
Abstract
This is a visual representation of the abstract.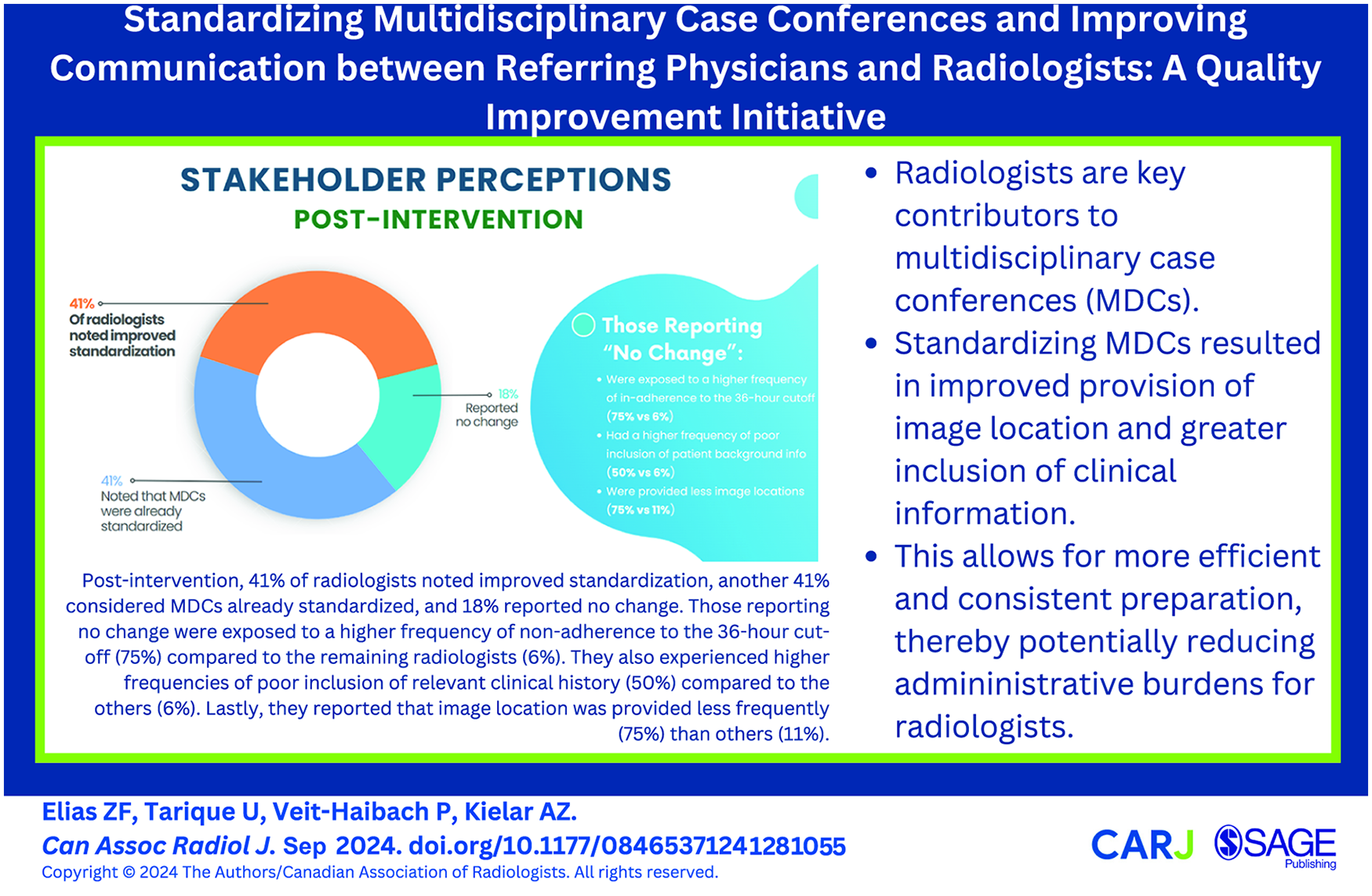
Introduction
In multidisciplinary case conferences (MDCs), radiologists play a pivotal role in affecting treatment decisions for patients with diverse oncologic conditions. A meta-analysis of 12 676 imaging studies found that secondary interpretations at MDC were discrepant from the original in one-third of cases, management-altering in one-fifth of cases, and more accurate in 90% of cases. Abdominal scans showed a particularly high discrepancy rate. 1 While Cancer Care Ontario (CCO) mandates various case conferences for oncologic treatment decisions, 2 radiologists at several institutions, including our own, actively contribute to MDCs beyond just malignancies; encompassing conditions such as Crohn’s disease and endometriosis. Currently, the clinical information provided to abdominal radiologists in their preparation for MDCs varies across clinical groups and lacks standardization.
While evidence for the benefits of standard forms in MDCs is limited, standardization in other radiology contexts is well-documented. Structured reporting templates reduce variability, minimize diagnostic errors, and improve communication with referring physicians. 3 Additionally, classification systems such as LI-RADS (Liver Reporting and Data Systems) have effectively standardized liver imaging techniques, interpretation, and reporting with the goal of improving communication within and between medical disciplines.4,5
To establish a more cohesive approach, we created a quality improvement (QI) project with the aim of examining the clinical information provided to our abdominal radiologists prior to MDCs, and identify best practices related to appropriate information inclusion. Moreover, we aimed to assist radiologists in managing their MDC workloads and to enhance overall efficiency. The ultimate objective involves creating a standardized and comprehensive system integrating Epic (Health Management System). This would facilitate documentation of MDC decisions, and empower radiologists to effectively and efficiently prepare for MDC discussions, subsequently enhancing the standards of patient care.
