Control Number: 24-A-51-HVS
Presentation Number: 1
Publishing Title: Clinical Course Of Severe Pediatric Aortic Valve Stenosis: A Single-center Experience
Author Block:
Maximiliaan L. Notenboom, BSc, Sencer Albayrak, BSc, Jonathan R. Etnel, MD PhD, Kevin M. Veen, MD PhD, Jolien W. Roos-Hesselink, MD PhD,
Ingrid M. van Beynum, MD PhD,
Pieter C. van de Woestijne, MD,
Willem A. Helbing, MD PhD,
Johanna J. Takkenberg, MD PhD, Ad J. Bogers, MD PhD
Erasmus University Medical Center, Rotterdam, Netherlands
Abstract Body:
Objective: Congenital valvular aortic stenosis (AS) in children requires lifelong follow-up, and often multiple interventions. An overview of patient journeys after diagnosis of severe AS is lacking. This study aims to illuminate the possible (treatment-)pathways after diagnosis of severe valvular AS in children.
Methods: Clinical and echocardiographic data of children diagnosed with severe congenital valvular AS at a single center between 1985-2022 were retrospectively collected. Kaplan-Meier analysis was used for time-to-first-event data, followed by a visual overview of recurrent interventions.
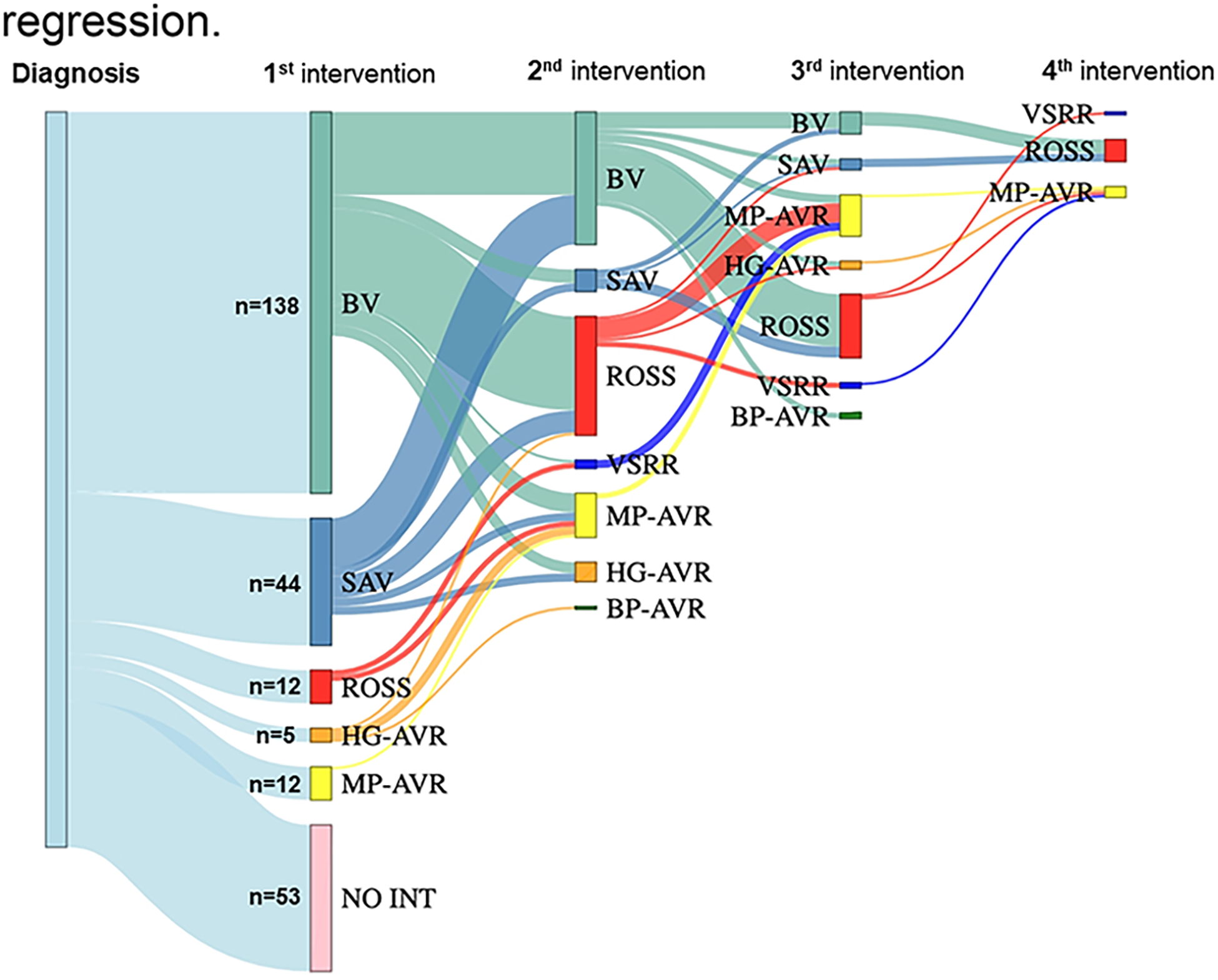
Results: In total, 264 children (median age: 1.2 years(IQR:0.1-7.0y), 73.1% male) were diagnosed with severe valvular AS, including 53 neonates (<30d;20.1%), 76 infants (30d-1y;28.8%), 95 children (1y-12y;36.0%) and 40 teenagers (12y-18y;15.2%). Median follow-up was 14.6 years (IQR:5.4-26.2years). Thirty-year survival after severe AS diagnosis was 84.6%(95%CI:78.5-91.2%), compared to 98.7% in the matched-general-population. Thirteen (46.5%) of all 28 deaths occurred in neonates in the first two years following diagnosis. Two-hundred-and-eleven children (79.9%) underwent 402 aortic valve interventions (average of 1.5/patient). Among interventions, most common was balloon valvuloplasty (47.5%), especially in neonates/infants, followed by aortic valve replacement (37.5%), especially in children/teenagers. Median time-to-intervention was 0.17(IQR:0.03-1.17) years and ten-year freedom from first aortic valve intervention was 17.1%(95%CI:12.7-22.9%). Of 53 children without an intervention, thirty-three children (12.5%) showed sustained regression to mild/moderate AS, with a 20-year survival of 100%. Ten children (3.8%) had asymptomatic AS that remained severe and four children (1.5%) died before a planned intervention.
Conclusions: Severe pediatric AS is associated with satisfactory long-term survival if diagnosed after the neonatal period, but may necessitate multiple, widely varying interventions in most children. In one-out-of-five children, no intervention was performed and in one-out-of-eight children, sustained regression of the peak gradient to mild-or-moderate AS without intervention was observed, highlighting the need for further insights into predictors of disease severity regression.
Control Number: 24-A-123-HVS
Presentation Number: 2
Publishing Title: Real-world Data On The Avalus™ Pericardial Aortic Valve: Initial Results From A Prospective, Multi-center Registry
Author Block:
Tom Verbelen1, Jean-Christian Roussel2, Koen Cathenis3, Giovanni Troise4, Lenard Conradi5, Julien Guihaire6, Christian Lildal Carranza7, Paolo Centofanti8, Javier Estigarribia9, Davide Pacini10, Nicolas Doll11, Juan Bustamante-Munguira12, Alberto Giovanni Tripodi13, Laurent De Kerchove14, Tine Philipsen15, Roberto Lorusso16, Lorenzo Menicanti17, Antti Valtola18, Ruggero De Paulis19, Jean Defraigne20, Ben Gal Yanai21, Francesco Musumeci22, Chris Van Kerrebroeck23, Leonid Sternik24, Andreas Liebold25, Bart Meuris1
1University Hospitals Leuven, Leuven, Belgium, 2Centre Hospitalier Universitaire de Nantes, Nantes, France, 3Academisch Ziekenhuis Maria Middelares, Gent, Belgium, 4Fondazione Poliambulanza Istituto Ospedaliero, Brescia, Italy, 5University Heart and Vascular Center Hamburg, Hamburg, Germany, 6Hôpital Marie Lannelongue, Groupe Hospitalier Paris Saint-Joseph, Le Plessis Robinson, Paris, France, 7Rigshospitalet, Kopenhagen, Denmark, 8Azienda Ospedaliera Oridine Mauriziano Torino, Torino, Italy, 9Hospital Universitario Hospiten Rambla, Santa Cruz de Tenerife, Spain, 10Ospedaliero-Universitaria Sant’Orsola-Malpighi, Bologna, Italy, 11Schüchtermann-Klinik, Bad Rothenfelde, Germany, 12Hospital Clínico Universitario, Valladolid, Spain, 13Maria Cecilia Hospital, Cotignola, Italy, 14Cliniques universitaires Saint-Luc, Brussels, Belgium, 15UZ Gent, Gent, Belgium, 16Maastricht University Medical Center, Maastricht, Netherlands, 17Policlinico San Donato, Milan, Italy, 18Kuopio University Hospital, Kuopio, Finland, 19European Hospital, Rome, Italy, 20CHU Liège, Liège, Belgium, 21Tel Aviv Medical Center, Tel Aviv, Israel, 22San Camillo Hospital Roma, Rome, Italy, 23ZOL Genk, Genk, Belgium, 24Haim Sheba Medical Center, Ramat Gan, Israel, 25Universitatsklinikum Ulm, Ulm, Germany
Abstract Body:
Objective: The Avalus™ pericardial aortic valve was introduced into worldwide clinical practice in 2017. Evidence-generating clinical research is mainly based on randomized controlled trials. However, the ACE (Avalus Clinical Evidence) investigators aim to report from a prospective, real-world registry.
Methods: The ACE registry is a prospective, observational, single-arm, multi-center registry aiming at 1000 inclusions throughout Europe and the Middle-East. Aortic valve replacement (AVR) in patients < 18 years and salvage procedures are the only exclusion criteria. Outcome is evaluated in accordance with VARC-2 criteria.
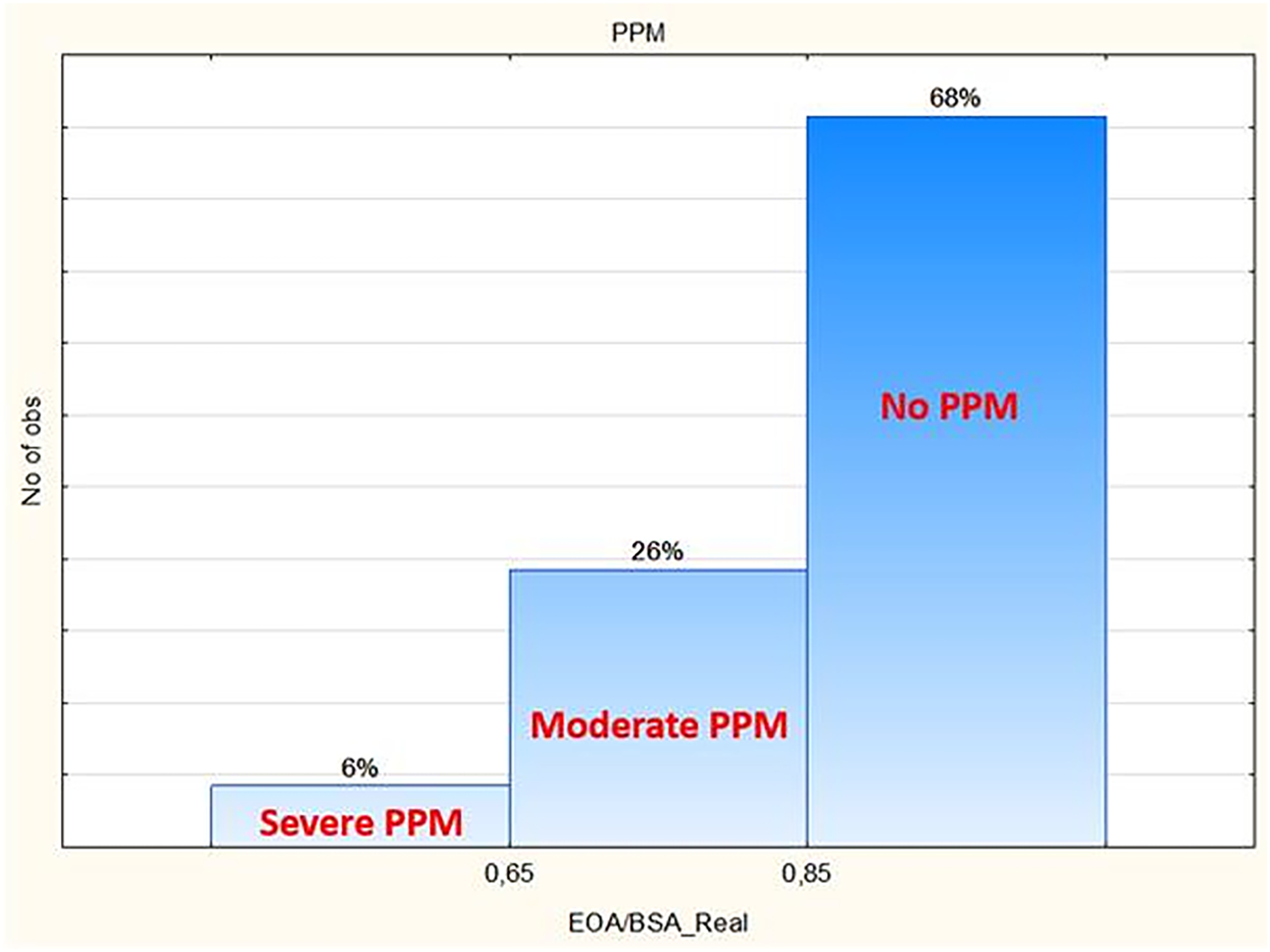
Results: Up to September 2023, 719 patients from 25 centers are enrolled. Mean age is 72±6 years (42-87), mean EuroSCORE II is 3.2±5.1 (0.5-62). Combined surgery (57%, n=410) consists out of CABG (27%, n=194), double valve (8%, n=57), triple valve (3%, n=23), ascending aorta (14%, n=102), ablation (5%, n=33) or other combinations (12%, n=89). Minimal access is used in 43% (134/311) of single AVR cases. Early mortality and stroke rates are low: 1.7% (n=12) and 1.5% (n=11) respectively. In single AVR, these death and stroke rates are 0.6% (2/311) and 0.6% (2/311), respectively. Postoperative hemodynamics show peak and mean gradients of 21±8 mmHg and 12±5 mmHg, respectively; effective orifice area (EOA) of 2.0±0.6 cm2 and an EOA-index of 1.1±0.2. This results in 68% having no patient-prosthesis mismatch (PPM); 26% having moderate PPM and 6% severe PPM (Fig. 1). Paravalvular leakage >1/4 is present in 0.1% (n=1) of cases. Postoperative pacemaker implantation is needed in 3.5% (n=25).
Conclusions: The first results from a real-world, prospective, multi-center registry on the Avalus™ valve show very low rates of early major events and excellent hemodynamics with low gradients and low PPM rates. This registry aims to enroll 1000 patients from more than 30 centers and will continue to monitor the outcome.
Control Number: 24-A-53-HVS
Presentation Number: 3
Publishing Title: 28 Years’ Experience With The Freestyle Bioprothesis: A Single Centre Retrospective Study On Overall Results And Sex Difference
Author Block:
Patrick T. Timmermans, Alex Cotovanu, Adriaan Schneider, Nina Aijmone, Mark Hazekamp, Jerry Braun, Robert Klautz, Jesper Hjortnaes
LUMC, Leiden, Netherlands
Abstract Body:
Objective: This study describes the long-term and reoperation free survival (RFS) in a large cohort of patients that underwent aortic root replacement with the Freestyle Stentless Bioprothesis, focusing on differences in outcomes between male and female patients.
Methods: Data were collected from 775 unselected adult that underwent implantation of the Freestyle Bioprothesis at the Leiden University Medical Centre between 1993 and 2022 (80% since 2010). Perioperative and follow up data were collected retrospectively. Survival status was sourced from national registries, while reoperation status was retrieved from hospital medical records. Follow-up was 100% complete (median follow-up: 7 years), with 234 patients exceeding 10 years. A competing risk analysis was performed to evaluate the mid- and long-term outcomes of the whole cohort and a Kaplan Meier analysis to determine sex differences.
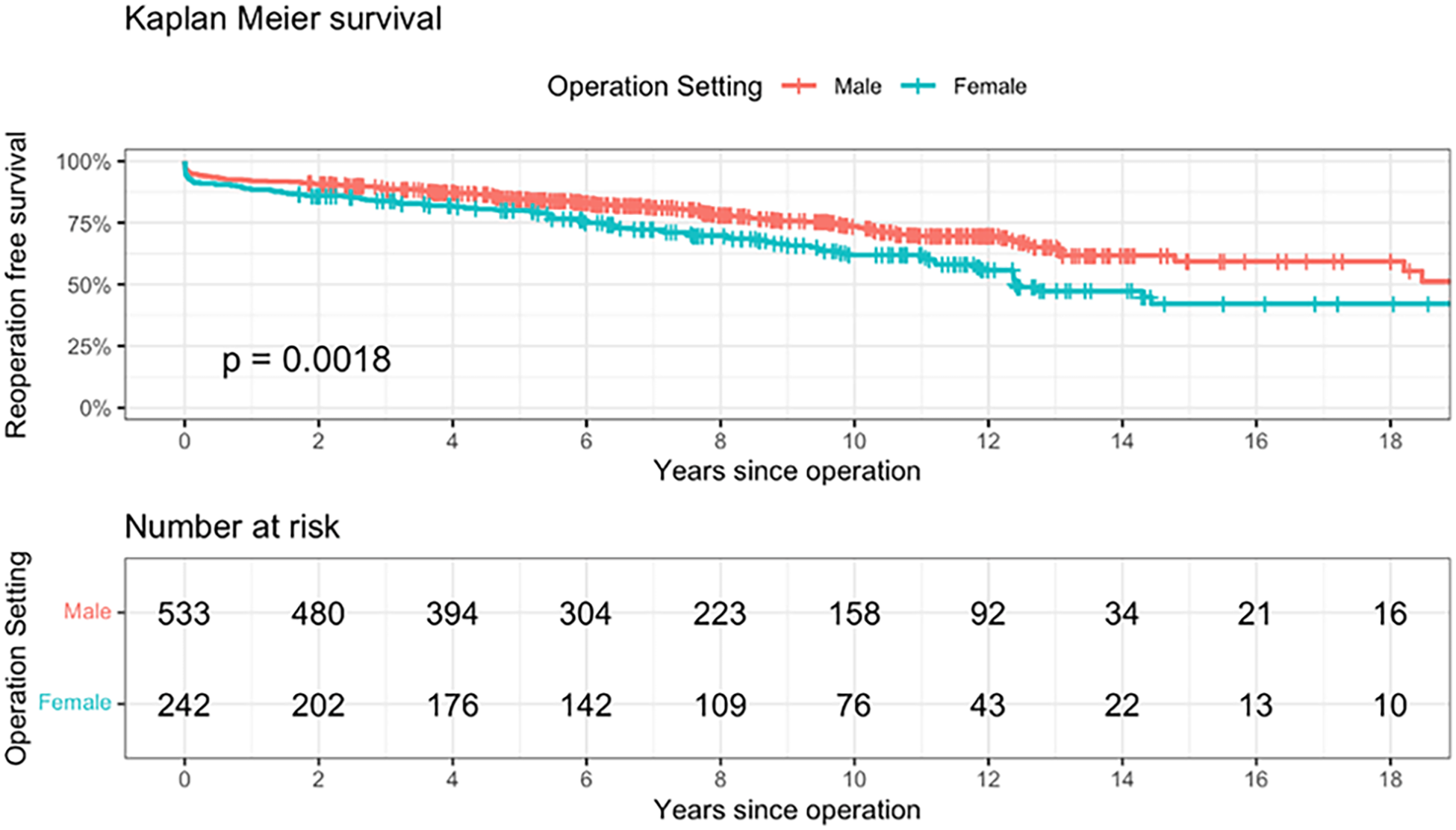
Results: Median age at operation was 62 (IQR 56, 71) years with no significant difference between sex. Females presented more often with type A aortic dissection compared to males, (17.2% vs 11.8%, respectively) but less often with valve stenosis (20.3% vs 25.1%, respectively). Males more frequently had a bicuspid aortic valve compared to females (39.4% vs 22.9%). Early mortality was slightly higher in females, 7,4% vs. 4.9 (p=0.21). RFS was consistently lower in the female population compared to the male (p< 0.001). The 1-, 5- 10- and 15-year RFS free was, respectively, 92% vs. 88%, 83% vs 77%, 67% vs. 56% and 46% vs. 30%.
