
Abstract
Objectives:
The goal of the prospective study was to understand changes in pain and function among patients with knee or hip osteoarthritis (OA) in an integrative pain center. Little is known about how integrative health treatments interact with mainstream medical treatments for knee or hip osteoarthritis. Our clinical case series describes the outcomes of 42 patients diagnosed with knee or hip osteoarthritis who were assessed in the Comprehensive Pain Center at Oregon Health & Science University from July 2020 to July 2022 during the onset of the COVID-19 pandemic.
Methods:
Most patient visits shifted to virtual appointments due to COVID-19. As part of usual care during COVID-19, patients received virtual visits with pain providers and health psychologists. In addition, in-person visits for acupuncture, chiropractic, massage, and Rolfing were available. Patient-reported outcomes were collected via phone and stored in REDCap Cloud prior to visits. A multipronged data-gathering approach was implemented with REDCap Cloud, including questionnaires obtained over the telephone and in person with iPads using a QR code for participant identification.
Results:
There were 34 females and 8 males with a median age of 63.1 (range: 34–78) with an average of 11 clinic visits. Their initial PROMIS Global physical mean score was 33.9, and mental was 38.7. At 12 months, mean outcomes were improved among 17 patients who provided follow-up data on the Hip Dysfunction and Osteoarthritis Outcome Score, Knee Dysfunction and Osteoarthritis Outcome Score, and Brief Pain Inventory.
Conclusions:
With patient care shifted to virtual appointments, data collection was challenging. Although one cannot infer causality from a case series, some patients seeking integrative care for osteoarthritis trended towards improved outcomes despite difficulties due to widespread treatment disruption with COVID-19.
Introduction
Patients with osteoarthritis (OA) of the knee and hip often present as complex patients with multiple pain diagnoses and symptoms. 1 This population often has elevated levels of functional impairment, as well as sleep disruption, depression, and anxiety. 2 As such, they often require more medical visits, provider types, and a higher degree of coordination. 3 This case series was compiled as part of a quality improvement (QI) project that sought to elucidate how integrative health treatments interact with and may be synergistic with medication and other mainstream medical treatments for osteoarthritis of the knee and hip. QI projects involve systematic, data-guided activities designed to improve delivery of health care at the local level, rather than through testing the efficacy of particular interventions, such as in clinical trials. 4
The project was a collaboration between the Comprehensive Pain Center (CPC), an integrative medicine pain clinic at Oregon Health & Science University (OHSU) in Portland, OR and the Pfizer Field Medical Outcomes and Analytics team headquartered in New York, NY. The CPC is a distinctive pain center that provides a broad range of integrative medicine treatments within an academic medical health care system. In addition to allopathic medicine (e.g., interventional pain management), treatments include acupuncture, chiropractic care, dietary and nutritional guidance, massage, cognitive behavioral therapy, mindfulness, naturopathic care, and Rolfing. Patients seen within the CPC usually receive care from multiple types of providers within the context of a whole-person approach to their pain management. 5
This QI project was focused on understanding how patients navigate these multiple types of treatments to provide a means of hypothesis generation for future research on the referral pathways and characteristics of patients who may be better suited to a whole health approach. However, as we initiated this project, our plans were dramatically altered by the onset of the COVID-19 pandemic. This report describes the patient-reported data outcomes of the project; a separate commentary article describes our team’s process of navigating through multiple COVID-19-related challenges to complete the project. 4
Methods
Patients with osteoarthritis were identified through the electronic medical record as potential participants. Those that had a treatment scheduled in the CPC from July 2020 to July 2022 were contacted, and baseline patient reported outcomes (PRO) were obtained and stored in REDCap Cloud (nPhase, Inc., Encinitas, CA; https://www.redcapcloud.com/). Standard of care was provided throughout this time period. Due to COVID-19-related changes in treatment patterns and safety precautions (shifting to virtual visits for medical doctors and psychologists, plus interruptions for acupuncture, chiropractic, massage, and Rolfing), the PRO tools could not be handed to patients prior to visits. A multipronged approach to PRO data gathering was implemented with REDCap Cloud, including questionnaires obtained over the telephone and in person with iPads. iPads utilized a QR code for participant identification.