Materials and Methods
Research Ethics Board (REB) exemption for QI projects was obtained through the institutional Quality Improvement Review Committee. This project was conducted following SQUIRE 2.0 guidelines. 6 We identified 28 subspecialty MDCs where abdominal subspecialist radiologists from our tertiary centre academic hospital department are recurrent participants. Physicians from the pathology department were additionally consulted on the design of the survey as well as the MDC template, as they are key stakeholders who frequently participate in MDCs. An anonymous electronic internal survey, aligned with stakeholder preferences, CCO guidelines, 2 and literature findings7,8 was administered to staff abdominal radiologists who participate in one or more MDC. Survey data was collected with SurveyMonkey software, which was accessed via a password-protected departmental account (Survey in Supplemental Appendix A). The survey consisted of questions pertaining to the radiologists’ professional background/demographics, followed by open-ended questions, and Likert-scale assessments to gauge stakeholder opinions and preferences.
Adhering to the Plan-Do-Study-Act (PDSA) protocol, 9 and informed by results from the information acquired from our literature findings and survey, we developed a standardized excel template based on committee decision. This template incorporated all information pertinent to radiology/pathology to be inputted by requesting physicians in preparation for MDCs. We circulated the new templates accompanied by a rationale via E-mail, and invited questions and commentary from MDC managers and participating physicians. After commentary, the updated template was circulated to the department and discussed at divisional meetings for consensus. There were no specific areas of disagreement in the group after the presentation and discussion.
After 1.5 and 8 months, we assessed template adherence, as well as completeness of the requested information. As part of this project, we requested that cases be ready for review by radiologists 36 hours prior to the MDCs. We also communicated the need for physicians submitting cases to attend the subsequent MDC, and if unable to, designate a delegate familiar with the case to avoid repetition of work for the radiologists at later meetings.
In the final phase of the PDSA cycle, we sent a follow-up survey 4 months post-implementation of the new MDC standards to delegate radiologists who participated in multiple meetings. This was done with the aim of determining if the MDC standardization has met radiologists’ expectations to improve efficiency and safety of case preparation.
Results
We surveyed abdominal radiologists in a single tertiary care hospital system who participate in one or more of the 28 MDCs, many of which occur weekly (Table 1). Baseline response rate was 27/32 (84%). Each radiologist participated in a range of 1 to 6 MDCs and each MDC had between 2 and 6 radiologists who are on a rotating roster. Forty-seven survey responses were collected (range 0-5 responses for each MDC, with at least 1 response for MDCs that occur on a weekly basis). Given the limitations in sampling data for each individual MDC, results were analyzed both on an individual MDC basis and collectively for all MDCs.
List of Multidisciplinary Case Conferences in Which Abdominal Radiologists Participate at Our Institution.
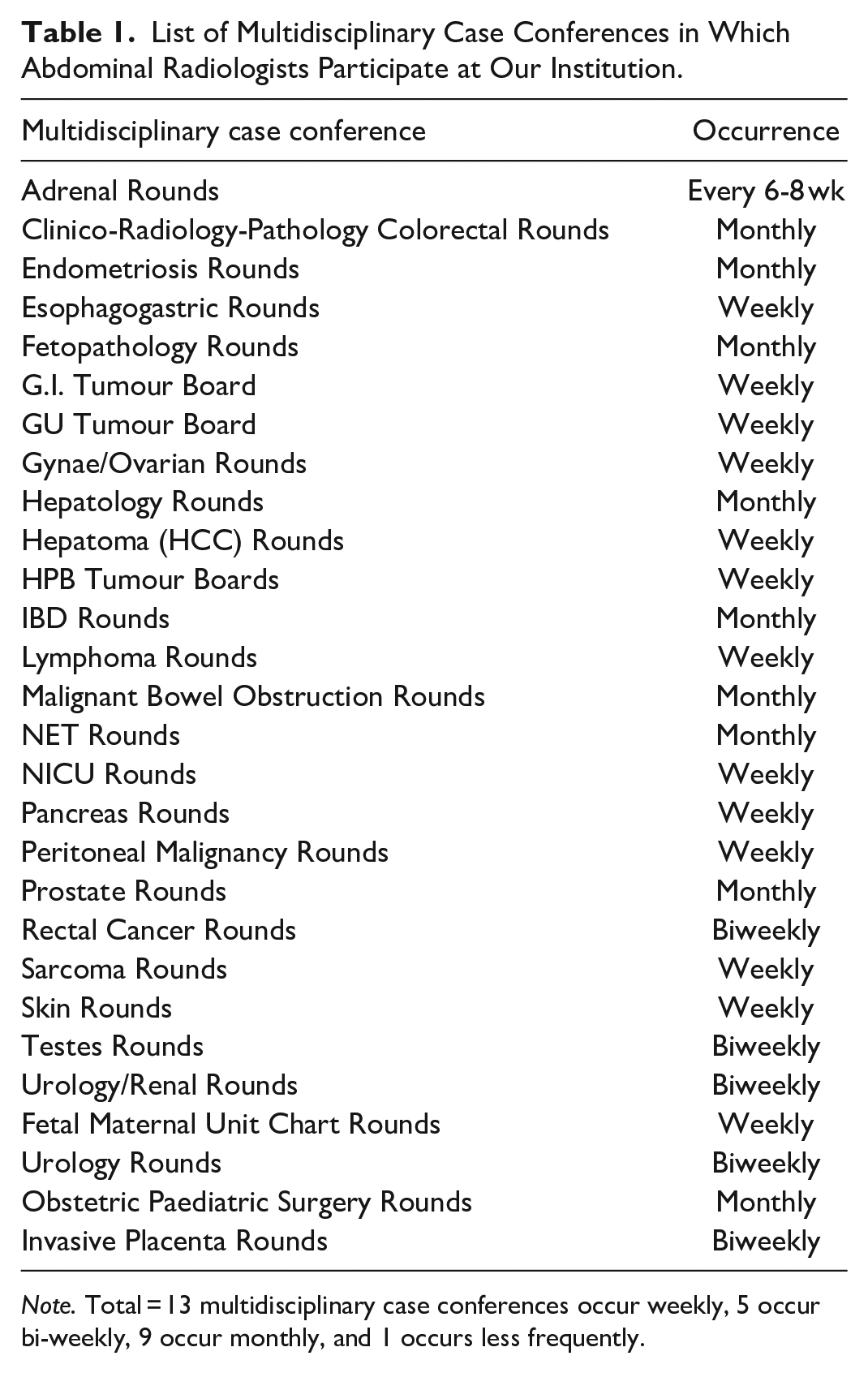
Note. Total = 13 multidisciplinary case conferences occur weekly, 5 occur bi-weekly, 9 occur monthly, and 1 occurs less frequently.