Conclusions: Female patients had significantly worse outcomes after root replacement with the Freestyle Stentless Bioprosthesis with decreased long-term survival and increased reoperation rates.
Control Number: 24-A-39-HVS
Presentation Number: 4
Publishing Title: 15 Years Of Experience With Sutureless AVR: Long-term Outcome In 1135 Patients
Author Block:
Marie Lamberigts1, Bert Sarrazin1, Delphine Szecel2, Filip Rega2, Christophe Dubois2, Peter Verbrugghe2, Bart Meuris2
1KU Leuven, Leuven, Belgium, 2UZ Leuven, Leuven, Belgium
Abstract Body:
Objective: The aim of this study was to analyze the long-term 15 years of outcome of sutureless valves at our center.
Methods: In this monocentric, retrospective study, all patients that received a sutureless valve between 2007 and June 2022 at our center were included (N = 1135). The inclusion criteria was any sutureless AVR, regardless of combined procedures (CABG and/or multiple valves). Follow-up data was included until 31-6-2022. A competing risk analysis using cumulative incidences was used for the long-term endpoints. Statistical analysis was performed using SPSS version 27 (IBM Corp) and RStudio 2021.09.0+351 for Windows (RStudio Team).
Results: A total of 1135 patients received a sutureless valve, with a mean age of 78 ± 7 years and 50.2% male. The median EuroSCORE II was 4.1 (interquartile range: 2.4-7.2%). 44.8% of procedures were single AVR, 26.9% were AVR with CABG, 28.4% were multiple valve procedures (with/without CABG) or other concomitant procedures.In-hospital mortality was 3.4% (n = 39), postoperative complications include 4.2% reoperation for bleeding, a 1.7% stroke-rate, 1.3% need for new dialysis and 6.3% pacemaker implantation at 30 days since the sizing shift in 2017. Survival at 5 years was 71.1% and 25.2% at 10 years. Long term valve-related events included endocarditis and severe SVD, with an incidence rate of 0.51% for endocarditis and 0.77% for severe SVD. A total of 14 patients needed a reoperation for endocarditis and 4 patients were treated with a TAVR valve-in-valve for severe SVD.
Conclusions: Sutureless AVR can be used in various settings, as it is both very suitable for MICS single AVR and as an option to limit procedure time during more difficult combined procedures. Our study shows highly favorable early outcome and long-term outcome shows low rates of endocarditis, severe SVD and reinterventions.
Control Number: 24-A-110-HVS
Presentation Number: 5
Publishing Title: In-hospital And Long-term Outcomes Of Balloon Expandable Versus Self Expanding Bioprotheses In Patients Undergoing Valve-in-valve Transcatheter Aortic Valve Replacement
Author Block:
Mohiuddin Cheema, Eduardo Perez, Raymond Mckay, Nicole Hoover, Jawad Haider
Hartford Hospital, Hartford, CT, USA
Abstract Body:
Objective: Valve-in-Valve (VIV) transcatheter aortic valve replacement (TAVR) for failed surgical valves has been documented to be a safe and efficacious alternative to redo surgical aortic valve replacement. We sought to compare the use of balloon-expandable(BE) versus self-expanding(SE) TAVR valves in this patient subset.
Methods: From a total cohort of 162 VIV TAVR procedures performed since 2012, we compared in-hospital and intermediate outcomes in 44 patients treated with BE valves (Sapien (n=9), Sapien XT (n=3), Sapien 3/Ultra (n=32)) with 118 patients treated with SE valves (Corevalve (n=4), Evolut R (n=54), Evolut PRO (n=14), Evolut PRO+ (n=46))
Results: BE and SE VIV cohorts were well matched for age, gender, race and STS risk Score (13.9 ± 9.5% vs 12.01 ± 9.0%, p=0.146). BE patients had more diabetes (50% vs 26%, p =004) and less pre-TAVR atrial fibrillation (34% vs 43%, p =0.028), but the two cohorts were well matched for cardiac risk factors and comorbidities. BE and SE patients did not differ with respect to pre-procedure echocardiographic findings (LV ejection fraction, mean aortic gradient, degree of aortic insufficiency), although the BE cohort has a higher pre-TAVR AVA (0.9±0.4 vs 0.7±0.3 cm2, p=0.022). BE patients required more non-femoral alternative access (20% vs 8%, p=0.008) and required more general anesthesia (70% vs 44%, p=0.014).
In-hospital outcomes are presented below. Kaplan-Meier survival curves following hospital discharge for the two cohorts demonstrated no significant difference in all-cause mortality (BE 31.8% vs SE 21.9%, p=0.20) with an overall mean (95% CI) survival time of 78.4 months (68.0-88.8), (p=0.786).
Conclusions: In comparison to SE VIV, BE VIV was associated with higher post-TAVR mean aortic valve gradients, but no differences in effective orifice area, aortic insufficiency and in-hospital complications including coronary obstruction and permanent pacemaker use. BE and SE cohorts had similar survival rates on intermediate follow-up.
Control Number: 24-A-24-HVS
Presentation Number: 6
Publishing Title: Clinical Implication Of ‘constrictive Physiology' In The Postoperative Echocardiography After Heart Valve Surgery
Author Block:
Hwang chan-sop, Lee Soojin, Lee Juhyun, Joo Seohee, Park YouKyeong, Kim Kang Min, Jung Joon Chul, Chang Hyoung Woo, Lee Jae Hang, Kim Dong Jung, Kim Jun Sung, Cheong Lim, Park Kay-Hyun
Seoul National University Bundang Hospital, Seongnam-si, Gyeonggi-do, Republic of Korea, Korea, Republic of Korea
Abstract Body:
Objective: Recently, there has been an increased description of constrictive physiology (CP) in postoperative echocardiography following heart valve surgery. In this study, we sought to identify which patients tend to exhibit signs of CP after valve surgery and to determine the clinical significance of CP in relation to surgical outcomes.
Methods: We conducted a retrospective study involving 443 patients who underwent heart valve surgery at a single center between January 2020 and November 2022. Of these, 386 patients were included in the analysis. Patients were categorized into two groups based on the presence of CP in postoperative echocardiography: CP group (n=54) and non-CP group (n=332). The Cox-proportional hazard model was used to calculate hazard ratios of the variables, and survival analyses were conducted for overall survival and major adverse cardiovascular and cerebrovascular events (MACCE) free survival.
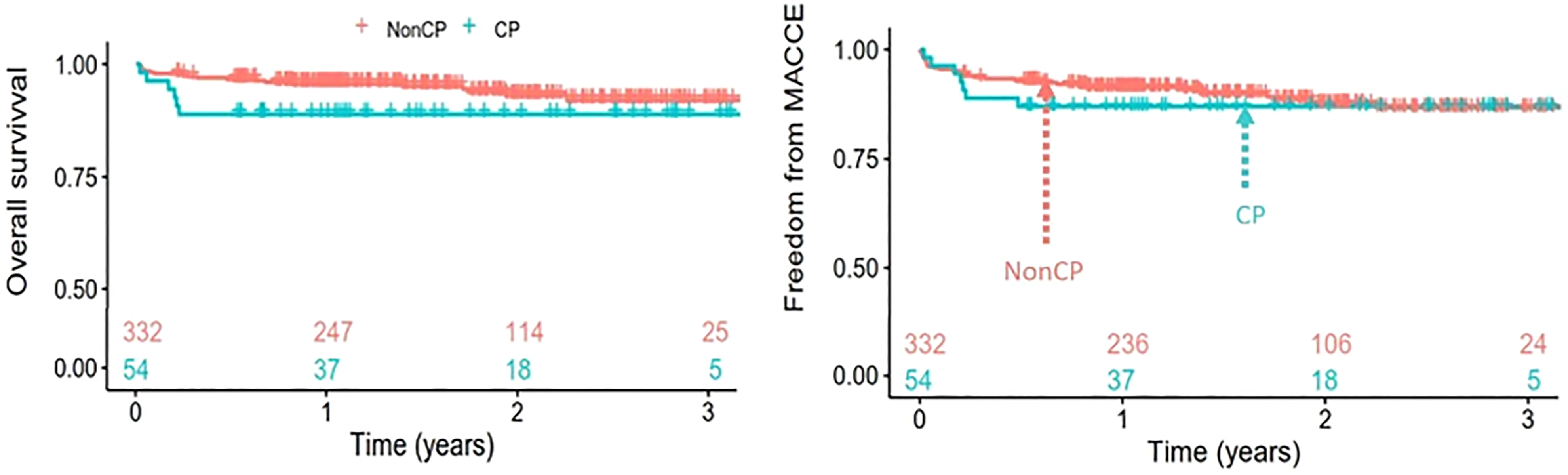
Results: Preoperative characteristics between the two groups did not differ significantly. In the CP group, both the amount of blood products transfused and chest tube drainage within the first 24 postoperative hours were significantly greater (P=0.031 and P<0.01, respectively). The incidences of re-exploration due to bleeding and respiratory complications were also significantly higher in the CP group (P=0.034 and P=0.047, respectively). However there were no significant differences between the groups in terms of early mortality (P=0.366) or MACCE (P=0.861). Survival analyses revealed that midterm overall and MACCE-free survival rates were comparable between two groups (P=0.117 and P=0.581, respectively, "figure 1"). In multivariable survival analyses using Cox regression, CP was not associated with an increased risk of overall mortality or MACCE; hazard ratio [HR] 1.576, 95% confidence interval [CI] 0.54-4.57, P=0.41, And HR 0.702, 95% CI 0.27-1.82, P=0.467 respectively.
Conclusions: The presence of ‘constrictive physiology’ in postoperative echocardiography does not appear to influence postoperative outcomes.
Control Number: 24-A-45-HVS
Presentation Number: 7
Publishing Title: The Ross Procedure - Long Term Results Of Minimal Invasive Vs. Conventional Access
Author Block:
Marc Albert, Adrian Ursulescu, Nora Goebel, Ulrich F. Franke
Robert-Bosch Hospital, Stuttgart, Germany
Abstract Body:
Objective: The Ross-procedure has excellent long-term results published lately. As it is a complex procedure, surgeons prefer a complete sternotomy. The minimal invasive Ross procedure via partial upper hemisternotomy is feasible and safe but only described by one center and two publications. So, the question remains whether the minimally invasive Ross procedure has a similar long-term outcome as a conventional sternotomy.
Methods: In our department, 218 Patients (83 patients median sternotomy, 135 minimal invasive upper hemisternotomy) received a Ross procedure between 2007 and 2023. For this retrospective, single-center study, we did an annual in-hospital follow-up, including transthoracic echocardiography and a questionnaire about the quality of life (SF-36).
Results: The two groups had similar demographic and pre-OP data in most items. The minimally invasive access had longer cross-clamp and bypass time while having similar skin-to-skin time but showed shorter ventilation time, ICU, and in-hospital length of stay. The mean follow-up period was 71 ± 30 months. In that period, 2 sternotomy patients died (p=0.445). There were 8 re-do procedures after sternotomy and 6 after minimal invasive hemisternotomy in the follow-up period (p=0.410). 2 patients of the sternotomy and none of the hemisternotomy group needed an aortic and pulmonary valve procedure. 4 patients of sternotomy and 5 patients of the hemisternotomy group required an isolated aortic valve procedure (p=0.690), and 4 vs. 1 patient required a pulmonary valve procedure (p=0.390), respectively.
Conclusions: Minimally invasive access is feasible and safe. It may have longer cross-clamp and bypass time while having similar skin-to-skin time. As a sign of better mobilization and faster recovery, those patients showed a shorter ventilation time, ICU, and in-hospital length of stay. Both groups showed equal long-term results regarding the need for repeated aortic or pulmonary valve procedures and mortality.
Control Number: 24-A-27-HVS
Presentation Number: 8
Publishing Title: Long-term Outcomes Following Aortic Valve Replacement: A Comparison Of Bioprosthetic And Mechanical Valves In Patients Aged 50-70
Author Block:
Abeline R. Watkins, Ryaan EL-Andari, Nicholas M. Fialka, Jimmy J. Kang, Yongzhe Hong, Sabin J. Bozso, Devilliers Jonker, Michael Moon, Jayan Nagendran, Jeevan Nagendran
University of Alberta, Edmonton, AB, Canada
Abstract Body:
Objective: Aortic valve disease is the leading cause of patient morbidity despite accounting for only 33% of valvular heart disease cases. Current valve prosthesis options used in aortic valve replacement (AVR)require patients to choose between durability and functionality. For patients between 50-70 years old, these risks are equivalent, leading the decision of valve prosthesis type on patient preference. To investigate whether long-term differences exist between these options, we present the results of a 15-year retrospective comparison between patients aged 50-70 years old who received mechanical and bioprosthetic AVR.
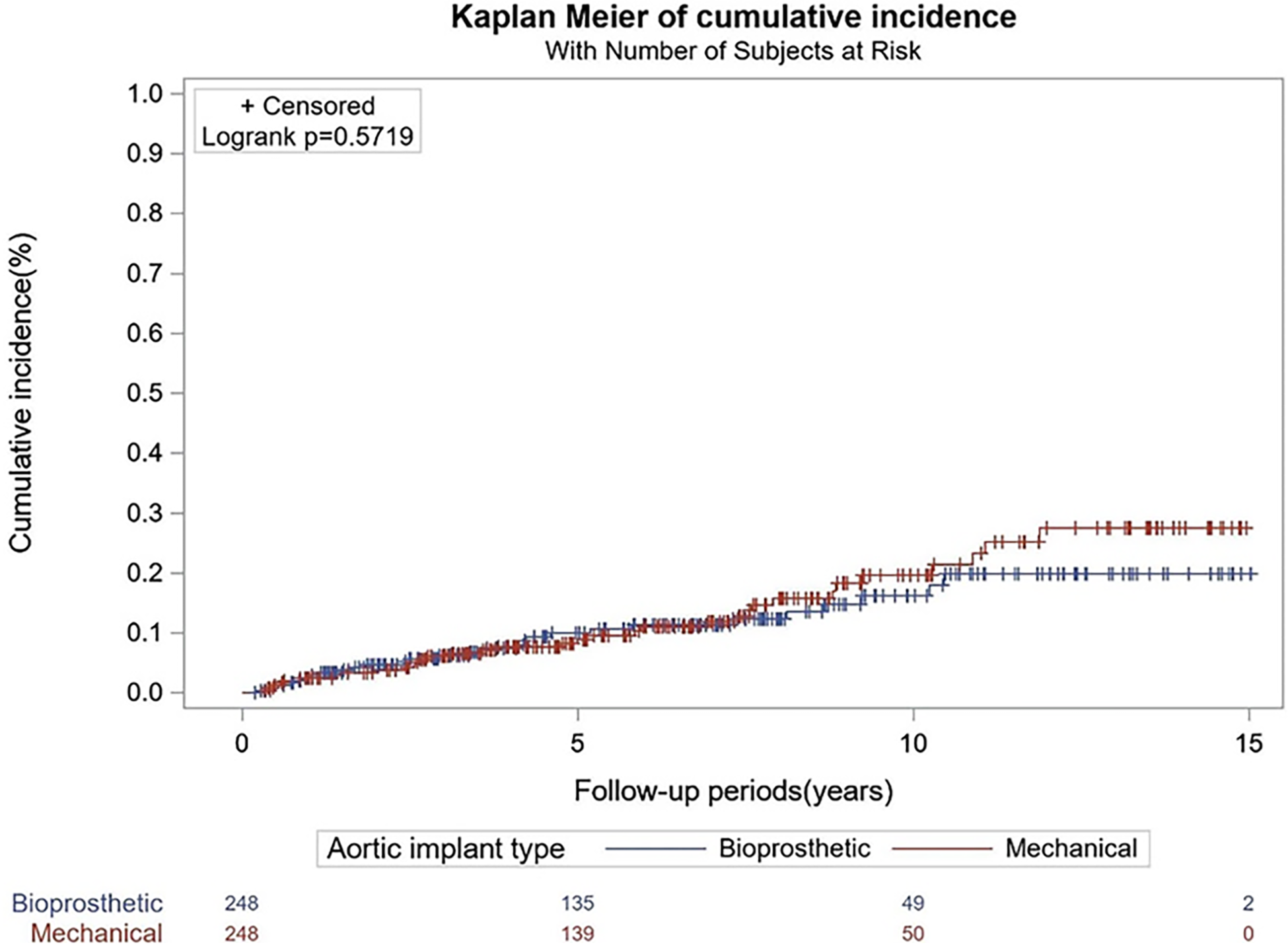
Methods: We analyzed all patients receiving surgical AVR at our institution between 2004 and 2018. 496 propensity-matched patients were analyzed, comparing those who received mechanical valves to those who received bioprosthetic valves. Outcomes included short- and long-term mortality, incidences of myocardial infarction, stroke, infection, and bleeding, and rates of reoperation.
Results: There were no deaths at 30 days postoperatively and in-hospital complication rates did not differ between groups (p>0.05). Short-term, long-term, and all-cause mortality over the entire 15-year follow-up period did not significantly differ between groups (p=0.5719). Reoperation rates at 5, 10, and 15 years did not significantly differ between bioprosthetic and mechanical valves (p=1.0, p=0.168, p=0.106).
Conclusions: Patients receiving AVR between the ages of 50 and 70 years old have similar post-operative and long-term outcomes irrespective of whether they received bioprosthetic or mechanical valves. With low rates of reoperation comparable to mechanical valves in patients aged 50-70, bioprosthetic valves become a reasonable option for patients in this age group. As bioprosthetic valves are becoming more durable and with the possibility of reintervention being performed percutaneously, these results help support its use in younger patients that do not want to risk lifelong anticoagulation.
Control Number: 24-A-18-HVS
Presentation Number: 9
Publishing Title: Postoperative Thrombocytopenia After Aortic Valve Replacement With Sutureless Valve
Author Block:
Mil Hoo Kim, Juhyun Lee, Soojin Lee, Seohee Joo, You Kyeong Park, Kang Min Kim, Joon Chul Jung, Hyoung Woo Chang, Jae Hang Lee, Dong Joong Kim, Jun Sung Kim, Kay-Hyun Park, Cheong Lim
Seoul National University Bundang Hospital, Bundang-gu, Seongnam-si, Gyeonggi-do, Korea, Republic of Korea
Abstract Body:
Objective: Sutureless valves are widely used in aortic valve replacement surgery, with the Perceval valve and Intuity valve being prominent among them. However, there is research suggesting a tendency for postoperative thrombocytopenia with the Perceval valve. To confirm this and compare it with the Intuity valve to assess the significant occurrence of thrombocytopenia and its adverse impact on patients, as well as investigate its association with transfusion volume.