Health outcomes
The PRO tools included the Hip Dysfunction and Osteoarthritis Outcome Score (HOOS), 6 a score ranging from 0 to 100, with 0 indicating the worst possible hip symptoms and 100 indicating no hip symptoms; the Knee Dysfunction and Osteoarthritis Outcome Score (KOOS), 7 a 0% to 100% score, with 0 representing extreme problems and 100 representing no problems; the Brief Pain Inventory (BPI), 8 a scale that measures both overall pain and pain interference; and PROMIS Global 10 to assess physical, mental, and social health, with higher scores reflecting better health. 9 The PROs were gathered by the project assistant at return visits for 1 year.
Data collection
Data were collected by the project assistant in advance of the patient’s scheduled visit. Patients had access to virtual visits with pain providers (physiatry- and anesthesiology-trained) and health psychologists. In addition, in-person visits for acupuncture, chiropractic, massage, and Rolfing were available. The project was intended to start in the spring of 2020, but due to the onset of the COVID-19 pandemic and the changing nature of treatment patterns, data collection did not start until May 2021. The OHSU Institutional Review Board (IRB) determined that the project did not need IRB oversite due to its QI nature (07/30/2020, study ID 00021916).
Statistical analysis
All summarized data are presented as mean ± SD. Stata/MP 16.1 for Mac (Intel 64-bit) Revision 11 Oct 2022, Copyright 1985-2019 StataCorp LLC) was used for statistical analysis. As this is a case series and preliminary in nature, hypothesis testing is inappropriate and was not conducted.
Results
By May 2021, the treatment patterns were different than before the onset of COVID-19. Patients were no longer seeing physicians or health psychologists in person and many patients were reluctant to commit to in-person visits required by the integrative medicine modalities. In addition, as all procedure-based pain care was halted, many of these patients reported higher than normal pain levels.
From May 2021 to June 2022, 42 patients with a diagnosis of osteoarthritis were included and provided baseline data. The primary site of pain for these patients was the hips (n = 14) or knees (n = 16), with the remaining patients having the most pain in their hands (n = 7), feet (n = 2), neck (n = 2), or low back (n = 1). Most had multiple body areas with pain (n = 36, 86%). The population was primarily female (81%), non-Hispanic (98%), and Caucasian (96%). Patients averaged 11 visits (range: 1–49) within our pain clinic during the year following their initial visit. They also averaged 3.2 diagnoses per visit (Table 1). Among participants in the study, patients saw at least two types of providers, with acupuncture the most frequent type of provider (6.2 visits), followed by chiropractic (3.1 visits) and massage (1.9 visits). At baseline, the population had elevated levels of both pain (mean = 5.6, SD = 1.9) and pain interference (mean = 6.4, SD = 2.5) and were highly impacted as reflected in their Global PROMIS scores (mental mean = 39.4, SD = 6.6; physical mean = 33.8, SD = 8.2). At 12 months, 17 patients provided some form of follow-up data on the HOOS, KOOS, and BPI PRO measures. As shown in Table 2, mean outcomes for these measures were improved in the portion of our sample that provided follow-up data.
