
Abstract
Keywords
Introduction
Integrated health systems, and more recently, Accountable Care Organizations (ACOs), have been praised for their potential to improve quality and reduce costs through better coordination across the inpatient-ambulatory continuum. 1 These twin goals rely heavily on robust interdisciplinary care teams within primary care sites and a sense of “systemness” between the primary care network and the rest of the care continuum. 2 However, even such integrated primary care networks still experience significant variations in quality of care for chronic diseases like diabetes.3,4 These differences allow us to study how factors beyond patient characteristics such as differences in workforce resources among sites can affect diabetes care, particularly in integrated networks that serve urban populations.
The literature supports changes in “diabetes care teams” such as the addition of certified diabetes educators (CDEs) as a powerful quality improvement (QI) intervention in diabetes.5,6 The impact of such a change in workforce within an integrated primary care network is unknown. Montefiore has a fully integrated primary care network serving a diverse urban population and was selected as a Pioneer ACO. This network includes teaching and nonteaching sites and the sites vary in their performance on nationally recognized diabetes outcome measures. Since 2008, Montefiore has begun a transformation into Patient-Centered Medical Homes (PCMHs), including adding CDEs in about half of their primary care sites.
The impact of the addition of CDEs was studied to answer 2 main questions: (1) Is the presence of CDEs associated with higher diabetes performance compared to clinics without their presence? and (2) Does the presence of CDEs impact changes in diabetes performance over time compared to clinics without their presence? Understanding how a workforce QI intervention can impact diabetes care among primary care sites that are heterogeneous, despite belonging to the same system, will help inform integrated systems (and those that are seeking more integration) on the possible utility of deploying similar workforce QI initiatives.
Methods
Setting
Patients at 20 primary care sites within Montefiore Medical Center in the Bronx, New York, were studied. These sites include from 3 to 108 internal and family medicine attendings and housestaff and are located in diverse neighborhoods (incomes below the poverty line range from 3.7% in Eastchester to 36.6% in the South Bronx).7,8 The addition of CDEs was funded by Montefiore’s Care Management Organization, which coordinates the care of and assumes complete risk for a portion of Montefiore’s patients. CDEs were deployed starting in late 2008 with the goal of improved population health for diabetics and reduced costs of complications, as well as to provide needed management and education support to providers in lieu of more difficult to access subspecialists. The patient’s physician at each site decided whether or not to refer to the CDE; about 10% of diabetics are seen by CDEs, many with uncontrolled disease (J. Deluca, Medical Director, personal communication). The addition of CDEs was the first step in a PCMH transformation, which also included a new electronic record. To the authors’ knowledge, there were no other major QI initiatives during the study.
Population
Patients included were ≥18 years old and had diabetes (defined by a diabetes-related ICD-9 code, glycosylated hemoglobin [HbA1c] 6.5% or a diabetes-related problem on their problem list in the electronic medical record). Patients were chosen if they had at least 2 visits in a 1-year period and were excluded if they were known to have died or had a positive quantitative human chorionic gonadotropin (to exclude gestational diabetes).
To determine the impact of the addition of CDEs, patients who met criteria (diabetics seen at least twice in 2009) were selected to allow for at least a year of CDE presence. Only patients who were seen and with lab results in both the 2007 (pre-CDE) and 2009 (post-CDE) time periods were evaluated to study the impact of the addition of CDEs on changes over time.
Outcomes
Data were extracted from a replicate of Montefiore’s Clinical Information System, Clinical Looking Glass. 9 The replicate was queried for each patient who met criteria for the latest laboratory value during calendar year 2008 or 2010, as appropriate. This allowed time for management changes made by providers, including CDEs, to be reflected in the laboratory data. The main outcomes were then dichotomized as follows in accordance with HEDIS 2008 criteria 10 : (1) HbA1c ≤8%, (2) low-density lipoprotein (LDL) ≤100 mg/dL, (3) microalbumin checked, (4) blood pressure ≤130/80 mm Hg (tight control), and (5) blood pressure ≤140/90 mm Hg (lenient control). Unchecked values were considered unmet.