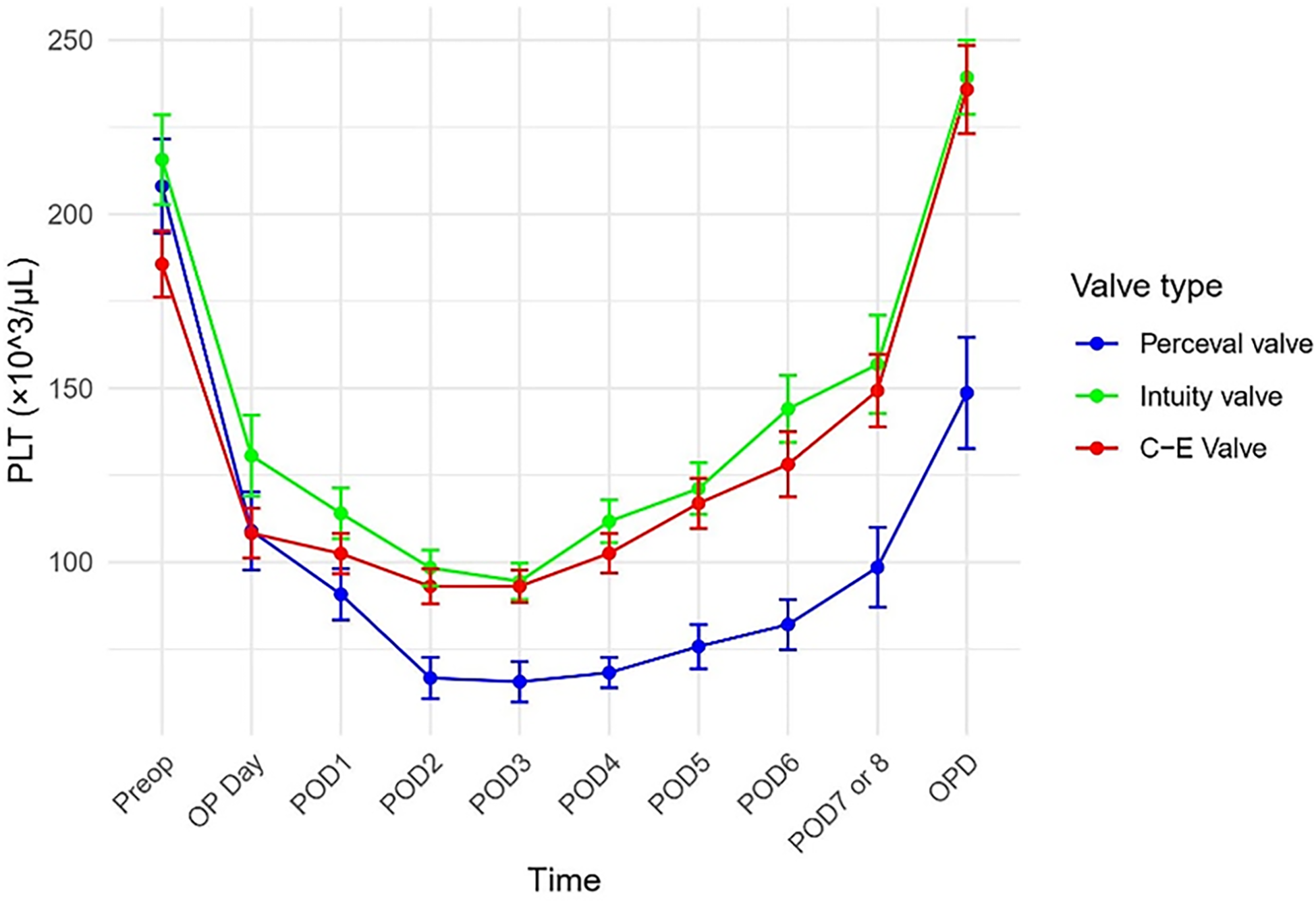
Methods: Among 595 patients who underwent aortic valve replacement from June 2016 to March 2023, 53 patients received sutureless valve aortic valve replacement; 23 patients with Perceval valve, and 30 patients with Intuity valve. Platelet counts were observed during the hospitalization period and were also tracked in outpatient visits. Platelet count changes were compared using chi-square tests, and the trend of changes was visualized including the C-E valve for comparison (see figure).
Results: Compared to the Intuity valve, the Perceval valve showed a significantly higher amount of platelet transfusion (5.48±1.64 vs. 0.60±0.44, p = 0.008). Severe thrombocytopenia (<50,000/uL) was significantly more prevalent with the Perceval valve (56.5%, n=13) compared to the Intuity valve (6.7%, n=2). When comparing the Perceval valve and Intuity valve, platelet count changes yielded significant results over time (p<0.001). There was no significant difference in early mortality or the incidence of neurological complications between the two groups.
Conclusions: The severity of postoperative thrombocytopenia was significantly different in using Perceval and Intuity valves. Perceval group showed significantly severe thrombocytopenia and significantly higher platelet transfusion volumes. However, the thrombocytopenia gradually recovered during the postoperative period in both groups. The use of the Perceval valve was associated with more severe postoperative thrombocytopenia, but the early mortality was similar in both groups.
Control Number: 24-A-96-HVS
Presentation Number: 10
Publishing Title: Calcific Aortic Valve Disease Progression Is Modulated By Vitamin K-Dependent γ-Carboxylated Growth Arrest Specific Protein 6 On The Protein Corona Of Extracellular Vesicles
Author Block:
Mandy E. Turner, Shinsuke Itoh, Joost K. Hoekstra, Mark C. Blaser, Kentaro Mikami, Cassandra L. Clift, Singh A. Singh, Masanori Aikawa, Elena Aikawa
Brigham and Women's Hospital, Boston, MA, USA
Abstract Body:
Objective: Extracellular vesicles (EVs) aggregate in the extracellular matrix of aortic valves to initiate pathological calcification. Our objective was to use proteomics of both calcified aortic valves and their associated tissue EVs to identify novel disease drivers. We identified growth arrest specific protein 6 (GAS6) as a secreted γ-carboxylated vitamin K-dependent protein that is currently undescribed in heart valves.
Methods: Whole aortic valve and tissue EV label-free proteomics, histopathology, and valvular interstitial cell (VIC) isolation was performed on specimens collected from surgical aortic valve replacements. EVs were isolated from whole valves using collagenase digestion and density gradient ultracentrifugation. Mass-spectrometry was used to validate γ-carboxylation.
Results: The calcified aortic valve proteome (N=18, 2319 proteins) and associated proteome of tissue EVs (N=9, 1943 proteins) was differentially enriched in GAS6 compared to non-diseased aortic valves (log2FC=3.8, p=1.1e-6, log2FC=1.7, p=1.7e-2, respectively). Using immunohistopathology of calcified aortic valve specimens, GAS6 co-localized with VIC signatures (vimentin+) in areas of inflammation (CD68+) and calcification. GAS6 also co-localized with acellular areas of remodelling collagen via picrosirius red staining, an area known to be associated with EV aggregation. Using primary valvular interstitial cell culture, 85% of secreted GAS6 was identified bound to the surface on the EV corona using ELISA measurements on intact EVs following ultracentrifugation (N=9, p<0.001), a phenomenon dependent on post-translational γ-carboxylation. Using vitamin K supplementation or inhibition with warfarin, we established amino acid site specific assessments of γ-carboxylation using mass spectrometry. GAS6 expression increased in VICs cultured in osteogenic media to stimulate calcification as indicated by Alizarin red staining (N=5-8, p<0.05), and knockdown of GAS6 using siRNA in VICs attenuated calcification (N=4).
Conclusions: These findings support that GAS6 is a novel protein of pathological significance in calcific aortic valve disease. Regulation of post-translational γ-carboxylation of this EV-bound protein may have implications for future disease pharmacology.
Control Number: 24-A-46-HVS
Presentation Number: 11
Publishing Title: Distinct Regulatory Mechanisms Of Bioprosthetic And Native Aortic Valve Calcification: A Proteomic Comparison
Author Block:
Rachel M. Cahalane1, Cassandra L. Clift1, Mandy E. Turner1, Mark C. Blaser1, Taku Kasai1, Amber Hendrickx2, Alesandra Campedelli1, Marie Billaud1, Filip Rega2, Laoise McNamara3, Masanori Aikawa1, Bart Meuris2, Sasha A. Singh1, Elena Aikawa1
1Brigham and Women's Hospital, Boston, MA, USA, 2KU Leuven, Leuven, Belgium, 3University of Galway, Galway, Ireland
Abstract Body:
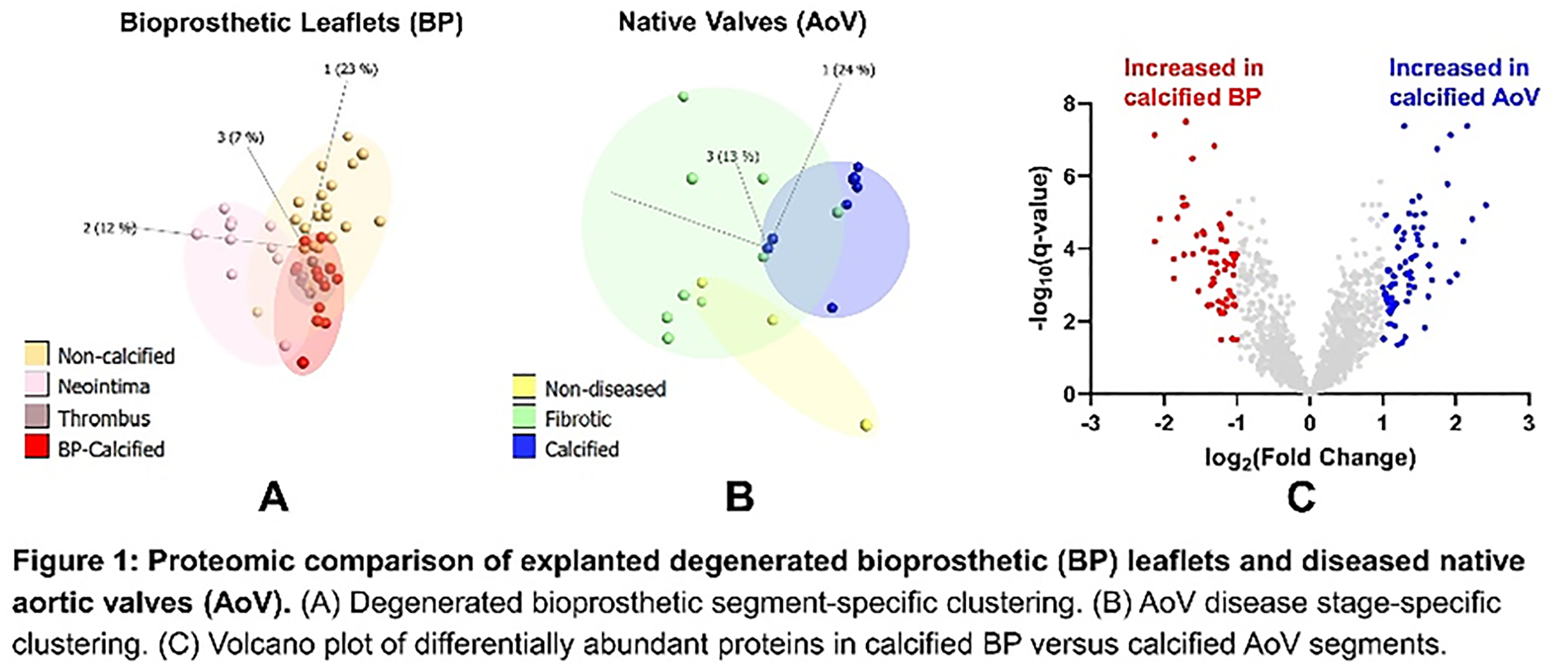
Objective: The underlying molecular mechanisms of bioprosthetic (BP) valve calcification are largely unknown. Pediatric and younger patients are at risk of accelerated degeneration, suggesting an active host contribution. The purpose of the current study was to conduct a histopathological and ultrastructural analysis of BP calcification and use proteomics to characterize shared and separate pathological processes occurring in native aortic valve (AoV) and BP calcification.
Methods: Degenerated BP leaflets (N=29) and diseased AoV leaflets (N=10) were acquired. BP leaflets were segmented into non-calcified, calcified, neointima, and thrombotic regions. AoV leaflets were segmented into non-diseased, fibrotic, and calcified regions. A cross-section was processed for both histology and transmission electron microscopy (TEM). BP and AoV segments were analyzed using mass spectrometry-enabled proteomics.
Results: Histopathology revealed calcification in both the internally degraded matrix (19/29 leaflets) and areas of neotissue formation (thrombus or pannus) of BP leaflets (6/29 leaflets). Lipid and extracellular vesicle accumulation in a disrupted BP collagen matrix was evident from ultrastructural TEM analysis. Proteomics identified 2,310 proteins across the two tissue datasets. Principle component analysis of BP and AoV tissue proteomes demonstrated BP and AoV segment-specific clustering (Fig.1A-B). Comparing the calcified segments of BP and AoV, 74 and 60 proteins were more abundant in calcified BP and calcified AoV regions, respectively (q≤0.1; logFC>1; Fig.1C). Gene Ontology searches of the differentially enriched proteins indicated impaired nitric oxide biosynthetic (GO:0045019; p<0.001) was increased in AoV calcification, and platelet activation (GO:0010572; p<0.001) was increased in BP calcification. This finding was supported by our histological observation of fibrin deposition in BP leaflets.
Conclusions: This is the first study to compare calcified BP and AoV proteomes. This data may predict if anti-calcification therapeutics that are currently being developed for AoV disease would additionally alleviate BP calcification.
Control Number: 24-A-138-HVS
Presentation Number: 12
Publishing Title: A Role For The Mineralocorticoid Receptor In Aortic Regurgitation
Author Block:
Mattie Garaikoetxea Zubillaga, Susana San Ildefonso, Alba Sádaba, Carolina Tiraplegui, Ernesto Martín-Núñez, Lara Matilla, Adela Navarro, Amaya Fernández-Celis, Alicia Gainza, Virginia Álvarez, Rafael Sádaba, Eva Jover-Garcia, Natalia López-Andrés
Navarrabiomed, Iruña, Spain
Abstract Body:
Objective: The molecular mechanisms involved in aortic regurgitation (AR) remain unclear. AR is characterized by aortic valve (AV) extracellular matrix (ECM) fibro-myxomatous abnormalities and is more prevalent in men. Aldosterone/mineralocorticoid receptor (Aldo/MR) pathway is involved in mitral valve prolapse and aortic stenosis, so we aim to investigate its participation in AR.
Methods: High-throughput full-length RNA sequencing was performed in primary valve interstitial cells (VICs) of 6 patients with AR (n=3/sex). Complementarily, single-cell RNA sequencing was analysed. Cytokine arrays were conducted in VIC-derived secretomes (n=4/sex) and AVs from AR patients (n=42/sex). Results were validated by qPCR, ELISA or western blotting using independent donors’ VICs and in 150 AR patients’ AVs.
Results: Pro-inflammatory and pro-fibrotic pathways were enriched in men (IL-1B, IL-6, TGFB1) while women exhibited increased transcripts of genes related with lipid metabolism (based on KEGG pathways and Gene Ontology). Importantly, NR3C2/MR as well as ACTA2 (activated VIC) and ECM remodelling targets (SDC4 and ADAMTS2/8/14) were higher in male VICs. 4-day spironolactone treatment decreased IL-6 and PAI-1 secretion in male VICs compared to controls. In a cohort of 150 AR patients (72.7 % men), NR3C2 was increased in men and positively correlated with ECM remodelling (ACTA2, lumican and ADAMTS2) and inflammatory markers (IL8 and PAI-1). 7 male patients receiving a MR antagonist (MRA) were compared with 33 patients with similar left ventricular dysfunction who were not receiving MRAs. AVs of MRA-treated patients showed lower VIC activation (ACTA2), ECM remodelling (collagen type I, aggrecan, syndecan-1 and ADAMTS2/8) and inflammatory markers (IL-6 and PAI-1).
Conclusions: MR is overexpressed in VICs and AVs from AR men. Interestingly, MR is associated with ECM remodelling and inflammation preferably in men. MRA treatment may be a promising option to reduce AV pathologic features in AR patients.
Control Number: 24-A-29-HVS
Presentation Number: 13
Publishing Title: Integrative Molecular Pathogenesis Of Human Adult Congenital Heart Valve Disease
Author Block:
Mark C. Blaser1, Daniel Reichart2, Abhijeet Sonawane1, Florian Schlotter1, Daniel DeLaughter2, Livia S. Passos1, Arda Halu1, Hideyuki Higashi1, Mandy E. Turner1, Tan Pham1, Wunan Zhou1, Ron Blankstein1, Marcelo F. DiCarli1, Maria C. Nunes3, Marie Billaud1, Ashraf A. Sabe1, Simon C. Robson4, Simon C. Body5, Jochen D. Muehlschlegel6, Masanori Aikawa1, Sasha A. Singh1, Jonathan G. Seidman2, Christine E. Seidman2, Elena Aikawa1
1Brigham and Women's Hospital, Boston, MA, USA, 2Harvard Medical School, Boston, MA, USA, 3Federal University of Minas Gerais, Minas Gerais, Brazil, 4Beth Israel Deaconess Medical Center, Boston, MA, USA, 5Boston University School of Medicine, Boston, MA, USA, 6Johns Hopkins University School of Medicine, Baltimore, MD, USA
Abstract Body:
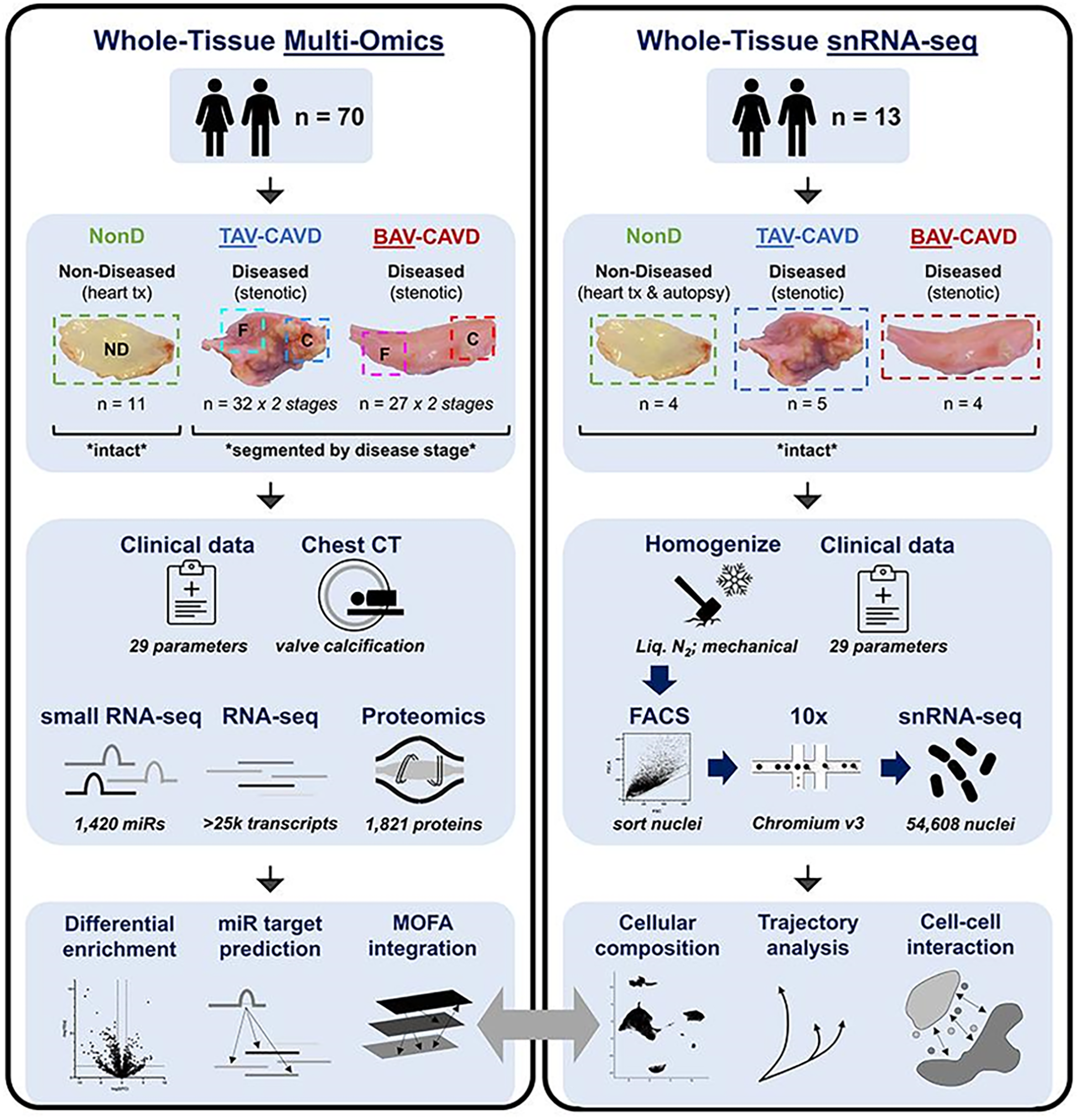
Objective: Bicuspid aortic valve (BAV) is the most common cause of adult congenital heart disease. These patients comprise <2% of the population but represent ∼50% of valve replacement surgeries and the pathogenic mechanisms underlying this disproportionate incidence of calcific aortic valve disease (CAVD) are unknown. We aimed to identify molecular contributors to accelerated disease in BAV-CAVD.
Methods: Bulk multi-omics (miRNA-seq, RNA-seq, proteomics) was performed on 70 human aortic valves (11 non-diseased; fibrotic and calcific portions of 32 tricuspid aortic valves (TAVs) and 27 BAVs with CAVD). Single nuclei RNA-seq (snRNA-seq) was completed on 54,608 nuclei from 13 additional human valves (4 non-diseased; 5 TAVs and 4 BAVs with CAVD).
