surgical Aortic Valve Replacement
Authors:Philemon Gukop, Pouya Youssefi, Justin Nowell, Robin Kanagasabay, Rajan Sharma, Marjan Jahangiri
St George's University hospital NHS London, London, United Kingdom
Abstract Body:
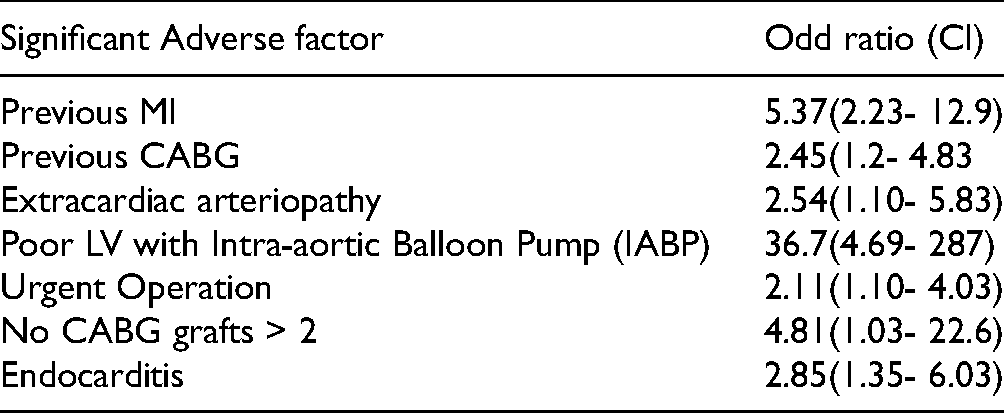
Objective: 1. Sternal re-entry for surgical Aortic Valve Replacement(AVR) is associated with significant morbidity and mortality upto 10%.2.To mitigate this risks we identify factors associated with adverse outcomes during sternal re-entry for Aortic valve replacement (AVR).
Methods: Retrospective data analysis on 178 consecutive patients who had sternal re-entry for AVR in a single centre between 2010 to 2018. Univariate and multivariate regression analysis of significant variables that predict death was done. Significant Results presented as hazard ratio and Kaplan-Meier’s survival curves.
Conclusions: Factors associated with adverse outcomes for sternal re-entry for AVR include previous CABG, Extracardiac arteriopathy, Impaired LV with IABP, urgent operation, Endocarditis. This data could guide Careful patient selection and information to improve outcomes
Control Number: 24-A-172-HVS
Presentation Number: AA7
Intra-patients Variability of Mechanical and Anatomical Properties in Dilated Aortic Wall: An Ex Vivo Study Comparing Patients with Bicuspid and Tricuspid Aortic Valve
1Cardiac Surgery IRCCS Foundation San Matteo, Pavia, Italy, 2Department of Electrical, Computer and Biomedical Engineering - University of Pavia, Pavia, Italy, 3Deparment of Civil Engineering and Architecture - University of PAVIA, Pavia, Italy
Abstract Body:
Objective: Ex-vivo evaluation of aortic wall specimen from dilated aorta has been popularized in order to detect potential predictive risk factors of acute aortic syndrome. Previous studies focused on the comparison between patients with bicuspid and tricuspid aortic wall showed significant intra-patient variability. Here we investigated the significance of intra-patient variability of anatomical and mechanical properties of aortic wall comparing patients with bicuspid or tricuspid aortic valve.
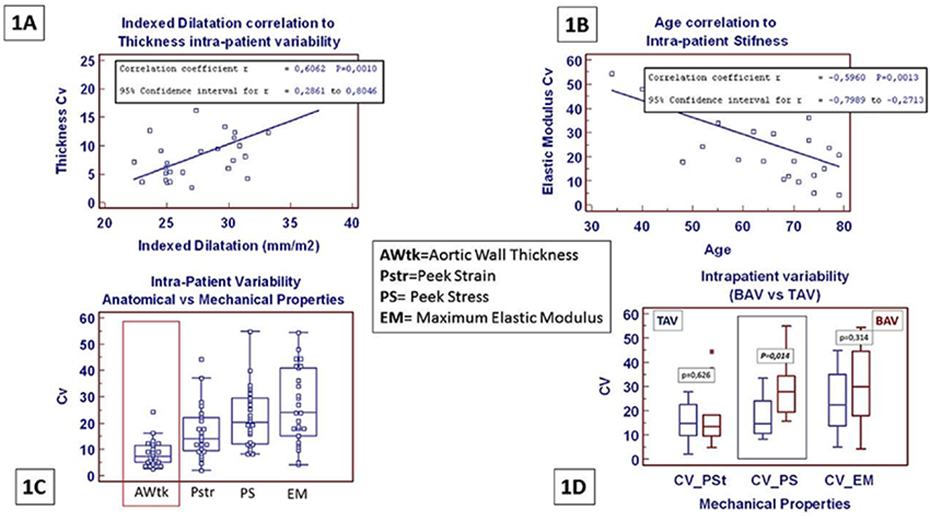
Methods: Out of 238 patients undergoing elective surgery of ascending aorta, 94 were enrolled for aortic wall harvesting and mechanical test (ultimate uniaxial tensile test). 26 patients, with >3 specimens obtained, were enrolled in the intra-patient variability study. Intra-patient variability was assed, using the coefficient of variability (cV= standard deviation/mathematical mean*100), in regard of aortic wall thickness, peek stress, peek strain and maximum elastic modulus. Results were compared between patients with bicuspid aortic valve (10 pts - BAV) and patients with tricuspid aortic valve (16 pts - TAV).
Results: Overall cV of aortic wall thickness was correlated to the extent of aortic dilatation (1A) while overall cV of aortic wall stiffness was reversly correlated to the patients age (1B). Mechanical properties showed higher variability than aortic thickness (1C). BAV vs TAV comparison, furthermore showed that the average of cV of peak stress (marker of aortic wall strength) was significantly increased in BAV patients compared to TAV patient (1D). No significant differences were shown in BAV vs TAV comparison in respect to cV of aortic wall thickness.
Conclusions: Our study shows that aortic wall characteristics in patients with aortic dilatation are not homogeneous. Intra-patient variability is more significant in mechanical properties than in aortic wall thickness. Variability of mechanical properties furthermore seems to be more pronounced in patients with BAV compared to TAV.
Control Number: 24-A-42-HVS
Presentation Number: AA8
The Effect of BMI on the Clinical Outcomes after Endoscopic Aortic Valve Replacement
Authors:Jade Claessens, Loren Packle, Silke Van Genechten, Alaaddin Yilmaz
Jessa Hospital, Hasselt, Belgium
Abstract Body:
Objective: In recent years, the incidence of obesity has become a major concern. Referrals for cardiac surgery of these patients have consistently increased, highlighting the need to optimize strategies for qualitative and efficient care. Totally endoscopic aortic valve replacement (TEAVR), a new minimally invasive technique, could be beneficial for obese patients.
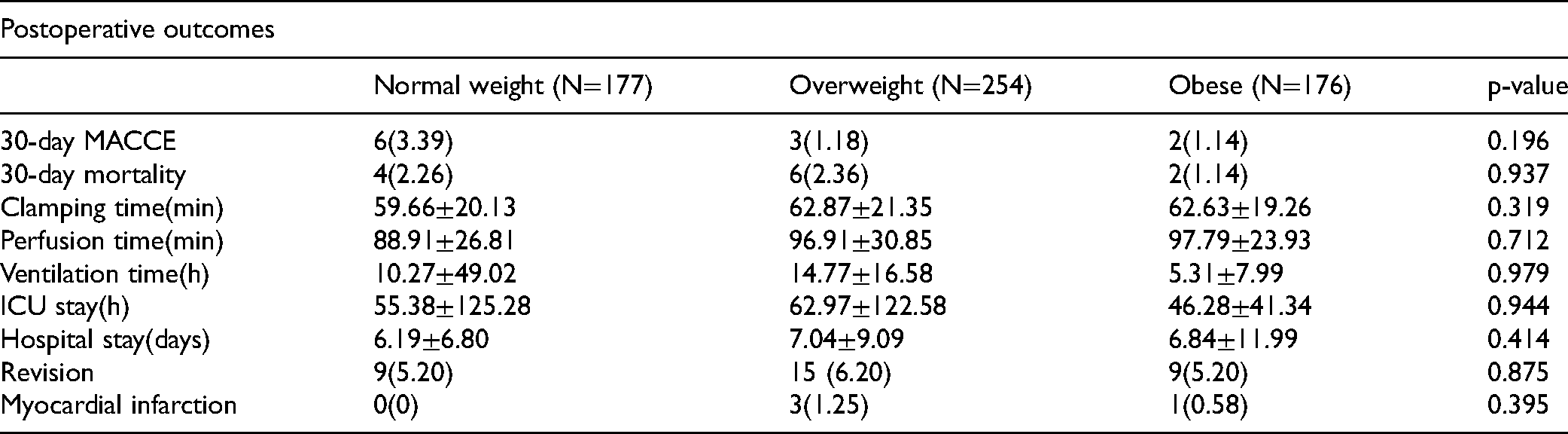
Methods: Our objective was to retrospectively investigate the possible adverse effects of body mass index on the clinical outcomes after TEAVR. There were 614 patients, that underwent TEAVR between October 2017 and June 2023. Aortic access is gained by a 20 mm working port in the 2nd intercostal space and three 5mm trocars in the 2nd and 3th intercostal spaces. No preoperative computed tomography scan was made for patient selection hence all patients can be included for TEAVR. The patients were subsequently divided into five subgroups based on their body mass index (<18.5kg/m2: underweight,n=7; 18.5-24.99kg/m2: normal,n=177; 25-29.99kg/m2: overweight,n=254; >30kg/m2: obese,n=176). There were only seven patients with underweight, so these were left out of the analysis. The primary outcomes were major adverse cardiac and cerebrovascular events (MACCE) within 30 days after the surgery and 30-day mortality.
Results: Both the 30-day MACCE and 30-day mortality did not significantly differ between normal weight, overweight and obese patients. Moreover, the postoperative outcomes such as intensive care unit length of stay, ventilation time, hospital length of stay, revisions, blood loss, pacemaker implantation, myocardial infarction, and atrial fibrillation did not differ significantly.
Conclusions: In conclusion, BMI does not affect any postoperative parameters after TEAVR. Accordingly, the risk factor obesity does not induce worse outcomes. It can be stated that TEAVR is a good option for obese patients.
Postoperative outcomes
Normal weight (N=177)
Overweight (N=254)
Obese (N=176)
p-value
30-day MACCE
6(3.39)
3(1.18)
2(1.14)
0.196
30-day mortality
4(2.26)
6(2.36)
2(1.14)
0.937
Clamping time(min)
59.66±20.13
62.87±21.35
62.63±19.26
0.319
Perfusion time(min)
88.91±26.81
96.91±30.85
97.79±23.93
0.712
Ventilation time(h)
10.27±49.02
14.77±16.58
5.31±7.99
0.979
ICU stay(h)
55.38±125.28
62.97±122.58
46.28±41.34
0.944
Hospital stay(days)
6.19±6.80
7.04±9.09
6.84±11.99
0.414
Revision
9(5.20)
15 (6.20)
9(5.20)
0.875
Myocardial infarction
0(0)
3(1.25)
1(0.58)
0.395
Control Number: 24-A-11-HVS
Presentation Number: AA9
Simple Echocardiographic Scoring in Screening Aortic Stenosis with Focused Cardiac Ultrasonography in the Emergency Department
Authors:Pierpaolo Maietta
Aorn Moscati, Aversa, Italy
Abstract Body:
Objective: No established methodology exists for diagnosis of aortic stenosis (AS) using focused cardiac ultrasound (FOCUS). We evaluated the diagnostic accuracy of our developed visual AS score for screening AS in an emergency department.
Methods: Seventy-two emergency outpatients with suspected cardiovascular disease were studied. Emergency physicians assessed the visual AS score in addition to conducting the standard FOCUS, and then the aortic valve area index (AVAI) was measured by expert sonographers in the echocardiography laboratory. AVAI values >0.85 cm2/m2, 0.6-0.85 cm2/m2, and <0.6 cm2/m2 were defined as no or mild AS, moderate AS, and severe AS, respectively.
Results: Seventeen (24%) patients had moderate or severe AS. Visual AS scores assessed by emergency physicians and by expert sonographers showed excellent agreement (κ = 0.93), and a strong association was noted between the visual AS score assessed by emergency physicians and the AVAI assessed by expert sonographers (R = -0.71, p < 0.0001). A visual AS score ≥3 assessed by emergency physicians had a sensitivity of 82%, specificity of 100%, positive predictive value of 100%, and negative predictive value of 95% for diagnosing moderate or severe AS. The prevalence of new-onset AS-related events during hospitalization was higher in patients with visual AS score ≥3 assessed by emergency physicians than in the remaining patients [7 (50%) vs. 2 (3%), p < 0.0001].
Conclusions: The visual AS score is a useful AS screening tool for emergency physicians who are not expert cardiologists.
Control Number: 24-A-9-HVS
Presentation Number: AA10
Examining Lack of Referrals to Heart Valve Specialists as Mechanisms of Potential Underutilization of Aortic Valve Replacement
Authors:Muhammad Etiwy1, Laura D. Flannery2, Shawn X. Li3, Fritha J. Morrison4, Joonghee Kim4, Varsha Tanguturi4, Chiara Fraccaro5, Megan Coylewright6, Alexander Turchin7, Sammy Elmariah3, Jason H. Wasfy4
1Dartmouth-Hitchcock Medical Center, Lebanon, NH, USA, 2OhioHealth Doctors Hospital, Columbus, OH, USA, 3University of California-San Francisco, San Francisco, CA, USA, 4Massachusetts General Hospital, Boston, MA, USA, 5University of Padua Medical School, Padua, Italy, 6Erlanger Health System, Chattanooga, TN, USA, 7Brigham and Women's Hospital, Boston, MA, USA
Abstract Body:
Objective: This study sought to investigate factors associated with referrals of patients with symptomatic severe aortic stenosis (AS) to Heart Valve Specialists (HVS) and better understand the potential role of a lack of referral on Aortic Valve Replacement (AVR) underutilization.
Methods: We identified patients with severe AS defined as aortic valve area ≤ 1.0 cm2 between 2015 to 2018, who met class I indication criteria for intervention outlined in the 2014 AHA/ACC guidelines. Baseline clinical characteristics, process-related parameters, and provider-reported reasons for non-referral to HVS were collected. Additionally, we examined predictors for referral, and assessed outcomes.
Results: We included 981 patients with a class I indication for AVR. Among them, 790 patients (80.5%) were assessed by HVS within six months of their index transthoracic echocardiogram (TTE). Factors linked to reduced referral rates included increasing age (OR: 0.95; 95% CI: 0.94-0.97; P <0.001), being unmarried (OR: 0.59; 95% CI: 0.43-0.83; P =0.002), and having an inpatient index TTE (OR: 0.27; 95% CI: 0.19-0.38; P <0.001). Conversely, higher hematocrit (OR: 1.13; 95% CI: 1.09-1.16; P <0.001) and eGFR (OR: 1.01; 95% CI: 1.00-1.02; P =0.003), along with higher mean aortic valve gradient (OR: 1.03; 95% CI: 1.01-1.04; P <0.001) and preserved LVEF (OR: 1.59; 95% CI: 1.02-2.48; P =0.04), were associated with increased referral likelihood. Moreover, patients assessed by HVS had better two-year survival rates than those who were not (62.8% vs. 18.3%; aHR: 0.133; CI: 0.09 - 0.19; P <0.001).