Radiologist responders have participated in MDCs for 1 to 5 years in 51% of responses (24/47) and for longer than 20 years in 26% of cases (12/47), representing with the diverse career stages of the radiologists. Time spent on MDC preparation weekly ranged from 0.5 to 7 hours (average 2.8 hours/week across all MDC), with the most time for preparation work spent on Hepatoma (HCC) Rounds (average 5.3 hours/week). The amount of time spent on post-MDC work ranged from 0 to 60 minutes (average 38 minutes), with formal dictations for outside imaging consultations accounting for this time. The majority had no protected time for rounds (42/47, 89%), with protected time provided solely for Hepatoma (HCC) rounds. 51% of MDCs regularly discussed 6 to 10 patients’ cases (24/47) and 28% discussed 11 to 15 cases (13/47; Figure 1). 53% of the radiologists thought that there was no maximum number of cases to be discussed in MDC, and of the MDCs with a maximum number of cases discussed, Hepatoma (HCC) MDC had the highest number of cases (average 22 cases). In the case of Hepato-Pancreato-Biliary (HPB) rounds, the multidisciplinary team has maintained a maximum of 12 cases per MDC this year.
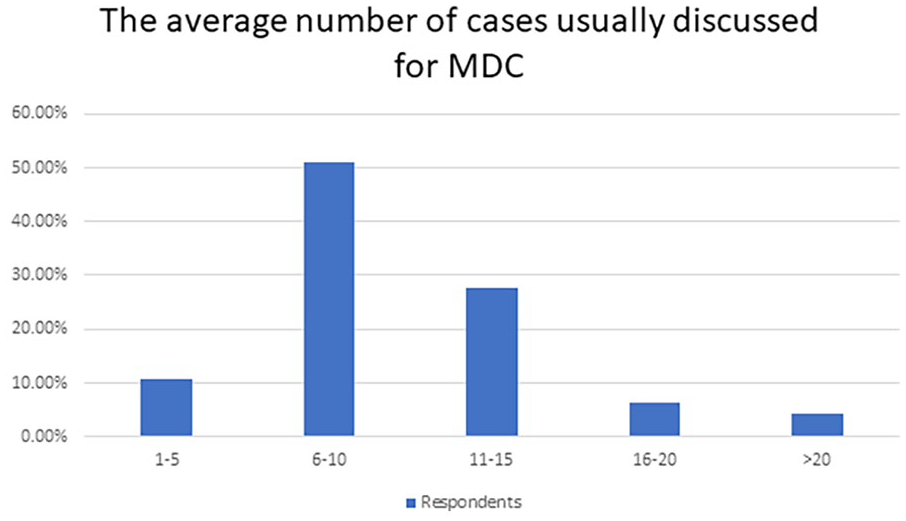
The average number of cases usually discussed across all MDC.
The majority of radiologists completing the first survey either agreed or strongly agreed that clear guidelines existed on how to list patients for MDC discussion (29/43, 67%). However, approximately 44% of radiologists (19/43) felt neutral/disagreed that there are clear guidelines on what clinical information to provide for radiologists preparing for MDC. The vast majority