Results: Calcification did not differ between diseased TAVs and BAVs (p=0.77), but BAV mineralization was accelerated by 11.5+/-1.7 years vs. TAVs (p<0.001). Latent factor-based covariate-corrected multi-omics analyses (q<0.05), CT-derived valve calcification, and 29 clinical parameters uncovered extensive involvement of adaptive immune responses where T cell/B cell inflammatory activation associated with autoimmune signals was enhanced in the early stages of BAV disease. Integrated multi-omics also revealed elevated platelet activation potentially as a result of lifelong exposure to the high-shear BAV microenvironment, and implicated altered SLIT-ROBO signaling in BAV-CAVD progression. snRNA-seq identified 5 major cell types (27 states) in human aortic valves: valvular interstitial cells (VICs; 65% of cells; 7 states), endothelial cells (10%; 4 states), macrophages (13%; 7 states), T cells (8%; 5 states), and B cells (3%; 4 states). CAVD drove differentiation of VICs along distinct myofibrogenic (ACTA2/CARMN/MYH11-high) vs. osteogenic (RUNX2/CDH11/POSTN-high) lineages, induction of endothelial-to-mesenchymal transition in valve endothelium, and significant accumulation of macrophage and T-cell states (p<0.05) in BAV-CAVD.
Conclusions: Aberrant adaptive immune responses are critical drivers of BAV-CAVD, and our findings delineate a novel strategy for discovery of morphology-specific therapeutics.
Control Number: 24-A-170-HVS
Presentation Number: 14
Publishing Title: Increased TGFbeta1 Activity In Valve Interstitial Cells Causes Calcific Aortic Valve Disease
Author Block:
Mohamad Azhar
University of South Carolina, Columbia, SC, USA
Abstract Body:
Objective: Calcific aortic valve disease (CAVD) is the third leading cause of heart disease. Increased transforming growth factor beta1 (TGFB1) levels is found in surgically collected aortic valve (AV) specimens from CAVD patients. It remains unclear if there is a direct cause-and-effect relationship between increased TGFβ1 levels and development and/or progression of CAVD.
Methods: We generated Tgfb1Tg;PostnCre (i.e., Tgfb1OE) mice with an overexpression of the constitutively active form of TGFβ1 in valve interstitial cells (VIC). Echocardiography and microcomputed tomography (micro-CT) imaging approaches were used to monitor longitudinal progression of AV function and calcification in live male and female mice. Histology, immunohistochemistry, qPCR, biochemical analysis, immunoprecipitation, and western blot analyses were used to determine cellular and molecular mechanisms involved in development and pathogenesis of CAVD.
Results: Adult VIC-specific Tgfb1 transgenic (Tgfb1OE) male mice had higher TGFβ1 and TGFβ signaling in AV tissue compared to adult female mice. While both young male and female Tgfb1OE mice developed CAVD, only male Tgfb1OE mice developed calcific AV stenosis (AS) after 8 months of age. Postnatal fusion of left and right AV coronary cusps, the raphe type, significantly contributed to calcific AS in male Tgfb1OE mice. Heterozygous conditional genetic deletion of Tgfb1 in VIC rescued the calcific AS in male Tgfb1OE mice. TGFβ1 hyperactivation resulted in increased VIC activation and interaction of activated SMAD3 with RUNX2 in the AV tissue. Biochemical analyses of AV tissue indicate that TGFβ1 downregulated NAD+-dependent poly-ADP(ribose)polymerase (PARP1)- and tyrosyl-tRNA synthetase (TyrRS)-regulated ADP-ribosylation of RUNX2, resulting in increased RUNX2-dependent osteoblast differentiation of VIC. The NAD+-boosting natural compounds (nicotinamide, nicotinamide riboside) significantly restored TGFβ signaling and reduced RUNX2 activation, and blocked AV calcification.
Conclusions: TGFβ1 hyperactivation in valve interstitial cells causes CAVD, but in older male mice sustained TGFβ1 activation promotes calcific AS. Targeted therapy to preserve TGFβ1 signaling can prevent CAVD.
Control Number: 24-A-121-HVS
Presentation Number: 15
Publishing Title: Long-term Endothelin-1-mediated Contractility Of Aortic Valve Interstitial Cells Is Held In Check By ROCK1/2 And GRK2/3
Author Block:
Toni M. West1, Daniel P. Howsmon2, Robin Tuscher1, Mia G. Zheng1, Olivia Snapper1, Sanjana Chemuturi1, Jodie H. Pham1, Michael S. Sacks1
1University of Texas, Austin, TX, USA, 2Tulane University, New Orleans, LA, USA
Abstract Body:
Objective: Aortic valve stenosis is a leading cause of regurgitation and can lead to death if not replaced or repaired. Currently there is no pharmacological therapy for this disease. A hallmark of aortic valve stenosis is activation of the valve interstitial cells (VICs) where the VICs produce robust actin/myosin cytoskeletons. We have recently reported that VICs from stenotic raphe regions of bicuspid aortic valves have a higher basal contractility than those of the surrounding healthier tissue. To better understand the biochemistry to aid in identifying druggable targets, we gathered data and produced models which tease apart the contributions of polymerized actin mass vs. myosin activity when cells are made to fully contract with endothelin-1.
Methods: Inhibitors that target actin polymerization and myosin phosphorylation were chosen with a goal of separating the effects of increased actin mass from that of myosin activity. Takeda compound 101 was implemented for inhibiting GRK2/3, hydroxyfasudil for ROCK1/2, and Y16 for RhoA-GEFs. Time series studies of 50 nM endothelin-1 were completed under inhibition, with ultracentrifugation followed by Western Blot being performed to assess F/G-actin ratios and quantitative ICC being performed to measure F-actin, myosin phosphorylation, and cell morphometrics. 3D traction force microscopy was performed to measure contractility dynamics.
Results: We first produced a mechanistic model parameterized to the data that is based on mass action and Michaelis-Menten kinetics which then allowed us to further develop our previously published stress fiber material model to include a delineation between the effects of actin polymerization to that of myosin activity.
Conclusions: While short-term contraction of VICs is highly powered by increases in myosin phosphorylation, long-term contraction is mostly powered by an increase in polymerized actin mass which is highly regulated by ROCK1/2 and GRK2/3 activity. Therefore, future research into ROCK1/2 and GRK2/3 pathways is promising for finding druggable targets.
Control Number: 24-A-111-HVS
Presentation Number: 16
Publishing Title: Multiomic Analysis Reveals Altered Biochemical Profile In Human Thoracic Aneurysms With Associated Valve Dysfunction
Author Block:
Malak Elbatarny, Uros Kuzmanov, Daniella Eliathamby, Jennifer C. Chung, Craig Simmons, Anthony Gramolini, Maral Ouzounian, on behalf of MultiTAAD investigators
University of Toronto, Toronto, ON, Canada
Abstract Body:
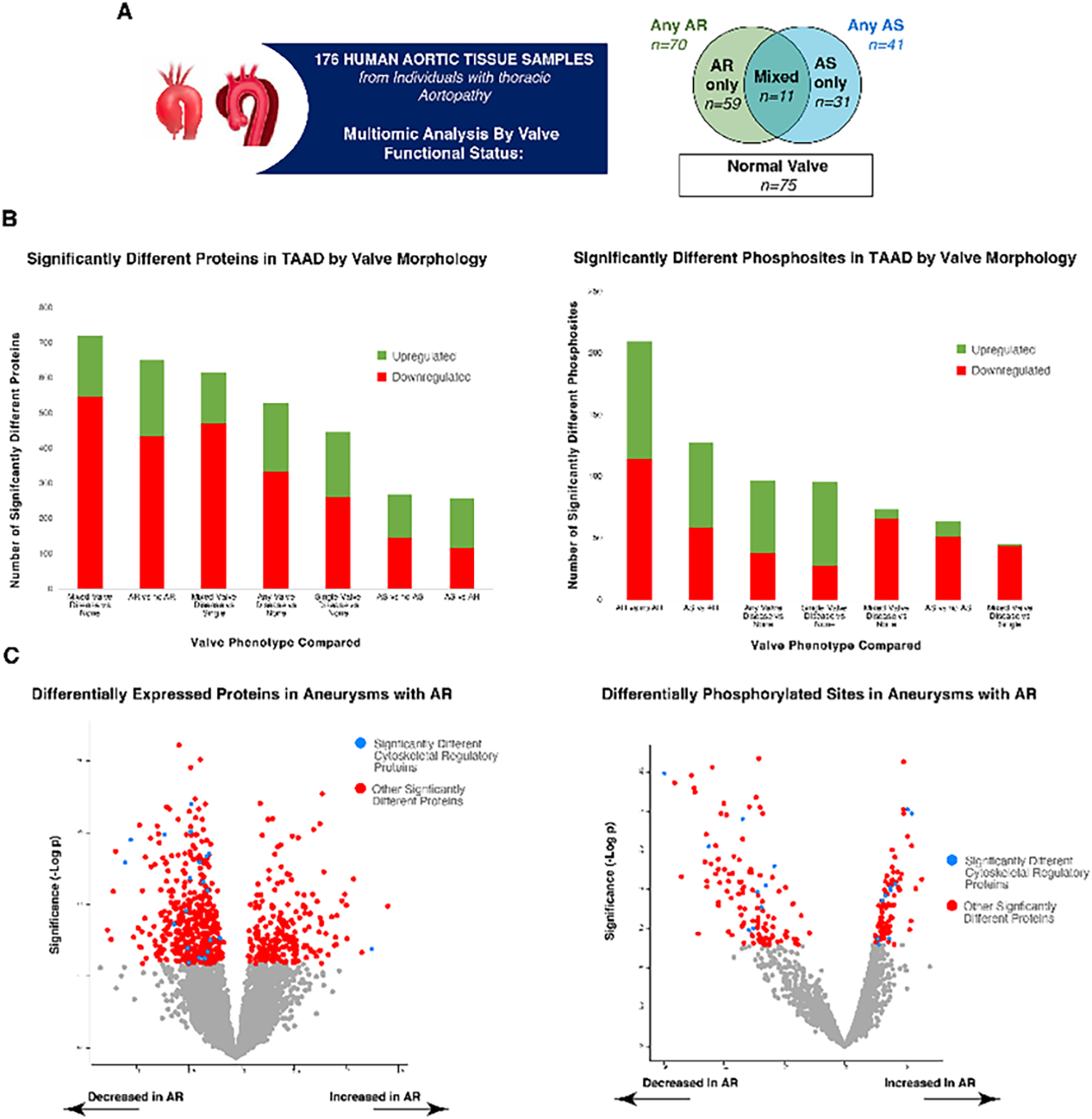
Objective: Aortic valve pathology (stenosis, AS or regurgitation, AR) often accompanies thoracic aortopathy. We compared biochemical profiles of diseased aortas associated with AS, AR, mixed (AS+AR), and normal valves to determine whether valve disease-associated aortopathy is phenotypically distinct. Methods: 176 human aortic samples were collected prospectively from aortopathy individuals with various aortic valve phenotypes (Figure 1A). All samples were analyzed using a novel deep-coverage protocol for mass spectrometry proteomics (data independent acquisition) and double enrichment technique to identify phosphorylation sites in detected proteins. Proteomic and phosphoproteomic data were directly compared by valve morphology (p<0.05 considered significant) to determine impact of valve function on aortopathy biochemical profile.
Results: Samples included N=123 males (74%) and mean age was 58±16. Among samples derived from individuals with concomitant valve disease, N=70 were AR-associated, N=41 were AS-associated, and N=11 were AS+AR. Considering the entire cohort, we quantified 6094 proteins and 2125 phosphorylation sites. At the proteomic level, when AS+AR was compared to normal valve-associated aortopathy, 721 proteins were differentially expressed (174 up in AS+AR, 547 down in AS+AR Figure 1B). Additionally, AR-associated aortopathy was associated with substantial phenotypic differences in both proteomic (total proteins 651; up in AR: 216; down in AR: 435) and phosphoproteomic data sets (total sites 210; hyperphosphorylated in AR: 96; hypophosphorylated in AR: 114 Figure 1B). Examining proteomic profiles in more detail, cytoskeletal proteins were predominantly decreased in AR-associated aortopathy while both hyper- and hypo-phosphorylation of cytoskeletal proteins was observed in AR (Figure 1C).
Conclusions: We performed the first multiproteomic analysis of aortopathy by aortic valve function on a large cohort of human samples using a novel protocol. Valve dysfunction, especially AR, is associated with altered aortic tissue biochemistry which suggests differences in mechanism and progression of aortopathy.
Control Number: 24-A-34-HVS
Presentation Number: 17
Publishing Title: Wnt Signaling Inhibition Prevents Disease Progression In Congenital Myxomatous Valve Disease
Author Block:
Na Xu, Christina M. Alfieri, Yang Yu, Minzhe Guo, Katherine E. Yutzey
Cincinnati Children's Hospital Medical Center, Cincinnati, OH, USA
Abstract Body:
Objective: Myxomatous valve disease (MVD) is the most common cause of mitral regurgitation, which can lead to heart failure. MVD in a mouse model of Marfan syndrome (MFS) includes valve leaflet thickening and increased immune cell infiltration. However, the underlying mechanisms by which disease is initiated and progresses remain undefined.
Methods: Wnt signaling activity was detected using TCF/Lef-lacZ reporter in MFS mice with Fibrillin 1 variant Fbn1C1039G/+. Single-cell RNA sequencing was performed from mitral valves of WT and Fbn1C1039G/+ mice at 1 month-of-age. Inhibition of Wnt signaling was achieved by conditional induction of Wnt inhibitor Dkk1 in valve interstitial cells of Fbn1C1039G/+; Periostin-Cre; tetO-Dkk1; R26-rtTA mice. Dietary doxycycline was administered for 1 month beginning with MVD initiation (1-month-old) or MVD progression (2-month-old). Histological evaluation and immunofluorescence for immune cells were performed.
Results: Wnt signaling pathway gene expression is activated early in mitral valve disease progression, prior to immune cell infiltration, in Fbn1C1039G/+ mice. Single cell transcriptomics revealed similar mitral valve cell heterogeneity and cell proportion between WT and Fbn1C1039G/+ mice at 1 month-of-age. Wnt ligands and responsive genes were predominantly expressed in valve interstitial cells and valve endothelial cells of Fbn1C1039G/+ mice. Inhibition of Wnt signaling by Dkk1 induction at 1 month-of-age prevented the initiation of MVD as indicated by reduced valve leaflet thickness with decreased infiltrating macrophages in Fbn1C1039G/+ mice. However, later Wnt inhibition starting at 2 months when inflammation and myxomatous changes are occurring did not prevent the progression of MVD.
Conclusions: Wnt signaling is involved in the initiation of mitral valve abnormalities and inflammation, but is not responsible for valve disease progression once it has been initiated. Thus, Wnt signaling inhibition prevents initiation of congenital MVD, which provides a promising therapeutic target for the early treatment of congenital MVD.
Control Number: 24-A-50-HVS
Presentation Number: 18
Publishing Title: Male-female Differences In Distinct Aortic Growth Phenotypes In The Thoracic Aortic Aneurysm
Author Block:
Adine Rosalie de Keijzer, Bsc1, Maximiliaan L. Notenboom, Bsc1, Kevin M. Veen, MD, PhD1, Arjen Gökalp, MD1, Ad J.J.C. Bogers, MD, PhD1, Robin H. Heijmen, MD, PhD2, Roland R.J. van Kimmenade, MD, PhD2, Guillaume S.C. Geuzebroek, MD, PhD2, M. Mostafa Mokhles, MD, PhD3, Jolanda Kluin, MD, PhD1, Jos A. Bekkers, MD, PhD1, Jolien W. Roos-Hesselink, MD, PhD1, Johanna J.M. Takkenberg, MD, PhD1
1Erasmus University Medical Center, Rotterdam, Netherlands, 2Radboud University Medical Center, Nijmegen, Netherlands, 3University Medical Center Utrecht, Utrecht, Netherlands
Abstract Body:
Objective: AscAAs can develop in the aortic root or the tubular ascending aorta, and growth patterns may differ. This study investigates male-female differences across various ascending aortic aneurysm (AscAA) presentation and growth phenotypes.
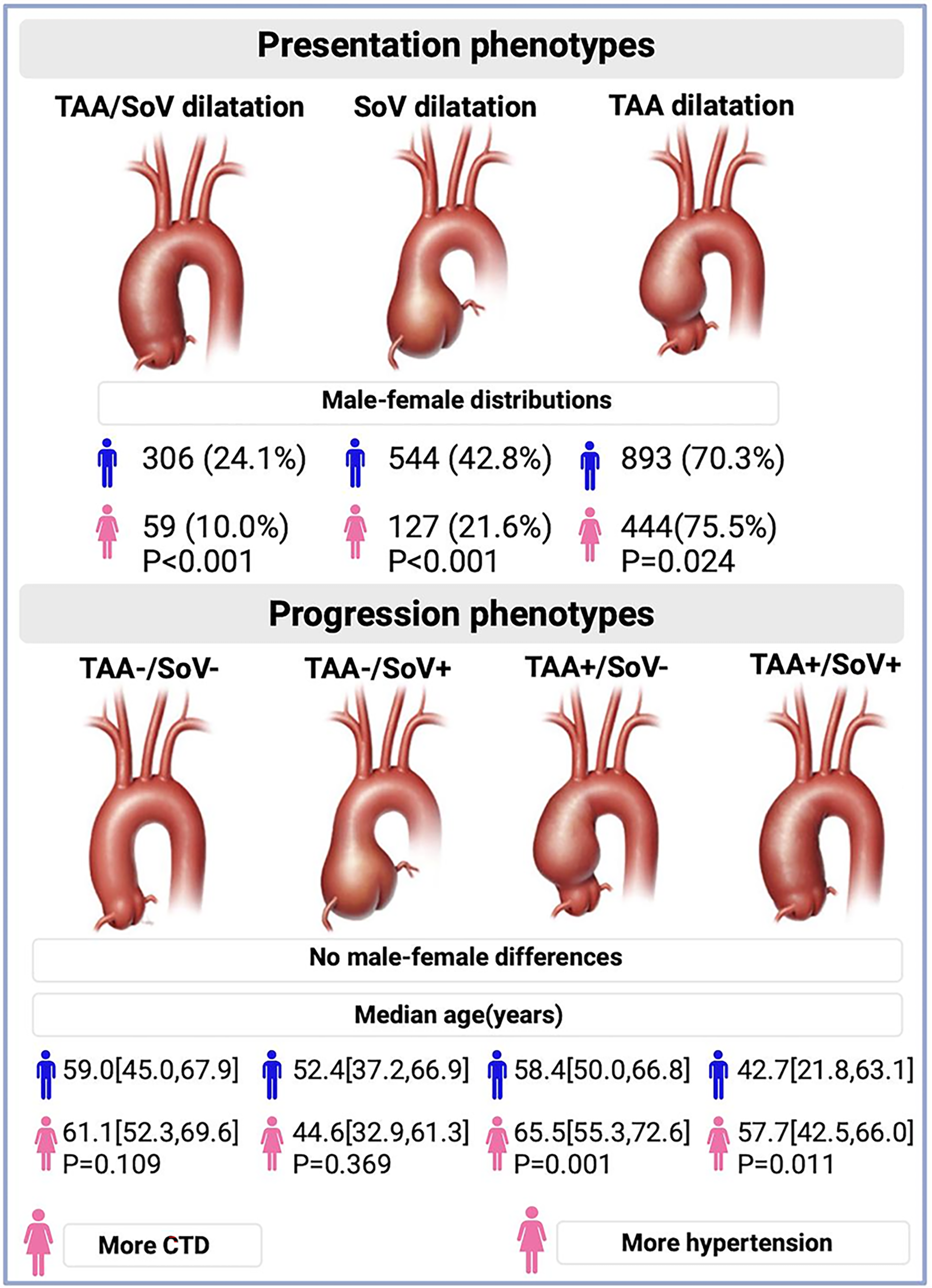
Methods: Adults who received diagnostic and/or follow-up imaging of an ascending aortic aneurysm in two centers (2007-2022) were included. Aortic dilation at presentation was assigned if the diameter was >40 mm. Growth estimates were established using individual linear regression for patients with >1 imaging evaluations in a same imaging modality on two levels: tubular ascending aorta (TAA) and the Sinus of Valsalva (SoV)). Growth was categorized as <0.45 mm/year (no-progression(-)) and >0.44 mm/year (progression(+)), leading to 4 phenotypes: TAA+/SoV+, TAA+/SoV-, TAA-/SoV+, TAA-/SoV- (Figure 1).