Conclusion: A substantial proportion of severe AS patients meeting indications for AVR are not evaluated by HVS within six months and therefore experience markedly increased mortality. Research is warranted to assess the efficacy of care delivery mechanisms, including registries, automated alerts, e-consults, and telemedicine, to improve access to HVS expertise beyond relying solely on traditional referrals.
Control Number: 24-A-82-HVS
Presentation Number: AP3
Ten-year Bioprosthetic Valve Failure-free Survival after Aortic Root Replacement with a Stentless Xenograft
Authors:Hanna H. Dagnegård1, Gustav H. Thyregod1, Christoffer Wallén2, Solveig M. Kolseth3, Natalie Glaser4, Ismail El-Hamamsy5, Jørgen B. Vennemo3, Kristjan O. Vidisson6, Kirstine Bekke1, Jan B. Valentin7, Ulrik Sartipy8, Rune Haaverstad3, Farkas Vanky2, Laurence Lefebvre5, Tomas Gudbjartsson6, Søren P. Johnsen9, Jens T. Lund10, Morten H. Smerup1, Nikolaj Ihlemann1
1Rigshospitalet, University Hospital of Copenhagen, Copenhagen O, Denmark, 2Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden, 3Haukeland University Hospital and University of Bergen, Bergen, Norway, 4Department of Cardiology, Södersjukhuset, Stockholm, Sweden, 5Montreal Heart Institute, University of Montreal, Montreal, Quebec, Canada, the aortic centre, Montreal, QC, Canada, 6Landspítali, University Hospital, Faculty of Medicine, University of Iceland, Reykjavik, Iceland, Reykjavik, Iceland, 7Danish Center for Clinical Health Services Research (DACS), Department of Clinical Medicine, Aalborg University and Aalborg University Hospital, Aalborg, Denmark, 8Department of Molecular Medicine and Surgery; Karolinska Institutet, and Department of Cardiothoracic Surgery, Karolinska University Hospital, Stockholm, Sweden, division of cardiac surgery, Sto, Sweden, 9Danish Center for Clinical Health Services Research (DACS), Department of Clinical Medicine, Aalborg University and Aalborg University Hospital, Aalborg, Denmark, 10Department of Cardiothoracic surgery, Odense University Hospital, Odense, Denmark, division of cardiac surgery, Odense, Denmark
Abstract Body:
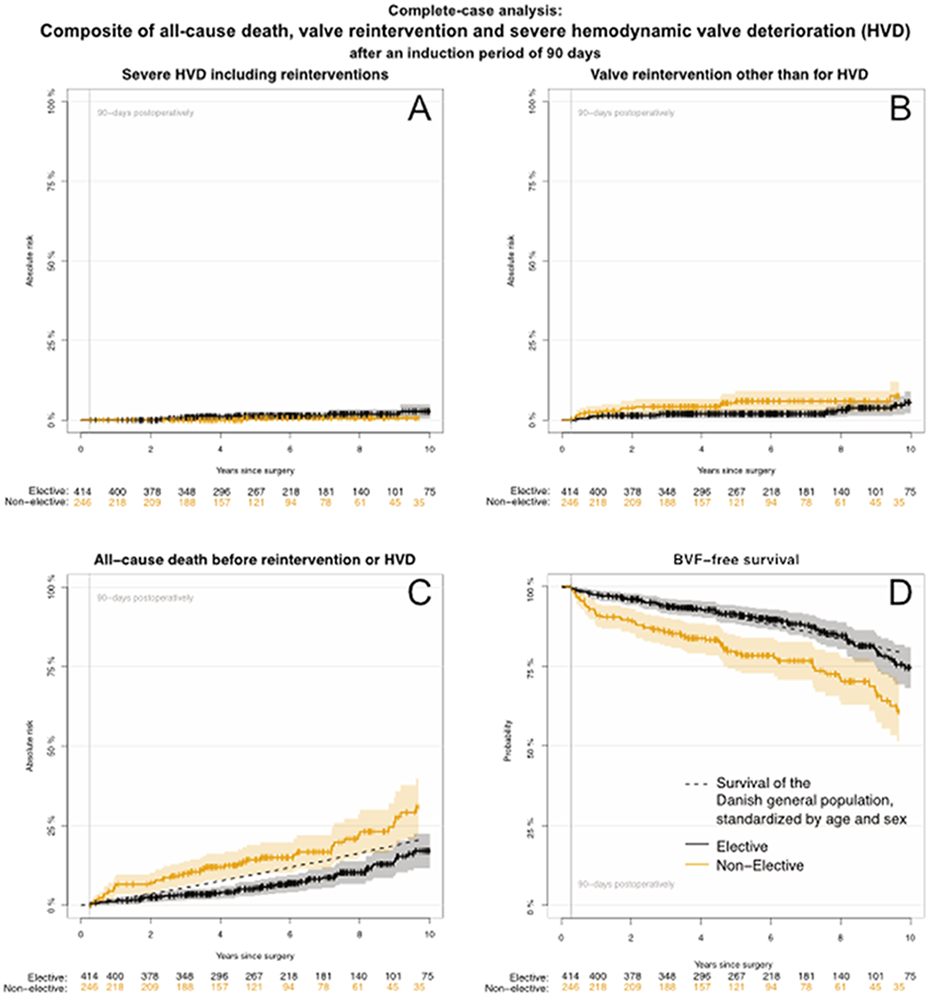
Objective: Bioprosthetic valve failure of the Medtronic Freestyle® bioprosthesis is not previously reported, and durability only in mixed or elective populations. Our objective was to estimate biological valve failure(BVF)-free survival later than 90 days after aortic root replacement with the Freestyle, in elective and non-elective patients.
Methods: This retrospective, multicenter study included unselected Freestyle aortic root patients, stratified for surgical priority. BVF-free survival after a 90-day induction period, defined as freedom of all-cause death, valve reintervention and severe hemodynamic valve deterioration, was related to the survival of the standardized Danish general population.
Results: Out of 799 patients, 659 (82.5%) survived without valve failure >90 days. Median follow-up for BVF was 5.9 years (IQR 3.2-8.6). Median age was 66 years, 31% were ≤60 years, 68% were male and 55% were elective cases. BVF-free survival after a 90-day induction-period was for elective patients 91% (95%CI: 88-94), 84.7% (95%CI: 80-89) and 76% (95%CI: 69-82) at 5, 8 and 10 years, respectively, and comparable to the survival of the Danish general population. For non-elective patients, results were 79.1% (95%CI: 74-85), 70.3% (95%CI: 63-78) and 60.9% (95%CI: 51-70) at 5, 8 and 9.7 years, respectively. For both groups, the outcome was driven by all-cause death. Severe hemodynamic valve deterioration at 8 years was 1.4% (95%CI 0.5-2.4).
Conclusions: Elective patient’s probability of death or valve-failure resembled the survival of the standardized Danish general population after 10 years. Severe hemodynamic valve deterioration and valve-reinterventions were rare and did not differ between elective and non-elective patients.
Control Number: 24-A-58-HVS
Presentation Number: AP5
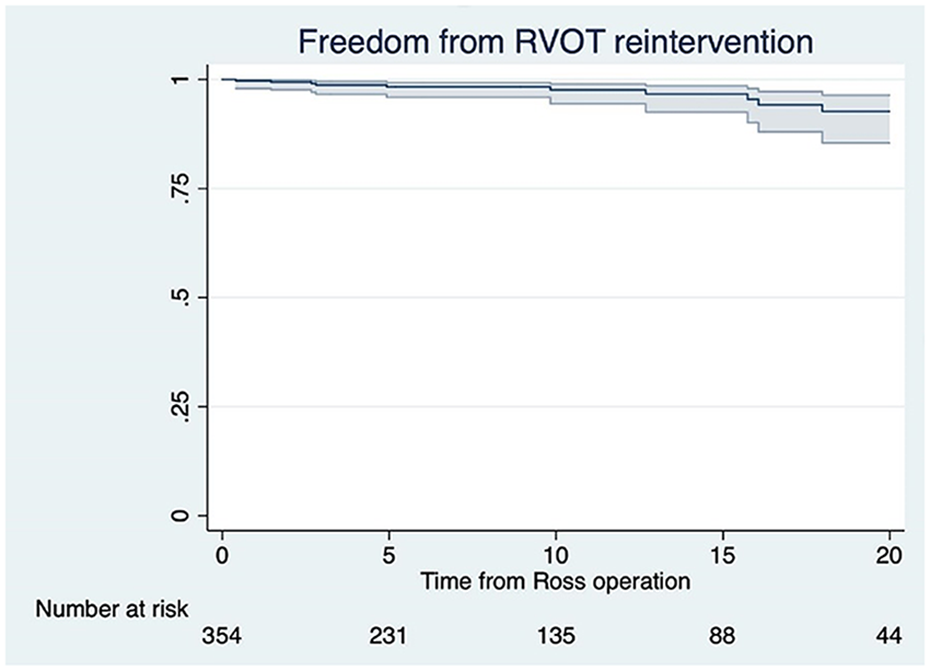
The Fate of Pulmonary Homograft in Ross Surgery: 25 Years of Follow-up Focus on Donor'S Features
Authors:Antonio Segreto1, Maria Jose Maria Jose Alcaraz2, Veronica Lorenz1, Gaby Aphram1, Laurent De Kerchove1, Gebrine El Khoury1, Ramadan Jashari2, Stefano Mastrobuoni1
1Department of Cardiovascular & Thoracic Surgery, Cliniques Universitaires Saint-Luc, Université Catholique de Louvain (UCL), Brussels, Belgium, 2European Homograft Bank, Brussels, Belgium
Abstract Body:
Objective: The majority of studies evaluate the Cryopreserved pulmonary homograft (CPH) after Ross operation based on the recipient's characteristics. Instead, this study takes into account the characteristics of the donor to identify potential predictive elements that may contribute to graft degeneration over time
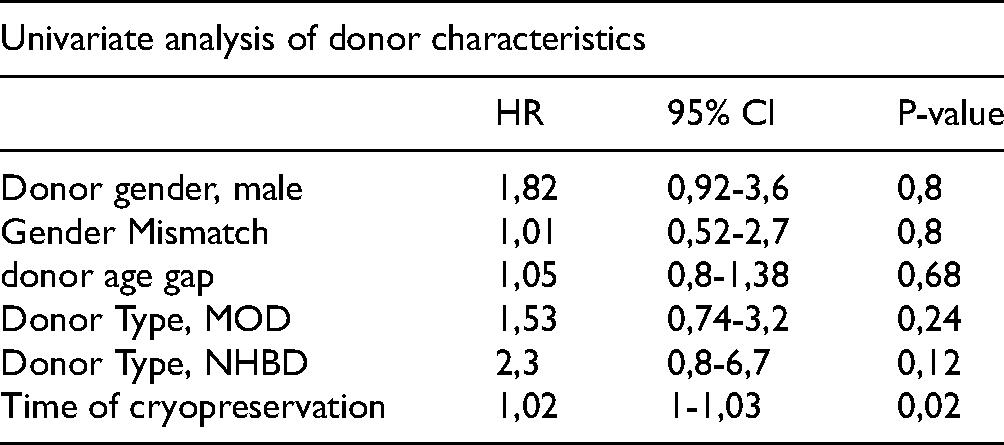
Methods: Retrospective analysis of 365 patients underwent Ross from 1991 to 2021 at our institution. Data of homograft’s donor were collected from our reference center for CPH. Primary endpoints: patient survival, rate of CPH stenosis or insufficiency and reintervention. Secondary endpoints: research for donor-related predictive factors for homograft dysfunction.
Results: The early mortality rate was 1.9%. Late mortality occurred in 6.1% of cases. Survival at 10, 15, and 20 years were 93%, 84%, and 78%, respectively. Endocarditis affected 6 patients, with 4 CPH releted-only. 22 patients underwent a reintervention, with homograft degeneration as indication in only 11 cases. The median time to reintervention was 13.47 years. Univariate analysis showed that only the cryopreservation time of the CPH was a possible risk factor.
Conclusions: CPH for RVOT reconstruction for Ross surgery remains the gold standard, yielding consistently excellent long-term outcomes. This reflects a paradigm shift away from the outdated notion that Ross surgery merely converts a one-valve disease into a two-valve disease.Isolated pulmonary stenosis has a low incidence, pulmonary insufficiency is quite rare. Systematic oversizing of the homograft should be used in all possible cases.The potential of transcatheter procedures, dilatations or Melody prothesis, can extend the life of the pulmonary homograft. Our research indicates that donor choice does not significantly impact the durability of CPH
Univariate analysis of donor characteristics
HR
95% CI
P-value
Donor gender, male
1,82
0,92-3,6
0,8
Gender Mismatch
1,01
0,52-2,7
0,8
donor age gap
1,05
0,8-1,38
0,68
Donor Type, MOD
1,53
0,74-3,2
0,24
Donor Type, NHBD
2,3
0,8-6,7
0,12
Time of cryopreservation
1,02
1-1,03
0,02
Control Number: 24-A-23-HVS
Presentation Number: AP6
Outcomes of Valve Sparing Root Reimplantation with Concomitant Coronary Artery Revascularization
Authors:Jake L. Rosen, John J. Kelly, Nimesh D. Desai, William L. Patrick, Brittany J. Cannon, Amit Iyengar, Siddharth Yarlagadda, Nicholas J. Goel, Wilson Y. Szeto, Joseph E. Bavaria
University of Pennsylvania, Philadelphia, PA, USA
Abstract Body:
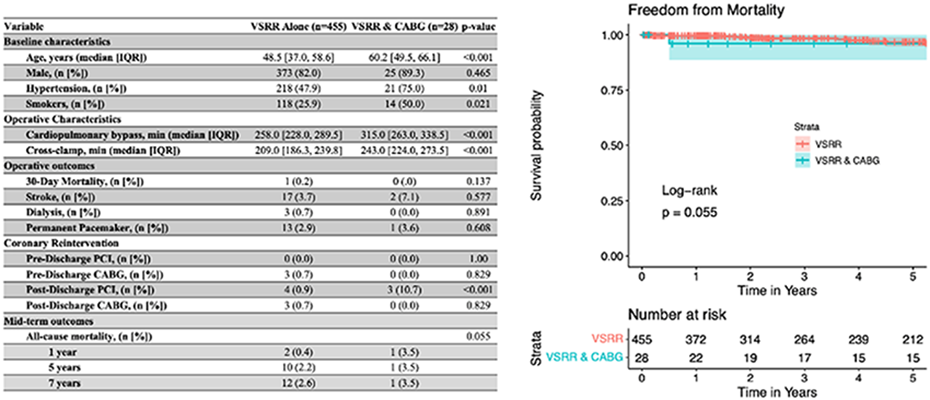
Objective: Valve sparing root reimplantation (VSRR) is mostly performed in younger patients with isolated root aneurysms. These patients may be indicated for coronary artery bypass grafting (CABG) typically found on preoperative coronary angiography. This study was performed to investigate outcomes in those undergoing VSRR versus VSRR and CABG.