of radiologists agreed/strongly agreed that discussion around patients in MDC are conducted professionally and in an organized manner (43/47, 91%). Although most radiologists felt that there is adequate time to satisfactorily discuss patients during MDC (35/47, 74%), approximately 15% of the respondents (7/47) indicated there was not adequate time, noting that there would occasionally be a few cases being postponed to subsequent week for another radiologist to review (Figure 2). This typically occurred in MDCs with high-volume caseloads (ie, HCC and Pancreas MDC).
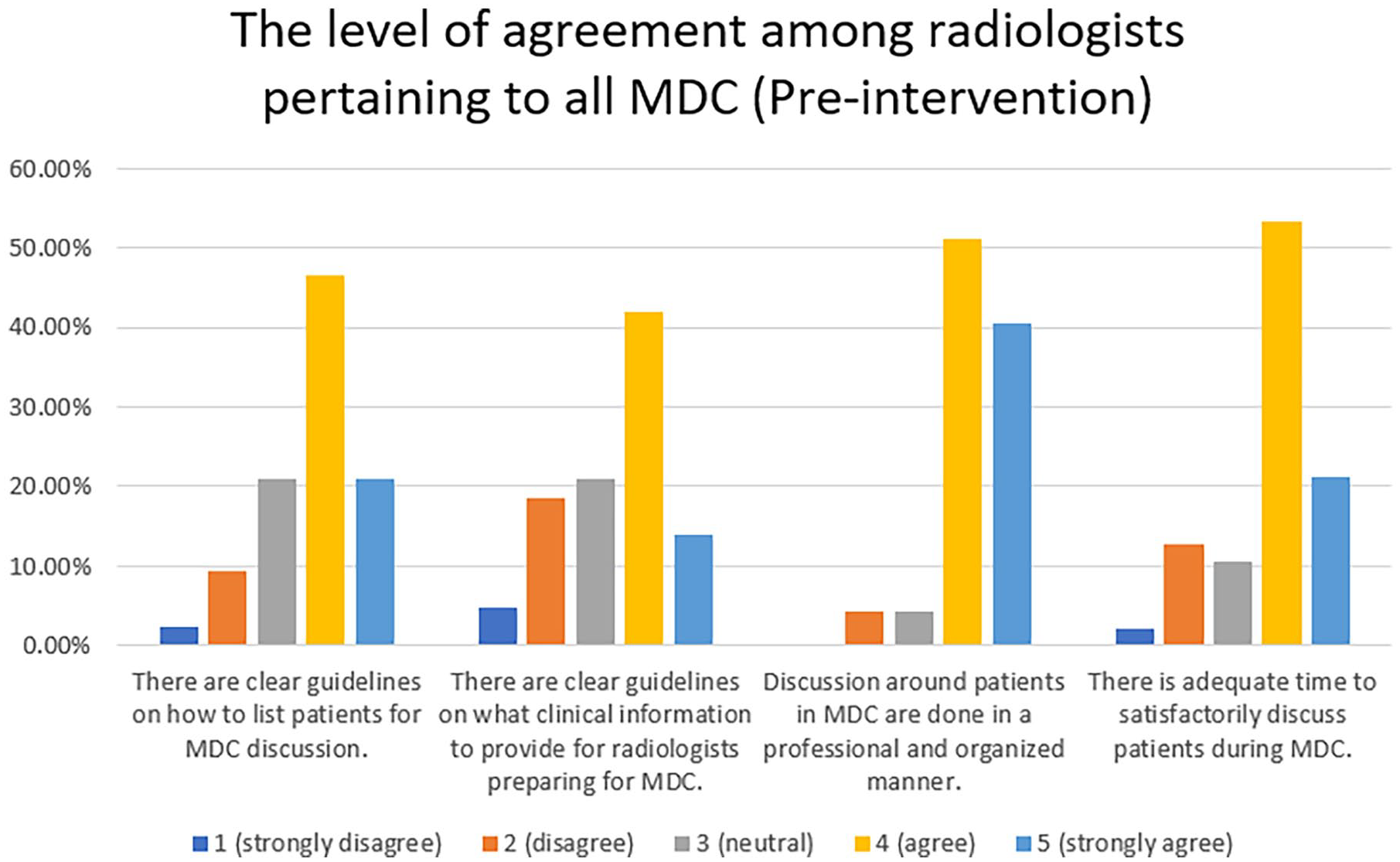
The level of agreement among radiologists pertaining to all MDC.
Many radiologists felt neutral or disagreed that they were always reviewing finalized radiology reports prior to MDC discussion (20/46, 43%), indicating that very recent imaging was being discussed at MDC before a finalized radiology report could be created. At our institution, we do not always provide finalized outpatient reports on the same day the images are acquired due to workforce issues and surges in patient scheduling. Radiologists also felt neutral/disagreed that concordance between the original radiology report and the MDC findings is common (16/47, 34%), a finding consistent with the meta-analysis by Rosenkrantz et al. 1 Most radiologists preparing for MDC preferred for every radiology report to follow a standardized template (31/47, 66%) or felt neutral toward template use (11/47, 23%). 100% of responders felt that their role adds value to the MDC discussion (47/47; Figure 3).
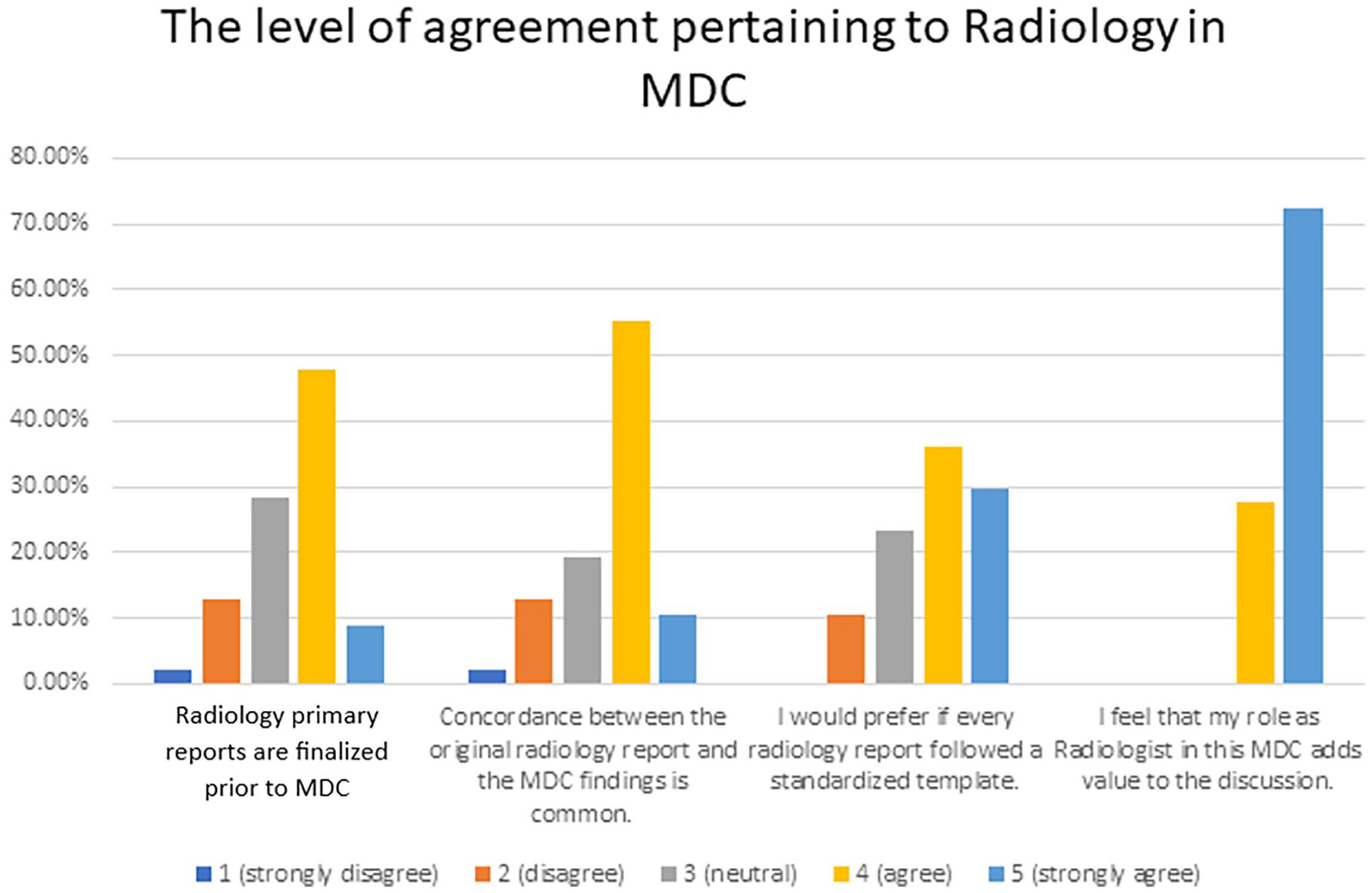
The level of agreement pertaining to Radiology in MDC.
