
Abstract
Objectives:
This study aims to compare primary care providers and medical assistants in degrees of comfort, confidence, and consistency when addressing behavioral health concerns with patients before and after the implementation of a model of integrated behavioral health in primary care (IBHPC), and evaluate whether these perceptions differ based on increased access to behavioral health clinicians.
Methods:
This longitudinal study was conducted at 2 primary care clinics in Northern California while implementing an IBHPC model. The Integrated Behavioral Health Staff Perceptions Survey was administered to assess the comfort, confidence, and consistency of behavioral health practices. Confidential online surveys were distributed to primary care faculty and staff members before and post-implementation. Responses from providers and medical assistants were compared between pre- and post-implementation with linear regression analyses. The relationships between accessibility to behavioral health clinicians and a change in comfort, confidence, and consistency of behavioral health practices were explored using a linear mixed-effects model.
Results:
A total of 35 providers and medical assistants completed the survey both before and post-implementation of IBHPC. Over time, there were increasingly positive perceptions about the consistency of behavioral health screening (P = .03) and overall confidence in addressing behavioral health concerns (P = .005). Comfort in addressing behavioral health concerns did not significantly change for either providers or staff over time. Medical assistants were initially more confident and comfortable addressing behavioral health concerns than providers, but providers’ attitudes increased post-IBHPC implementation. Improved access to behavioral health clinicians was associated with greater consistency of screening and referral to specialty mental health care (P < .001).
Conclusion:
The present study is the first to explore differences in provider and medical assistant perceptions during the course of an IBHPC implementation. Findings underscore the importance of integrating medical assistants, along with providers, into all phases of the implementation process.
Keywords
Introduction
Patients with behavioral health concerns are typically first identified in primary care settings.1,2 In fact, nearly 70% of all primary care visits are directly or indirectly related to psychiatric or psychosomatic problems. 3 Primary care providers prescribe 79% of all antidepressant medications and provide mental health care for 60% of people treated for depression in the United States. 4 Increasingly, providers are addressing other behavioral health concerns, such as substance use and dependence, with little support from subspecialists. If left untreated, behavioral health conditions exacerbate physical health outcomes in primary care, result in higher healthcare costs and increase the clinical care burden on providers. Despite their high prevalence, behavioral health diagnoses are often underrecognized and undertreated in primary care, suggesting a need for more effective identification and management. 5
In response, primary care has adopted various integrated behavioral health models, which combine medical and behavioral health care within the same setting.6,7 Integrated behavioral health in primary care (IBHPC) is one such model, designed to increase the identification and treatment of behavioral health conditions, including mental health and substance use problems. The vision for this model is to provide behavioral health and medical care at the same location in a fully integrated system with a seamless array of patient-centered services. 6 Primary care providers and behavioral health professionals work as a team and are actively involved in co-managing patient care. 6 IBHPC models have been found to increase service utilization, lower costs, enhance treatment outcomes and patient engagement, and elevate satisfaction among clinic staff and patients.5,8-10
Despite the effectiveness of integrated models addressing behavioral health concerns, there are inherent challenges. 11 In integrated clinics, all staff members assume critical roles by working collaboratively to manage care for patients with behavioral health conditions.12,13 Thus, effective implementation relies on the willingness of primary care team members to reshape their practice patterns, collaborate with behavioral health specialists, and prioritize behavioral health as an essential service. 14
Integrated services are highly valued among staff in primary care settings once programs are implemented.12,15-18 Yet, compared to data on the primary care provider experience with IBHPC, little is known about the perspectives of medical assistants. Medical assistants are at the frontline of patient care and, therefore, IBHPC implementation.15,17-20 In the few studies conducted, medical assistants reported higher comfort levels responding to behavioral health concerns than providers. Regardless of role, clinic members with more exposure to behavioral health clinicians (psychiatrists, social workers) tended to have more positive attitudes toward IBHPC.12,18 Even fewer studies have explored broader perceptions of IBHPC beyond satisfaction, such as confidence, comfort, and consistency in addressing behavioral health concerns.12,14 Finally, studies to date have only collected data post-IBHPC implementation, lacking a baseline to compare team member perceptions over time.12,14,15,17,21
The present study is the first to evaluate provider and medical assistant perceptions of behavioral health practices before and after the implementation of IBHPC. This study aims to: (1) compare providers’ and medical assistants’ comfort, confidence, and consistency in addressing behavioral health concerns during the implementation of IBHPC at two clinics in Northern California; and (2) evaluate whether increased access to behavioral health clinicians is associated with improved perceptions of IBHPC practices. This evaluation of perceptions between providers and medical assistants can help inform future implementations of IBHPC, particularly incorporating all patient care team members in the implementation process.