Independent Variables
Site structural and workforce characteristics, such as teaching status and the presence of CDEs were obtained from an online survey of the 20 site medical directors (with a 100% response rate after follow-up with e-mail reminders). Patient characteristics of age, sex, race/ethnicity, payer (commercial, Medicare, Medicaid, or self-pay) were extracted from the Clinical Looking Glass.
In our initial work, we demonstrated a significant association between site-level payer mix and aggregate site-level HbA1c and LDL control (before introduction of CDEs). 11 Also, given the particular structure and resources of the teaching sites (eg discontinuity of care, enhanced Medicaid reimbursement as federally qualified health centers), an attempt was made to reduce confounding by analyzing sites according to teaching status. Based on these findings, sites were divided into 3 categories according to the predominant payer for 60% of their patients (commercial vs government-sponsored such as Medicaid or Medicare, which were labeled “mixed” payer) and the presence or absence of residents. This resulted in 10 commercial/nonteaching sites, 5 sites designated as mixed/teaching, and the remaining 5 sites as mixed/nonteaching. There were no commercial/teaching sites. CDEs were added to 11 sites, equally distributed among all 3 site types (Table 1).
Baseline Characteristics of Commercial, Mixed Payer/Teaching, and Mixed Payer/Nonteaching Clinic Sites.
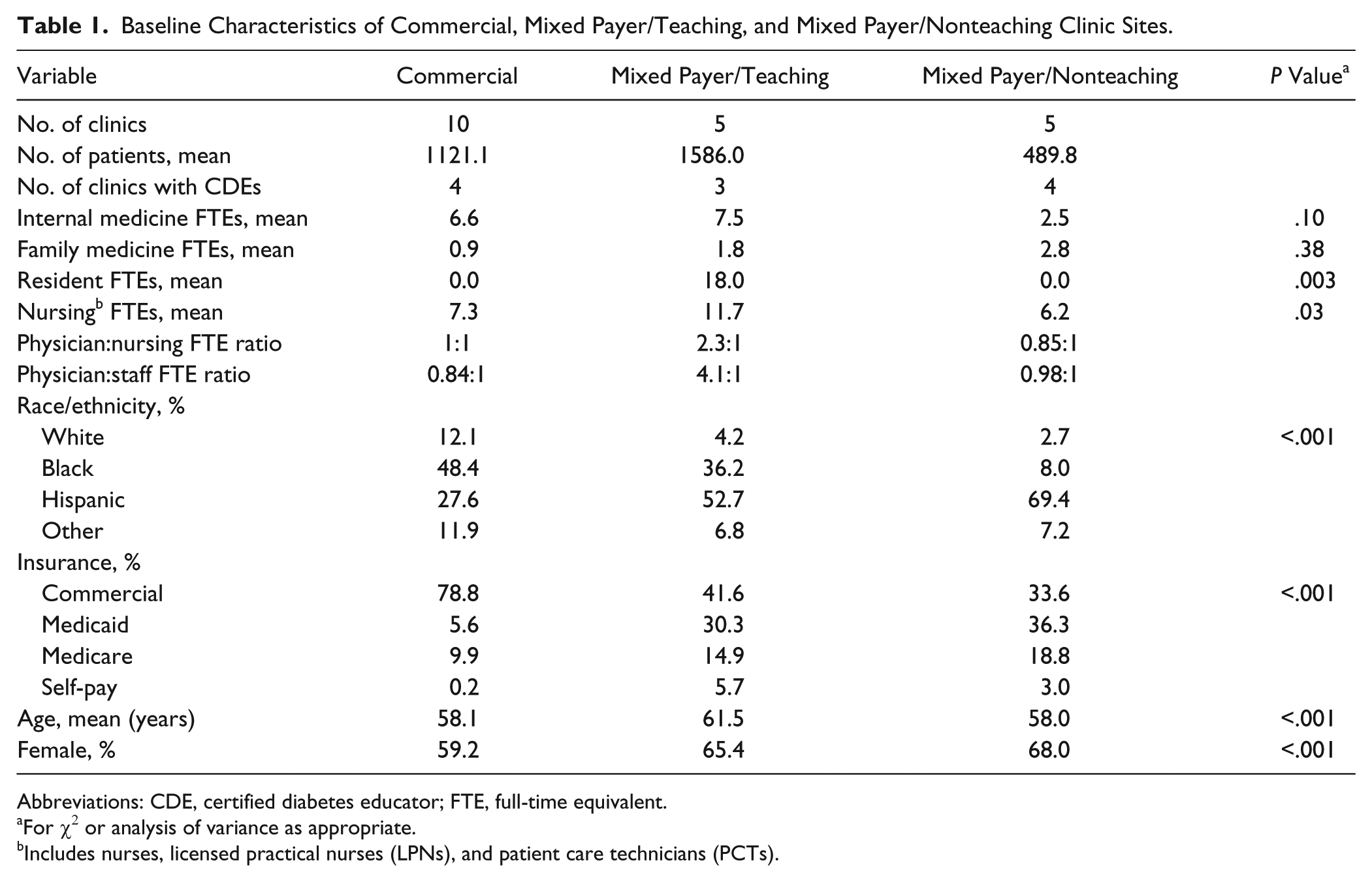
Abbreviations: CDE, certified diabetes educator; FTE, full-time equivalent.
For χ2 or analysis of variance as appropriate.
Includes nurses, licensed practical nurses (LPNs), and patient care technicians (PCTs).
Statistical Analysis
The association between CDEs and each outcome was tested using a 2-level mixed effects logistic regression with site type (eg, commercial/nonteaching) as a random effect. This technique accounts for clustering of patients within sites and within-site variation. Patient-level covariates adjusted for included age, sex, race/ethnicity and payer.