In the initial MDC format, the majority of radiologists agreed/strongly agreed that virtual invites are received for every MDC (45/47, 96%), MDC is easy to join (44/47, 94%), and the virtual platform utilized (eg, Zoom) is reliable with minimal technical issues (45/47, 96%). Most radiologists preferred the virtual format (29/47, 62%) or hybrid virtual/in-person format (13/47, 28%) of MDC. In the current virtual format, radiologists felt that the ability to make a decision has increased somewhat or significantly (32/47, 68%) and learning opportunity has increased somewhat or significantly (32/46, 70%).
Regarding logistics, 57% of radiologists strongly disagreed that uploading remote imaging to our academic university hospital servers is easy (26/46). The opinions on dictating consults on remote images uploaded to hospital servers being easy were mixed, with 34% of radiologists disagreeing/strongly disagreeing (16/47) and 32% agreeing/strongly agreeing (15/47). Notably, around 22% of MDC cases are reviewed and discussed using ConnectingOntario.
Concerning the clinical information provided for MDCs, the patient’s name, medical record number, and age are consistently provided often/always (45/47, 96%). However, information pertaining to the location of images (internal Picture Archiving and Communication System [PACS], vs external, eg, ConnectingOntario) is rarely/never provided (16/47, 34%) or sometimes provided (14/47, 30%). Patient background and relevant clinical history is often (18/47, 38%) or always (10/47, 21%) provided, however about 15% of the respondents (7/47) felt that background clinical history is rarely/never provided. The specific question to answer at rounds is often/always provided in 60% of cases (28/47, 60%), with some radiologists noting that it is only “sometimes” (11/47, 23%) or “rarely/never” (8/47, 17%) provided (Figure 4). Notably, the lack of guidelines on a clear clinical question at MDC was highlighted as an area of improvement to consider when establishing guidelines on what clinical information to provide for radiologists preparing for MDC. Radiologists noted that a cut-off of 36 hours for add-on cases was rarely/never (16/45, 36%) or sometimes (12/45, 27%) followed.
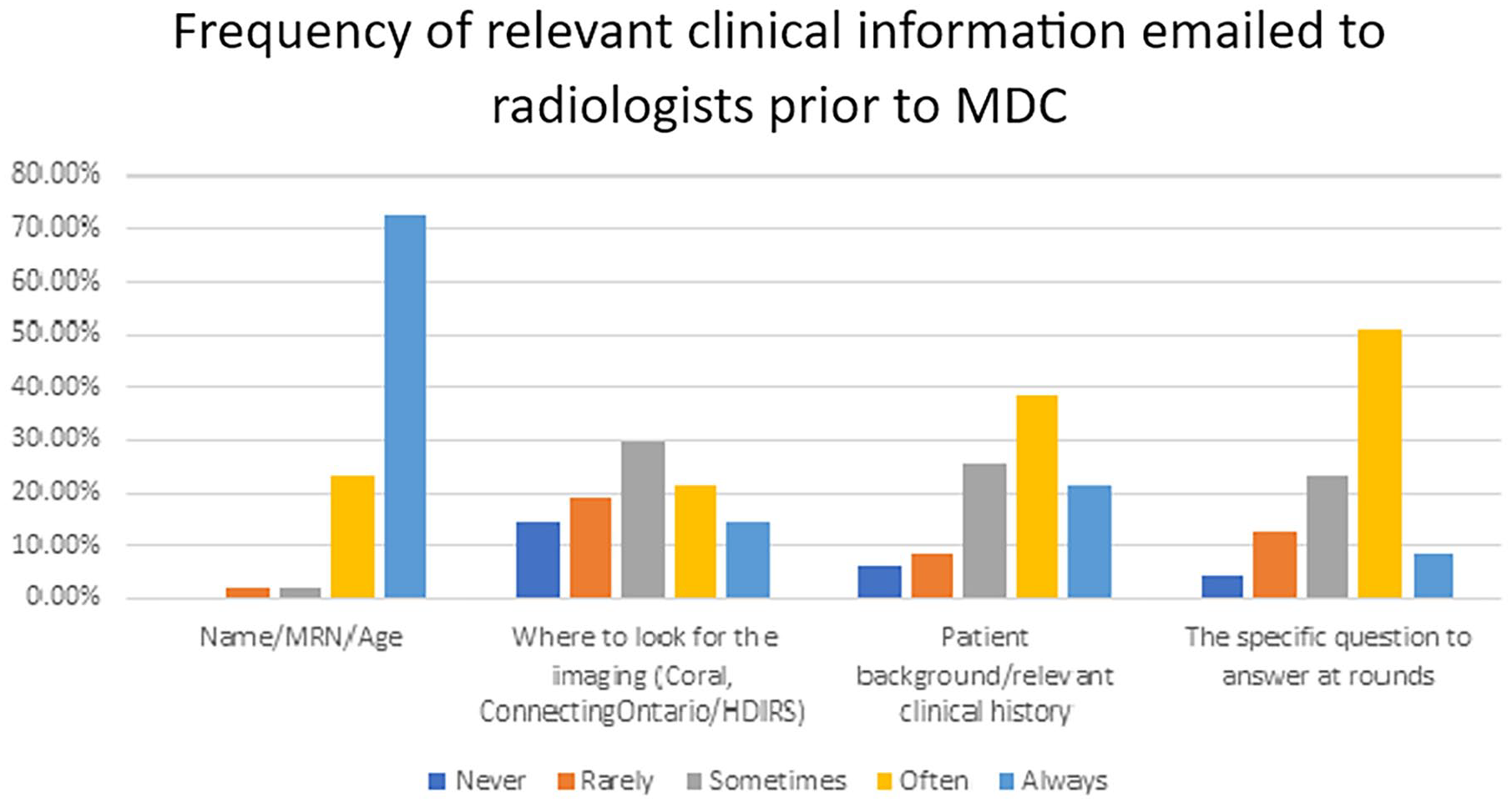
Frequency of relevant clinical information provided in preparation for MDC.
