
Abstract
Information about where medicines are in stock and how much they cost facilitates consumers’ timely access to affordable medicines by enabling price comparisons and the identification of stockists. Our aims were to: (1) Review how consumer access to price and availability information is engaged within the Medicine Access discourse and (2) identify factors associated with the existence of interventions that provide consumers with medicine availability and price information. We conducted two scoping reviews. We reviewed 26 medicine access and pharmaceutical system strengthening frameworks to assess how they conceptualise information access. We then reviewed four interventions that provide consumers with availability and price information to identify the factors associated with these interventions’ existence. We found that in the medical access discourse, information is mainly cast as helpful to entities that ensure medicine access for populations. Information as an enabler of medicine procurement for consumers/households is less emphasised. We then identified the following eight factors that facilitate consumer access to reliable medicine price and availability information: the recognition of a medicine access problem that can be mitigated by consumer access to information; cross-sectoral collaboration; the willingness of medicine sellers to disclose their inventory information; having information quality control measures; appropriate incentives for intervention adoption; enabling legal environments; systems of pooling information; and access to digital information technology infrastructure. We recommend that more theoretical and implementation attention ought to be directed at how medicine price and medicine availability information can empower individual consumers to make sound purchasing decisions.
Keywords
Background
Information as an enabler of timely medicine access
The importance of medicines in global health and development is well-established. Concepts and paradigms which have shaped global health discourse and underpinned health and development policy in over 150 countries1–8 all include access to medicines (ATMs) as a critical element.
‘ATM’ is ‘having (medicines) continuously available and affordable at public or private health facilities or drug outlets that are within one hour’s walk of the population.’. 9 ‘Access’ considers the timeliness (1 h) and (continuous) supply, for at least two reasons. First, some medicines’ therapeutic effects depend on timely administration. Second, the continuous adherence to chronic treatment positively affects health outcomes. 10 It is accepted that timely and continuous access to affordable medicines and indeed wider pharmaceutical systems strengthening (PSS), 11 is facilitated by information access. However, a preliminary examination of prominent ATM and PSS frameworks revealed that these frameworks emphasise information as a tool to empower governments and organisations to procure medicines for populations or communities. Less emphasis is placed on information as a decision-making tool for consumers as they search for affordable medicines for themselves along the last mile. (The ‘last mile’ here denotes where the consumer interacts with the point of care such as a community pharmacy. ‘Consumers’ means individuals or households purchasing medicines for their own use). Just as national-level medicine data can obscure important inequities at lower levels of organisation, 12 engaging with ‘information’ as a purely macro-level decision-making tool could potentially obscure micro-level access problems that consumer information could mitigate.
Why information about medicine prices and availability is important for consumers/households
Sustainable Development Target 16.10 13 calls for the guaranteeing of individuals’ access to information as a step towards building more inclusive societies. Information about where particular medicines are in stock and how much they cost facilitates consumers’ timely access to affordable medicines in several ways. First, price information enables consumers to compare costs. 12 Price information provided to prescribers is also associated with lower prescription costs.14,15 Second, information about medicine availability facilitates the swift identification of the pharmacies where these medicines are in stock at the time they are needed. 16 Patients’ lack of real-time information about where specific medicines are available and affordable is one key example of market failure in pharmaceutical systems 17 and a cause of medicines underutilisation. 12 Real-world evidence of the need for information about where to purchase medicines affordably exists. For instance, in Zimbabwe, a Southern African Lower Middle-Income Country, severe medicine shortages18–21 and price variations across pharmacies22,23 make it worthwhile for consumers to compare prices and to find out which pharmacies have particular medicines in stock. Furthermore, Direct-to-Consumer Pharmaceutical Advertising regulations 16 in Zimbabwe prohibit pharmacies from broadcasting details of the prescription medicines they have in stock, or the prices thereof. The pharmacy that has a specific medicine that is in short supply everywhere else, for instance, is prevented from legally broadcasting this fact. Patients or their caregivers, therefore, have to travel from one pharmacy to another enquiring about medicine availability and price at each stop, until they find a pharmacy able to fill their prescription at an affordable price. Door-to-door searches for medicines increase the transaction costs of accessing medicines and undermine the effectiveness of time-sensitive treatments. Moreover, during pandemics that require people to minimise mobility and face-to-face contact (e.g. the novel Coronavirus disease (COVID-19), 24 door-to-door searches potentially place consumers and pharmacy personnel at elevated risks.