Methods: Patients who underwent VSRR with and without planned concomitant CABG at our institution from 2004 - 2023 were included. Operative (30-day) outcomes were of primary interest; freedom from mortality was a secondary outcome and was computed using the Kaplan-Meier estimator.
Results: 94% patients underwent VSRR alone, while 6% underwent VSRR and CABG. 86% received a single graft while 14% >1 graft. 39% of patients received an internal mammary to left anterior descending anastomosis, while 46% received a saphenous vein to right coronary graft. Patients undergoing VSRR and CABG were older, and had higher percentages of hypertension and smokers. Bypass, clamp, and arrest times were greater in VSRR with CABG. Operative mortality was similar (p = 0.137); other operative outcomes, including stroke, pacemaker placement, and dialysis were similar. 5-year freedom from mortality was 97% for all patients, 97% for VSRR alone, and 96% for VSRR and CABG (p = 0.055). No patients underwent postoperative percutaneous coronary intervention (PCI) before discharge (p=1.00). Three patients with isolated VSRR underwent urgent CABG on the same operative day due to acute coronary occlusion. After discharge, a more patients with VSRR and CABG underwent PCI for repeat revascularization (p < 0.001) with similar rates of post-discharge CABG and STEMI or NSTEMI readmissions.
Conclusions: There were no significant differences in operative or mid-term outcomes between patients who underwent VSRR alone versus with CABG. Therefore, the need to perform coronary revascularization should not deter pursuit of VSRR when indicated.
Control Number: 24-A-101-HVS
Presentation Number: AP7
Comparison of Isolated Valve Sparing Aortic Root Replacement Versus Biological Bentall with Inspiris: 5-year Single Center Experience
Authors:Romy R. Hegeman1, Hans Smeenk1, Uday Sonker1, Patrick Klein2
1St. Antonius Hospital, Nieuwegein, Netherlands, 2Amsterdam UMC, Amsterdam, Netherlands
Abstract Body:
Objective: Use of new generation Inspiris Resilia bioprothesis hand-sewn in a vascular prosthesis (BioBentall) in young patients with aortic root pathology could provide a reasonable alternative to valve sparing root replacement (David-procedure). The BioBentall procedure is technically less complicated and could be associated with less perioperative risk due to shorter crossclamping times especially in less experienced hands. The BioBentall with Inspiris valve is prepared for future transcatheter valve in root procedure, which is still an issue with current transcatheter valves after a David procedure. Objective of this study was to compare the outcome of the BioBentall with Inspiris valve with the David-procedure.
Methods: Retrospective single center comparison of patients whom underwent a David-procedure vs. BioBentall procedure with the Inspiris Resilia aortic valve between 2018 and 2023. Patients who underwent concomitant surgery were excluded. Primary outcome was cardiopulmonary bypass and aortic cross-clamp times. Secondary outcome was mortality and freedom from re-intervention during follow-up.
Results: Between 2018 and 2023, 23 patients (48%) underwent a David procedure and 25 patients (52%) underwent a BioBentall procedure with the Inspiris Resilia aortic valve in our center. Aortic cross-clamp times were significantly shorter in patients who underwent a BioBentall procedure (95±38 min vs. 123±21 min for BioBentall and David respectively; p=0.004). Cardiopulmonary bypass times did not show a statistically significant difference between groups (p=0.24). During follow-up, there was no significant difference in survival between groups (p=0.337). No reinterventions were performed in both groups.
Conclusions: BioBentall with the new generation Inspiris Resilia bioprosthesis could provide an interesting alternative to a valve sparing root replacement in young patients with aortic root pathology. The BioBentall with Inspiris bioprothesis is technically less complicated and associated with significantly shorter aortic crossclamping times, but did not result in less perioperative morbidity and/or mortality.
Control Number: 24-A-16-HVS
Presentation Number: AP8
Clinical Results of Combined Aortic Valve Sparing Reimplantation and Mitral Valve Repair
Authors:Veronica Lorenz, Antonio Segreto, Luca Zanella, Stefano Mastrobuoni, Gebrine El Khoury, Laurent de Kerchove
Clinique Universitaires Saint Luc, Bruxelles, Belgium
Abstract Body:
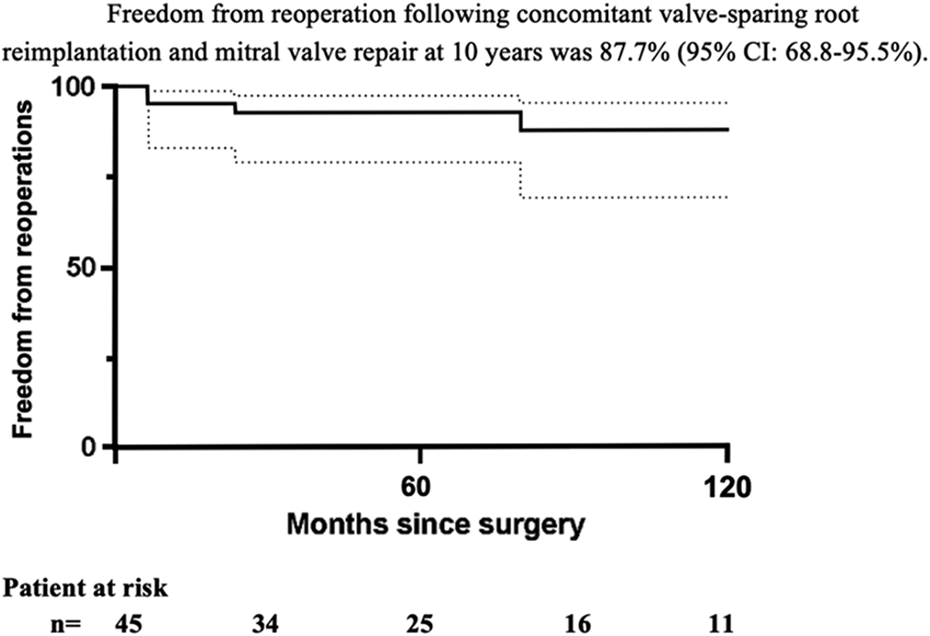
Objective: Aortic valve sparing root reimplantation (VSR) and mitral valve (MV) repair are established surgical options to treat aortic root pathologies or mitral valve regurgitation. In literature, most of the current studies report the results of the replacement of the aortic root with valved conduits associated with MV repair or replacement. However, knowledge regarding the association of both valves preserving techniques is limited. The aim of our study is to report our experience in combined VSR and MV repair.
Methods: From January 2000 to June 2022, a total of 45 patients underwent combined VSR and MV repair at the St. Luc University Hospital in Bruxelles.
Results: The median age was 54,4 years (IQR 34,8-64) and 88.9% were male. 12 patients (26.7%) had a connective tissue disorder (most of them were Marfan, n=10). No patients died during hospital stay and 3 patients (6.7%) required postoperative pacemaker implantation. Overall survival at 10 years was 89.6% (95% CI: 64.3-97.3%). Further, freedom from all reoperations at 5 years was 92.6% (95% CI: 78.8-97.6%) and at 10 years 87.7% (95% CI: 68.8-95.5%). One patient required aortic valve replacement with a bioprothesis for recurrent severe aortic insufficiency, two patients underwent successful mitral re-repair and one patient required both aortic and mitral repair
Conclusions: Combined aortic root and MV operations are complex surgeries. However, when performed in centers experienced in both procedures, they are safe and associated with excellent long-term survival and durability. This study confirms that preserving both valves is feasible applying anatomic principles normally used for aortic valve sparing and mitral valve repair and allows to obtain excellent results and freedom from reoperation.
Control Number: 24-A-59-HVS
Presentation Number: AP9
Predictors for the Occurrence of Postoperative Dressler's Syndrome after Native Valve-sparing Aortic Valve Surgery in Non-elderly Adults
Authors:Theresa Holst, Lisa Mueller, Sina Stock, Tatiana Maria Sequeira Gross, Evaldas Girdauskas
University Hospital Augsburg, Augsburg, Germany
Abstract Body:
Objective: We aimed to determine the perioperative factors associated with the occurrence of Dressler’s syndrome (DS) after native valve-sparing aortic valve (AV) surgery in non-elderly patients.
Methods: From 01/2021 to 08/2023, 91 consecutive patients (mean age: 46±12 years, 89% male) underwent native valve-sparing AV surgery (isolated AV repair, AV repair and ascending aorta replacement, AV-sparing root replacement, isolated Ross procedure or Ross procedure and ascending aorta replacement) at our institution. DS was defined as progressive serous pericardial or bilateral pleural effusions requiring intervention/surgery or at least anti-inflammatory medication. A logistic regression model was used to determine factors significantly associated with the occurrence of DS.
Results: A total of 21 patients (23%) developed DS during the early postoperative course (DS group). Six DS patients required intervention/surgery for hemodynamically relevant pericardial effusion. Further 6 DS patients required drainage of bilateral pleural effusions. The remaining 70 patients (77%) showed no signs of DS (non-DS group). No significant age or sex differences could be detected between both groups. However, the relative frequency of AV-sparing root replacement (67% vs. 30%,p=0.002), tricuspid AV morphology (48% vs. 26%,p=0.040) and partial upper sternotomy (81% vs. 51%,p=0.016) was significantly higher in DS vs. non-DS patients. Maximum C-reactive protein (CRP) level within the first 48 hours postoperatively (22.3±7.2 vs. 16.6±6.6 mg/dl,p=0.001) and absolute peak postoperative CRP level (24.8±8.0 vs. 18.3±7.3 mg/dl,p<0.001) were also significantly higher in DS vs. non-DS patients. Multivariate logistic regression revealed AV-sparing root replacement (OR: 3.07, 95%CI:1.02-9.29, p=0.047) and maximum CRP >15 mg/dl within the first 48 hours postoperatively (OR: 3.99, 95%CI:1.01-15.84, p=0.049) as independent factors associated with onset of DS.
Conclusions: AV-sparing root replacement and maximum CRP >15 mg/dl within the first 2 days after autologous AV surgery are significantly associated with the occurrence of postoperative DS. Prophylactic antiphlogistic treatment should be considered in such cases.
Control Number: 24-A-52-HVS
Presentation Number: AP10
Patient Experiences in Clinical Decision-making in Ascending Aortic Aneurysms
Authors:Maximiliaan Notenboom, BSc1, Arjen Gökalp, MD1, Hector W. de Beaufort, MD PhD2, Regina The, MSc3, Carlijn G. Thijssen, MD1, Kevin M. Veen, MD PhD1, Jonathan R. Etnel, MD PhD1, Antoine H. Driessen, MD PhD4, Roland R. van Kimmenade, MD PhD5, Marco C. Post, MD PhD6, Robin H. Heijmen, MD PhD5, M. M. Mokhles, MD PhD6, Ad J. Bogers, MD PhD1, Jolien W. Roos-Hesselink, MD PhD1, Jos A. Bekkers, MD PhD1, Johanna J. Takkenberg, MD PhD1
1Erasmus University Medical Center, Rotterdam, Netherlands, 2Sint Antonius Hospital Nieuwegein, Nieuwegein, Netherlands, 3ZorgKeuzeLab, Delft, Netherlands, 4Amsterdam University Medical Center, Amsterdam, Netherlands, 5Radboud University Medical Center, Nijmegen, Netherlands, 6University Medical Center Utrecht, Utrecht, Netherlands
Abstract Body:
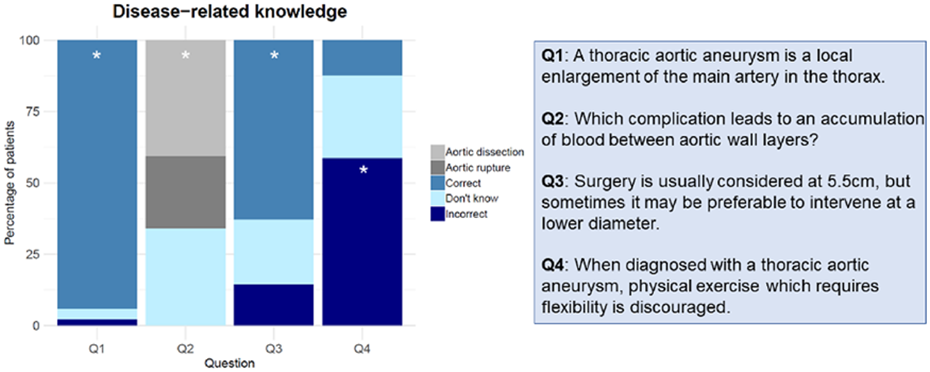
Objective: This study aims to investigate the current patient experiences in clinical decision-making in ascending aortic aneurysm (AscAA).
Methods: This study encompasses an interim analysis of the control phase (no access to information tool) of a prospective patient information portal implementation trial in three Dutch aortic centres. Patients who visited the outpatient clinic with recent diagnosis, an indication for surgical treatment or after surgery of an AscAA between 2021-2023 were included. Patients completed a questionnaire that explored disease knowledge, anxiety and depression (HADS), quality of life (SF36), involvement in decision making, and the information that the patient received from the treating physician, assessed by multiple choice questions, and a 1-5 Likert Scale.
Results: At interim analysis, the questionnaire was completed by 138 patients (median age: 65.2y(IQR:57.0-71.4y), 33.3% women) with an AscAA (55% without surgical indication, 14.5% with surgical indication, 26.8% after surgery). Figure 1 shows the distribution of answers to disease-related knowledge questions. Eighteen patients (17.4%) were able to answer all 4 questions correctly, with no difference between men and women (19.6% vs 13.1%, p=0.341). Twenty-two percent felt they had insufficient knowledge about their AscAA, and 23% regarding treatment options. In HADS, 21% scored above normal in the anxiety section, and 9% in the depression section. Impaired overall health was reported by 30.4%, and the SF36 revealed a median general health score of 65.0(IQR:50.0-85.0). Regarding decision-making, 88.4% believed that decision-making should be done together with patient and doctor, while 11.5%, in retrospect, reported to feel insufficiently informed(≥4/5 Likert scale).
Conclusions: In patients with ascending aortic aneurysms, disease-specific knowledge, wellbeing and patient experiences with clinical decision-making are currently suboptimal. Implementation of shared decision making, including tools to inform and empower patients, has great potential to improve the quality of decision making.
Control Number: 24-A-168-HVS
Presentation Number: B1
Association of Wall Stress with Diameter Indices in Predicting All-cause Mortality in Ascending Thoracic Aortic Aneurysm Patients
Authors:Shiv Verma, William Carroway, Marko Boskovski, Liang Ge, Elaine Tseng
University of California, San Francisco and San Francisco Veteran Affairs Medical Center, San Francisco, CA, USA
Abstract Body:
Objective: Current size-based treatment guidelines for ascending thoracic aortic aneurysms (aTAA) recommend surgical intervention at an aortic diameter of 5.0-5.5cm. However, it is well understood that roughly 50% of aortic dissections occur at diameters <5cm and that patients with aneurysm sizes >=5.5cm who are unfit for surgery can often survive years without complications. Novel methods to better understand the aTAA risk profile are needed. This study aimed to compare peak circumferential and longitudinal wall stresses with diameter indices in predicting 3-year all-cause mortality in aTAA patients.