Results: In total, 1,858 patients were included (31.2% women), of whom 1,172 had 2 or more serial imaging evaluations. Figure 1 shows male-female distribution and mean age at presentation of the different phenotypes. Among the progression phenotypes, no differences in sex-distributions were observed (p=0.207). Within progession phenotypes, women in the TAA+/SoV+ and TAA+/SoV- groups were older (57.7 vs. 42.7 years, P=0.011; 65.5 vs. 58.4 years, P=0.001, respectively). These differences persisted when patients with genetic disease were excluded. Women in the TAA+/SoV+-progression-group had more hypertension compared to men (61.8% vs 32.8%, P=0.010). Women in the TAA-/SoV-progression-group had more genetic disease compared to men (20.8% vs 15%, P=0.008).
Conclusions: AscAAs show significant male-female differences in different presentation phenotypes, and not in progression phenotypes. Within TAA growth phenotypes, women presented at an older age, suggesting that male-female differences are location-dependent. Further research is needed to understand the several intertwined factors accociated in different AscAA phenotypes.
Control Number: 24-A-40-HVS
Presentation Number: 19
Publishing Title: The Heart Valve Society’s Medical Registry: Going Beyond Procedure Related Outcomes
Author Block:
Reda Rhellab1, Kevin M. Veen1, Johanna J. Takkenberg1, Jolanda Kluin1, Pouya Youssefi2
1Erasmus MC, Rotterdam, Netherlands, 2St George's Hospital, London, United Kingdom
Abstract Body:
Objective: Within the field of heart valve disease (HVD), providers are increasingly involving patients in their decision making, shifting away from prioritizing only procedure-related outcomes, towards also focusing on patient related outcome measures (PROMs). This shift has led to a need to collect detailed long-term preoperative multi-centre data and patient-centred information while adhering to uniform outcome evaluation measurements. This data can help guide surgeons, physicians and patients in choosing whether to intervene or not and help optimize timing of intervention. The existing HVS Aortic Valve Database comprises entry of patients at time of intervention, with data collected over the patient’s lifespan of follow-up. This new Medical Arm Registry for the database will be an invaluable tool to assess the natural history of HVD from diagnosis, through surveillance and medical management, to the point of intervention.
Methods: The HVS Medical Arm Registry will include patients with at least moderate valve disease according to the definitions agreed upon by the ICHOM-initiative, with or without aneurysm of the proximal aorta. The Registry will have an ambispective design.
Results: Data are entered on a web-based case report form containing 569 fields with a hierarchical structure through a secure data-entry system (Castor EDC), according to a predefined data dictionary. The data capture system is set up according to good clinical practice guidelines and is compliant with both American and European legislation. Collected data include: patient characteristics at diagnosis including prescribed medication, longitudinal echocardiographic measurements, hospital admissions, and (valve related) events during at least yearly follow-up. Collection of PROMs will be optional but strongly encouraged. If patients undergo an intervention, they will be followed in the linked HVS Aortic Valve Database for lifelong HVD outcome observation.
Conclusions: A multinational multicentre pilot study will be performed as a proof of concept. Participation of other centres is welcomed.
Control Number: 24-A-120-HVS
Presentation Number: 21
Publishing Title: Mitral Annular Disjunction Length, ECG Abnormalities And Myocardial Fibrosis In A Large Cohort Of Patients With Mitral Valve Prolapse
Author Block:
Luca Cristin, Lionel Tastet, Gene Hu, Shalini Dixit, Lisa J. Lim, Dwight Bibby, Arya Farzin, Yoo Jin Lee, Francesca Nesta Delling
University of California San Francisco, San Francisco, CA, USA
Abstract Body:
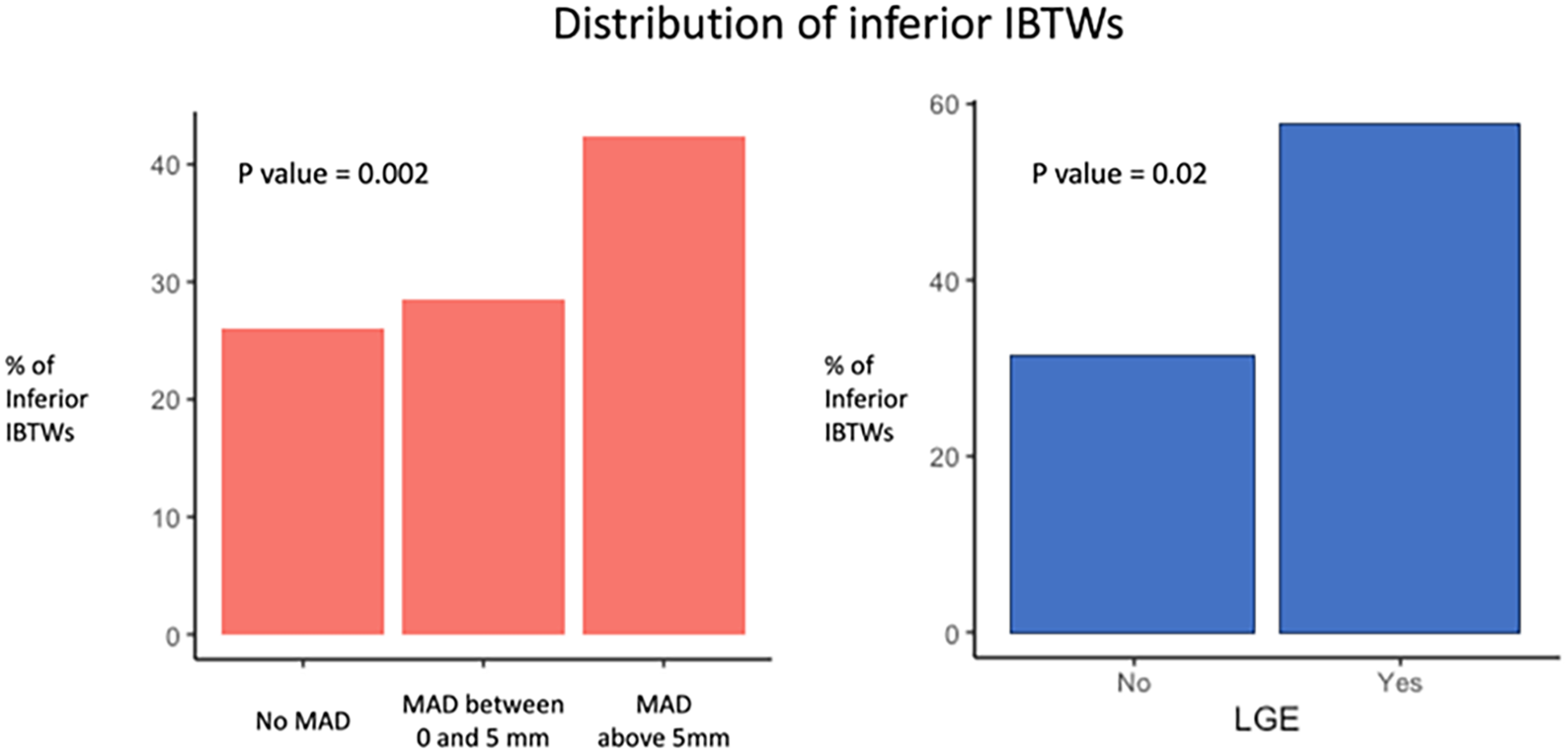
Objective: Mitral annular disjunction (MAD) can exacerbate the abnormal valvular-myocardial mechanics observed in patients with mitral valve prolapse (MVP) and is linked to a higher risk of complex ventricular ectopy (ComVE). Our objective is to determine whether the severity of MAD predicts greater myocardial traction, as expressed by a higher prevalence of inverted or biphasic T waves (IBTWs) on ECG and focal fibrosis.
Methods: We reviewed ECGs from 747 MVP patients at the University of California San Francisco between 2013 and 2023. MAD was measured on transthoracic echocardiography at end-systole. In a subset of 179 patients with contrast cardiac magnetic resonance (CMR), we assessed the presence and location of late gadolinium enhancement (LGE).
Results: Among 747 MVP patients (49% female, mean age 65±18), 33% had IBTWs, 35% had ComVE, 64% had no MAD, 7% had MAD between 0 and 5mm, and 29% had MAD >5mm. Patients without MAD had similar prevalence of IBTWs compared to patients with MAD between 0 and 5mm (26% vs 29%, p=0.94). In contrast, patients with MAD >5mm had a substantially higher IBTW prevalence than those without MAD (42% vs. 26%, p=0.002). MVPs with CMR showed higher IBTW rates when LGE was present in the papillary muscle and/or basal inferolateral wall than those without LGE (19/33 vs 23/74, p=0.02). In multivariable analysis, MAD >5mm remained a significant predictor (p=0.002) of IBTWs independent of age, sex, bileaflet subtype, mitral regurgitation severity, and cardiovascular risk factors. Conversely, MAD between 0 and 5mm was not associated with IBTWs (p=0.60).
Conclusions: In a large, unselected MVP sample, only MAD >5mm is associated with a higher prevalence of IBTWs. Among individuals with IBTWs, LGE presence is common, suggesting that repolarization abnormalities in MVP may be evident when more severe MAD and myocardial traction are present.
Control Number: 24-A-163-HVS
Presentation Number: 22
Publishing Title: Mitral Valve Prolapse Induces Localized Left Ventricular Myocardial Fibrosis In A Novel Large Animal Model
Author Block:
Antonia van Kampen1, Jordan E. Morningstar2, Yasufumi Nagata1, Guillaume Goudot1, David Izquierdo-Garcia1, Peter Caravan1, J. Luis Guerrero1, Koushiar M. Yaghoubian1, Rebecca S. Woodcock1, Andrea Slate1, Brittan Morris1, Suzanne Sullivan1, Usha Tedrow3, Nathaniel Steiger3, Michael A. Borger4, Serguei Melnitchouk1, Russell A. Norris2, Robert A. Levine1
1Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA, 2Medical University of South Carolina, Charleston, SC, USA, 3Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA, 4Leipzig Heart Center, Leipzig, Germany
Abstract Body:
Objective: Mitral valve prolapse (MVP) has recently been associated with localized left ventricular (LV) fibrosis linked to malignant arrhythmia and sudden cardiac death. However, fibrosis mechanisms remain unknown, with no large animal model to distinguish mechanical and genetic influences. We tested the hypothesis that surgically induced MVP leads to localized myocardial fibrosis in LV regions mechanically linked to the mitral valve, aiming to establish a reproducible large animal model of MVP as a platform for mechanistic studies.
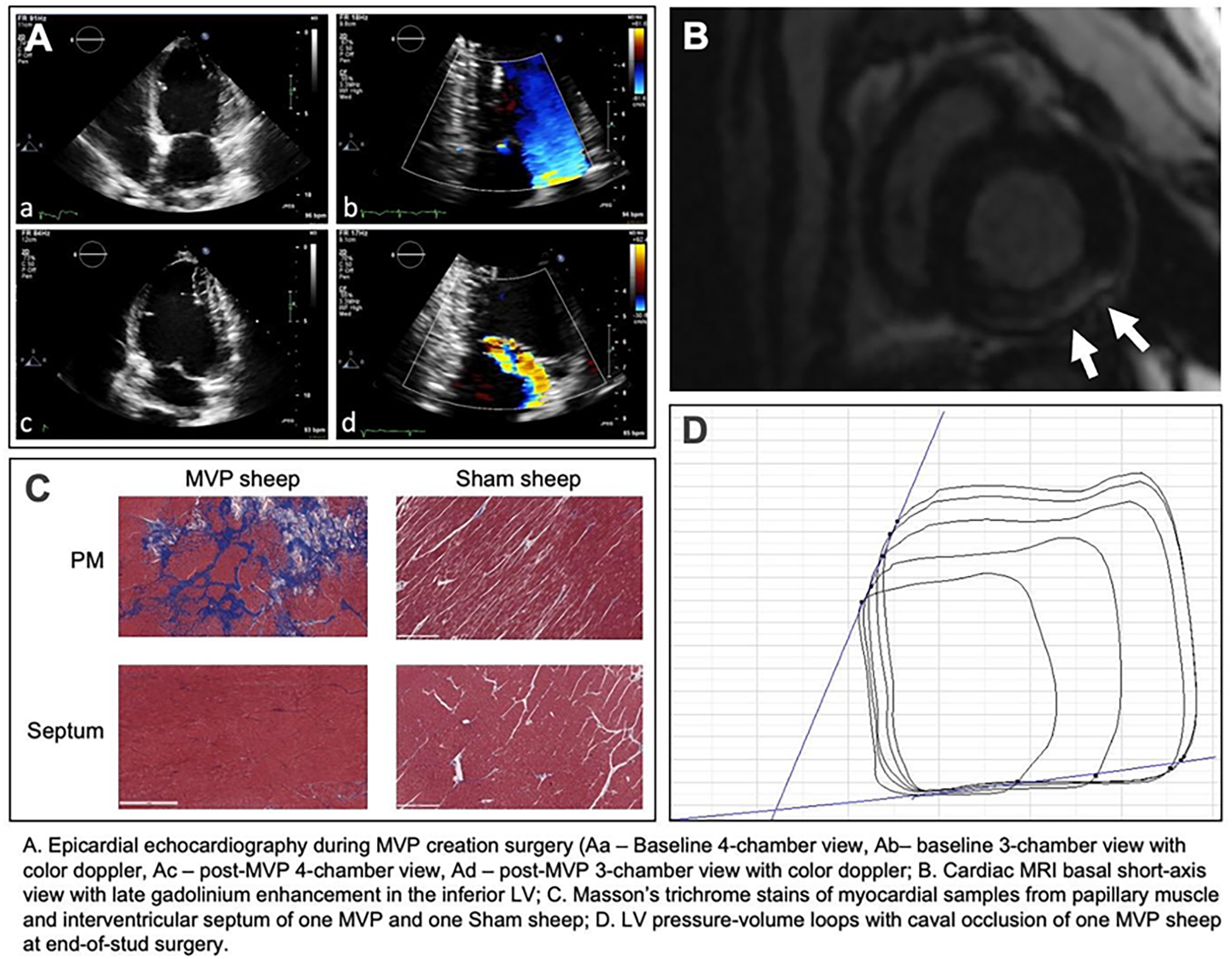
Methods: In 6 adolescent sheep, MVP was created surgically by replacing primary chordae tendineae to P2 with longer artificial chords. Intraoperative echocardiography and LV pressure-volume loops were obtained. After 7 months recovery, cardiac MRI with gadolinium and T1-mapping were done before end-of-study surgery with repeat echo and pressure-volume loops. Three naive sheep were similarly studied. Myocardial samples from valve-linked papillary muscle and inferobasal LV and control septal regions were analyzed by histology. Electrophysiological exams were performed using intracardiac echocardiography and the CARTO-system.
Results: All 6 MVP sheep showed pronounced localized LV fibrosis in valve-linked regions but not control regions on MRI, with replacement fibrosis by Masson’s trichrome stain. Sham sheep had no fibrosis, with similar LV function and contractility at end-of-study. Electro-anatomic mapping revealed fractionated papillary muscle electrograms and steeper restitution curves, both markers of predisposition for ventricular arrhythmias, in the MVP but not the naive sheep.
Conclusions: In a novel surgically created large animal model of MVP, localized fibrosis with resulting pro-arrrhythmic features is induced in formerly healthy LV myocardium. This suggests a mechanical mechanism is sufficient to create the localized LV fibrosis associated with arrhythmia in MVP patients. This model provides a platform to study fibrosis mechanisms and investigate therapeutic approaches to avoid catastrophic events in MVP patients.
Control Number: 24-A-165-HVS
Presentation Number: 23
Publishing Title: Effects Of Functional Mitral Regurgitation Repair With Different MitraClip Sizes
Author Block:
Gediminas Gaidulis1, Lakshmi Dasi2, Muralidhar Padala3
1Emory University, Atlanta, GA, USA, 2Georgia Institute of Technology, Atlanta, GA, USA, 3Nyra Medical, Atlanta, GA, USA
Abstract Body:
Objective: MitraClip implant for transcatheter edge-to-edge repair (TEER) is available in four sizes, yet we lack a quantitative understanding of how differently sized clips alter mitral valve (MV) biomechanics. We report patient-specific computational analysis that shows the biomechanical effects of TEER with different clip sizes for functional mitral regurgitation (FMR) repair.
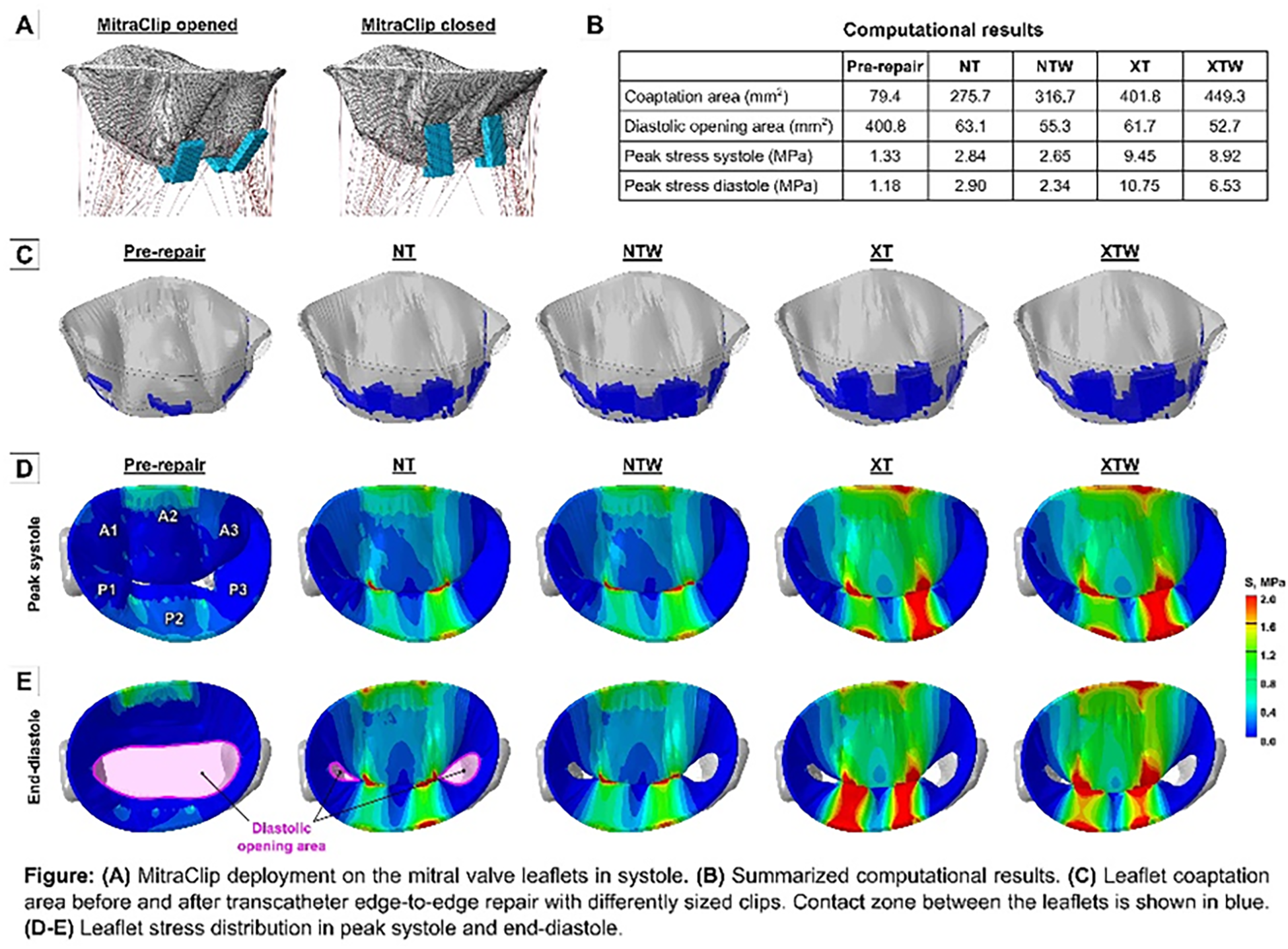
Methods: 3D echo dataset was obtained from a post-myocardial infarction pig with FMR, and computational MV model was generated. The closure of the valve was simulated, and two regurgitant gaps were observed. TEER was mimicked by applying a pair of MitraClip NT (4×9 mm), NTW (6×9 mm), XT (4×12 mm), and XTW (6×12 mm) implants at the regurgitant sites (Fig A). Simulation of post-repair MV function during a full cardiac cycle was done for each implant size.