Several changes to help prepare MDC more effectively were identified. Notably, accessing/uploading external images to institutionally-developed PACS (Coral inc.), timely provision of the list of patients for review with no last-minute add-ons, protected time for preparation for longer caseloads, and setting a maximum manageable number of patients for review. Additionally, ensuring attendance of clinicians or their delegates was also noted as an area of improvement to minimize delays. However, some radiologists acknowledged that last-minute cases may be accepted if clinically relevant for decision-making and a cut-off of 36 hours may not be always possible. In the year before this project, the multidisciplinary team at HPB rounds had been successful in having a maximum of 12 cases discussed, ensuring that the patient’s date of birth is included (helpful for locating a patient’s file on ConnectingOntario), and the staff or a delegate was always present at MDCs.
According to the internal survey, the top 5 MDC aspects considered most important by radiologists are: (1) compiled clinical information enabling accurate treatment recommendations, (2) a multidisciplinary lens for evaluating clinical problems, (3) increased patient safety, (4) promotion of adherence to clinical guidelines, and (5) strengthening teamwork (Figure 5). Learning about treatment options and the clinical perspective were also noted as additional values of MDC. Additionally, the majority (79%, 37/47) felt that it would be valuable to have clinical fellows present at MDCs, anticipating a valuable learning experience and contribution. Figure 6 represents the final standardized MDC template to be used across all current and future MDCs for which our institution’s abdominal radiologists provide services. Within 1.5 month of sharing this, 24 of 28 (86%) MDCs had adopted the standard MDC template. This improved to 25 of 28 (89%) by 8 months. The 3 outliers are all MDCs related to a particular surgical specialty, organized by the same administrative assistant. One of these 3 MDCs only involves 2 radiologists, only takes place once a month, includes a very specific patient group, and has the same clinical question during each meeting.
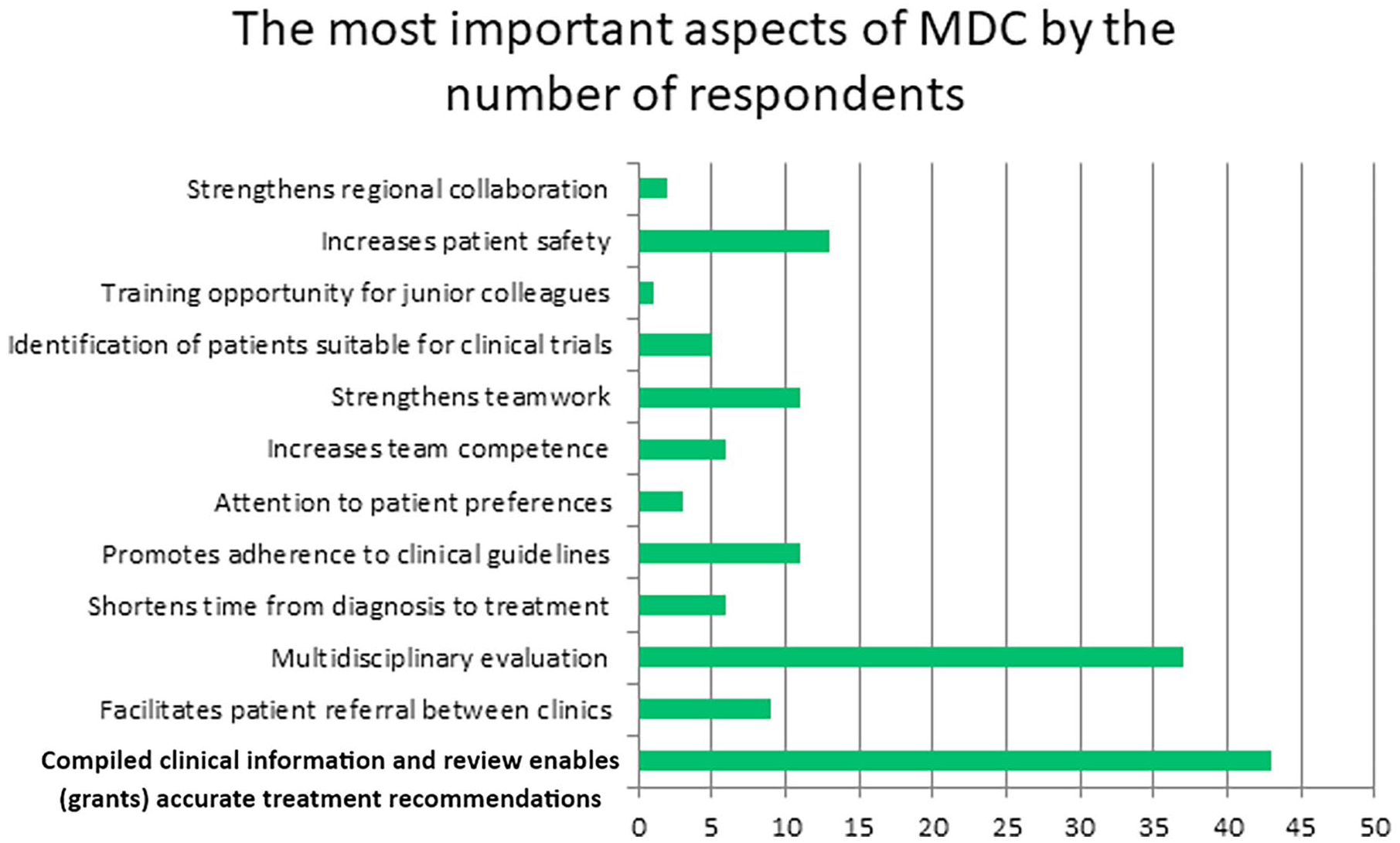
The most important aspects of MDC by the number of respondents.