As the need exists, it is unsurprising that real-world interventions that provide consumers with information about where certain medicines are in stock and the prices thereof, are emerging through the efforts of private sector, governments, civil society and health professionals–signalling a growing recognition of the need to inform consumers.
The aim and contribution of this article
It has been recognised that medicines information, notably the kind that enables patients to know where to access medicines and the kind that enables them to compare prices, is underprovided.12,17 It has been recommended that this be remedied, especially in low- to middle-income countries (LMICs). 12 Yet, guidance regarding how this can be achieved is still lacking. Given the importance of providing patients with real-time information about where specific medicines are available at an affordable price, this article addresses two research questions:
To what extent is consumers’ access to real-time information about where specific medicines are available at affordable prices, addressed in existing frameworks for ATM and PSS? A scoping review of ATM and PSS frameworks was therefore done and reported in this article, to formally review if and how patient access to information is attended to in the medicine access discourse.
What factors are associated with the establishment and sustainability of interventions that provide individual consumers with information about medicine availability and prices? A scoping review of these interventions was therefore done and reported in this article, to draw out insights into what promoted their emergence and persistence.
We advance the medicines access discourse in two ways. First, we call for the inclusion and more explicit enunciation of consumers’ access to medicine availability and price information within the corpus of ATM frameworks. This is important because frameworks and well-defined constructs, (which tend to be conceived for specific purposes 25 ), orient the attention of global health actors, guide research and policy, communicate priorities and inform interventions.5,11,25,26 What is not included in a framework risks getting overlooked. Second, we propose health system factors that are associated with the provision of medicine price and availability information to individual consumers.
Methods
Study design
Two scoping literature reviews were conducted. The review protocol was not registered with PROSPERO because PROSPERO did not accept scoping review protocols at the time this work was conducted.
Scoping reviews are literature reviews that are appropriate when the goal is to:
explore a nascent or unfamiliar field, or one that comprises diverse literature that is located in diverse domains (e.g. in peer-reviewed journals, grey literature sources and or commercial and media sites),
map a highly populated research area,
uncover research or knowledge or conceptual gaps in a subject area.27,28
The scoping review was considered an appropriate study design for this work because ‘Access to Medicine’ is a highly researched subject and the medicine access literature comprises diverse documents that are located in diverse domains (such as peer-reviewed journals and grey literature produced by inter-governmental, non-governmental or commercial organisations). Preliminary reading had suggested the existence of a gap in the medicine access discourse, that is the under-representation of information as a decision-making tool for consumers as they search for affordable medicines for their own use. Systematically characterising this gap, if it indeed existed, required the scoping review study design. Furthermore, the subject of tools that assist patients with medicine availability and price information, appeared nascent, with some implementation literature located in diverse sources. Mapping this field and identifying relevant literature therefore was also suited to a scoping review.
The first review identified ATM frameworks plus recommendations and guidelines for PSS. This was done to assess the extent to which consumer access to price and availability information is attended to in the ATM discourse. The second scoping review identified interventions that provide individual consumers with price and availability information with the view to infer factors that enable the establishment and persistence of these interventions. The methodological framework for conducting scoping reviews advanced by Arksey and O’Malley 27 and Armstrong et al., 28 and depicted in Figure 1, guided both reviews. This framework spells out that the scoping process involves research question identification, identifying relevant studies, study selection, charting the data, collating, summarising and disseminating the findings, and consultation throughout the process with colleagues and organisations knowledgeable about the subject of the scoping review.

Scoping review steps by Armstrong et al. 28
The section below describes how the scoping review methodological steps for both reviews were executed.
Scoping review 1: review of ATM and PSS frameworks
Identification of research question
The research question for this review was: To what extent is consumers’ access to real-time information about where specific medicines are available at affordable prices, addressed in existing ATM and PSS frameworks? This was considered as an important question to answer in order to gauge the extent to which citizens’ access to on-demand information about medicine availability and price was recognised in ATM and PSS theory.