Results: Computational results are summarized in Fig B. In systole, regurgitant gaps were eliminated and leaflet coaptation improved with each implant size (Fig C). However, TEER increased leaflet stresses and greatly reduced diastolic opening area of the valve. In systole, peak stress increased from 1.33 MPa pre-repair to 2.84 MPa with NT, 2.65 MPa with NTW, 9.45 MPa with XT, and 8.92 MPa with XTW implant (Fig D). In diastole, stresses further increased to 2.90 MPa with NT and 10.75 MPa with XT but dropped to 2.34 MPa with NTW and 6.53 MPa with XTW clip (Fig E). Diastolic opening area after TEER was reduced by 84.3% with NT, 86.2% with NTW, 84.6% with XT, and 86.9% with XTW implant.
Conclusions: In this model, larger coaptation area and lower stresses were observed with wider implants compared to the same arm length narrower clips, but the reduction of diastolic opening area was greater as well, which may be considered during TEER procedure planning.
Control Number: 24-A-124-HVS
Presentation Number: 24
Publishing Title: Clinical And Echocardiographic Outcomes After Mitral Valve Repair For Organic Mitral Regurgitation Using A New Saddle Shaped Semirigid Annuloplasty Ring
Author Block:
Giovanni Domenico Cresce, Daniele Zoni, Salvatore Poddi, Luciana Benvegnù, Ilaria Tropea, Tommaso Hinna Danesi, Loris Salvador
San Bortolo Hospital, Vicenza, Italy
Abstract Body:
Objective: Mimic the native annular geometry is the goal of newer generations of annuloplasty rings. In this study we aimed to investigate outcomes of mitral valve repair (MVR) for degenerative mitral valve disease using a new saddle-shaped semirigid annuloplasty ring.
Methods: All consecutive patients underwent MVR using a saddle-shaped annuloplasty ring between February 2019 and August 2023 were included. Preoperative characteristics, operative data, in-hospital outcomes and clinical and echocardiographic follow-up were analyzed. The severity of the mitral regurgitation was classified as none/trivial, mild, moderate, and severe and assessed in a semiquantitative manner by color-Doppler flow mapping.
Results: The analysis included 301 patients (196 males, mean age 60±13.0 years, mean EuroSCORE II 1.78±1.42). Preoperative NYHA class III-IV was present in 81 cases (26.9%) and 90 patients (29.9%) had preoperative atrial fibrillation. The mean LVEF was 61.1±8.4%. Ninenty-nine patients (32.8%) underwent one or more concomitant procedures. All cases were performed using a totally endoscopic approach, through a 3-4 cm. right mini-thoracotomy. Mean cardiopulmonary bypass and cross-clamp time were 155.0±42.7 and 101.6±52.7 minutes respectively. Two patients died during hospitalization (0.66%). Patients’ follow-up was 100% completed and the mean follow-up was 1.61±1.33 (0.32-2.96) year and a total of 99.4% of patients had an echocardiographic assessment at a mean of 1.09±1.34 (0.26-1.66) years after the operation. The Kaplan-Meier survival was 97.8% and 97.1% at 1 and 2 years respectively. Freedom from mitral valve reoperation was 98.9% both at year 1 and 2. At the latest follow-up, 294 patients(97.7%) showed none/trivial-mild mitral valve regurgitation and 282(93.7%) showed NYHA class I-II.
Conclusions: MVR with a saddle shaped semirigid annuloplasty ring is associated with low operative mortality and excellent clinical and functional outcomes. The low incidence of reoperation demonstrated that the semirigid design restoring the physiological 3-dimensional morphology and physiological movement contributed to the repair effectiveness and durability.
Control Number: 24-A-116-HVS
Presentation Number: 25
Publishing Title: Comparing Outcomes Between Minimally Invasive-first Approach For Mitral Valve Surgery And Sternotomy In Acute Bacterial Endocarditis
Author Block:
Puwadon Thitivaraporn1, Michel Pellerin1, Maude-Éloïse Piché-Lemieux2, Denis Bouchard1
1Montreal heart institute, montreal, QC, Canada, 2University of Montreal, Montreal, QC, Canada
Abstract Body:
OBjective: To compare short and long-term clinical outcomes of minimally invasive-first approach for acute bacterial mitral valve endocarditis in a Canadian patient cohort.
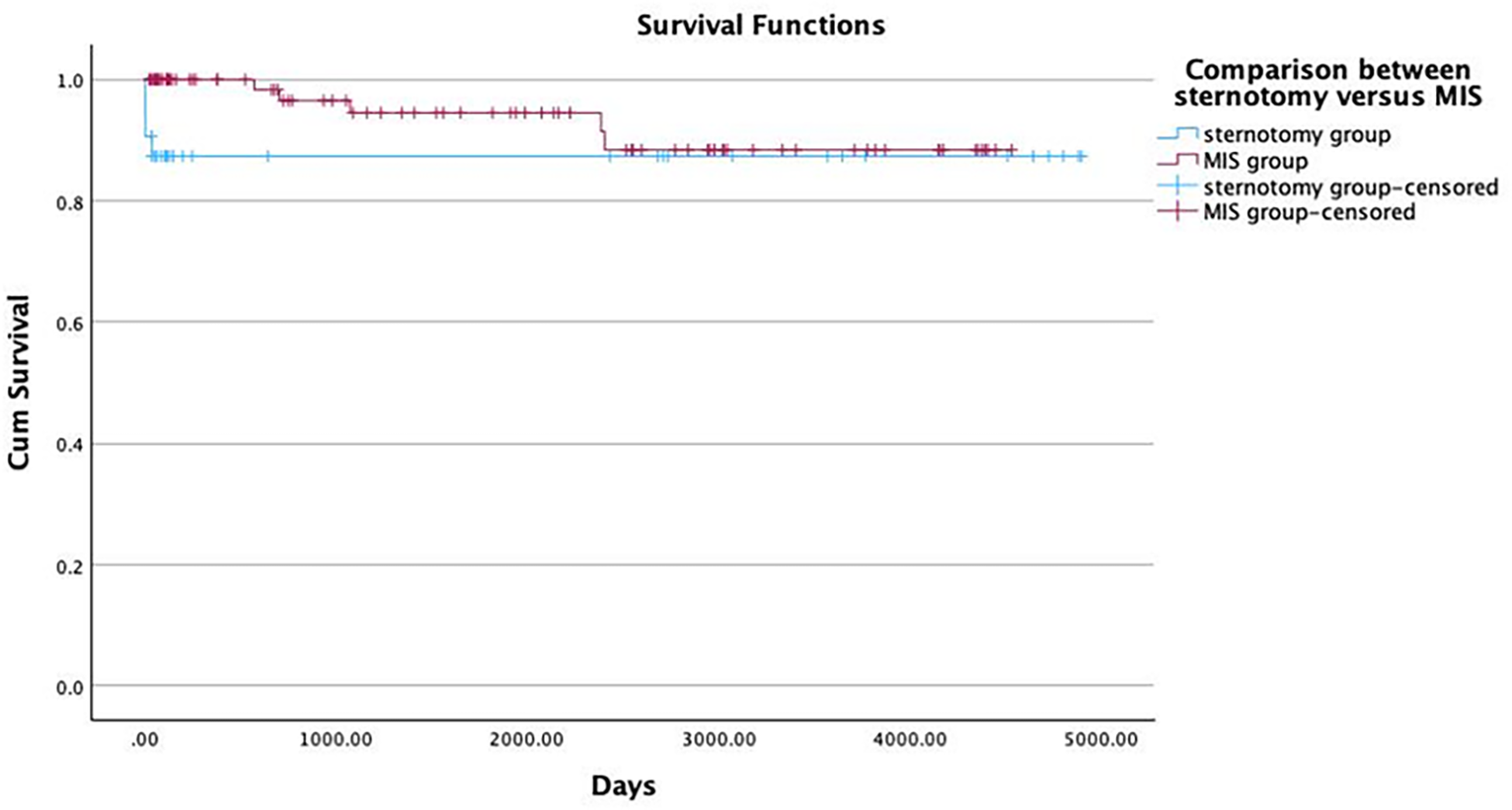
Methods: This retrospective study compared between sternotomy mitral and minimally invasive surgical approach (MIS). During 2010-2023, a total number of 118 patients (32 in sternotomy and 86 in the MIS group) were reviewed. Primary outcomes included ICU stay, length of stay, and mortality rate. Statistical analyses, including Kaplan-Meier survival curves, were conducted.
Results: Median ages were 57.56±15.61vs.58.91±16.48 in sternotomy and MIS group. Prosthetic valve endocarditis was 3.1 and 3.5% in each group. Other demographic data were comparable and not statistically different. Concomitant cardiac surgery necessitates sternotomy was 43.8% in the sternotomy and 9.3% in the MIS group. The reparation rate was 54.8% in sternotomy while 72.1% in the MIS group (0.079). Successful repair confirmed by echocardiography were 93.3% in sternotomy and 91.2%(p=0.793) in MIS group at mean pressure gradient 3.953 and 3.627 (p=0.415) respectively. Cardiopulmonary bypass and clamp time were shorter in the MIS cohort at 109.41±55.64vs.99.13±33.43; p<0.001 and 87.38±49.57vs.76.94±28.36; p<0.001. The lower postoperative cardiac enzyme, ventilation time, transfusion, permanent pacemaker implantation, and inotropic/vasoactive drug in the MIS group were observed yet insignificant. We found lower rate of acute kidney injury/requiring hemodialysis 12.5%vs2.3%(p=0.025), and postoperative infection 15.6%vs2.3%(p=0.007) in the MIS cohort. ICU stay in the MIS was 1(1,10) day, on the contrary, 3(1,42) days in the sternotomy group, p<0.001. In-hospital mortality was 12.5% in the sternotomy and 2.3% in the MIS group; p=0.025. Reinfection rates were not different throughout follow-up period(p=0.577).
Conclusions: A minimally invasive-first approach for mitral valve surgery in acute endocarditis for specific patients is feasible and revealed beneficial aspects of acute phase recovery: lower acute kidney injury/long-term dialysis, ICU, and length of stay.
Control Number: 24-A-76-HVS
Presentation Number: 26
Publishing Title: Impact Of Surgical Approach On Quality Of Life
Author Block:
Elena Sandoval, Ignacio Morales-Rey, Anna Muro, Silvia Camon, Montserrat Trashorras, Daniel Pereda
Hospital Clinic, Barcelona, Spain
Abstract Body:
Objective: We sought to investigate if robotic mitral surgery had a positive impact on postoperative quality of life.
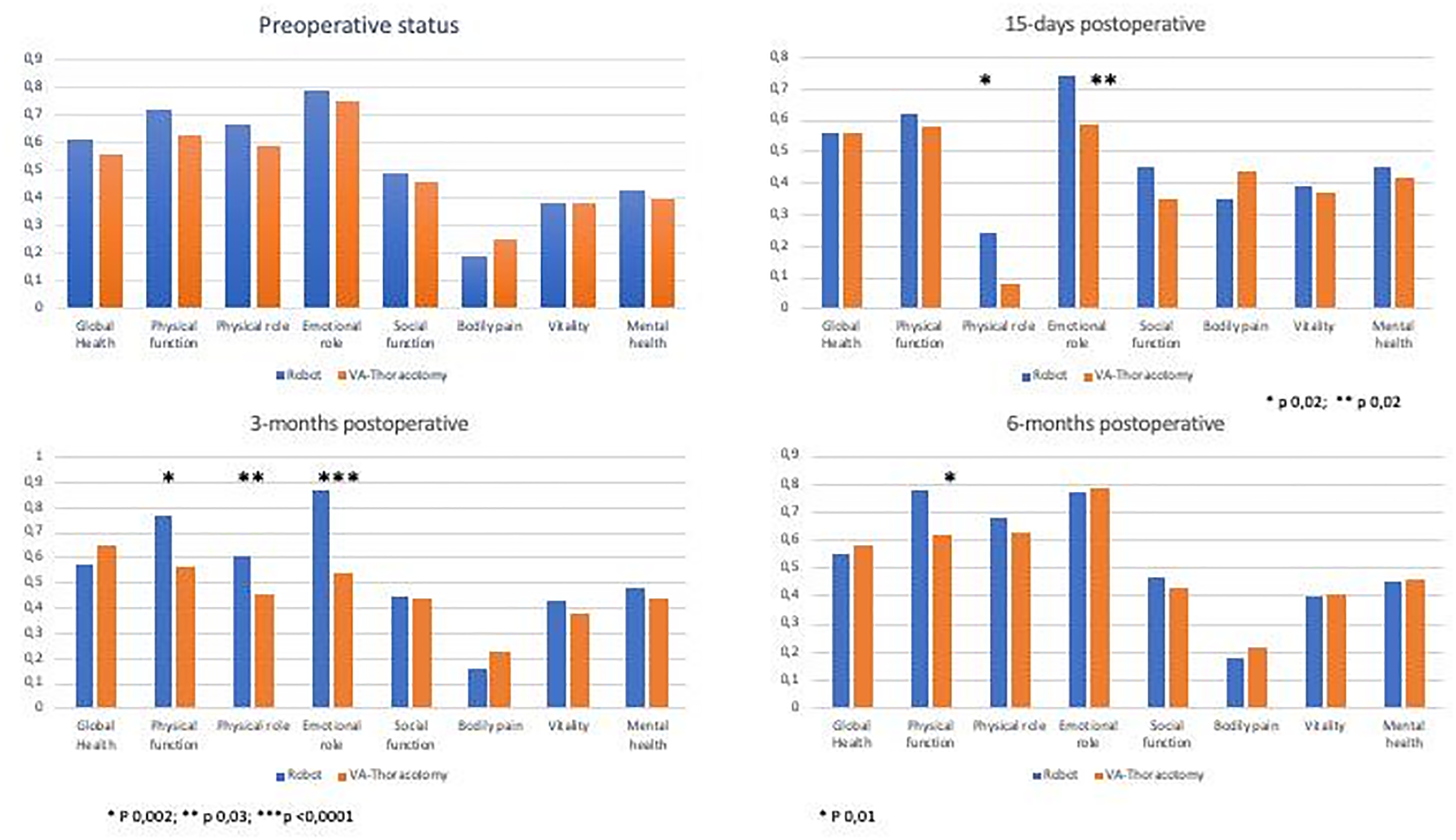
Methods: Patients who underwent isolated mitral repair or replacement in our institution since 2020 were offered to participate. A previously validated quality of life questionnaire (SF-36) was given to the patients at different postoperative timeframes (preoperative, 15 days postoperative, 3 months and 6 months after the surgery). After collecting data, patients were divided in 2 groups depending on the surgical approach (robotic-R or video-assisted thoracotomy-VAT). Data are presented as percentages; comparisons of the eight quality of life items were made between groups using the Chi-square test.
Results: There were no preoperative differences in any of three 8 items between R and VAT group. However, the R group showed better results in both the physical role functioning (23% vs 8%, p 0,002) and emotional role functioning (74% vs 59%, p 0,02) when compared to the VAT group at 15 days. Three months after the surgery, physical function (76% vs 56%; p 0,002), physical role (60% vs 45%; p 0,03) and emotional role (86% vs 53%; p<0,0001) were significantly better in the R group. At 6 months only physical function showed significant differences between groups (78% vs 62%; p 0,01).
Conclusions: Despite the study limitations, the robotic approach seems to provide a better postoperative recovery and thus and improved quality of life compared to a video-assisted thoracotomy approach.Further studies are needed to confirm the findings.
Control Number: 24-A-132-HVS
Presentation Number: 27
Publishing Title: Computational Prediction Of Heart Valve Dynamics To Aid Diagnosis And Cardiac Interventions: Are We There Yet?
Author Block:
Vijay Govindarajan1, Nils P. Johnson2, Krishnan Chandran3, David D. McPherson2
1Boston Children's Hospital, Boston, MA, USA, 2University of Texas Health Science Center, Houston, TX, USA, 3The University of Iowa, Iowa City, IA, USA
Abstract Body:
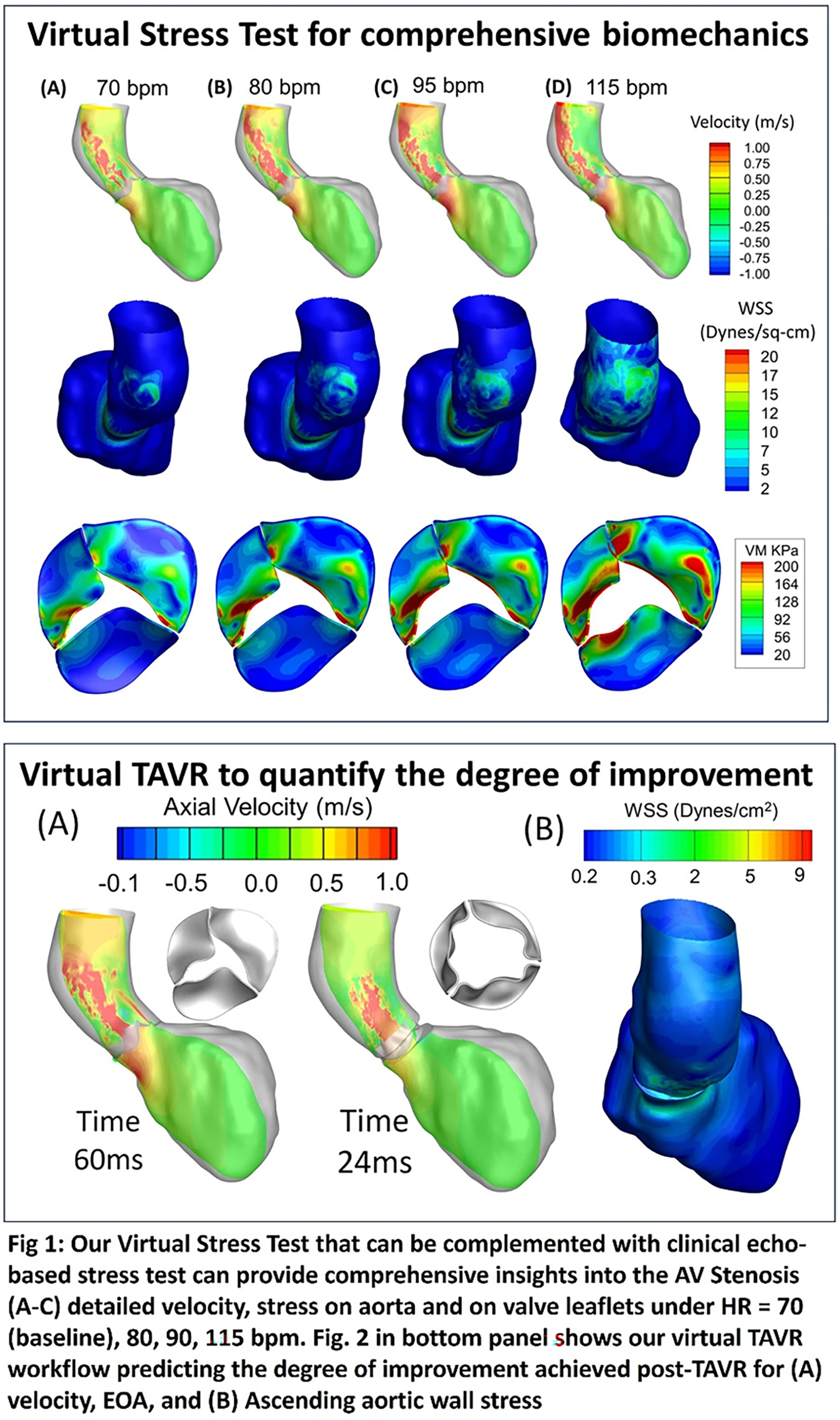
Objective: Computational modeling is increasingly used to understand cardiac disease progression and improve interventional predictability. However, physiologically realistic models of heart valves incorporating patient’s left ventricular dynamics and aorta do not exist due to its complex dynamics. To this end, we present a novel high-performance modeling approach aimed at providing comprehensive biomechanics for improved diagnosis, intervention predictability, and personalization in aortic valves by allowing virtual stress test on diseased valves and predict post-op valve function and hemodynamics.