Methods
Design
This longitudinal study was conducted with clinic staff at two primary care clinics in Northern California. The study sites, a family medicine practice and an internal medicine practice, are housed in the same building. The clinics have a combined panel size of 27 988 patients with an estimated 1015 patient visits weekly.
Clinic staff members with direct patient care responsibilities were eligible for participation, including medical assistants, nurses, physician assistants, nurse practitioners, and physicians. This study compared medical assistants with direct medical providers, including nurse practitioners, physician assistants, and physicians.
Procedures
Data were collected before (March 2019) and at post-implementation (December 2020) of a model of IBHPC in both clinics. The confidential and online surveys were distributed to 65 clinic team members before and 128 after implementation across the two participating clinics, asking about their experience caring for patients with behavioral health concerns. Individuals in leadership positions, such as Medical Directors, distributed these emails to employees to increase the likelihood of participation.
At the first data collection in March 2019, behavioral health service offerings were limited and served as a baseline for data collection (Table 1). Clinics had launched a limited educational campaign around the importance of depression screening using a paper-based system. Several behavioral health initiatives were implemented at the second data collection point in December 2020. By the second timepoint these clinics were partially integrated.23,24 A social worker had started working at the internal medicine clinic while offering support to the family medicine clinic. The social worker was trained to actively provide brief evidence-based clinical interventions and help with community resource linkage. These interventions were documented in the clinical records and communications with providers. Since these clinics were housed in the same building, the social worker was readily available for consultation at both clinics.
Availability of key elements of a model of integrated behavioral health in primary care in both the Internal Medicine and Family Medicine clinics before (March, 2019) and after (December, 2020).
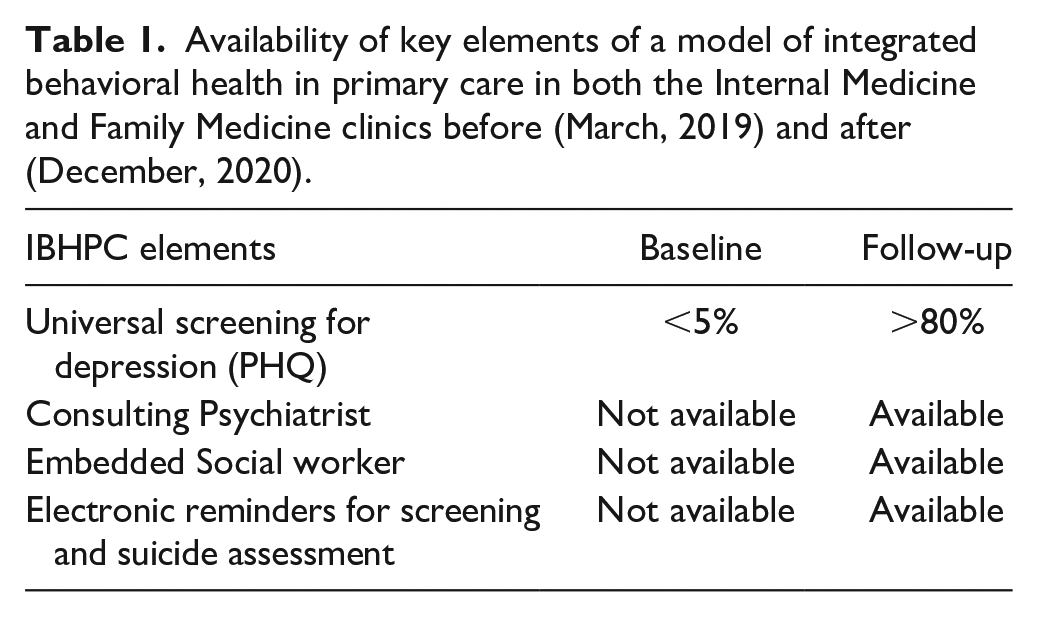
Additionally, electronic reminders for screening and suicide assessment were implemented in the electronic medical record, an evidence-based clinical decision-making algorithm was created for primary care providers, and electronic consultation from a psychiatrist was available. In addition, a consulting psychiatrist was available to primary care providers via electronic health record communication, phone, text, and co-visits. Co-management was established at the second timepoint between the social worker, the consulting psychiatrist, and the primary care providers. All social workers were available for urgent consults. Providers were the focus for IBHPC information and training, but limited team-based training was made available at the program’s launch.
This study was approved by the Stanford University School of Medicine Institutional Review Board. A waiver of consent was obtained before the distribution of the survey. No identifiable information was collected from participants, and no monetary compensation was provided for participation.