Methods: We calculated peak wall stresses in the ascending aorta for 275 aTAA patients from the San Francisco Veteran Affairs Medical Center. Chest computed tomography images were uploaded to MeVisLab, where 3D geometric models were created. This initial geometry was then refined using Geomagic. Finite element analysis computational simulations were performed on these models using LS-DYNA in order to calculate peak cirumferential and longitudinal wall stresses at end-systolic pressure. We matched these wall stress values to diameter/(body surface area [BSA]) and diameter/(height [ht]) of the same patients in relation to 3-year all-cause mortality. Cause-specific Cox proportional hazard models were used to estimate all-cause mortality hazard ratios.
Results: Peak longitudinal stress independent of age and indexed diameter showed a hazard ratio of 1.24 (95% CI, 1.00-1.53, p=0.04), indicating a significant association with all-cause mortality. Neither peak circumferential stress (p=0.16) nor diameter/ht index (p=0.33) were associated with an increased mortality rate. On multivariate Cox proportional hazard analysis, diameter/BSA index independently did not show to be significantly associated with all-cause mortality (p=0.13).
Conclusions: Peak longitudinal wall stress predicted 3-year all cause mortality after adjustment for age and diameter/BSA index, whereas diameter/BSA independently did not. Peak longitudinal stress may represent a clinical variable to be used for assessment of adverse event risk in aTAA patients.
Control Number: 24-A-108-HVS
Presentation Number: B2
Local Hemodynamic Perturbation at Proximal Outflow Tract Leads to Consistent Congenital Heart Malformations
Authors:Shuofei Sun, Rohit Agarwal, Iwijn De Vlaminck, Jonathan Butcher
Cornell University, Ithaca, NY, USA
Abstract Body:
Objective: Embryonic chick hearts with altered blood flow, free of genetic biases, present heart malformations comparable to those in human infants. Common surgical methods, such as left atrial ligation, vitelline vein ligation, and outflow tract banding, substantially change the heart's mechanical environment. This results in a diverse set of CHDs, complicating the correlation between local biomechanical forces and heart valve developmental processes. To address this, our study introduces a localized hemodynamic perturbation method using two-photon microscopy-guided deep femtosecond photoablation of proximal outflow tract cushions. We aim to produce a genetically unbiased embryonic CHD model and, using spatial transcriptomic technology, investigate how blood flow changes affect valvulogenic programs.
Methods: Laser photoablation was applied to the proximal OFT at HH23. Ablated embryos and sham controls were harvested at HH31 and HH36. Morphological changes in the ablated hearts were documented with nano CT scanning and 3D analysis. Spatial single-cell RNA sequencing was then performed on both sets at comparable stages. The sequencing data was processed using our custom bioinformatic workflow to pinpoint gene expression alterations.
Results: Our technique consistently resulted in embryos showing only the persistent truncus arteriosus phenotype. We were able to map spatiotemporal gene expression profiles in the outflow tract of both sham and ablated hearts with near single-cell resolution. These findings indicate that even minor local hemodynamic perturbations in the proximal outflow tract can shift the expression of genes pivotal to the growth and maturation of semilunar valves.
Conclusions: Our research underscores that specific, localized hemodynamic changes can lead to consistent CHDs, like persistent truncus arteriosus, establishing a non-genetic foundation for PTA. This study illuminates the nuanced gene expression shifts in cardiac outflow tracts under altered hemodynamic conditions, spotlighting intricate signaling pathways and potential molecular targets, laying the groundwork for future inquiries.
Control Number: 24-A-119-HVS
Presentation Number: B3
Proximal Thoracic Aortic Aneurysms Have Distinct Biochemical Profiles in Males and Females
Authors:Yu Tong Linda Lu, Malak Elbatarny, Uros Kuzmanov, Daniella Eliathamby, Jennifer CY Chung, Craig Simmons, Anthony O. Gramolini, Maral Ouzounian, on behalf of MultiTAAD investigators
University of Toronto, Toronto, ON, Canada
Abstract Body:
Objective: Female sex is associated with rapid thoracic aortic aneurysm (TAA) growth rate and poorer TAA outcomes however mechanisms are unclear. This study aimed to compare biochemical profiles of male and female proximal TAA tissues to elucidate phenotypic differences.
Methods: 169 TAA aortic samples were collected prospectively (N=131 male, 74%). All samples were analyzed using a customized deep-coverage protocol for mass spectrometry proteomics. Clinical and proteomic data were directly compared in Males vs. Females (p≤0.05 considered significant). Gene Ontology (GO) analyses were performed for all significant proteins to determine biological function. Multivariable logistic regression was used to determine proteomic significance after correcting for clinical baseline differences.
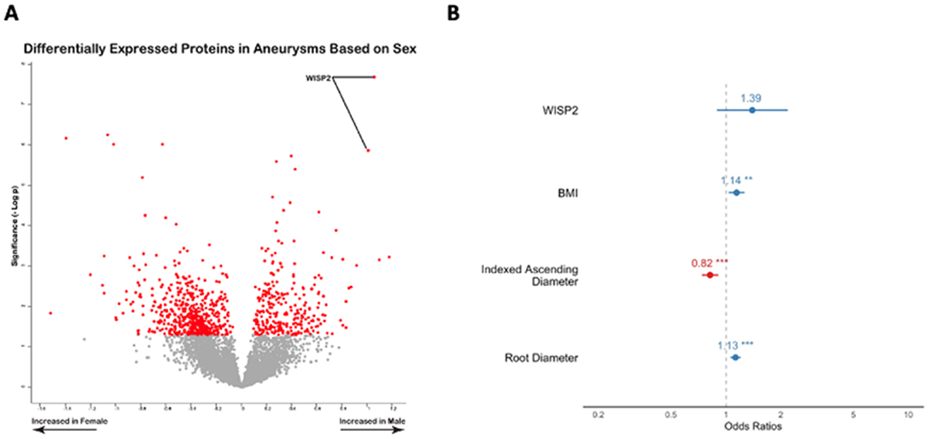
Results: Females had smaller BMI (p<0.001) and less smoking history (p=0.02) than males. Compared to males, female TAA diameters also differed significantly with smaller absolute root sizes (39.3±6.6mm vs 46.6 ± 7.4mm, p<0.001) and larger ascending aortas (27.7±5.0mm/m2 vs. 22.4 ±4.7mm/m2, p<0.001) and arches (22.3±9.3mm/m2 vs. 16.4 ± 5.5mm/m2; p<0.001) after indexing. A total of 795 differentially expressed proteins were quantified (521 downregulated and 274 upregulated). GO term analysis revealed binding, metabolic proteins, biological regulation, and catalytic activity to be enriched in aneurysms of males. Notably, WISP2, a protein involved in the inhibition of vascular smooth muscle cell proliferation was significantly upregulated in males compared to females (Figure 1A). After adjusting for baseline differences, a signal towards elevated WISP2 in males remained (OR 1.39; 95% CI 0.96-2.03, p=0.14, Figure 1B).
Conclusions: Significant differences in anatomy and proteomic profiles of male and female TAAs suggest distinct aneurysm phenotypes among the sexes. Some sex-based biochemical differences may be partially driven by differences in body and aortic size. Further investigation will determine whether these biochemical differences contribute to known prognostic differences in TAAs of males and females.
Control Number: 24-A-169-HVS
Presentation Number: B4
A Genome-wide Copy-number Association Study in Calcific Aortic Valve Disease
Authors:Ran XU
Institut universitaire de cardiologie et de pneumologie de Québec - Université Laval, Québec, QC, Canada
Abstract Body:
Objective: Calcific aortic valve disease (CAVD) is the most common cause of aortic valve replacement in the developed countries, without effective medical treatment. Epidemiological studies indicated that genetic factors contribute more to the pathogenesis of CAVD than environmental factors. Copy number variations (CNVs) are a type of genetic polymorphism with well-established impact on a range of human diseases. However, the role of CNVs in CAVD is understudied. In this research, we aimed to identify potential CNVs associated with CAVD.
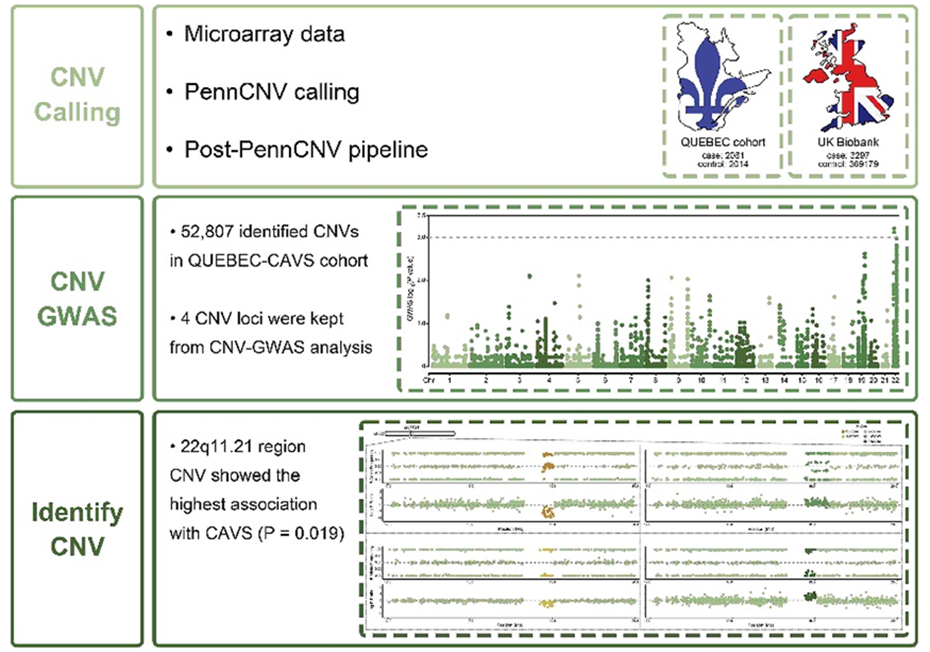
Methods: We performed a genome-wide copy-number association study (CNV-GWAS) in the Quebec City Case-Control Calcific Aortic Valve Stenosis Cohort (QUEBEC-CAVS). CNVs were called using the PennCNV software and genome-wide genotyping data from 2,097 QUEBEC-CAVS cases and 2,071 QUEBEC control. Moreover, genome-wide genetic data including 3,297 cases and 369,179 controls from UK Biobank were also used for validation.
Results: In total, 121,419 CNVs were predicted from QUEBEC-CAVS cohort. After quality controls (QCs), 52,807 identified CNVs were retained. In UK Biobank, 1,672,393 CNVs were identified and retained after QCs. By combining analysis from CNV-GWAS in QUEBEC-CAVS and UK Biobank, four CNV loci were identified to be significantly associated with CAVS. Among them, a CNV located in the 22q11.21 region (18,889,969-19,007,688bp) showed the highest association with CAVS (P = 0.019).
Conclusions: This study shows that CNVs may participate in the pathogenesis of CAVD, and, for the first time, emphasizes the putative role of this mutational class in disease development. The identification of CNV-GWAS loci is important to guide clinically relevant laboratory-based research in CAVS.
Control Number: 24-A-90-HVS
Presentation Number: B6
Endothelial-to-mesenchymal Transition during Cardiovascular Calcification Can Be Managed by Notch Signalling Pathway
1University of Oslo, Oslo, Norway, 2University of Ferrara, Ferrara, Italy
Abstract Body:
Objective: Endothelial cells contribute to the development of cardiovascular calcification. A variety of biomechanical stimuli may provoke cardiovascular endothelial cells to undergo endothelial-to-mesenchymal transition (EndMT). Then endothelial cells may migrate into the interstitium and calcify or stimulate the underlying mesenchymal cells to calcify. Notch is an essential regulator of endothelial differentiation. Notch is also suggested to play a role in EndMT. Notch signalling contains receptors (NOTCH 1-4) and ligands (DLL1,3,4, and JAG1,2). CSL is a key transcription factor for Notch regulation when it interacts with Notch intracellular domain (NICD). In this study we investigated the involvement of Notch signalling in EndMT.
Methods: The study was carried out on primary human umbilical cord vein endothelial cells (HUVEC). Notch signalling was activated via lentiviral transduction (NICD or JAG1). Notch signalling was down-regulated by short-hairpin RNA against either CSL or JAG1. To induce EndMT, HUVEC were transduced with lentiviral concentrate encoding NICD or JAG1. Promoter activity assay was used to assess the interactions of the Notch components (NICD and JAG1) with CSL. qPCR, Western blotting were used to quantify gene expression at RNA and protein level. Immunocytochemistry on αSMA was used to evaluate EndMT.
Results: NICD induced expression of Notch signalling component genes - target genes HEY1 and SLUG, and receptors NOTCH2, NOTCH3 - followed by EndMT. JAG1 overexpression alone modestly increased expression of Notch genes without inducing EndMT. Inhibition of Notch signalling by blocking CSL completely inhibited EndMT.
Conclusions: Modifications of Notch signalling influenced the activation of EndMT in primary endothelial cells. Notch inhibition may have therapeutic potential of targeting EndMT, both preventing and inducing the transition depending on the context.
Background: We described a family with LTBP2 mutation segregating MVP. Similarly a large GWAS associated the gene with MVP. We discibe changes in the valvular matrix in knockout mic.
Methods and results: We generated two strains of mice using CRISPR technology. A complete knockout and a knock in mouse. 19 mice were dissected so far. None of the wt mice (n=8) demonstrated myxomatous degeneration. Of the 11 mice with mutation, 8 homozygote for deletion and 3 homozygote for the human mutation, 8 demonstrated myxomatous Degeneration by histology (1 knockin mouse ∼ 70% penetrance in male mice, p=0.001, Fisher exact test). The pathologist that read the studies was blinded to the genotype. Echocardiography of theses mice demonstrated findings consistent with MVP in 50%of affected mice and not in controls. Immunohistochemical analysis of the valve in the knockouts demonstrate disruption of Collagen structure as well as changes in elastin structure.
Conclusion: LTBP2 mutation is associated with myxomatous degeneration. The mechanism may be related to disruption of elastin and collagen structure in the valve tissue.
Control Number: 24-A-47-HVS
Presentation Number: B8
Dynamic Changes in Mitral Valve ECM, Tissue Mechanics and Function in a Mouse Model of Marfan Syndrome
Authors:Brittany A. Gonzalez1, Samuel W. Harmeyer1, Taejeong Song2, Sakthivel Sadayappan2, Katherine E. Yutzey1
1Cincinnati Children's Hospital, Cincinnati, OH, USA, 2University of Cincinnati College of Medicine, Cincinnati, OH, USA
Abstract Body:
Objective: Marfan syndrome (MFS), caused by a dominant mutation in Fibrillin1 (Fbn1), can lead to congenital heart valve abnormalities including myxomatous valve disease (MVD). Progressive MVD is characterized by collagen fiber fragmentation and leaflet thickening, however, the mechanistic links between mechanical forces and biological changes in valve degeneration remain unknown. Here, we examine longitudinal changes in mitral valve structure, function, tissue mechanics, ECM organization, and gene expression in progressive MVD in MFS mice.
Methods: Functional and mechanical valve characteristics were determined in healthy and Fbn1C1039G/+ MFS mouse mitral valve leaflets by echocardiography (ECHOs) and uniaxial mechanical testing at 2-, 6- and 12-months-of-age. ECM remodeling was quantified histologically by Movat’s Pentachrome staining as a proteoglycan:collagen ratio. Collagen structure and organization were examined by Picrosirius Red staining of collagen I and III and multiphoton and second harmonic imaging.