Methods: A moderate AS with increasing LV contraction was subjected to virtual stress tests to determine the dynamics of systolic ejection under baseline (70 bpm) and stress (80, 90, 115 bpm) using our validated in-house Fluid-structure Interaction (FSI) algorithm that makes it simple to translate patient-specific anatomy. To quantify the degree of improvement in post-op aortic hemodynamics, TAVR was virtually implanted and compared with pre-op (diseased) data at baseline heart data.
Results: Predictions demonstrated that that aortic flow turbulence in moderate AS (Re = 11,700) during exercise (115 bpm) can be similar to severe AS at rest (Re=10,000) resulting in a greater dissipation losses rising linearly with heart rates. As LV contraction rose, each valve cusp underwent a distinct non-linear rise (>100%) in mechanical stresses that can accelerate calcification. Interestingly, our evaluation revealed that the heterogenous ΔP vs. Q relationship in AS observed clinically can be attributed to a non-linear rise in aortic valve area occurring during mid-systole. Aortic hemodynamics improved post-TAVR by reducing dissipation losses by ∼5 fold and restoring near-normal peak-systolic velocity (1.7 m/s) in the ascending aorta.
Conclusions: Utilizing patient data in conjunction with high-performance multi-physics algorithms can serve as a potent approach for enhancing our understanding of biomechanics, thereby advancing the accuracy of heart valve diagnosis, interventional prediction and personalization.
Control Number: 24-A-122-HVS
Presentation Number: 28
Publishing Title: Biomechanical Indices That Contribute To Premature Calcification In The Pediatric Bicuspid Aortic Valve Population
Author Block:
Hail Kazik1, Harkamaljot Kandail2, Julie Kessler1, Carol Mattern1, El-Sayed Ibrahim1, Benjamin Goot1, John F. LaDisa, Jr1, Joy Lincoln1
1Medical College of Wisconsin, Wauwautosa, WI, USA, 2Medtronic, Irvine, CA, USA
Abstract Body:
Objective: Bicuspid aortic valve (BAV) is the most common congenital cardiovascular defect and characterized by formation of two, rather than three cusps. Approximately 50% of BAV patients prematurely develop calcification and aortic stenosis by the age of 35. The mechanisms underlying premature calcification are unknown, but it has been suggested that abnormal biomechanical stimuli induced by the bicuspid anatomy plays a role, although this speculation has not been fully delineated. Our objective is to define BAV-induced fluid dynamics preceding calcification and identify mechanosensitive responses that promote calcific changes at molecular and cellular levels.
Methods: After IRB approval, we used cardiac MRI studies from 23-year-old patients (BAV and control) to conduct fluid structure interaction (FSI) simulations quantifying biomechanical indices including wall shear stress (WSS) and maximum principal stress prior to calcium deposition. To complement human studies, we used a mouse model of BAV (Nfatc1cre;Exoc5fl/+) to associate local biomechanical indices with spatial transcriptomics.
Results: FSI studies of the young adult BAV patient revealed higher magnitudes of WSS and maximum principal stress regionalized to the raphe, attachment, and coaptation regions compared to an age-matched tri-leaflet aortic valve control. At a comparable young adult stage, 10-week-old Nfatc1cre;Exoc5fl/+ mice exhibit increased peak aortic velocity by echocardiography, suggesting alterations in WSS and maximum principal stress vs wild-type controls. Spatial transcriptomics from BAV mice show that areas of high WSS and maximum principal stress observed in patients, associate with increased expression of calcification markers (spp1, Sparc) at 18 weeks in mice, which are not detectable at 10 weeks.
Conclusions: These findings suggest that regions prone to calcification are exposed to higher WSS and maximum principal stress magnitudes prior to pre-calcific molecular changes. Ongoing studies will integrate biomechanical indices with mechanosensitive transcriptomics underlying premature calcification to develop comprehensive risk profiles for BAV patients and more effective clinical management.
Control Number: 24-A-36-HVS
Presentation Number: 29
Publishing Title: Fatigue Resistant Polymeric Heart Valve Replacements
Author Block:
Sina Naficy1, Tina Hoang1, Xinying Liu1, Jacoppo Giarreta1, Matthew Crago1, Aeryne Lee1, David S. Winlaw2
1The University of Sydney, Sydney, Australia, 2Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, USA
Abstract Body:
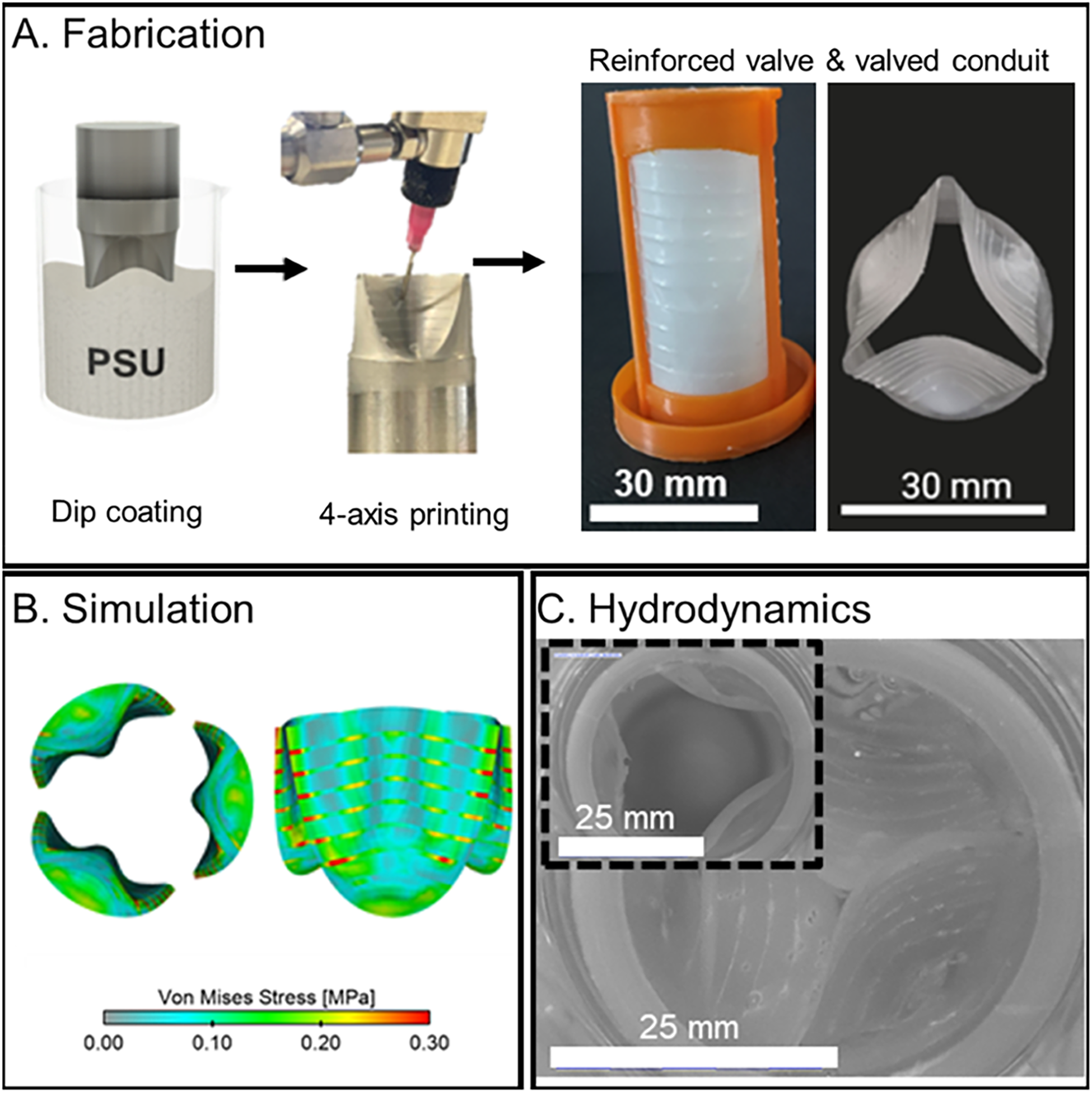
Objective: Valvular heart diseases are commonly addressed by the implantation of heart valve replacements; however, current prosthetics remain suboptimal in their durability. Fatigue-resistant polymeric heart valves can be fabricated utilizing robotic printing where elastomeric topological patterns are introduced to the valves and their leaflets. Such topological patterns are shown to prevent the progression of potential defects, significantly enhancing the valves' longevity.
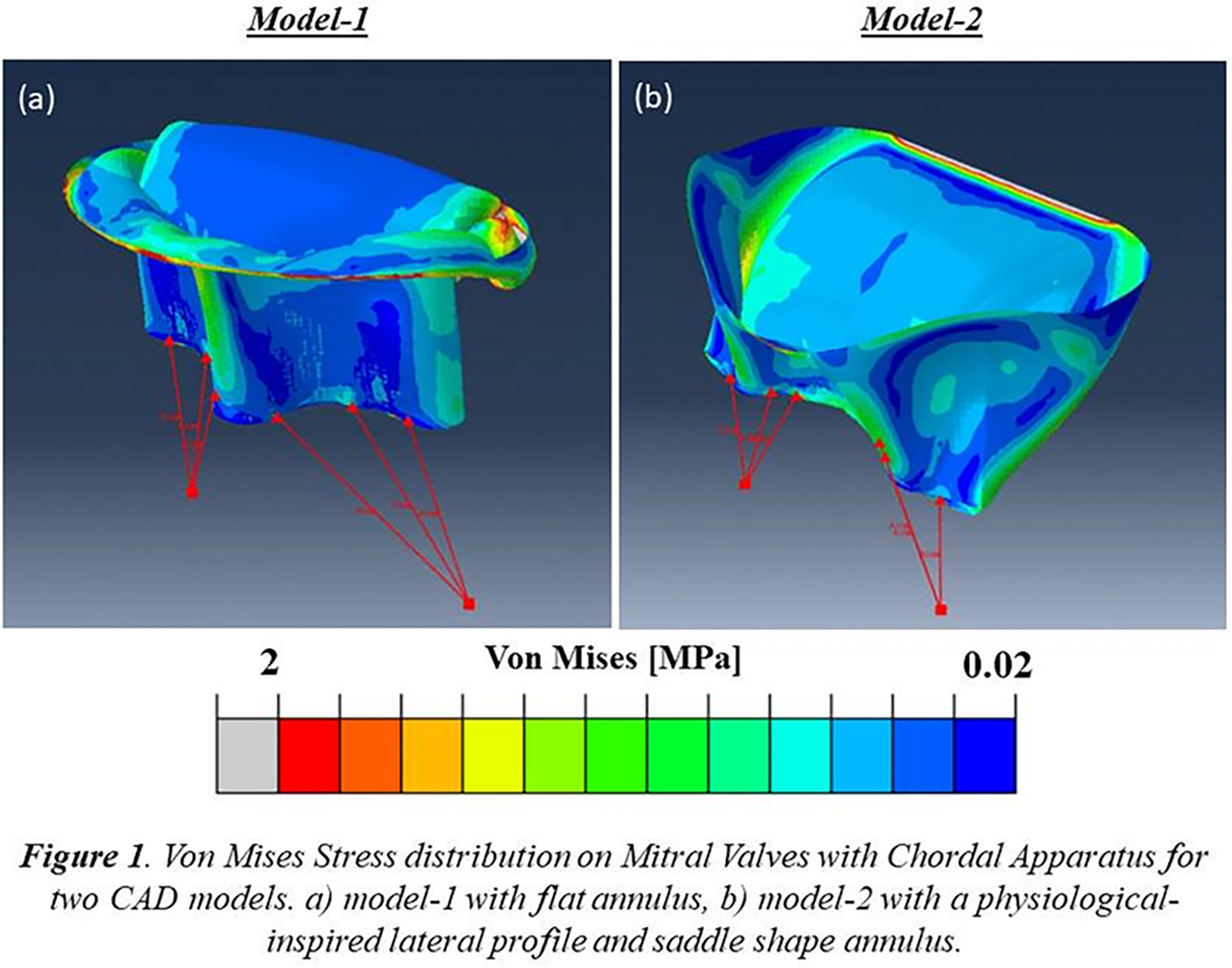
Methods: Valve designs were developed from a micro-computed tomography scan of a sheep heart valve and used to mathematically define mould geometries. A highly elastic biomedical polyurethane was used for the fabrication of polymeric valves via dip-coating. Another biomedical polyurethane with a higher stiffness was 3D printed on the valve leaflets using a 4-axis robotic printer. The effect of structural reinforcements on toughness, fatigue resistance and hydrodynamic performance was investigated. Further, computational simulation was employed using an Arbitrary Lagrangian-Eulerian method and in vitro systolic valve pressure profile as the input to assess the von-Mises stress profile across the reinforced valves. Finally, the possibility of applying structural reinforcement in flexible valved conduits was briefly explored.
Results: Structurally reinforced elastomers exhibited up to nine-fold increase in toughness and 150% increase in fatigue resistance. All reinforced valves exceeded the ISO 5840-2 standard. Furthermore, the structural reinforcement prevented the progression of induced incisions during accelerated cardiac cycling and reduced regurgitation by about 50% compared with unreinforced valves, without compromising opening performance. Subsequently, a valved conduit was developed using the structural reinforcement concept where leaflets and conduit were reinforced with circumferential elastomeric patterns. The reinforced valved conduits also exceeded the ISO 5840-2 specifications for effective orifice area and regurgitation fraction.
Conclusions: These structurally reinforced polymeric heart valve replacements could offer improved device performance and durability, lowering reoperation requirements and promoting patient quality of life.
Control Number: 24-A-14-HVS
Presentation Number: 30
Publishing Title: A Rapid And Non-invasive Approach For Aortic Stenosis Assessment And Monitoring
Author Block:
Claudia Iannini1, Joshua Bowren1, Tracy Goeken, MD2, Maximilian Emmert, MD3, Kaustubh Kale1
1Aventusoft, Boca Raton, FL, USA, 2Q2K Medical Consulting, LLC, Palm Beach Gardens, FL, USA, 3German Heart Center, Berlin, Germany
Abstract Body:
Objective: Current non-invasive methods for the assessment of aortic stenosis (AS) at point of care are unreliable and nonspecific, whereas the gold standard echocardiography assessment is expensive and complex. Given these limitations, an accurate and absolute alternative for rapid assessment is needed.
Methods: Semismocardiography (SCG) recordings of healthy patients and patients with different stages of AS were taken near the aortic and pulmonic auscultation points and near the sternum. Next, each patient’s recording was segmented into its corresponding heart beats (based on the R wave of a simultaneous electrocardiogram) and averaged to obtain the average beat for each patient. It was hypothesized here that AS introduces noise in SCG recordings between the first and second cardiac sounds during midsystole. To investigate this hypothesis, the largest mean absolute error (MAE) between the average beat (clean approximation) and each individual beat was calculated during midsystole for each patient and compared across patients.
Results: A total of 76 patients were analyzed where 63 patients were healthy, 3 patients had mild AS, 4 patients had moderate AS, and 6 patients had severe AS. These patients were divided into two groups: healthy and mild, and moderate and severe. With the optimal MAE threshold, the subjects were classified into the two groups with a sensitivity of 80%, specificity of 89.4%, positive predictive value of 53.3%, negative predictive value of 96.7%, and area under the curve of 0.908.
Conclusions: The presence of significant noise during midsystole distinguished the majority of healthy and mild AS patients from the moderate and severe AS patients. This method may provide an effective non-invasive approach for the assessment and monitoring of aortic stenosis.
Control Number: 24-A-104-HVS
Presentation Number: 31
Publishing Title: Bio-inspired Anti-calcific And Anti-thrombotic Polymeric Tavr
Author Block:
Srujana S. Joshi1, Justin Gangwish2, Nipa Khair2, Susan James2, Lakshmi Prasad Dasi1
1Georgia Institute of Technology, Atlanta, GA, USA, 2Colorado State University, Fort Collins, CO, USA
Abstract Body:
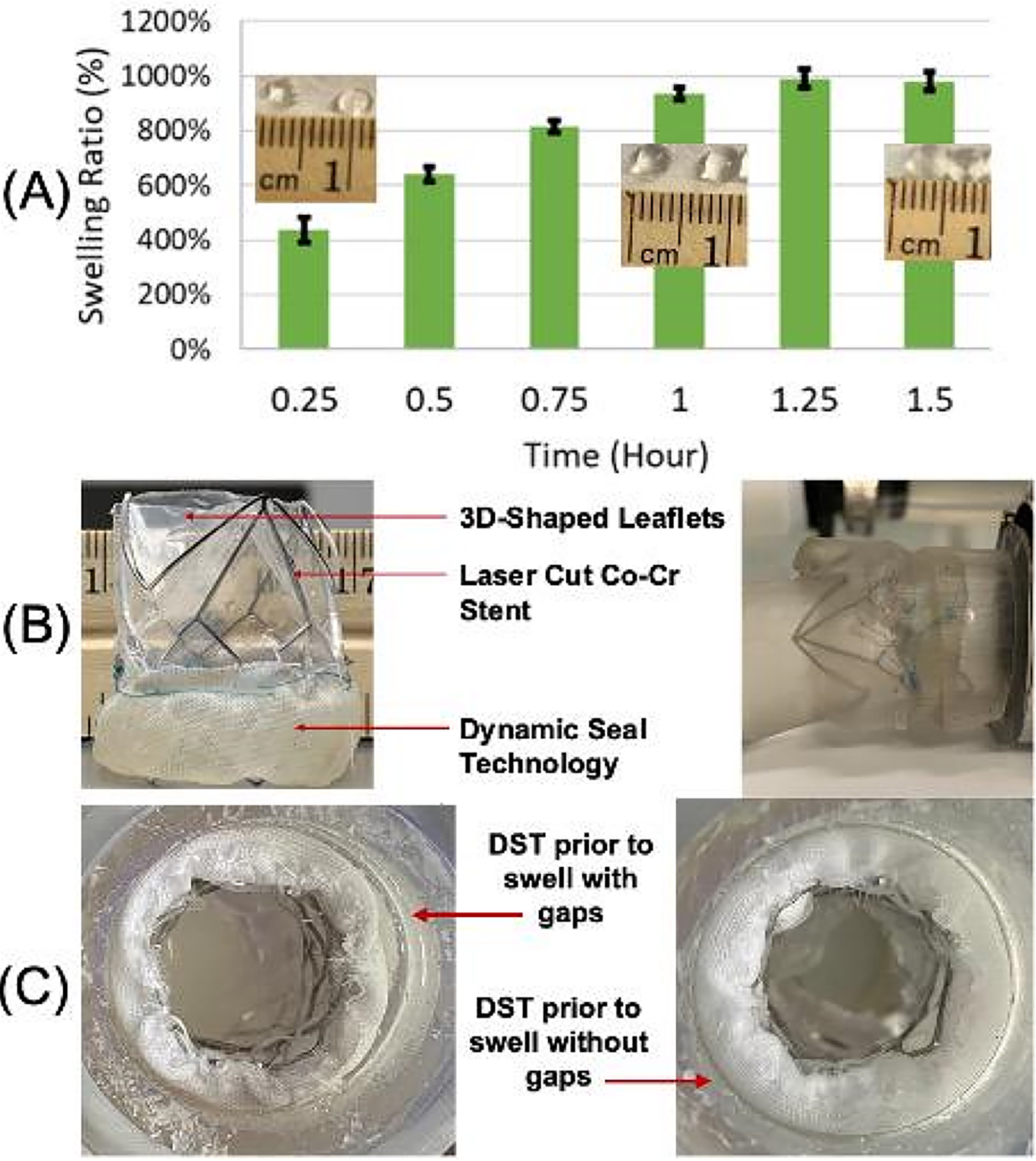
Objective: Current tissue-based TAVRs have drawbacks like calcification, structural valve degeneration, hypo attenuated leaflet thickening, paravalvular leakage - limiting device durability. To combat such drawbacks, this study aims at developing a novel polymeric TAVR, with a dynamic seal to prevent PVL. The biomaterial used is hyaluronan enhanced linear low density polyethylene, which makes the leaflets anti-thrombotic, calcification resistant, and highly durable due to the polymer’s mechanical properties.