Patient Demographics
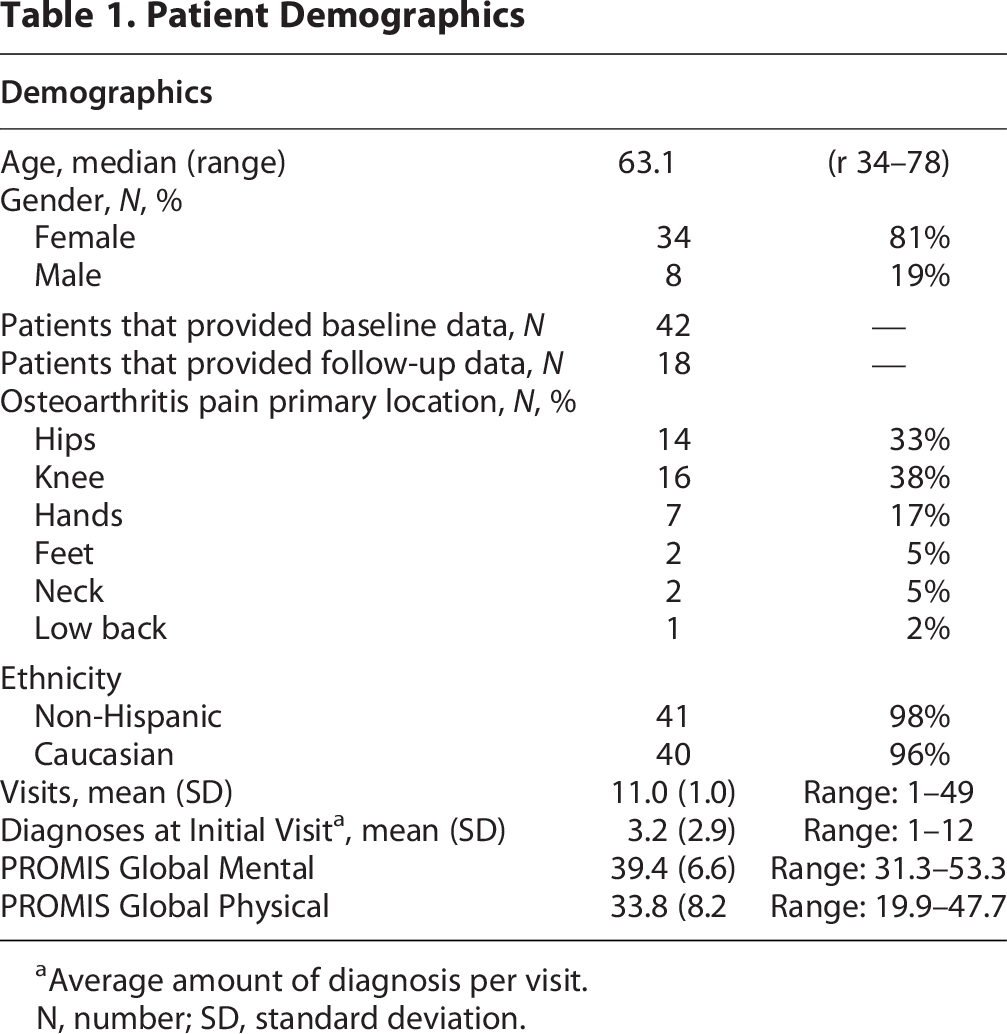
Average amount of diagnosis per visit.
N, number; SD, standard deviation.
Hip Disability and Osteoarthritis Outcome Score (HOOS), Knee Injury and Osteoarthritis Outcome Score (KOOS), and Brief Pain Inventory (BPI) Outcomes

For patients with multiple follow-ups, only the last follow-up is reported.
BPI, brief pain inventory; HOOS, hip disability and osteoarthritis outcome score; KOOS; knee injury and osteoarthritis outcome score; N, number; pt, patients; QOL, Quality of life; SD, standard deviation.
Discussion
This clinical case series reports on a sample of patients with osteoarthritis of the knee or hip who sought treatment in a large integrative medicine pain clinic during the COVID-19 pandemic. As with most research efforts initiated during COVID-19, this QI project was greatly reshaped by sudden changes in patient pathways through the health care system. Comparative literature is very limited, which highlights the unique nature of this study.
While circumstances changed dramatically during the course of this QI project, we observed that among this population of patients who are generally high utilizers of health care, mean outcomes were improved in the portion of our sample that provided follow-up PRO measurements. This is notable given that, consistent with other COVID-19 era studies, overall pain levels rose within our clinic following the onset of COVID-19. 10 Multiple factors likely contributed to this overall increase in pain, including increased isolation, depression, and anxiety in the general population. However, given the small numbers of patients participating in this QI project and the high attrition rate we encountered in attempting to obtain follow-up data, it is important to not overinterpret these findings.