Results: Altered ECM mechanics and mitral valve leaflet morphology are detected before functional abnormalities in Fbn1C1039G/+ MFS mice. At 2 months, myxomatous ECM is apparent in increased proteoglycan composition, decreased stiffness, and decreased function of the mitral valve. By 6 and 12 months, there is an increase in collagen, matrifibrocyte gene expression characteristic of collagen-rich connective tissue and functional abnormalities in the MFS mice. Furthermore, the collagen structure and organization are abnormal postnatally with increased dysregulation with age in the MFS mice.
Conclusions: Together, these data indicate that the amount, as well as the structure and organization of ECM proteins is important for valve integrity. The progression of MVD in MFS mice is manifested in abnormal collagen fiber organization and orientation, along with altered tissue mechanics and dysfunction of the mitral valve. Gene expression characteristic of matrifibrocyte activity also is increased with collagen fiber dysregulation, suggesting a potential role in valve aging and MVD progression in MFS.
Control Number: 24-A-79-HVS
Presentation Number: E1
Material Characteristics of Human Pericardium and its Calcification According to Glutaraldehyde Concentration and Fixation-time
Authors:Sahra Tasdelen, M.Sc, Barbara Messner, PhD, Martin Andreas, MD, PhD
Medical University of Vienna, Vienna, Austria
Abstract Body:
Objective: This study aimed to investigate the impact of varying concentrations of glutaraldehyde on the structural, mechanical and calcification properties of human pericardium. As a result, the optimal conditions should be identified for implanting autologous pericardial aortic valve prostheses.
Methods: Samples of human pericardium were collected and cross-linked under controlled conditions with glutaraldehyde concentrations ranging from 0.1% to 2.5% for exposure times ranging from 5 minutes to 90 minutes. After cross-linking, structural changes were assessed through histological examination and scanning electron microscopy (SEM). Calcification susceptibility was evaluated through in vitro calcification assays in a simulated physiological environment. A mechanical test and a thermal stability test were conducted to assess the material characteristics of the fixed tissues.
Results: Histological analysis indicated that there were discernible differences in tissue morphology and collagen structure among the groups exposed to various concentrations of glutaraldehyde and various exposure times. Scanning electron microscopy (SEM) observations showed alterations in surface characteristics, with some variations in pore size across the different concentration and time groups. The mechanical stability assessments revealed variations among the groups exposed to different glutaraldehyde concentrations. While there were observable differences in tensile strength and elasticity, further investigation is necessary to precisely quantify these variances and assess their clinical significance.
Conclusions: This study demonstrates that glutaraldehyde concentration plays a pivotal role in preserving the structural integrity of human pericardium and mitigating calcification. The findings suggest that careful selection of glutaraldehyde concentration in the cross-linking process can significantly influence the performance and longevity of human pericardium as a biomaterial in cardiac valve prostheses. These results contribute to a better understanding of the optimization of biomaterial processing for improved clinical outcomes in cardiovascular surgery.
Control Number: 24-A-65-HVS
Presentation Number: E2
The Effect of Automated Fastener in Isolated Aortic Valve Replacement
Authors:Juhyun Lee, Cheong Lim
Seoul National University Bundang Hospital, Seongnam-si, Korea, Republic of
Abstract Body:
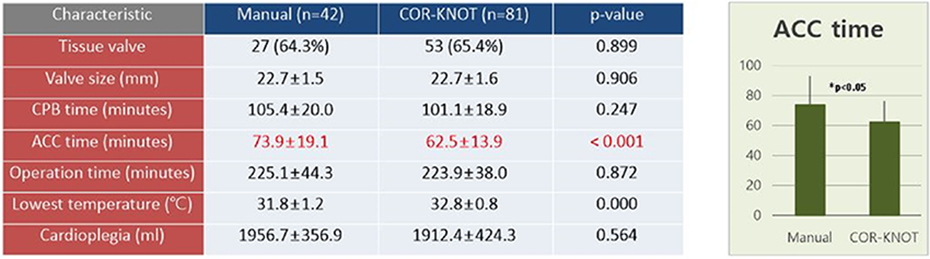
Objective: During heart valve surgeries, the Cor-Knot®, automated fastener, is intended to replace the traditional manual process of tying knots with sutures, making it faster and more efficient. This study is to evaluate the outcomes of patients undergoing isolated aortic valve surgery using the Cor-Knot®.
Methods: This is a historical cohort study of all patients who underwent isolated aortic valve replacement through median sternotomy at Seoul National University Bundang Hospital between 2013 and 2023. During the study period, 141 patients with aortic disease underwent isolated surgical AVR. To increase homogeneity in both groups 18 patients who underwent sutureless AVR were excluded. The study compared patients characteristics, intraoperative parameters, early postoperative outcomes.
Results: No significant differences were observed in any of the baseline characteristics and the incidence of major postoperative complications between the Cor-knot and hand-tied sutures. The use of Cor-Knot was associated with reduced aortic cross clamp time about 11 minutes. Cor-Knot system incurred approximately 1,600 US dollors higher surgical material costs, but the out-of-pocket cost was not significantly different.
Conclusions: To keep striving for relief of the surgical burden, the Cor-Knot® is a novel technology that reduces operation time, especially aortic cross clamp time. Although the cost of surgical material was larger with Cor-Knot, the out-of-pocket cost was similar.
Control Number: 24-A-25-HVS
Presentation Number: E3
A New Mechanical Aortic Valve Design to Reduce Unphysiological Flow
Authors:Shaokai Zheng, Ali Mokhtari, Dominik Obrist
Cardiovascular Engineering, ARTORG Center, University of Bern, Bern, Switzerland
Abstract Body:
Objective: We explore the idea of accelerating turbulence decay as a novel strategy to reduce the unphysiological shear stress and turbulence level generated by mechanical aortic heart valves (MHV).
Methods: We performed three-dimensional in silico simulations using OpenFOAM on the Swiss National Supercomputing Center. A straight ascending aortic model of 22mm in diameter and 100mm in length was used, including the aortic sinus. Two MHV models were tested, one with canonical bi-leaflet design, similar to that of the On-X valve, and one with our fractal bi-leaflet design. The inlet boundary condition was prescribed with a time-varying flow rate with a cardiac cycle of 0.7s and a peak flow rate of 20L/min. For this study, we only look at 0.1-0.4s of the cardiac cycle, where the leaflets are fully open.
Results: With our initial fractal leaflet design, we were able to reduce the mean shear stress by 2% and accelerate the decay of turbulent kinetic energy (TKE). The higher decay rate will lead to a reduction of TKE over the cardiac cycle. These numbers are further optimized by tuning the design parameters of the fractal leaflets. By examining the negative streamwise velocity component at peak flow, a stronger washout (p<0.001) is generated by our design by comparing the negative velocity in the sinus, which is likely to ameliorate the stasis in the sinus.
Conclusions: The new MHV design that features fractal leaflets has shown several benefits in the generated turbulence. It is a promising option to improve the hemodynamic performance of MHV and to reduce the thrombogenicity over time.
Figure1. (a) The mean shear rate of the flow over time. (b) Washout effects (negative longitudinal velocity contours) in the sinus for the canonical and fractal cases.
Control Number: 24-A-72-HVS
Presentation Number: E4
Quantitative Assessment of Volume Expansion Using a Novel Aortic Root Retraction System for Minimally Invasive Surgical Valve Replacement
Authors:Shaelyn Cavanaugh, MD1, Ariana Goodman, MD1, Kyle Purrman, MD2, Brian Peterson, MS2, Benjamin Boseck2, Jacob Hammond2, Jude Sauer, MD2, Peter Knight, MD1, Daniel Ziazadeh, MD1
1University of Rochester Medical Center, Rochester, NY, USA, 2LSI SOLUTIONS®, Victor, NY, USA
Abstract Body:
Objective: Less invasive approaches to surgical aortic valve replacement (SAVR) have been shown to reduce recovery time, pain, and morbidity. However, achieving adequate visualization of the annulus can be challenging, especially through less invasive incisions. A novel aortic root retraction system, the AVR NAVIGATOR™ (LSI SOLUTIONS®, Victor, NY, USA), can facilitate annular visualization and suturing. Herein, we quantify the degree to which this technology enhances visualization of the aortic root and annulus during SAVR relative to root exposure using only stay sutures.
Methods: The AVR NAVIGATOR™ is a flexible, atraumatic retractor that is deployed in the aortic root below the sino-tubular junction. This study utilized 10 ex vivo porcine hearts. In each heart, commissural stay sutures were placed into the aortic annulus. The aortic root and annulus were filled with a silicone mold. The solidified molds were removed and 3D scanned for digital volume assessment. An AVR NAVIGATOR™ was then deployed into the aortic root and the molding process was repeated. The 3D models of the aortic root with and without the AVR NAVIGATOR™ were compared to assess the relative volumes. Surgeons also qualitatively assessed the relative visualization.
Results: The average aortic root volume with the AVR NAVIGATOR™ was 9316.8 mm3; the average volume without the AVR NAVIGATOR™ was 6335.6 mm3. On average, the AVR NAVIGATOR™ provided a 57.9% exposed volumetric increase in the aortic root compared to using stay sutures alone. Surgeons determined that the AVR NAVIGATOR™ improved annular and sub-annular visualization in every heart.
Conclusions: Compared to using stay sutures alone, the AVR NAVIGATOR™ significantly increases the exposed volume of the aortic root, demonstrating potential to improve the visualization of the annulus during minimally invasive AVR. Qualitative surgeon assessment also confirmed that visualization was enhanced using this novel device.
Control Number: 24-A-107-HVS
Presentation Number: E5
In-vivo Dynamic Geometry of the Murine Aortic Valve
Authors:Michael S. Sacks1, Craig Goergen2
1University of Texas, Austin, TX, USA, 2Purdue University, West Lafayette, IN, USA
Abstract Body:
Objective: There are currently no non-surgical alternatives to treat AV disease, in large part because our understanding of its etiology remains incomplete. The study of human AV disease by direct assessment remains hampered by the fact data is only available at the time of treatment, where the disease is at or near end stage and time progression information is not available. Alternatively, large animal models remain unusable due to the inability to reproduce AV disease processes. Transgenic murine models provide are powerful experimental tool for investigating the genetic basis of human diseases, as the mouse shares more than 85% protein-coding genome with humans. In the present study we developed an integrated multi-scale computational-imaging specialized for the murine aortic valve (mAV) small size and high heart rate.
Methods: We obtained novel in vivo time mAV geometry over the cardiac cycle by extending our approach originally for cardiac imaging to acquire in vivo 4DUS images of mAVs with spatial voxel size and temporal resolution to be 40 microns and 2ms, respectively. We then developed a detailed mAV geometric model based on the segmented in vivo data at the fully opened and closed states.
Results: The mAV in vivo surfaces were accurately reconstructed from the segmented points (errors within 0.1 microns). Results were also checked against in vitro excised mAV imaged by microCT. Results revealed that the in vivo shape of the mAV was accurately reconstructed.
Conclusions. With the present methodology established, The outcome of this comprehensive study will be the establishment of an integrated experimental-computational-imaging approach to establish the mAV for the study of AV disease, exploiting modern murine transgenics. Collectively, it will help to lay the basis for the future non-surgical approaches to treat CAVD.
Control Number: 24-A-157-HVS
Presentation Number: E6
Novel Workflow for Developing a 3d Mitral Valve-left Ventricular Model from Transesophageal Echocardiography
Authors:Charles Wanna1, Akshita Sahni2, Patrick Kee1, Nils P. Johnson1, Hyunggun Kim3, Melanie R. Moody1, Krishnan B. Chandran4, Danny Ramzy1, David D. McPherson1, Vijay Govindarajan2
1University of Texas Health Science Center, Houston, TX, USA, 2Boston Children's Hospital, Boston, MA, USA, 3Sungkyunkwan University, Suwon, Korea, Republic of, 4The University of Iowa, Iowa City, IA, USA
Abstract Body:
Objective: Mitral valve (MV) repair is the preferred method of correcting mitral valve regurgitation. Realistic analysis of MV function and prediction of successful repair should include both the left ventricle (LV) and the MV to capture their coupled behavior. However, simultaneous imaging and processing of LV and MV has been a challenge. We present a novel and efficient method to convert transesophageal echocardiography (TEE) images into virtual 3D models for enhanced visualization and predictive flow modeling to assist with presurgical planning.
Methods: A total of 5 pigs were anesthetized prior to obtaining 3D TEE. DICOM data was processed using Slicer software. MV anatomy while maximally opened was segmented using its Valve Segmentation tool (Fig. 1A left panel). LV at the start and end of diastole was segmented in Slicer (Fig. 1A right panel). The MV was smoothened in MeshLab (Fig. 1A) then unified with the LV using Meshmixer. 3D models generated with our workflow were validated against the harvested MV and LV tissue.
Results: The generated 3D model of both MV and LV at end diastole geometrically correlated with the harvested sample with discrepancies due to tissue shrinkage postmortem (Fig. 1B). Unified anatomically accurate virtual models of the MV-LV for each animal throughout diastole were successfully developed (Fig. 2). Virtually, the annular circumference, LV length from annulus to apex, posterior MV leaflet, anterolateral leaflet, and anteromedial leaflet were 11.8, 5.1, 1.9, 1.8, and 1.7 cm. Anatomically, the corresponding measurements are 8.6, 6.0, 1.4, 1.0, and 1.1 cm.
Conclusions: We have developed an efficient, relatively automated workflow to create 3D models of MVs and LVs for hemodynamic modeling and visualization. This algorithm and 3D protocol may help to improve our mitral valve understanding prior to planning surgical repair.
Control Number: 24-A-64-HVS
Presentation Number: E7
Quantitation of Aortic Valve Regurgitation: Difference between Single and Biplane Mitral Annulus Area Calculation by Transthoracic Echocardiography
Objective: Continuity method is one of the quantitation methods of valvular regurgitation. ASE guidelines recommend mitral annulus measure calculated with single plane, but there is an argument for using single dimension may be an over-simplification. We investigated single vs biplane mitral annulus area (MAA) calculations in aortic regurgitation (AR) to evaluate their ability of AR severity assessment.
Methods: Patients with moderate or higher AR were retrospectively selected from our echocardiography database between January and June 2018. AR severity was determined based on qualitative and quantitative parameters of comprehensive transthoracic echocardiography (TTE). Patients with prosthesis, other valvular disease, non-sinus rhythms, and significant intracardiac shunt were excluded. In selected 35 patients, 19 patients who had mitral annulus pulsed-wave Doppler recordings were evaluated for mitral annular dimensions of 4 chamber (4Ch) and 2 chamber (2Ch) view. MAA was calculated as a circle using a single dimension and as an ellipse using both dimensions.
Results: Mitral annulus measurements and regurgitant volume (RV) are presented in the table. The mean of the differences between 4Ch derived and biplane derived MAA was 0.13cm2 (95% limits of agreement: -1.43 to 1.69 cm2) with possible proportional bias. For RV, the mean of the difference was -0.51mL (95% limits of agreement: -15.5 to 14.5mL). By ROC curve analyses to evaluate the performance to diagnose severe AR, the area under curve is 0.84 by 4Ch derived RV, 0.80 by 2Ch derived RV, and 0.87 by biplane derived RV.
Conclusions: Both single and biplane measures for continuity method show decent diagnostic ability. However, proportional bias and wide limits of agreement exist in single vs biplane quantitation method. Further research and methodological improvement including 3DTTE is warranted.