To evaluate change over time with or without CDEs, change over time was defined as site percentage of each outcome met in 2010 minus the 2008 percentage; a change >0 would mean an improvement over time in our analysis. Two-level mixed effects logistic regression was used with site type as a random effect, adjusted for patient-level age, sex, race/ethnicity, and payer in the baseline period.
Results
The baseline study population included 26 225 patients, 13 001 of who were seen and tested before and after CDEs. Site-aggregated age, sex (percentage female patients), race/ethnicity, and payer type were all significantly different between site types (Table 1).
The differences between site type and each outcome were significant (P < .001) after introduction of CDEs (Figure 1). Across all outcomes, commercial sites performed best followed by mixed/teaching sites and finally mixed/nonteaching sites, although no one individual site was consistently the best or the worst performer. After adjustment for patient-level demographics, the diabetes outcomes in sites with CDEs were not better than for sites without CDEs.

Diabetes quality indicators met (%) at mixed payer/nonteaching, mixed payer/teaching, and commercial clinic sites post–certified diabetes educators (CDEs) implementation.
Among patients with lab results in both 2008 and 2010, the presence of CDEs was associated with significant improvements in microalbumin checks and blood pressure control (≤140/90 mm Hg) for commercial/nonteaching and mixed/teaching sites (Figure 2). There was no improvement in the other measures of diabetic quality. Of note, even without including CDEs in the model, commercial/nonteaching and mixed/teaching sites were more likely to improve in their microalbumin checks over this period compared to mixed/nonteaching sites (odds ratio = 1.81 and 1.41, P < .001 for both). Similarly, both site types significantly improved their strict blood pressure control (≤130/80 mm Hg) compared with mixed/nonteaching sites (odds ratio = 1.75 and 1.40, P < .005 for both).

Impact of certified diabetes educator (CDE) on improvement in diabetic quality measures, 2010 versus 2008 (odds ratios [ORs] and 95% confidence interval for improved performance post-CDE versus pre-CDE relative sites without CDEs).