Literature identification
Frameworks that conceptualise ATM as well as sets of recommendations for PSS were identified over a 4-year period using the following strategies:
In 2017, when the literature search began, Google and Google Scholar searches using the key phrases ‘access to medicines framework’ and ‘pharmaceutical system strengthening’ were first conducted to identify systematic reviews of ‘access to medicines’ and ‘pharmaceutical system strengthening’ frameworks. No filters were applied. Two reviews11,25 were identified as relevant. To avoid unnecessary duplication of search work in academic literature databases, forward and backward citation tracing of these highly cited systematic reviews was done. This iterative process resulted in the identification of 18 relevant unique publications.5,12,17,26,29–42
Using the keywords and phrases ‘Access’, ‘medication use’ and ‘medication management’ ‘transparency’ ‘medicine information’, grey literature was searched for and retrieved from the websites of prominent organisations that work on ATM and PSS. Organisations whose websites were searched were: the World Health Organization (WHO), the United States’ International Development agency, the Access to Medicines Foundation, the World Bank and Management Sciences for Health (MSH). No filters were applied. Four additional unique publications were identified as a result of this strategy.43–46
Relying on alerts from the E-drug listserv (http://lists.healthnet.org/mailman/listinfo/e-drug), a global mailing list subscribed to by one of the authors. This listserv delivers news and notifications of new publications in the area of essential medicines. One unique publication was identified through an E-drug notification. 47
Pursuing leads on potentially relevant authors and publications, based on personal communications from colleagues, also proved useful for identifying published ATM frameworks. These works48–50 were identified this way.
Reference tracing in all included frameworks led to the identification of four additional publications.3,7–9
Literature identification continued until the end of the year 2020.
Study selection and application of inclusion criteria
Table 1 outlines the inclusion and exclusion criteria for the first scoping review (review of ATM and PSS frameworks). The PRISMA Chart (Figure 2) shows the progression from initial publication identification to finalisation of the set of publications reviewed.
Inclusion and exclusion criteria for scoping review 1.

Data extraction and charting of key data elements
Publications which met the inclusion criteria were read iteratively. The sections that referred to the role of information in ATM or PSS were identified and summarised. The findings from this exercise are presented in Table 2 in the Results section. Table 2 in the Results sections also shows the elements extracted from each publication: Author and year of publication, purpose of publication and how that publication frames the role of information in ATM or PSS.
How information is conceptualised/cast in existing ATM and PSS frameworks.


PRISMA chart for scoping review 1 (review of access to medicines (ATM) and pharmaceutical system strengthening (PSS) frameworks).
Data handling and synthesis
The qualitative data charted was inspected for trends in how authors of frameworks conceptualise the role of information in ATM or PSS. Effort was then devoted to finding any mention of the value of price and availability information for patients. Conclusions were then drawn about how authors of frameworks conceptualise the role of information in ATM or PSS. Conclusions were also then drawn about the extent to which attention is paid to patient access to information as a theme.
Scoping review 2: review of interventions that provide individual consumers with information about medicine availability and prices
Identification of research question
We were interested in answering the broad question: What factors are associated with the establishment and sustainability of interventions that provide individual consumers with information about medicine availability and prices?
Literature identification
Medline, Embase, PsycInfo, Global Health CABI, Scopus and ProQuest Dissertations and Theses Global, were searched. Searches were run on 29 December 2020. The search strings used for isolating the literature are attached as Supplemental File 1: Search Strategy for Scoping review 2 and were reviewed by all authors. It was known that the area of medicines availability and price information interventions was one of some implementation activity, despite being relatively under-documented in peer-reviewed journals. Therefore, the search included non-academic literature sources. Searches were conducted on webpages and within data repositories of organisations that have been cited as funders of medication-related information technology projects in developing countries by Konduri et al. 51 and Jahangirian and Taylor. 52 Google and Google Scholar searches of projects identified from grey literature reports and academic articles were performed using the intervention names as search terms. This was to identify information contained in blogs, news articles and on the interventions’ promotional websites. Non-academic literature sources carry a risk of being unreliable. Attempts to mitigate the risk of analysing unreliable accounts were therefore made in the following ways:
The interventions reported in the included non-academic literature sources were also reported in peer-reviewed journal articles or a doctoral academic thesis. Therefore, we could be confident that the intervention existed and were being implemented as the non-academic sources reported.
The non-academic sources included were:
One news article 53 (which was corroborated by several peer-reviewed articles) [e.g. Yuan et al. 54 and Chen 55 ].
One document issued by a for-profit company that is implementing one of the interventions reviewed (this document, which details the intervention’s main elements, was produced to fulfil a statutory requirement. 56 The risk of this document containing unreliable information still existed but was considered minimal).