Mitral Annulus Measurements and Calculated Regurgitant Volume by Echocardiography
AR severity
Moderate (n=14)
Severe (n=5)
LVEF(%)
61±5
60±6
Mitral Valve Annulus Dimension by 4Ch (cm)
3.16±0.24
3.43±0.34
Mitral Valve Annulus Dimension by 2Ch (cm)
3.16±0.26
3.30±0.28
MItral Annulus Area using 4Ch (cm2)
7.89±1.24
9.30±1.91
MItral Annulus Area using 2Ch (cm2)
7.89±1.26
8.62±1.43
MItral Annulus Area using 4Ch/2Ch (cm2)
7.86±1.01
8.92±1.34
Regurgitant Volume using 4Ch (mL)
40±22
60±6
Regurgitant Volume using 2Ch (mL)
39±25
64±15
Regurgitant Volume using 4Ch/2Ch (mL)
40±22
62±8
Control Number: 24-A-97-HVS
Presentation Number: C1
Experimental Flow Field Assessment of the TRIFLO Valve Compared to State-of-the-art Surgical Valve Prostheses
Authors:Lorenzo Ferrari, Dominik Obrist
ARTORG Center, University of Bern, Bern, Switzerland
Abstract Body:
Objective: Limited data are available on prosthetic heart valve performance at reduced and increased cardiac output (CO) as most studies were carried at 5L/min. This study aims to close this gap by investigating blood flow patterns in aortic mechanical (MHV) and biological (BHV) heart valves at low, normal and elevated CO using Tomographic Particle Image Velocimetry (Tomo-PIV).
Methods: Two MHVs (TRIFLO, Novostia; On-X, CryoLife) and a BHV (PERIMOUNT, Edwards Lifesciences) of 21mm were mounted in a pulse duplicator. The three-dimensional flow field was measured with a multi-view imaging system (Tomo-PIV). The flow rate was set at 3, 5 and 7L/min with aortic pressure of 60/40, 120/80 and 170/105mmHg for low, normal and elevated CO, respectively.
Results: Three valves had similar flow rates but varied in systolic retrograde flow. The tri-leaflet valves showed similar flow topology characterized by a central systolic jet, with three side jets in the sinuses for the TRIFLO. The BMHV featured two semi-circular jets near the aortic wall and a smaller central jet. The TRIFLO showed lower planar turbulent kinetic energy (TKE) while it was comparable for the BMHV and the BHV. However, peak values were identified closer to the sinuses for the BMHV.
Conclusions: Increasing CO led to higher turbulent kinetic energy and a spatially extended influence of the valve on the flow in the ascending aorta. In all configurations, the BMHV shows higher turbulent production and dissipation rate than other valves. The higher TKE levels near the sinuses associate with higher retrograde flow suggest that the blood flowing back into the sinuses experiences a higher stress level. Lower peak values of TKE and velocity, together with a flow topology similar to the BHV, indicated that blood is exposed to lower level of stress for the TRIFLO.
Control Number: 24-A-156-HVS
Presentation Number: C2
Enhancing Surgical Predictability for Bicuspid Aortic Valve Patients Through a Personalized Fluid-structure Interaction Approach
Authors:Charles Wanna1, Nils P. Johnson1, Krishnan B. Chandran2, Jane Grande-Allen3, Danai Kitkungvan1, Hyunggun Kim4, Danny Ramzy1, David D. McPherson1, Siddharth K. Prakash1, Vijay Govindarajan5
1University of Texas Health Science Center, Houston, TX, USA, 2The University of Iowa, Iowa City, IA, USA, 3Rice University, Houston, TX, USA, 4Sungkyunkwan University, Suwon, Korea, Republic of, 5Boston Children's Hospital, Boston, MA, USA
Abstract Body:
Objective: Bicuspid aortic valve (BAV) represents the most prevalent congenital heart anomaly, affecting approximately 1.4% of the population. This condition elevates the risk of aortopathy, involving coarctation, aneurysms, dissection, and accelerated calcification leading to stenosis or aortic insufficiency. The quantification of BAV function, the alteration of blood flow, and the resulting hemodynamic forces, along with their influence on the accelerated deterioration of BAV, plays a crucial role in enhancing the diagnosis of BAV. Furthermore, the ability to predict how these parameters may improve following interventions holds the potential to enhance surgical predictability and long-term patient outcomes.
Methods: A protocol for modeling specific to individual patients, utilizing patient image data and employing a robust fluid-structure interaction (FSI) technique, was developed for the assessment of BAV. This protocol involved simulating the flow through the left ventricle, BAV, ascending and descending aorta to gain insights into the biomechanical aspects near the valve area and to investigate its downstream effects. Our analysis included comparative analysis of the diseased anatomy with virtual interventions of surgical aortic valve replacement (SAVR) (Fig 1A-B).
Results: According to our model's predictions, level of viscous dissipation (or energy loss) that was observed in the compromised BAV was considerably mitigated following virtual intervention of SAVR (Fig. 1C). More precisely, during peak systole, energy loss decreased by a factor of ∼2.5 after implementing the SAVR procedure, simultaneously leading to a notable enhancement in the effective orifice area. In the BAV, valve stresses was highest specifically in the raphe region (Fig. 1D).
Conclusions: Our workflow provides crucial insights into BAV dynamics, aiding in personalized intervention selection. These insights can enhance diagnostic accuracy, predict surgical results, optimize treatments, and aid clinical decision-making for at-risk BAV patients.
Control Number: 24-A-161-HVS
Presentation Number: C3
Computational Fluid-structure Interaction Models of Transcatheter Aortic Valve Replacement: CoreValve Evolut R Vs. SAPIEN 3
Authors:Jordan A. Brown1, David Wells2, Jae H. Lee3, Margaret Anne Smith4, Aaron Barrett5, Charles Puelz6, Arash Kheradvar7, John P. Vavalle4, Boyce E. Griffith2
1Belmont University, Nashville, TN, USA, 2University of North Carolina at Chapel Hill, Chapel Hill, NC, USA, 3US Food and Drug Administration, Silver Spring, MD, USA, 4University of North Carolina at Chapel Hill School of Medicine, Chapel Hill, NC, USA, 5University of Utah, Salt Lake City, UT, USA, 6Baylor College of Medicine, Houston, TX, USA, 7University of California, Irvine, Irvine, CA, USA
Abstract Body:
Objective: Computer modeling and simulation (CM&S) is an important tool in the process of Transcatheter Aortic Valve (TAV) device design, regulatory approval, and indication in the care of specific patients, since there are still many open questions surrounding post-implantation complications. Improved computational models beyond those in the existing literature have the ability to provide more accurate performance predictions for individual patients.
Methods: We present computational fluid-structure interaction models of the Evolut R and SAPIEN 3 using the immersed finite element-difference method. We perform dynamic simulations of crimping and deployment of both devices as well as their behavior across the cardiac cycle in a patient-specific aortic root anatomy reconstructed from CT image data. These simulations incorporate biomechanics models fit to experimental data and automatically capture the contact between the devices and the native anatomies. We apply realistic driving and loading conditions based on clinical measurements of human ventricular and aortic pressures and flow rates.
Results: Our models provide informative performance predictions consistent with clinical data, such as pre- and post-procedure transvalvular pressure differences, detailed flow patterns (Fig. 1), leaflet dynamics, and valve orifice areas. They show a significant difference in the flow patterns and pressure differences between the two devices.
Conclusions: The main contribution of this work is a detailed computational modeling framework for TAVR devices and a patient-specific comparison of the performance of two common TAVs. Ultimately, CM&S of TAVR devices with patient-specific models has the potential to enhance clinicians’ ability to personalize treatment planning to improve long-term prognoses.
Control Number: 24-A-153-HVS
Presentation Number: C4
The Role of Estimated Pulmonary Artery Pressure and C-reactive Protein in Heart Failure with Preserved Ejection Fraction: Machine Learning Methods
Authors:Roza Badr Eslam1, Beguem Oeztuerk1, Franz Duca1, Christina Binder-Rodriguez1, René Rettl1, Theresa Dachs1, Luciana Camuz Ligios1, Hong Qin1, Farideh Alasti1, Zohreh Toghrayee Semiromi2, Johannes Kastner1, Diana Bonderman1
1Medical University of Vienna, Vienna, Austria, 2University of Tehran, Tehran, Iran, Islamic
Abstract Body:
Objective: A widely recognized subtype of heart failure, with high morbidity and mortality rate, heart failure with preserved ejection fraction (HFpEF) is of absence of risk factors as a main challenge. Identifying the most important risk factors for this disease helps us to find effective therapies. Data analytics promises to do just that. Our study proposed the finding of most important risk factors of time to death and heart failure hospitalization by using appropriate machine learning methods.
Methods: In this research, 427 patients were under observation and about 76 characterizes including laboratory, imaging, basic characteristic, comorbidities, and right-sided heart catheterization (RHC) parameters, were measured. The whole observation duration of the study was up to 60 months. In order to detect effective risk factors, we applied different machine learning methods including support vector machine, decision tree, and Cox hazard model.
Results: The most prominent risk factors capable of predicting cardiac death time identified through Cox hazard model are CRP, estimated systolic PAP measured by echocardiography (EchosPAP), NT proBNP, six-MWT, and HbA1c as a marker for typ2 diabetes (p-value< 2.2e-16). Accuracy of these five risk factors which are 10% of whole variables to predict of cardiac death time was more than 77%, a considerably value. It is worthy to note that among these five prominent risk factors, accuracy of EchosPAP and CRP to predict death time was 70%, a dramatically part of total accuracy. Secondly, these five risk factors were at top variables in the survival decision tree model (Figure 1).
Conclusions: Our findings demonstrated that EchosPAP and CRP are dominant variables in predicting death time in HFpEF patients.
Control Number: 24-A-89-HVS
Presentation Number: C5
Computational Predictive Modeling for Bicuspid Transcatheter Aortic Valve Replacements
1The Ohio State University, Columbus, OH, USA, 2Piedmont Hospital, Atlanta, GA, USA, 3Georgia Institute of Technology & Emory University, Atlanta, GA, USA
Abstract Body:
Objective: The objective of this study was to evaluate our systematic use of computational predictive modeling prior to high-risk TAVR for bicuspid aortic valvulopathy (BAV).
Methods: 185 TAVR patients, 60 of which had elevated risk bicuspid aortic valve anatomy (excessive calcification), underwent prospective computational modeling to assess risk of aortic root injury and paravalvular leak (PVR). Many of the TAVR procedures were modified by either adding or subtracting volume from the balloon expandable valve (BEV), or pre/post dilating the TAVR prosthesis to avoid aortic root injury or PVR. Patients with high risk for PVR or root injury were offered surgery.
Results: The average patient age was 67.8 ± 9.95 and the majority were male (76.3%). Among the cohort, 9 patients received additional volume to the balloon during expansion to combat PVR and 11 had volume removed. Pre-dilation was performed for 2 patients and post-dilation was performed on 11 patients. 17 patients were offered surgery. Of the 43 patients who underwent TAVR, 67% had none/trace PVR, 9.3% had mild PVR, and 6.9% had moderate PVR. None of the patients had severe PVR or an aortic root injury. Complications unrelated to root injury or PVL were noted in the remaining 16.8% of patients.
Conclusions: Simulation of TAVR device deployment in BAV patient-specific enhances procedural planning to reduce risk of aortic root injury and PVR. Additionally, it leads to increased TAVR utilization in patients with complex aortic valvular and root pathology.
1The Ohio State University, Columbus, OH, USA, 2Baylor Scott & White The Heart Hospital, Plano, TX, USA, 3Georgia Institute of Technology & Emory University, Atlanta, GA, USA
Abstract Body:
Objective: Although aortic root rupture only occurs in less than 1% of Transcatheter Aortic Valve Replacement (TAVR) procedures, it can be a lethal complication. Additionally, several anatomies may be at increased risk, including heavy annular and LVOT calcium and bicuspid aortic valve pathology. This study aimed to analyze the sensitivity and specificity of peak areal stretch computationally derived from pre-TAVR computed tomography (CT) as a variable to predict aortic root rupture.
Methods: Pre-TAVR CT scans from 40 patients (35 tricuspid and 5 bicuspid) who had undergone TAVR at Baylor Scott & White The Heart Hospital were subjected to FDA approved computational simulation modeling (Dasi Simulations). Peak areal stretch corresponding to calcific nodule displacement induced aortic tissue deformation was extracted in a manner blinded to the clinical outcome of each case. Quantitative areal stretch were obtained in the right coronary sinus (RCS), left coronary sinus (LCS), and non-coronary sinus (NCS).
Results: Sensitivity and specificity curves were plotted to analyze the how well peak areal stretch will predict root rupture. When plotted (1 outlier excluded), the area under the curve at a peak area stretch of 1.8 was 0.84. When only the female patients in the cohort were analyzed, the AUC was 0.92 at a peak area stretch of 1.7.
Conclusions: Pre-TAVR CT derived peak areal stretch using the Dasi Simulations computational model is predictive of aortic root rupture thereby helping quantitatively risk stratify.
Control Number: 24-A-84-HVS
Presentation Number: C7
Patient-specific Silicone 3d Models of the Aortic Valve for TAVR Planification
Centre hospitalier de l'Université de Montréal, Montreal, QC, Canada
Abstract Body:
Objective: To develop patient-specific, cost-effective, anatomical silicone 3D models of the aortic valve to use them for TAVR planification.
Methods: 3D volumes of the aortic root are segmented from the planning CT scan using the open-source software 3D Slicer. They are then imported into the computer-aided design software Fusion 360 to create negative molds of the aortic valve. Molds are 3D printed by fused deposition modeling with an Ultimaker S5 printer using polylactic acid (PLA) and polyvinyl alcohol (PVA). Two silicone types from the brand Smooth-On were used to mold models of the valve with a 2 mm wall, Ecoflex 00-30 and Dragon Skin 10NV, the latter being the stiffest.
Results: To test our workflow and design, a comparison of valves made from the scan of a patient who underwent surgical aortic valve replacement was performed. The patient’s native valve was appreciated intraoperatively before the replacement to compare it to both models. For the two models, leaflets are slightly thicker than those on the native valve. The surgeon’s appreciation of the materials is that the calcified leaflets are slightly stiffer in the native valve when compared to the stiffest of both silicone used. The native aortic wall stiffness lies between the softest and the stiffest models.
Conclusions: The intraoperative comparison of 3D silicone models will be done with additional patients to adjust the design and choice of materials, mixing both silicone yields stiffness values that can be adjusted. Once satisfying results are achieved, they will be used to simulate TAVR deployments, allowing planning for complications such as paravalvular leaks and coronary ostia obstruction, with an emphasis on valve in valve as a future second procedure. We also aim to develop a system to test the hemodynamic properties of the models.
Control Number: 24-A-70-HVS
Presentation Number: C8
Multiphysics Modeling of a Patient-specific Transcatheter Edge-to-edge Repair (teer) for Mitral Regurgitation: The Prediction and Assessment of Key Structural and Hemodynamic Outputs for Clinical Decision-making
Authors:Jiang Yao1, Tom Battisti1, Philippe Guilhou2
1Dassault Systemes, Johnston, RI, USA, 2Dassault Systemes, Velizy, France
Abstract Body:
Objective: Clinical decisions and assessments around TEER rely on key biomarkers such as effective orifice area, transmitral pressure gradient, LA pressure, and regurgitation volume. A patient specific predictive model is created, calibrated with preoperative data, and used to replicate postoperative acute responses.