Measures
The Integrated Behavioral Health Staff Perceptions Survey is an instrument developed in a previous study to assess comfort and knowledge around behavioral health and substance use with excellent response rate and interpretability. 22 The survey was constructed by the authors of this study with input and feedback from organizational leadership and care providers and is available from the senior author (MM) upon request. The survey comprises 28 items across 7 domains: (1) confidence in addressing behavioral health concerns; (2) comfort in caring for patients with behavioral health needs; (3) percentage of time spent addressing behavioral health concerns; (4) actions and tools employed to address behavioral health needs; (5) consistency of care; (6) access to behavioral health care; and (7) burden in caring for patients with behavioral health concerns. In total, 16 items from the measure were used for this report focused on the confidence in the clinic’s ability to care for patients’ behavioral health needs, the comfort of managing care for patients with behavioral health needs, consistency of care, and access for staff to behavioral health providers. These items were measured on a Likert scale from Strongly Disagree to Strongly Agree, and considered continuous for this analysis. Additional self-reported demographic information was collected, including clinic and role type. Time was operationalized as the time point of data collection: t = 1 refers to data collected in March 2019 (pre-implementation), and t = 2 refers to December 2020 (post-implementation).
Statistical Analysis
All analyses were performed using STATA Version 17. Descriptive statistics were used to summarize the respondent characteristics using cross-tabulations and frequency distributions. Providers, such as physicians and nurse practitioners, were compared to medical assistants for all analyses.
T-tests were used to assess the difference in the mean score of comfort, confidence, and consistency in treating behavioral health problems before and after implementation. Additionally, a linear regression model was fitted to understand how the perceptions of providers and medical assistants changed before and post-implementation of the IBHPC model. The change in score was computed by subtracting the value of confidence, comfort, and consistency items at Time 1 from the value at Time 2.
Finally, a linear mixed-effects model was fitted to assess the relationship between access to behavioral health clinicians and a change in comfort, confidence, and consistency while implementing IBHPC, comparing providers and staff. Interaction terms were included between staff role and access to behavioral health clinicians, and access to behavioral health clinicians and time. Random effects were included on the clinic and participant level, with a random intercept for access to behavioral health clinicians. Robust standard errors were included to address the heteroskedasticity of the model.
Results
Descriptive Characteristics
In total, 35 participants from two different primary care clinics in California completed the survey at both time points. At pre-implementation, 59 out of 65 respondents participated (91%), while at post-implementation, 82% of those invited participated (105/128). A majority of participants were physicians (n = 19; 54%), followed by medical assistants (n = 14; 40%) and two nurses or nurse practitioners (6%). Eighteen respondents worked in the Internal Medicine clinic, and 17 participants from the Family Medicine clinic (Table 1).
Main Findings
Figure 1 displays the mean difference on the survey items before and post-implementation of IBHPC, stratified by staff role. Between before and post-implementation, there was a significant increase in confidence in identifying behavioral health needs (P = .04), providing good care for behavioral health concerns (P = .005), addressing needs for patients with chronic conditions (P = .009), and consistency of behavioral health screening (P = .003). Comfort around addressing substance use or mental health concerns remained stagnant for providers and staff before and after implementing IBHPC.

The change in confidence, comfort, and consistency of addressing behavioral health concerns before and post-implementation of Integrated Behavioral Health in Primary Care practices, stratified by providers and staff (n = 35).
In the linear regressions, there was evidence to suggest a greater overall increase across all items for providers than for medical assistants before and after-implementation of IBHPC (Figure 1). Medical assistants had a higher mean score on all items at Time 1 than providers. Providers’ perceptions across all items increased more than for medical assistants during IBHPC implementation. Specifically, providers had more of an increase in perceptions on the items of confidence in providing good behavioral health care (β: 0.95; 95% CI: 0.17-1.73; P = .02), consistency of behavioral health screening (β: 1.17; 95% CI: 0.31-2.03; P = .01), consistency of managing behavioral health needs for patients with chronic conditions (β: 0.81; 95% CI: 0.09-1.52; P = .03), and consistency of access to a social worker (β: 0.78; 95% CI: 0.03-1.53; P = .04).
The linear mixed-effects models showed an association between the accessibility to behavioral health clinicians for staff and the outcomes of confidence, comfort in addressing mental health and substance use, and consistency of behavioral health practices in the clinic at Time 1 (Table 2). For every unit increase in perceptions of access to behavioral health clinicians, there was approximately half a unit increase in confidence around identifying and providing good care for patients with behavioral health needs and referring patients to specialists (P < .01). Comfort addressing mental health and substance use only slightly increased due to increased access to behavioral health clinicians (P < .05). Perceived consistency of behavioral health practices also increased due to an increase in accessibility to behavioral health clinicians for staff (P < .001).
Linear Mixed-Effects Model of the Associations Between Access to Behavioral Health Clinicians for Staff and Outcome Variables (n = 35).

Coefficient estimates were derived from a linear mixed effects model on the association between access to behavioral health clinicians for staff and survey items about confidence, comfort, and consistency of providing behavioral health services. The main effect is the coefficient for the association between behavioral health clinician access and the outcomes at Time 1. The interaction term displays the change in the relationship between the access to behavioral health clinicians and the outcomes between Time 1 and 2. A model with a random intercept for behavioral health access and random effects on the participant and clinic level was used.