Two documents issued by the Government of Peru (which is implementing one of the interventions reviewed).57,58
Several documents published by or through the WHO which describe the same intervention that the Peruvian government documents describe.43,44,59
The contents of these non-academic sources were not used to assess or make judgements about the impact or effectiveness of the interventions.
Study selection and application of inclusion criteria
Eligible reports were those that mentioned interventions used to provide consumers with information about where particular medicines or other health products were available and the prices thereof, in countries of any income level. Although the initial plan was to focus only on LMICs, the paucity of reports from this setting justified the expansion of the eligibility criteria. The post hoc finalisation of inclusion criteria can be imperative in the context of a review that scopes an emerging or unfamiliar field. 27 Publications or documents were excluded if they provided insufficient detail about the intervention’s workings, its implementation or establishment. Reports were also excluded if the full-text versions could not be retrieved. Only reports that were in English and Spanish were included. No publication date limits were applied for this second scoping review. All authors reviewed the included interventions. The PRISMA diagram (Figure 3) depicts how the search and selection of reports for this review proceeded.

PRISMA for scoping review of interventions providing consumers with medicine availability and price information.
Data extraction and charting of key data elements
Consistent with the scoping review methodological guidelines,27,28 data extraction and charting to enable the identification of commonalities, gaps and themes, was done. The following elements were extracted and charted on a spreadsheet for each intervention identified:
Intervention description
For each source of information: Author(s), year of publication and type of publication
Country where intervention was implemented
Problem(s) the programme aimed to address/impetus for intervention establishment
Type of organisation involved in implementation
Factors that made the implementation possible and/or sustainable
Data handling and synthesis
An inductive thematic analysis of the data was carried out to illuminate the factors that were common to the interventions in the reviewed sources. During meetings, authors discussed the validity of each theme. A narrative summary of the charted data was then produced.
Results
Summary of findings
Twenty-six ATM frameworks and sets of recommendations for PSS, conceived for different agendas or global health priorities or programmes, were reviewed during the first scoping review. All of them identified different types of information as critical to achieving ATM and rational medicine use globally, at country level or at organisation level. There was however extremely limited engagement with the role of information as an enabler of timely medicine access at household level. Where the subject of medicines information for consumers has been engaged with, the focus has tended to be on how healthcare providers must supply consumers with information about the appropriate use of medicines (after those medicines have been acquired). This finding answered the first research question which was: To what extent is consumers’ access to real-time information about where specific medicines are available at affordable prices, addressed in existing frameworks for ATM and Pharmaceutical Systems Strengthening?
In the second scoping review, four interventions that facilitate consumers’ ATM price and availability information were reviewed. These interventions, documented in the 19 reports reviewed, were implemented in four different countries (Peru, Taiwan, the United States of America and Zimbabwe). The factors that were associated with these intervention’s emergence and persistence were identified as: the recognition of a medicine access problem that can be mitigated by consumer access to information; cross-sectoral collaboration; the willingness of medicine sellers to disclose their inventory information; having information quality control measures; appropriate incentives for intervention adoption; enabling legal environments; systems of pooling information and access to digital information technology infrastructure. This finding answered the second research question, which was: What factors are associated with the establishment and sustainability of interventions that provide individual consumers with information about medicine availability and prices?
How information is conceptualised in theoretical frameworks
Table 2 shows the different documents that conceptualise ATM and PSS strategies. Table 2 also summarises how each document casts the role of information in ensuring ATM and strengthening pharmaceutical systems.
Factors associated with the provision of medicines availability and price information to consumers
Table 3 summarises the main details of the four interventions that facilitate consumers’ ATM price and availability information. Each report was iteratively read and a thematic analysis, focusing on identifying the factors that were associated with the intervention’s emergence and persistence was done (Figure 4).
Interventions supplying consumers with information about medicine availability and prices at named location.

1 Several more applications identical to GoodRxTM exist in the United States. However, only GoodRxTM was reviewed because: it is the pioneer and market leader. It is also the application for which substantive literature, other than promotional material, was found. GoodRxTM has been documented in both peer-reviewed and grey literature.
2 This intervention pertains to masks rather than medicines, it was included because masks were considered health products and were accessible from pharmacies. The intervention embodied the principle of consumer access to information, which is the focus of this article.