Methods: This study compares outputs from a patient-specific model to clinical measurements for a secondary mitral valve regurgitation patient. Patient-specific geometry segmented from cardiac computed tomography (CT) and other clinical data are used to create a structural finite element (FE) model. Similarly, a lumped-parameter system (LPM) model is created and employed to capture patient hemodynamics. The models are used in tandem (co-simulation is performed) and quantitative and qualitative comparisons are made of the outputs with the clinical data, including that from transesophageal and transthoracic echocardiography, CT images, and catheterization measurements. The models are calibrated using the clinical data for the pre-operative state after which the treatment outcome is assessed by comparing the model predictions with the clinical measurements following deployment of a TEER device. The comparisons are performed using the clinical data as the reference.
Results: The comparisons are presented for the preoperative state and for the postoperative state. The model demonstrates the ability to predict hemodynamic quantities with less than a 20% error and exhibits reasonable qualitative agreement with the mitral valve shape both before and after treatment.
Conclusions: The model demonstrates robust predictive accuracy, comparable to clinical measurement uncertainty and error levels while effectively capturing mitral valve shape changes before and after a device placement. This underscores its potential as a valuable tool for clinical decision-making and personalized treatment planning in mitral regurgitation.
Control Number: 24-A-118-HVS
Presentation Number: O1
Randomized Trial of Hemoadsorption in Acute Endocarditis
1Montreal heart institute, montreal, QC, Canada, 2Charoenkrungpracharak hospital, Bangkok, Thailand
Abstract Body:
Objective: To evaluate the impact of the pre-emptively use of hemoadsorption connected through cardiopulmonary bypass circuit in valve endocarditis surgery to reduce hypercytokinemia and improve clinical outcomes.
Methods: The infective endocarditis patients required urgent to emergent cardiac surgery from December 2019 to December 2022 were 1:1 randomized between placebo and hemoadsorption group. There were 50 eligible patients excluded IL-6 <10 pg/ml, immunocompromised host and chronic kidney or chronic liver diseases. In study group, blood was filtrated at rate 400 ml/hr throughout bypass time. The primary endpoints were SOFA score and mortality rate, while the secondary endpoints were vasoactive-inotropic score (VIS) at 0, 24, 48 hours postop, ventilation time and IL-6 level throughout perioperative period.
Results: SOFA scores at 0 h postop were 4.46±4.19 and 4±4.57 in study and control group respectively(p=0.779). The SOFA scores at 24 hr postop were 4.76±4.24 and 4.5±4.10 in study and control group respectively(p=0.870). The VIS score at 24 and 48 hr postop in study group was lower yet statistically significant (VIS24h: study group at 23.07±58.60 vs control group at 35.78±58.77, p=0.622 and VIS48h: study 23±76.73 vs control 28.08±51.99, p=0.810). The IL-6 level were not different among the period but the reduction rate in study group is rapid descending from 0-12 h.
Conclusions: Despite the insignificant result in using hemoadsorption in acute endocarditis patient required cardiac surgery, we also noticed significant rapid reduction in IL-6 level at immediate postoperative phase. Postoperatively, high cytokine level in infective endocarditis surgery may attributate to CPB usage, septic shock process and manipulation/spreading of vegetation during the surgery. Data on application of Hemoadsorption in cardiac surgery is limited, but show some anticipation to diminish CPB-associated SIRs.
Control Number: 24-A-35-HVS
Presentation Number: O2
Underlying Valve Disease in Patients Meeting Imaging and Diagnostic Criteria for Cardiac Sarcoidosis
1Albany Medical Center, Albany, NY, USA, 2Rutgers RWJ, New Brunswick, NJ, USA
Abstract Body:
Objective: Cardiac sarcoidosis (CS) diagnostic guideline includes cardiac dysfunction as a major CS diagnostic criterion. Valvular disease can cause cardiac dysfunction independently of CS. Limited data is available with regards to valvular disease in CS according to 2017 diagnostic criteria.
Methods: A case control, single tertiary medical center study included 558 sarcoidosis patients (52.7% females, 58.9+/-12.6 years-old) with documented extracardiac sarcoidosis. Complete echocardiographic and/or cardiac MRI assessment were available in 540 patients. The study cohort included 52.5% females(293/558). Diabetes was prevalent in 29.2%(163/558), HTN in 51.1%(285/558), CAD in 12.9%(72/558), ESRD in 2.4%(13/549), and COPD in 6.8%(38/558).
Results: Moderate or severe mitral (MV), aortic (AV), or tricuspid (TV) regurgitation and/or stenosis were noted in 14.2%(79/558) of patients, present in 15.7%(46/293) females and 13.5%(33/265) males, p=0.686. Valvular disease was significantly more common in patients fulfilling major CS ECHO and/or MRI imaging criteria, 33.3%(26/78) vs. 11.7%(54/462) in the rest of the cohort, p<0.001. In patients fulfilling major CS ECHO and/or MRI imaging criteria, MV disease was most common, occurring in 53.6%(15/26), followed by TV in 22.7%(5/22) and AV in 20%(5/25), p<0.001. Valvular disease was noted in 29.2%(163/558) of DM patients and in 12.9%(72/558) of CAD patients. Similar to the rest of the cohort, in patients with DM fulfilling major CS criteria, MV disease was most common, occurring in 58.6%(17/29), followed by AV in 37%(10/27) and TV in 34.8%(8/23), p=0.002. On the contrary, in CAD patients fulfilling major CS criteria, AV disease was most common, occurring in 29.6%(8/27), followed by MV in 24.1%(7/29) and TV in 13%(3/23), p=0.011.
Conclusions: Moderate and severe valvular disease occurs in a large proportion of CS patients, with significantly increased prevalence in patients with DM. No gender differences were observed in patients with valve disease. Additional studies are needed to investigate the contribution of valvular abnormalities and co-morbidities to left ventricular dysfunction in CS.
Control Number: 24-A-88-HVS
Presentation Number: O3
The Impact of Patient Demographics on Discharge Patterns Following Valve Surgery
Authors:Jessica Katsiroubas, Sandhya Balaram
New York Presbyterian Brooklyn Methodist, Brooklyn, NY, USA
Abstract Body:
Objective: This retrospective study was performed to determine significant demographic factors associated with length of stay and patient disposition after cardiac valve surgery.
Methods: The New York Statewide Planning and Research Cooperative System (SPARCS) database was queried to identify patients who had undergone non-endovascular cardiac valve surgery over one year. Patient demographics including gender, race, and age were collected. Primary outcomes analyzed were length of stay and patient disposition.
Results: Data was reviewed on 4,815 patients who underwent a non-endovascular heart valve procedure in 2021. Males comprised 62.2% of patients. Age was categorized into five groups, with the largest proportion, 48.9%, falling within the 50 to 69 age range. Race data indicated that 67.1% were White, 9.1% were Black/African American, 1.2% were multiracial, and 22.7% identified as Other. The mean length of stay (LOS) for all patients was calculated at 11.4 days. Black/African American patients had the longest mean LOS at 14.3 days. White patients had an average LOS of 10.2 days, multiracial patients stayed an average of 11.3 days, and those identifying as other races averaged 13.7 days. Discharge disposition showed 47.6% were discharged home. A significant portion, 64.8%, of these patients were male, and 66.1% were White. Only 3.4% of patients were discharged to an inpatient rehabilitation facility, and within this group, 54.4% were aged 70 or older. Patients discharged to an inpatient rehabilitation facility averaged a LOS of 22.3 days versus 10.2 days for patients discharged home.
Conclusions: A variety of underlying factors influence the hospital stay and discharge patterns after cardiac valve surgery in New York State. Further research and analysis would be beneficial to understand the drivers of these trends in order to improve quality of care and resource allocation.
Control Number: 24-A-99-HVS
Presentation Number: O5
Investigation of Sinus Washout and Platelet Activation in Transcatheter Valve Thrombosis Patients
1ARTORG Center for Biomedical Engineering Research, University of Bern, Bern, Switzerland, 2Department of Cardiology, Inselspital, University of Bern, Bern, Switzerland
Abstract Body:
Objective: Transcatheter heart valve thrombosis (THVT) might reduce leaflet mobility and contribute to valve degeneration. Pre-procedural images of TAVI patients (Bern TAVI registry) indicate larger ascending aorta (AAo) dimensions for patients diagnosed with THVT compared to unaffected TAVI patients. As high shear stresses and flow stagnation are related to thrombus formation, this computational study targets to quantify the sinus washout in larger aortic geometries and assess platelet activation.
Methods: Computational models of a larger AAo model (dAAo=33mm) and a control model (dAAo=29.7mm) of an aortic root with biological tissue valve are created. Fluid-structure interaction simulations are performed coupling a high-order Navier-Stokes solver for blood flow with a structural solver for aorta and valve by an Immersed Boundary method. Mass-less Lagrangian particles are injected upstream of the valve and traced. Particles are categorized whether directly advected in the AAo, contributing to sinus washout or stagnating in sinus. To assess possible platelet activation potential of each group, we calculate platelet activation indices accounting for accumulated shear stresses.
Results: Lagrangian particle tracing shows the advection through the AAo of most particles for control and larger AAo model. However, a lower percentage of particles contributes to sinus washout (-34.1%) in larger AAo. Also, the possibility of particles stagnating once entering the sinus is higher (+7.7%) compared to the control model. Cumulative shear stresses expressed as platelet activation indices hold higher activation potential for particles stagnating in the sinus for the larger AAo model (+39.6%).
Conclusions: The combination of less particles contributing to sinus washout with higher platelet activation potentials for stagnating particles suggests lower washout efficiency and higher risk for accumulation of activated platelets in the sinus. These observations could provide an explanation for the relation between the occurrence of THVT and larger aortic dimensions.
Control Number: 24-A-17-HVS
Presentation Number: O7
Impact of Drop Off Primary Prevention in Sars-cov 2 Times and Its Impact on Emerging Cardiac Pathology
Authors:Elisabet Berastegui Garcia, Christian Muñoz Guijosa, Hipolito Perez Molto, Enrique Moret Ruiz, Carlos Labata, Jorge Lopez Ayerbe, Antoni Bayes Genis
Hospital Universitari Germans Trias i Pujol, badalona, Spain
Abstract Body:
Objective: The SARS-COV 2 pandemic has disrupted [c1] many processes of care related to prevention, diagnostic and therapeutic interventions, including emergency cardiac conditions. Primary care focused on COVID-19 management and vaccination has led to a preventive and therapeutic gap of many chronic conditions and risk factors, including hypertension, a main trigger for acute aortic dissection (AAD). To evaluate the increase in aortic pathology (AD) after the first lockdown
Methods: Retrospective study of 111 patients who underwent AD surgery in our center in the period 2015-2023. We analyzed incidence, technique, morbidity and hospital mortality comparing three periods (pre-SARS-COV 2 (1), SARS-COV 2 (2) and post-first lockdown, (3).
Results: There were no significant differences in relation to age or sex. We observed a significant difference in the incidence of AD between the three periods (1, 2 and 3), presenting a cumulative incidence of 12 ptes/year; 8 ptes/year and 23 ptes/year respectively. High blood pressure was the most frequent risk factor: 85%, 75% and 70%, and the absence of treatment was significantly higher in group 3: 16 (26%), 2 (25%) and 23 (42%). The majority surgical technique in the three periods was ascending aorta replacement; Cerebral anterograde protection was performed in all patients. There were no significant differences in mortality between periods, being 4 (6%), 1 (12%) and 2 (3%).
Conclusions: There is a decrease in emerging cardiac pathology during lockdown with an increase in different urgent pathologies such as aortic dissection. The difficult control of cardiovascular risk factors, at a time when resources and the system are saturated, could be the cause of this increase. Cardiovascular education and prevention continue to play a fundamental role in the prevention of any cardiac pathology.
Control Number: 24-A-33-HVS
Presentation Number: O9
Contemporary Management of Tricuspid Valve Endocarditis: Real World Experiences of Three Treatment Modalities
Authors:John Eisenga1, Kyle McCullough2, Ghadi Moubarak2, Radhika Vaishnav2, Lee Hafen3, Justin Schaffer3, Katherine Harrington3, Robert Smith3, Timothy George3, William Brinkman3, Kelley Hutcheson3, Molly Szerlip3, Sameh Sayfo3, Srinivasa Potluri3, Michael J. Mack3, J. Michael DiMaio3
1Baylor University Medical Center, Dallas, TX, USA, 2Baylor Scott and White Research Institute, Dallas, TX, USA, 3Baylor Scott and White The Heart Hospital Plano, Plano, TX, USA
Abstract Body:
Objective: Advancements in non-surgical valve intervention have created another route for management of tricuspid valve endocarditis (TVE). Little information exists regarding the results of catheter-based intervention in conjunction to other treatments. We performed a single-center retrospective analysis of patients treated for TVE at our institution.
Methods: A single center retrospective review was performed for patients treated for TVE from January 2020 to September 2023. Patient records were identified and reviewed for the outcomes of interest. The primary outcome was 30-day mortality. Secondary outcomes included: survival to discharge, 1-year survival, length of stay, complications, and discharge disposition. This study was approved by our institutional review board, and informed consent waived due to the retrospective nature.
Results: 23 patients were treated for TVE. Seven patients were managed with antibiotics solely, median age of 52 years [33.5-75], 28.5% (2/7) with history of IV drug usage. Four patients underwent Angiovac aspiration of TVE, median age of 31 years [27.75-37.25], 50% (2/4) with history of IVDU. Twelve received a tricuspid valve operation, median age of 47.5 years [32.5-64.5], 25% [3/12] with history of IVDU. 30-day survival was 57% (4/7) in the medical management cohort, 100% (4/4) in the catheter cohort and 100% (12/12) in surgical patients. One-year survival in these groups was 57% (4/7), 100% (4/4), and 83% (10/12) respectively. Survival to discharge in the medical management group was 75% (6/8), while it was 100% in both the catheter and surgical groups.
Conclusions: Our early experiences with Angiovac aspiration of TVE demonstrate zero in hospital mortalities along with excellent 30-day and 1-year mortality rates. Although limited in experience, catheter-based intervention appears to be a useful treatment option for TVE in a high-risk population. This may benefit patients at a prohibitive risk of surgical intervention.
Control Number: 24-A-87-HVS
Presentation Number: O10
Tricuspid Valve Replacement; Not a Metallic Touch
Authors:Yusuf CORBACIOGLU, M.D., M. Cahit SARICAOGLU, M.D., Nur DIKMEN, M.D., M. Bahadir INAN, M.D., A. Ruchan AKAR, M.D. FRCS
Ankara University Medical School, CANKAYA, Turkey
Abstract Body:
Objective: The debate concerning the optimal type and patients of tricuspid position continues. We analyzed the short and long-term results of biological prostheses in patients who underwent isolated or combined tricuspid valve replacement, at our cardiac surgical centre in capital of Turkey.
Methods: From September 2009 to May 2022, 74 patients underwent tricuspid valve replacement. Patients were divided into an isolated group or a combined group according to whether their surgery was combined with a left heart valve or aortic surgery. Mechanical tricuspid valve replacement was excluded and 33 patients underwent bioprosthetic tricuspid valve replacement (isolated group: 21 vs combined group: 12). We reviewed preoperative characteristics and analysed operative data, outcomes and mortality in combined or ITVR groups.