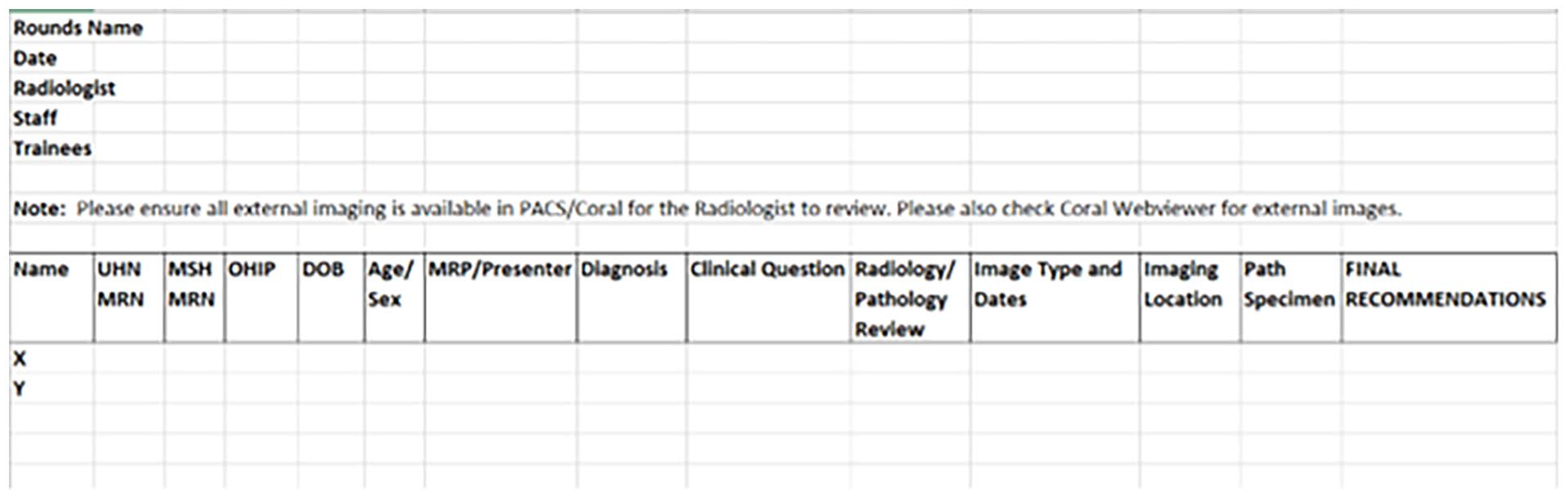
Final standardized MDC template.
The follow-up survey at 4 months was given to radiologists attending each of the weekly MDCs, such that one answer per MDC was available. Twenty-three responses from 12 radiologists were gathered “Often/always” being provided the image’s location improved to 70% (16/23) from a 36% (17/47) baseline. Adherence to the 36-hour cut-off improved, as radiologists rated them as “rarely/never” followed in 17% (4/23) of follow-up cases, compared to 36% (16/45) at baseline. It is expected that the 36-hour cutoff will not be adhered to in urgent cases or when clinically relevant for decision making. Lastly, 78% (18/23) disagreed that uploading remote imaging to hospital servers is easy, representing a 6% increase from baseline (33/46, 72%). Uploading images from external sources is controlled by the hospital information technology (IT) department, and is therefore outside the purview of our radiologists. It represents an objective that we aim to address in future initiatives.
When asked to assess their perceptions on the effect of the intervention, 41% (9/22) of radiologists noted improved standardization with some remaining inconsistencies, another 41% (9/22) considered MDCs to already be standardized and not requiring further changes, and 18% (4/22) reported no change, with remaining inconsistencies. Regardless of perception level, the majority of radiologists disagreed or strongly disagreed that uploading remote images to hospital servers is easy: 6/9 (67%) of those voting improved standardization; 7/9 (78%) of those voting that MDCs were already standardized; and 3/4 (75%) of those voting no change.
A subset analysis to further examine the radiologists who reported perceiving no changes post-standardization revealed: exposure to a higher frequency of non-adherence to the 36-hour cut-off (3/4, 75%) compared to the remaining radiologists (1/18, 6%). Furthermore, they experienced higher frequencies of poor inclusion of patient background information and relevant clinical history (2/4, 50%) compared to the other radiologists (1/18, 6%). Lastly, they reported less frequent “often/always” ratings for image location being provided (3/4, 75%) than others (2/18, 11%). The aforementioned survey statistics aligned with qualitative comments entered by the responding radiologists through SurveyMonkey.
When examining the effect of the addition of radiology fellows to the MDC presentations (which had started several months earlier), most (16/23, 70%) reported that no fellow was assigned to their particular MDC. The remaining responders were nearly evenly split between reporting a decrease in their workload (3/23, 13%), and no change in workload (4/23, 17%). None of the radiologists reported that their workload increased. Comments entered by radiologists explained increased efficiency with fellows helping with dictation of outside imaging consults, as well as positive changes especially in MDCs involving complex imaging and multi-systemic disease, such as skin/melanoma rounds.