Most of these patients had seen multiple provider types (e.g., primary care providers, neurologists, and rheumatologists) prior to arriving at the CPC clinic. As such, this population tends to present with more complex symptomatology, including higher amounts of disability than is seen in most clinics. During this pandemic period, most medical visits shifted to virtual visits except for manual therapies (chiropractic, massage, Rolfing, and acupuncture.) For many of these patients, these visits were the only in-person contact that they had within the medical arena. In general, it was seen that depression, anxiety, and pain scores all increased with the onset of COVID-19.11–14 In contrast, the portion of our sample that provided follow-up data had both stable pain scores and improved functional scores. This suggests that these patients viewed the integrative medicine component of their treatment regimen as especially valuable, in that they were willing to risk medical encounters and possible virus exposure during a time when patients as well as providers had little information about the overall risks of the disease. Patients regularly conveyed to the study coordinator that they were deeply appreciative of the care they received at the pain center. It was a regular occurrence for patients to describe the care provided by acupuncturists and massage therapy providers as having a very positive impact on their ability to complete daily activities.
Challenges and limitations
There are several notable limitations to this study that greatly restrict interpretation of our data results.
First, during COVID-19 we had no choice other than to drastically revise data collection methods during both telehealth visits and in-person visits, yet the implications of these revisions in terms of patient selection effects in the midst of a major worldwide pandemic are largely unknown.[cite in press paper] Second, again due to COVID-19, the sample size—especially in those providing follow-up data—is too small to draw any reliable conclusions. Third, as this was primarily a QI project, it did not include a control arm. Fourth, our primarily female Caucasian patient sample lacked diversity, rending generalizability moot. Lastly, it is possible that those patients who continued to receive treatments and provide follow-up data during the initial stages of COVID-19 might represent a distinct subgroup of patients with characteristics different than those in the full sample.
Despite these shortcomings, our case series does indicate several promising possibilities that could be more rigorously investigated in future studies. In particular, future studies might include an efficacy study to determine the ideal pathways—that is, what combinations of integrative and allopathic therapies, and in which sequence—are most likely to result in the best combination of symptom improvements. In addition, a more pragmatic trial could be implemented with pain clinics that do not currently have offer these integrative therapies, to elucidate ideal utilization pathways, ideal patients for these treatments, and cost differences in health care.
Conclusion
While SARS-CoV-2 (COVID-19) created significant barriers to health care, multiple patients in this case series seeking integrative medicine options for the treatment of osteoarthritis of the knee or hips had improvements in function and pain based on validated PRO measures. Due to COVID-19, most patient care visits shifted to virtual appointments, making data collection very challenging. Our case series suggests that integrative care should be further investigated as a treatment option for patients with osteoarthritis.
Authors’ Contributions
S.D.M.:—author, revisions, statistics, and final approval. J.W.C.:—author, revisions, and final approval. K.M.:—author, revisions, and final approval. S.F.:—author, revisions, and final approval.
Footnotes
Acknowledgments
The abstract of this report was previously published in: Glob Adv Health Med. 2022 May 2;11:2164957X221096590. doi: 10.1177/2164957X221096590
The authors would like to thank the team at Pfizer Inc. for supporting this project and their flexibility as all health care made this sudden shift in treatment patterns due to the COVID-19 pandemic.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project was sponsored by Pfizer Inc. S.D.M., J.C., and K.M. are employees of OHSU, who were paid consultants to Pfizer Inc. in connection with the execution of this study. Although all authors made conscious efforts to execute their study roles free of any bias, it is possible that unconscious bias did influence their work.
Research Ethics
The project was conducted in accordance with the Code of Ethics of the World Medical Association. The Oregon Health & Science University Institutional Review Board gave oversite to the project.
Informed Consent
All participants in the study gave informed consent.