Results: Thirty three patients underwent ITVR, mean age 54,1±15,9 years, 55% female and mean BMI 26,22kg/ m2. Etiologies were functional insufficiency (45%), endocarditis (36%), degenerative (3%), rheumatic (3%) and congenital (3%). Postoperative complications were: need for transfusional support (45.6%), inotropic support longer than 48 hours (38,2%), prolonged invasive ventilation over 24 hours (35,3%), new onset of atrial fibrillation (12.1%), duplication or postoperative creatinine over 2 mg/dl (5.9%), dialysis (9.1%), stroke (3%), intra-aortic balloon pump (6%), permanent pacemaker implantation (3%) and sepsis (3%).Post operative short-term mortality in the combined group was higher (n = 9, 4%) than that in the isolated group (n = 4, 3%).
Conclusions: Every decision regarding tricuspid valve prostheses should be individualized, but in isolated tricuspid valve surgery, biological prostheses replacement may be an optimal choice for patients.
Control Number: 24-A-140-HVS
Presentation Number: M1
Comparison of the Performance of Echocardiographic Parameters to Assess Right Ventricular Dysfunction and Outcomes in Primary Mitral Regurgitation
1Institut universitaire de cardiologie et de pneumologie de Québec - Université Laval, Québec, QC, Canada, 2Hôpital La Cavale Blanche–Centre Hospitalier Régional Universitaire de Brest, Brest, France
Abstract Body:
Objective: Recent studies demonstrated the prognostic value of adding echocardiography-based right ventricular (RV) parameters to the risk assessment of primary mitral regurgitation (PMR). However, the lack of comparative studies on the different RV parameters limits their integration in the assessment of global cardiac function in PMR. This study aimed to evaluate the performance of different parameters assessing RV dilation/dysfunction and their associations with the risk of mitral valve surgery in PMR patients.
Methods: Eight parameters were measured (basal and mid-cavity diameters in apical 4-chamber view [A4C], RV length in A4C view, RV diameter in parasternal long-axis view [PLAX], fractional area change [FAC], tricuspid annulus S' wave velocity by Doppler tissue imaging and plane systolic excursion [TAPSE] by 2D and M-mode) in 209 patients with ≥ mild PMR included in the multicentric PROGRAM study (NCT01835054). The parameters were measured according to the American Society of Echocardiographic (ASE) guidelines in an RV-focused view if available and were tested as continuous and dichotomic variables according to the ASE predefined thresholds.
Results: All RV parameters presented a feasibility ≥78% but did not establish a similar prevalence of RV dysfunction (2-12%). The parameters providing the best intraobserver reproducibility were TAPSE M-mode (intraclass correlation coefficient [95% confidence interval]: 0.99 [0.97-0.99], p≤0.001) and RV diameter in PLAX (0.99 [0.97-0.99], p≤0.001) and the parameter providing the best interobserver reproducibility was TAPSE M-mode (0.95 [0.87-0.98], p≤0.001). After comprehensive adjustment for sex, Charlson index, PMR severity, left ventricle (LV) end-systolic diameter, and LV ejection fraction by Simpson, FAC <35% (hazard ratio [95%CI]: 2.84[1.00-8.03], p=0.05) and RV length >83mm (7.05[1.50-33.10], p=0.01) were significantly associated with mitral valve surgery (83 [40%] events; median follow-up: 5.5[1.6-.8.9]years).
Conclusions: This study suggests that RV length and FAC are the best parameters to assess RV dilation/dysfunction and predict clinical outcomes in PMR patients.
Control Number: 24-A-152-HVS
Presentation Number: M2
Time Independent Myocardial Protection of Single Dose Htk Cardioplegia: Comparison of Conventional and Minimally Invasive Mitral Valve Repair
1University of Halle, Halle, Germany, 2University of Heidelberg, Heidelberg, Germany
Abstract Body:
Objective: Minimally invasive mitral valve surgery may require a prolonged period of myocardial ischemia. Cardioplegic solutions that necessitate a single dose for adequate myocardial protection are evoked to simplify surgery and result to be appealing in this setting. The aim of this study was to assess early outcomes after minimally invasive versus conventional mitral valve repair using one single dose of histidine-tryptophan-ketoglutarate solution (HTK; Custodiol) for myocardial protection.
Methods: A retrospective analysis of prospectively collected data of patients who underwent primary isolated mitral valve repair between 2015 - 2021 was undertaken. Primary end-point was peak CKMB within the first 24 hours after surgery. Secondary endpoints included operation and aortic crossclamp times, in-hospital mortality, hospital and ICU stay, postoperative bleeding and rethoracotomy, and cumulative blood transfusion. All values are given as mean±SD, p<0.05 was considered as statistically significant. Analysis was performed by using the SPSS statistic software.
Results: 276 patients were included in the study (64 conventional vs. 212 minimally invasive procedure). Baseline patient characteristics did not differ between the groups except gender distribution (43,7% vs. 22.2% female, p=0.02). There were no in-hospital death in the whole cohort. Operation and aortic crossclamp times were significantly lower in the conventional group (208±5 vs. 277±4 min, p=0.001 76±20 vs 107±26 min, p=0.001, respectively). Peak CKMB showed no significant differences between the groups (81±53 vs. 76±55 U/l). Postoperative outcome measures did not differ between the groups.
Conclusions: The present data confirms similar outcomes between conventional and minimally invasive mitral valve repair. Despite longer operation and aortic crossclamp times, single dose cardioplegia with HTK solution provides a time independent excellent myocardial protection during minimally invasive surgery.
Control Number: 24-A-73-HVS
Presentation Number: M3
Mitral Valve Replacement with Resilia Mitris Valve in Ischaemic Mitral Regurgitation in Severe Lv Dysfunction with Severe PAH
Authors:VIRENDAR SARWAL
IVY Hospital, Mohali, Chandigarh, India
Abstract Body:
Objective: The objective of this paper was to review surgical management in Ischemic MR with Severe PAH and Severe LV dysfunction
Methods: A 67 year old male old PCI to RCA for IWMI came with new onset DVD , LAD 90% and RI total cut off with Severe MR with Severe PAH and Severe LV dysfunction Ef being 30%. Patient was put on decongestive measures with Sildenafil 12.5mg BD for his PAH and along with carvedilol. His PA pressures coming down to 48mm Hg+ RAP. But again went up74mmHg +RAP after a bit of exertion. It was decided to take him for CABG + MVR with Mitris Resilia Valve. In OR his PAP were Systemic 101/52 mmHg and on TEE Ef was 25%. On CPB he was given 2 RSVG to LAD and RI after cross clamp with St. Thomas Cardioplegia repeated every 15 minutes. Mitral valve replacement done through RA/IAS approach by preserving the posterior mitral leaflet with 25mm Mitris mitral Valve. The guiding arrow was placed anteriorly and single line on Posteromedial Commissure and double line on anterolateral commissure. Came off with hotshot containing aspartate and glutamate. He required heavy inotropic support.
Results: In the immediate post period he was electively ventilated for 48 hrs when PA pressure started coming down to 42/28 . Inotropic support got reduced to half. His ABG settled with no acidosis. He was extubated and got discharged on 7th day with normal PA pressures.
Conclusions: Severe LV dysfunction in CAD with severe MR with severe PAH makes it inoperable and they go to Heart transplant category. But with pre operative preparation and adequate myocardial protection and preserving the posterior leaflet of MV and changing it with a low profile rightly oriented valve giving larger orifice helps in offering such patients surgical management .
Control Number: 24-A-56-HVS
Presentation Number: M4
Evaluation of a Hybrid Surgical Approach for Transcatheter Mitral Valve Replacement in the Domestic Sheep Model
Authors:John P. Carney1, Walt Tollison1, Matthew T. Lahti1, Leo Ogle1, Anna-Maria Kaparos2, Zachary Vidlund2, Michael Evans2, Jill T. Schappa Faustich1, Richard W. Bianco1
1University of Minnesota, Minneapolis, MN, USA, 2Abbott, Maple Grove, MN, USA
Abstract Body:
Objective: Advancements in novel transcatheter mitral valve replacement (TMVR) devices are critical for high risk and nonsurgical patients. However, device development requires long-term studies assessing safety and efficacy in animal models prior to clinical use. Although sheep are well-established preclinical models for surgical valves, the healthy native mitral anatomy impairs percutaneous positioning and securement of TMVR devices, ultimately decreasing long-term survivability and device evaluation. Thus, we aimed to evaluate the feasibility of using a hybrid surgical approach in sheep to determine the chronic performance of a novel TMVR device.
Methods: Eleven 15±2 month old sheep weighing 79±9 kgs were enrolled in this study. Eight Abbott Next-Generation Cephea (Cephea) TMVR devices were implanted using a hybrid surgical approach, with the valve deployed and secured under direct visualization on cardiopulmonary bypass. Three Medtronic Mosaic Bioprostheses (Mosaic) valves were implanted with standard techniques as control articles. Sheep were survived for 20 weeks, followed by humane euthanasia and comprehensive necropsy by a board-certified veterinary pathologist.
Results: All sheep were successfully implanted and recovered from surgery, with 7/8 Cephea and 3/3 Mosaic animals surviving to the 20-week study endpoint. A surgical access-related complication unrelated to TMVR performance resulted in one early death 58 days post-operatively. At term, all Cephea valves performed comparably to explanted control Mosaic valves, appearing well-healed circumferentially within the annulus with competent, flexible, unobstructed leaflets.
Conclusions: Our novel hybrid surgical approach allowed for a comprehensive evaluation of the long-term performance of a next generation Cephea TMVR, with 100% survival at 30 days and 88% at the 20-week endpoint. These results suggest that using a hybrid surgical approach in the sheep model may improve chronic survival in studies evaluating preclinical safety and efficacy of novel TMVR valves.
Control Number: 24-A-21-HVS
Presentation Number: M5
Back to the Left
Authors:Devendra S. Saksena, Sandeep Varma, Shivprasad Shetty, Ankita Choudhary
Bombay Hospital, MUMBAI, India
Abstract Body:
Objective: Mitral Valve is left sided structure and left atrium located posteriorly. We believe that the more direct approach to the mitral valve through the left chest would be better.
Methods: A small Left anterior Lat. thoracotomy on the 4th rib is adequate or Lt. Vertical Anterior Axillary approach. CP Bypass is established with peripheral cannulation.Advantages: 1)Direct access to Mitral Valve.2)Easy and secure excision of the Left Atrial appendage.3)We can accomplish an excellent Maze procedure either surgically or through some other energy source as the Pulmonary Vessels are directly accessible.4)What is more important is that we can reduce the size of the Left Atrium (as patients with a large left Atrium more commonly have Atrial Fibrillation which interferes with establishing of a sinus rhythm), Reduction of the Left Atrial size from a right sided incision is impossible and from the mid sternotomy, very difficult. 5)One can directly look at the quality of Mitral repair if one does Beating Heart Mitral Surgery.
Results: We have done 3 cases in our unit last year with excellent hemodynamic and cosmetic results. The left sided approach either anterior axillary or anterio-lateral thoracotomy are the more direct approach to the Mitral valve and make it easier for the surgeon and do a better procedure for the patient. Surgeons need to move out of their comfort zones in order to do something different and better. If one elects to do a beating heart mitral surgery than this will be a better approach.
Conclusions: Left sided approach is a more direct and better approach for the Mitral Valve.
Control Number: 24-A-61-HVS
Presentation Number: M6
Patient Prosthesis Mismatch After Mitral Valve Replacement: Technical Considerations in Preserving Native MitralValve Leaflets
Authors:Mohammad Hamidi, Dina Al Rameni, Arka Chatterjee, Tushar Acharya, Toshinobu Kazui
The University of Arizona, Tucson, AZ, USA
Abstract Body:
Objective: Patient prosthesis mismatch(PPM) after mitral valve replacement has not been well described compared to aortic valve. Thereports have been contradictory regarding PPM in mitral valve position and clinical outcomes. One has to understandpotential technical pitfall during the mitral valve replacement(MVR). Leaflets preservation/excision techniques can bedetrimental on the new valve size and function.
Methods: We are presenting a case of a patient with normal leftventricular(LV) function and not dilated LV who underwent mitral valve replacement with anterior and posterior leafletspreservation technique who later diagnosed with PPM necessitate redo valve replacement.
Results: A 61-year-old female with history of mitral valve replacement with a 27mm St. Jude Epic valve using bi-leafletpreservation technique for severe mitral valve regurgitation developed progressive worsening dyspnea and chest pain over 1year period after the surgery. TEE demonstrated normal leaflets opening but significant pressure gradient of 15mmHg at HRof 82/min. Based on these findings, patient diagnosed with PPM and we decided to proceed with redo MVR. Intraoperatively,the bioprosthetic mitral valve looked normal, however, the valve size seemed to be undersized due to bileaflet preservationtechnique. After resecting remnant of anterior leaflet and preserving posterior leaflet, we were able to place a 31mm EdwardsMgna Ease. Post replacement TEE showed a mean gradient of 3mmHg with no perivalvular leak. Post-operatively patientprogressed well and discharged home after 5 days.
Conclusions: PPM in mitral valve position can happen with inappropriate size of bioprosthesis. MVR with bi-leaflet preservation techniquecan lead to PPM if the patient has normal LVEF and not dilated LV. Posterior and/or anterior mitral valve leaflets preservationcan lead to PPM especially in patients with normal left ventricular size and function. Careful preservation techniques shouldbe considered to allow bigger valve diameter placement to avoid this detrimental complication.
Control Number: 24-A-151-HVS
Presentation Number: M7
Leaflet Strategies in Mitral Valve Repair: A Risk Assessment for Postoperative Systolic Anterior Motion
Authors:Ayman Raweh, M.D., Alexander Albert, Ph.D
Klinikum Dortmund, Dortmund, Germany
Abstract Body:
Objective: This research aims to examine the impact of mitral valve geometry and left ventricular dimensions on the risk of postoperative Systolic Anterior Motion (SAM) following mitral valve repair (MVRr). It assesses two surgical strategies: "Respect," using shortened neochordae to shift the posterior leaflet, and "Resect," removing a section of the leaflet. The goal is to identify which approach is more effective in preventing postoperative SAM.
Methods: We reviewed 222 MVRr surgeries performed between July 2015 and March 2020. Exclusion criteria included patients with primary SAM due to hypertrophic obstructive cardiomyopathy or prior MVRr. The study used preoperative, intraoperative, and postoperative echocardiograms to evaluate mitral valve and ventricular geometry. A range of patient and procedure-related factors were examined to identify potential SAM risk factors.
Results: Out of 222 patients, 213 (96%) did not experience postoperative SAM. The Respect approach was used in 199 patients, with 8 (4%) experiencing SAM, while the Resect approach was used in 23 patients, with 1 (4.4%) experiencing SAM (P-value 0.469). SAM was detected intraoperatively in 6 cases and postoperatively in 3. Treatment options for SAM included medical management in 2 cases, surgical re-intervention in 3, and valve replacement in 4.
Conclusions: No significant difference was observed in postoperative SAM occurrence between the Respect and Resect techniques. The study suggests that increasing leaflet coaptation height may reduce the length of the "residual" anterior leaflet, potentially lowering the risk of SAM post-surgery.