Discussion
Radiologists actively participate in MDCs, addressing conditions involving both malignancies and benign conditions, such as endometriosis. The complex nature of the patients presented underscores the need for standardization, ensuring complete history, adequate preparation time, and adequate information to retrieve imaging. Multidisciplinary care leads to improved treatment recommendations based on most up to date guidelines as well as improve communication among healthcare providers.10-13 Our QI project evaluated the effect of standardizing clinical information presented to radiologists in preparation for MDCs.
Our project revealed that radiologists felt neutral or disagreed that reviewing finalized radiology reports is always completed prior to MDC discussion (20/46, 43%). This suggests the necessity for protected time, or ensuring patient imaging is performed and interpreted earlier with regards to the timing of MDC, which may be related to person-power issues. Radiologists suggested a common pattern of desired areas of improvements: listing of patients within a reasonable timeframe (36 hours prior to MDC), presence of delegates to discuss the patient’s history and details of their current care, as well as information technology methods to upload external images more efficiently. Four-months after dissemination of the standardized MDC forms, a 34% improvement in provision of the image’s location was observed from baseline. Adherence to the 36-hour cut-off improved from 17% to 36%. Overall, 18% (4/22) of radiologists reported no improvement following the intervention. Of those 18%, a higher frequency was exposed to non-adherence of the 36-hour cut-off compared to the remaining radiologists (75% vs 6%). A higher frequency of radiologist experienced poor inclusion of patient background information (50% vs 6%), and less frequent provision of image location (75% vs 11%) compared to the remaining radiologists. Compliance to the standardization was high, as 25/28 (89%) of MDC groups adhered to it by the 8-month follow-up.
Although few clinical fellows were available for the timeframe of the project, incorporating them to present at MDCs was established as a valuable addition that may reduce workload. Their addition was also encouraged as a valuable learning opportunity to review and discuss complex cases and to be exposed to the relevant treatment plans.
Based on results of our internal survey, consultation with our pathologist colleagues, as well as review of CCO and other current literature, we propose the following standardized system integrating electronic patient records (Epic) to allow radiologists to effectively and efficiently prepare for MDCs and provide the best possible patient care:
Patient background/relevant clinical history and clear clinical/imaging question to be answered.
Uploading external images to institutional PACS (Coral-JDMI Informatics) and/or dictating consults on external scans.
Official radiology report available for review for patients with imaging at our institution.
Protected time for preparation, with the amount of time adjusted to reflect the average amount of time required for each MDC.
Manageable maximum number of cases for review as decided by the multidisciplinary team for each MDC and ensuring adequate time allotted for each case.
Timely list of patients for review including a cut-off of 36 hours prior to MDC for add-on cases, with occasional exceptions made for urgent cases that are clinically relevant for timely decision-making.
Ensuring attendance of clinicians or their delegates when their patients are to be reviewed.
Our project highlighted the substantial time invested by radiologists for MDC preparation, where time spent on MDC preparation weekly ranged from 0.5 to 7 hours (average 2.8 hours/week across all MDC). Furthermore, the majority of radiologists reported no protected time for MDC preparation (42/47, 89%). Recent findings by Stratchko et al revealed that a total of 4458 hours were devoted annually to MDCs at their institution. 14 This was equivalent to 1.9 FTE, or $1 155 152 in unreimbursed radiology departmental costs. These findings emphasize the need for improved efficient use of radiologist time, which was a major objective of our intervention. Radiologists often utilize clinical, academic, or personal time to prepare for MDCs. Such patterns warrant potential advocacy initiatives to explore reimbursements for radiologists participating in MDCs, as well as research exploring the effect of the inefficiencies of MDCs on burnout, and loss of academic or clinical productivity.
This study has several limitations. The survey design, which included Likert-scale and open-ended questions, may be prone to interpretation bias. The 8-month follow-up may not fully capture the long-term impact and adherence to the intervention. Our sample size of 27 radiologists, solely from the abdominal division, and from a single tertiary care hospital, may not be representative of broader radiologist viewpoints, however it is a stepping stone for larger standardization opportunities in the future. Tailoring to a single EMR (EPIC) may limit generalizability; given that no universal EMR exists, we chose the most widely implemented EMR. EPIC handles at least two-thirds of all electronic patient files in North America, with about half of these patients being Canadian. 15 Finally, the exclusion of other specialties from the survey could be another limitation, though pathologists, who are the other specialty that regularly present information related to these multidisciplinary case conferences, were included in the design of the project.
To our knowledge, this was the first QI intervention focusing on MDC efficiency and effectiveness. The aforementioned promising findings help set the stage for further progress. Such progress may be in the form of integration of standardized requisitions within Epic. This would allow for a record of final group decisions, creating a repository specific to each patient that would streamline future reviews. Epic integration may also allow for force functions, which would ensure that cases are requested within a reasonable timeframe before the MDC, guarantee the inclusion of sufficient information on patients’ clinical backgrounds, and maintain a reasonable maximum number of cases. Automation and large language models dedicated to radiology may also play a role in retrieving imaging from external sources such as ConnectingOntario.
Conclusions
Radiologists are key contributors to MDCs, which are crucial in the management of complex patient cases and have been shown to enhance communication and clinical decision-making. Standardizing MDCs resulted in improved provision of image location and greater inclusion of clinical information. This allows for more efficient and consistent preparation, thereby potentially reducing administrative burdens for radiologists. Future initiatives may address artificial intelligence integration and protected time for MDC preparation.
Supplemental Material
sj-docx-1-caj-10.1177_08465371241281055 – Supplemental material for Standardizing Multidisciplinary Case Conferences and Improving Communication Between Referring Physicians and Radiologists: A Quality Improvement Initiative
Supplemental material, sj-docx-1-caj-10.1177_08465371241281055 for Standardizing Multidisciplinary Case Conferences and Improving Communication Between Referring Physicians and Radiologists: A Quality Improvement Initiative by Zeyad Elias, Usman Tarique, Patrick Veit-Haibach and Ania Z. Kielar in Canadian Association of Radiologists Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ania Z. Kielar is the President of The Canadian Association of Radiologists.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.