Methods: 3D shaped polymeric leaflets were fabricated using vacuum thermoforming, assembled and mounted in an in vitro left heart simulator and tested under pulsatile adult physiological flow conditions. A dynamic seal was developed having an outer layer of texturized Dacron fabric, crosslinked gelatin beads, and an inner layer of highly porous, stretchy Dacron. The beads are synthesized by excreting a solution of gelatin into oil and then crosslinked. Using these beads, the prototype DST was assembled and deployed in a 3D printed, patient-specific, calcified aortic root using balloon expansion.
Results: The results demonstrated that the novel polymeric valve at excellent hemodynamic performance, with a pressure gradient of 4.77 mmHg and an effective orifice area of 2.33 cm2, matching the performance of current commercial TAVR devices, and ISO 5840 standards. The assembled prototype deployed in the aortic root demonstrated that the beads had swollen significantly reducing the regurgitation fraction (RF) from 35% (at 9 minutes post deployment) to 26% (30 minutes post deployment) demonstrating the functionality of both the beads as a method to reduce PVL, and the beads as a functional pocket to contain the beads upon deployment. At 90 minutes post deployment, the PVL was reduced to 23%.
Conclusions: The present study demonstrates the potential of a novel bio-inspired TAVR to overcome the concerns with the current TAVRs.
Control Number: 24-A-100-HVS
Presentation Number: 32
Publishing Title: Sex-based Differences In Tricuspid Leaflet Response To Pulmonary Hypertension
Author Block:
Colton J. Kostelnik, PhD1, Magdalena Piekarska, MD2, Boguslaw Gaweda, MD2, Austin Goodyke2, Tomasz A. Timek, MD PhD2, Manuel K. Rausch, PhD1.
1The University of Texas at Austin, Austin, TX, USA, 2Corewell Health, Grand Rapids, MI, USA.
Abstract Body:
Objective: Leaflets, once considered “passive flaps”, are now recognized as highly organized living systems composed of multiple cell types capable of responding to biomechanical and hemodynamic loads to optimize coaptation. While the mitral valve leaflet’s adaptive thickening and stiffening are well-documented, the active biological response of tricuspid valve (TV) leaflets is often overlooked. Investigating the maladaptive response to hemodynamic overload in both sexes will strengthen the understanding of TV leaflet remodeling and motivate differential treatments for female patients with functional tricuspid regurgitation (FTR).
Methods: Pulmonary hypertension (PHT) was induced in adult male and female sheep by tightening umbilical tape around the pulmonary trunk, raising systolic pulmonary artery pressure (sPAP) to ∼55 mmHg. After 12 weeks, the TV leaflets were excised for morphological comparisons and tissue characterization. Three-dimensional profilometry measured spatial thickness variations for each TV leaflet. Planar biaxial mechanical testing equibiaxially stretched 7x7mm belly samples to ∼300 mN.
Results: At the end of 12 weeks, 90.9% of sheep exhibited moderate to severe tricuspid regurgitation. Morphological analysis showed that both control and PHT TV leaflets of male sheep were consistently larger than females, and PHT leaflets were significantly larger than respective controls (p=0.03 for males, and p=0.01 for females) (Figure 1a). Average thicknesses for female PHT leaflets were thicker (489 µm) than female control leaflets (426 µm) (Figure 1b). Mechanical testing of anterior leaflets exhibited leftward shifts in the tension-stretch curves for the female PHT sheep (Figure 1c), with circumferential and radial calf stiffness increasing by 18% and 23%, respectively, compared to female controls.
Conclusions: Prolonged PHT exposure resulted in larger, thicker, and stiffer TV leaflets, especially in female sheep. Our ongoing studies resolve the heterogeneous thickening within and between each TV leaflet, which may assist in targeted treatment for FTR patients.
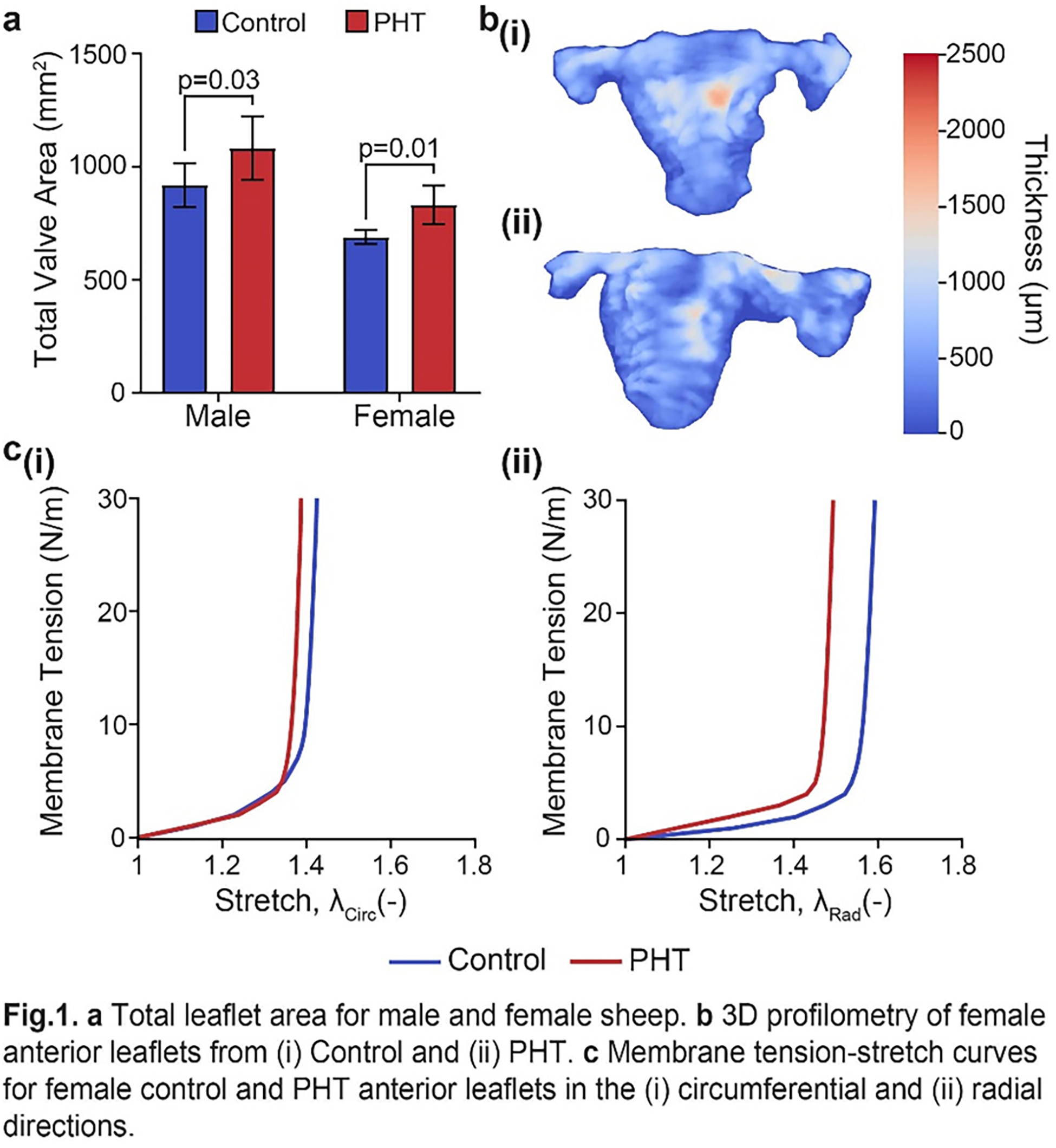
Control Number: 24-A-62-HVS
Presentation Number: 33
Publishing Title: A Mitral Valve Digital Twin For Transcatheter Edge-to-Edge Repair
Author Block:
Natalie T. Simonian1, Sneha Vakamudi2, Mark J. Pirwitz2, Michael S. Sacks1
1University of Texas at Austin, Austin, TX, USA, 2Ascension Texas Cardiovascular, Austin, TX, USA
Abstract Body:
OBjective: Transcatheter edge-to-edge repair (TEER) is a promising approach for the treatment of mitral regurgitation (MR), as the technique is generally safe and effective. However, long-term outcomes have been suboptimal and contradictory in clinical trials, and procedural optimization is complicated by the substantial heterogeneity of MR presentations and the combinatorial nature of TEER itself. A digital twin is an in-silico model that continually incorporates patient data to provide an up-to-date digital representation, and thus has enormous potential to improve patient-specific predictions. We have developed a digital twin of the human mitral valve (MV) that integrates the patient-specific full MV apparatus with time-evolving clinical data to both assess and predict the impact of TEER on MV behavior and long-term patient outcomes.
Methods: We developed an initial digital twin of the patient’s MV using standard-of-care 3D transesophageal echocardiography (TEE) images and population-averaged distributions of human MV chordae tendinae, which cannot be visualized on TEE. We calibrated the initial effective material properties of the MV apparatus by adjusting the leaflet and chordae prestrains to accurately simulate preoperative closure. We then acquired additional TEE images at 3-months post-TEER and used this data to update the digital twin to reflect changes in MV leaflet deformation in response to the TEER device (Figure 1).
Results: The MV digital twin was able to predict post-TEER geometry and deformation within 1 mm error. Follow-up data analysis of the diastolic MV 3-months post-TEER revealed notable changes in MV shape, indicating that the MV continues to adapt to the TEER device over time.
Conclusions: The MV digital twin presented here permits virtual testing of TEER in a strictly noninvasive, patient-specific context, and importantly, lays the foundation for quantitative treatment optimization based on the individual patient’s long-term response to the proposed procedure.
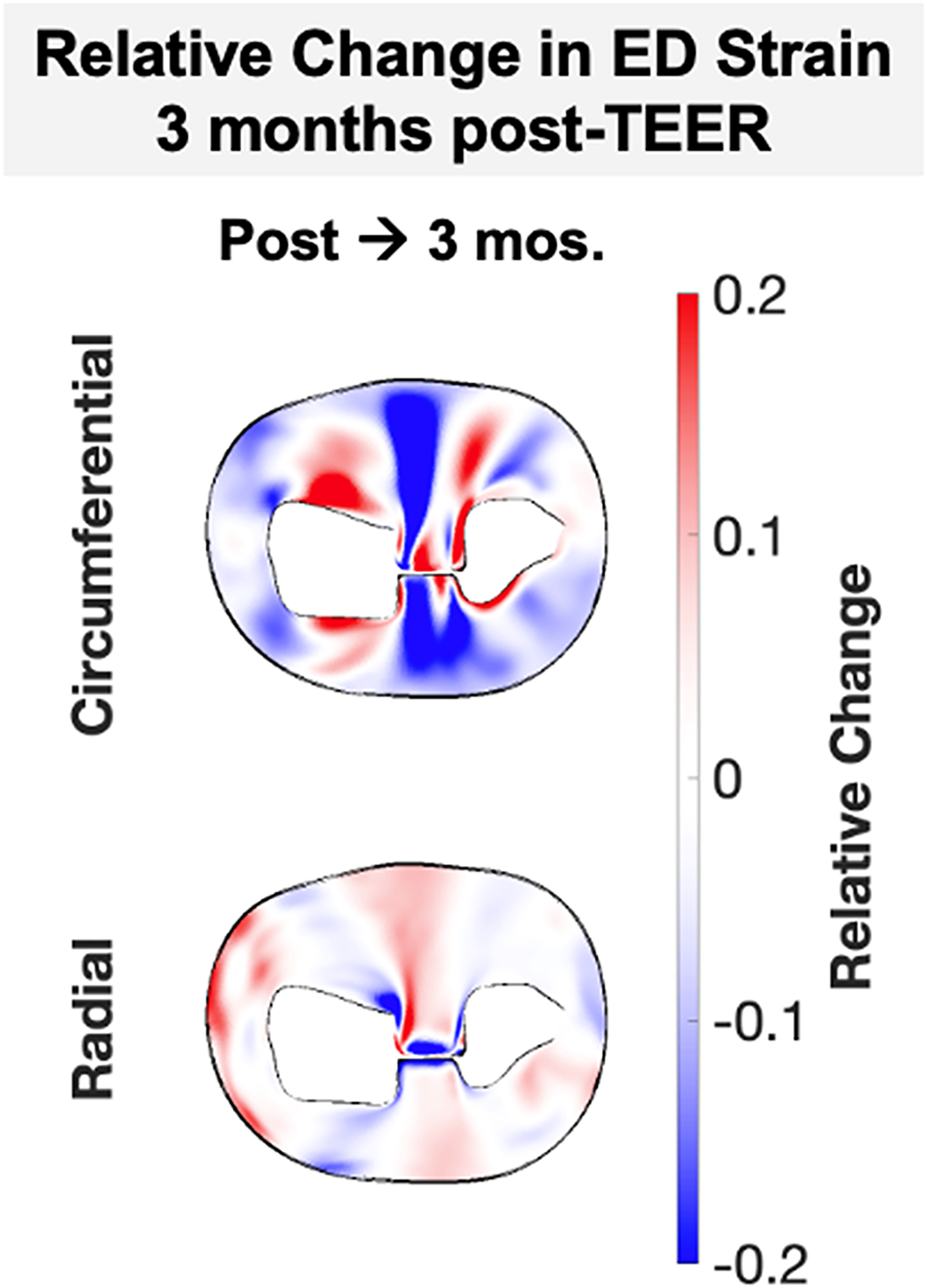
Control Number: 24-A-55-HVS
Presentation Number: 34
Publishing Title: An Integrated Finite Element, Fluid Structure Interaction And Machine Learning Approach For Biomechanical And Hemodynamics Assessment Of Patient Specific Transcatheter Aortic Valve Implantation
Author Block:
Huseyin C. Yalcin
Qatar University, Doha, Qatar
Abstract Body:
Objective: For transcatheter aortic valve implantation (TAVI), proper valve size selection and its orientation is crucial for preventing complications, such as coronary occlusion and paravalvular leak. Computational modeling offers comprehensive assessment of patient specific TAVI scenarios at pre-operative stage. Our objective is to develop computational modeling approaches for comprehensive biomechanical assessment of TAVI valves within patient specific geometries.
Methods: This investigation is in collaboration with Hamad Heart Hospital TAVI program in Qatar where Medtronic Core Valve is the most commonly used valve, hence we focused on this valve. About 120 retrospective patient data were involved. Finite element analysis (FEA) involved valve crimping, valve insertion and valve deployment to simulate complete TAVI, using ABAQUS software to calculate mechanical stresses on native leaflets and aortic root. To simulate TAVI valve hemodynamics, we implemented a fluid structure interaction (FSI) approach where computational fluid dynamics (CFD) and FEA are coupled via FlowVision and ABAQUS. Finally, to expedite FEA and FSI simulations, we implemented a machine learning (ML) approach, physics-informed neural networks for practical and fast prediction of mechanical and hemodynamics simulation data.
Results: Using ABAQUS, we successfully simulated complete TAVI implantation and carried out FEA for biomechanical assessment of retrospective TAVI operations. FEA analysis results for mechanical stress and contact pressure estimation correlated well with actual patient outcomes. Similarly, our FSI approach enabled us to assess hemodynamic valve performance for disturbed hemodynamics prediction such as paravalvular leak, which also correlated well with actual patient outcomes. Finally, our ML algorithm successfully reduced simulation times significantly while providing accurate FEA and CFD results.
Conclusions: Here, we have developed an FEA/FSI approach for simulation of TAVI implants for possible risk prediction due to contact and hemodynamics abnormalities. Simulation times were significantly reduced by a physics based ML approach
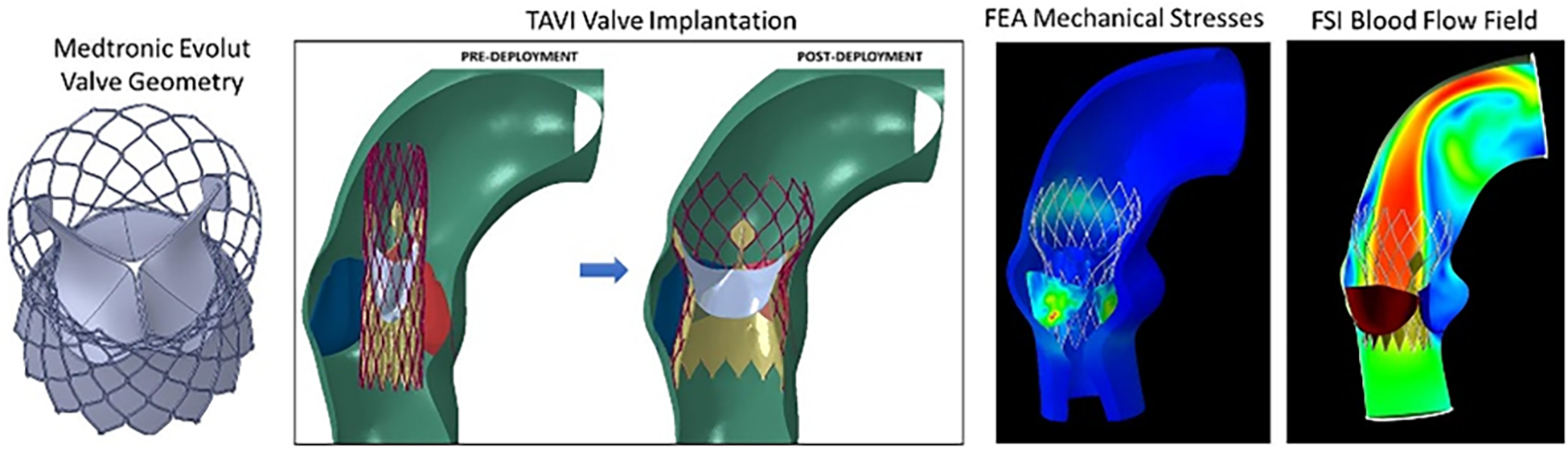
Control Number: 24-A-155-HVS
Presentation Number: 35
Publishing Title: Numerical Evaluation Of Tissue Mechanics And Organ Level Function Of Engineered Mitral Valve With Chordal Apparatus
Author Block:
Elisa Lanzalaco1, Joan D. Laubrie2, Federica Cosentino2, Viktor Balashov2, Pietro Terranova1, Giuseppe Raffa3, Michele Pilato3, Petra Mela4, Vincenzo La Carrubba5, Antonio Pantano5, Antonio D'Amore2
1University of Palermo and Rimed Foundation, Palermo, Italy, 2Rimed Foundation, Palermo, Italy, 3ISMETT, Palermo, Italy, 4Technical University of Munich, Munich, Germany, 5University of Palermo, Palermo, Italy
Abstract Body:
Objective: Mitral regurgitation (MR) represents a common mitral valve (MV) pathology. In secondary regurgitation, incomplete valve closure is due to ventricular dilation that is produced by cardiac infarction. MV replacement is the gold standard to address this pathology. However, valve repair remedies are still affected by significant failure rates and absence of chordal apparatus (CA), neglecting the natural mechanical continuum ventricle-cusps. Furthermore, clinically available devices are generally trileaflet, unlike the native bileaflet MV. This study assesses the tissue mechanics and the organ-level function of bileaflet MV with CA and identifies the most effective number and locations of chordae tendineae (CT). The evaluation also includes a comparative analysis of a flat annulus vs. a saddle shape, aiming to investigate the impact of biomimetic approaches.
Methods: A 2D flat annulus (model-1) and a 3D saddle-shaped annulus (model-2) were analyzed.Each model was evaluated with different CA designs including: CT=2,6,8, with a length=80,100,120% of the physiological one. The position of the CT anchoring points was varied (edge vs. center). The FEA was performed using Abaqus and a Yeoh model was used for the leaflet’s behavior. Quantitative metrics for the assessment included: stress-strain distribution, Geometric Orifice Area and Bending Deformation.
Results: Statistically significant differences in stress-strain distribution were detected between the models with CT=2 and those with CT=6,8. The configuration with CT=2 showed a visible bulge effect.The configurations with edge leaflet anchoring showed better closure of the valve than the center one.
Conclusions: This study demonstrated that, consistently with the general biomimetic paradigm: A) 2 CT do not provide sufficient stability to the valve; B) in the commissural zone and in the areas surrounding the CT insertions were identified highest levels of stress; C) the native-like 3D configuration in Model-2 showed more homogeneous stress distribution.