Discussion
We examined a large primary care network within an integrated health system and explored diabetes quality of care before and after the addition of CDEs. We found that although CDEs were not associated with better outcomes in general, they resulted in significant gains in 2 measures of diabetes performance among patients that were treated both before and after CDEs. While this was the case for microalbumin checks and blood pressure control, it was not true for other measures of diabetes performance (HbA1c and LDL control). These post-CDE gains did not ameliorate the variation that already existed within our network, where some sites (commercial/nonteaching and mixed/teaching) are consistently higher performers than mixed/nonteaching sites.
Although CDEs depend on physician referrals and thus do not see all patients with diabetes, it is possible their effect might be broader than the individual patients they see—they may raise awareness of management strategies and influence practice patterns for all patients. This might explain the finding restricted to blood pressure control and microalbumin checks if these measures are not typically on the primary care physician’s “radar” or are more difficult to achieve during traditional physician encounters. The necessary changes in practice patterns seemed to be restricted to patients who were seen throughout the duration of the study.
However, the additional CDEs did not blunt (and perhaps enhanced) the differences among site types that were present at baseline. This might be an example of “fundamental cause theory,” which states that if social capital differences are at the source of differences in outcomes, the addition of resources that do not tackle these fundamental causes can enhance rather than ameliorate disparities because those with higher social capital are better equipped to take advantage of the new resources. 12 Mixed/nonteaching sites might care for the same medically and socially complex patient population as other site types with neither the benefits of teaching sites (eg, continuous education in diabetes care and additional resources through grants or federally qualified health center status) nor the higher social capital of those with commercial insurance. Despite their favorable staffing ratios, diabetes care may still be physician intensive and make the development of new practice patterns through CDEs difficult.
Our findings must be interpreted in light of some limitations. This is an observational study and we cannot ascribe a causal link between CDEs and the observed outcomes. While we adjusted for patient-level factors known to influence diabetes control, it is possible that there are additional patient and site-level trends that affected diabetes control during the study or that the CDEs did not see enough patients to have an impact. By studying changes over time within individual patients, we attempted to account for these potential confounders. Although we are unaware of specific mechanisms, it is possible that other changes such as electronic records could overwhelm or counteract the impact of CDEs. Within the limitations of this QI design where random allocation of CDEs was not feasible, our finding that some outcomes are amenable to impact by CDEs is important when thinking about deploying this highly specialized resource.
While other studies have documented variation in diabetic quality of care in national systems like the Veterans Health Administration, 3 less is known about how variation “reacts” to QI interventions like CDEs. Although centrally managed, our system has important structural heterogeneity (eg, teaching status, size, availability of mental health providers). Our results suggest that CDEs are associated with an improvement in at least some measures of diabetic quality. These resources, however, do not eliminate differences among site types that are fundamental to the identity of these sites (eg, presence of residents and the insurance of the majority of patients) and not easily modifiable without considerable policy and economic changes.
Although many QI initiatives for diabetes in primary care focus on provider and patient behavior, the most effective initiatives seem to be structural such as changes in teams and workforce.5,6 Many primary care settings are attempting to make these structural changes by becoming PCMHs or enhancing integration using models like the ACO. This study adds clarity as to the potential impact of workforce enhancements as QI interventions within an integrated model of care. QI workforce interventions that are effective in one site or in multisite national studies would need to be carefully tailored to achieve similar results in heterogeneous integrated health systems. The factors that modify the impact of these interventions across diverse primary care sites must continue to be studied and modified. Although the promise of system integration is driving policy changes, we must continue to carefully develop and test QI interventions that can promote quality for all patients within a system, particularly in systems that serve vulnerable populations.
Footnotes
Acknowledgements
We are grateful to the faculty of the Division of General Internal Medicine for their feedback, to the Medical Directors for their support and participation, and to Melissa Grigg for her editorial comments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported through the National Institutes of Health’s Loan Repayment Program. Salary support was received from Montefiore Medical Center.