P < .05. **P < .01. ***P < .001.
The relationship between accessibility to a behavioral health clinician and several of the outcomes was stronger before than after the implementation of IBHPC, including confidence in referring patients to specialists, consistency of behavioral health screening, addressing behavioral health needs for patients with chronic conditions, and connecting patients to a behavioral health specialist (P < .001). Stratified by staff role, there was a significant difference between providers and staff in the relationship between access to behavioral health clinicians for staff items on the consistency of behavioral health practices in the clinic. The strength of the association was lower for providers compared to staff for consistency of behavioral health screening, behavioral health counseling, and addressing behavioral health needs for patients with chronic conditions (P < .01).
Discussion
Summary of Findings
This study describes the perceptions of providers and medical assistants during the early phases of IBHPC implementation in two primary care clinics within an academic medical center. The results suggest that clinics are progressing toward integration, demonstrated by increased confidence and consistency in delivering behavioral health services. Provider and staff comfort levels around addressing behavioral health concerns did not improve despite IBHPC implementation. Our findings suggest that within the context of their scope of practice, medical assistants have greater confidence in addressing behavioral health concerns and perceived consistency of behavioral health practices than providers. Increased access to behavioral health clinicians for the team during IBHPC implementation was related to increased confidence in providing care for behavioral health concerns and consistency of behavioral health practices in the clinic, but this relationship attenuated post-implementation.
These differences in perceptions between primary care roles throughout IBHPC implementation could be interpreted in various ways. Providers and staff have different levels of responsibility and scope of practice, which translates into different expectations around patient care. Providers are expected to establish a management plan and follow-up care for patients and may have had more awareness of behavioral health concerns than medical assistants before implementing IBHPC. Along with those practice-level differences, the IBHPC training was designed more for providers, and medical assistants did not have a role in directly referring patients to behavioral health services. Perhaps with more training, the perceptions of medical assistants around IBHPC may improve even more. Still, this study points to a differential impact of an IBHPC implementation by role and discipline.
IBHPC models also vary in the degree of implementation. In these two clinics, the level of integration was primarily at a co-location level.23,24 Providers could still refer and offload care of behavioral health concerns to more readily available specialists without necessarily developing an increased sense of efficacy and comfort in dealing with behavioral health concerns. Behavioral health specialists were not fully integrated into the primary care team. These clinics were in the early stages of implementation and the consistency of the behavioral health screening and identification of mental health disorders increased. Thus, the lack of behavioral health resources may have become more apparent to providers and medical assistants. In advanced IBHPC models, such as the Collaborative Care or IMPACT models, provider and staff efficacy grows through a more fully integrated rather than co-located team-based care approach and case-based learning with the consulting psychiatrist. 5
Limitations
Generalizability may be limited because this study was conducted with two primary care clinics within one healthcare system. At the second time point, surveys were distributed to a broader and larger range of staff. At baseline, surveys were distributed to all physicians but only were sent to a smaller number of representative staff, including medical assistants. The small sample of participants who had completed the survey at both time points may have limited the generalizability of this study. This unintended sampling bias in our study may have foreshadowed our findings that medical assistants need to be included in all phases of an IBHPC implementation process. The survey was constructed for quality improvement and emphasized feasibility over robust psychometric properties. Differences in the interpretation of certain items may have also arisen. For example, the item surveying the accessibility of staff to a behavioral health clinician could imply access to a social worker or consulting psychiatrist. Replications should consider assessing perceptions of behavioral health providers involved in IBHPC and supplement survey results with objective data on service use, referral rates, and treatment outcomes.
Conclusions and Next Steps
This study compared providers’ and medical assistants’ perceptions during the implementation of IBHPC in two clinics in California. Over time and as a consequence of IBHPC, perceptions improved. Some differences did emerge, where medical assistants reported more positive attitudes toward behavioral health practices than providers. Yet, providers experienced a greater change in perceptions due to implementation. These findings suggest that future integration should incorporate all staff and not only providers in IBHPC. Using a population health approach to identify and track patients with behavioral health needs could lead to the inclusion of all team members in training and workflows. Future surveys in these clinics are planned to assess staff perceptions on an ongoing basis. As IBHPC models evolve with increasingly more components and a higher level of integration, the entire healthcare team will take on shared responsibilities for providing robust behavioral healthcare in primary care settings.
Footnotes
Acknowledgements
The authors are grateful for the support of the following people for their contributions to this project, in particular, Sang-ick Chang, Timothy Seay-Morrison, Heather Filipowicz, Megan Mahoney, Baldeep Singh, and Steven Lin. We are appreciative for the participation of staff at the participating clinics.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.