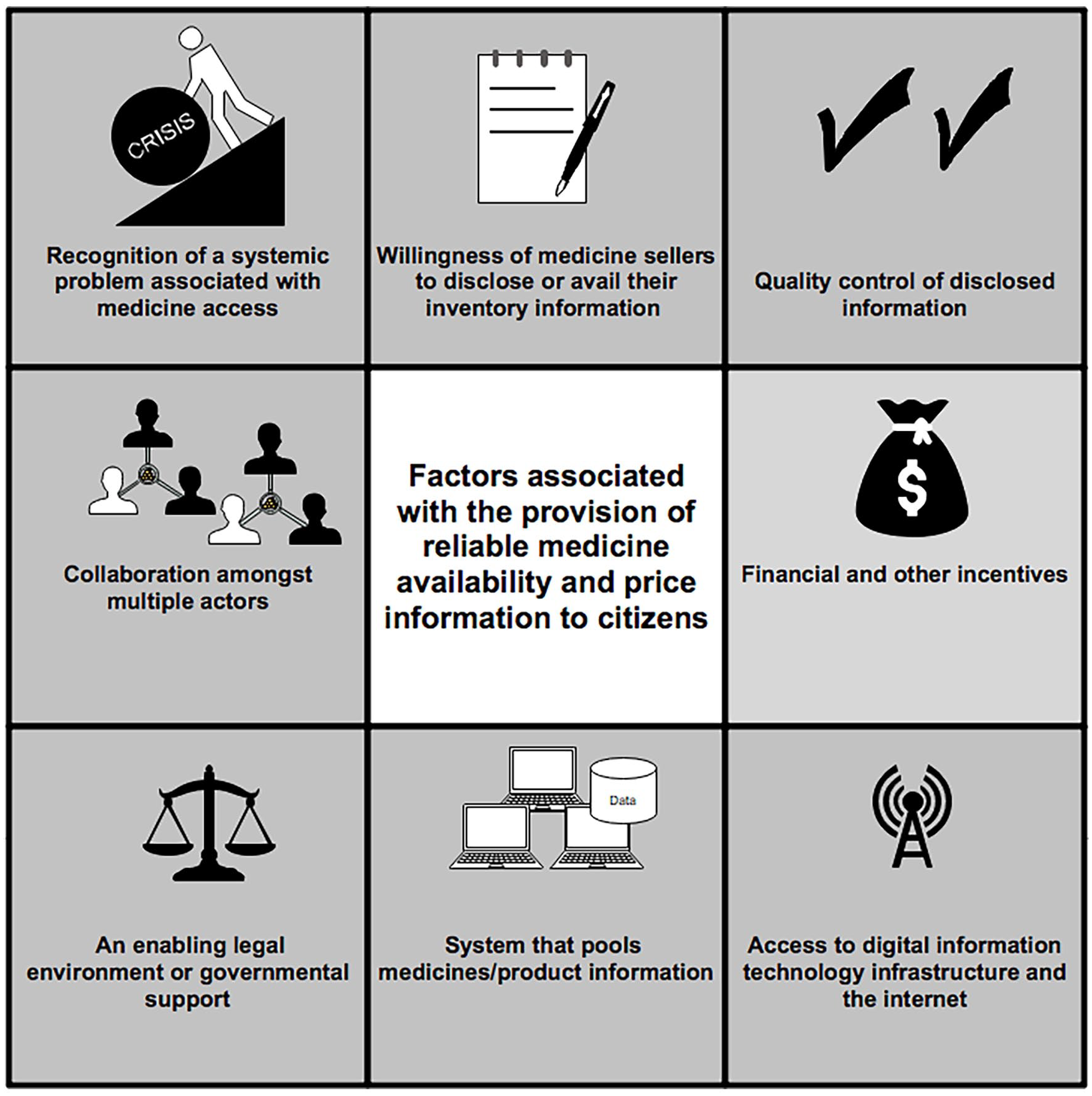
Factors associated with the provision of medicines availability and price information to consumers.
Recognition of a systemic access-related problem
The impetus for each intervention identified (Table 3) was a systemic problem related to the availability or prices of pharmacy products. In Peru, the sustained increase in medicine prices and out-of-pocket spending on medicines drove efforts to increase price transparency to empower consumers to make more informed purchasing choices. 44 In the United States, the variation in prescription medicine prices across pharmacies motivated the establishment of price comparison tools exemplified by GoodRxTM. 56 The heightened demand for face masks in Taiwan during the Coronavirus disease pandemic led people to develop digital tools to help consumers identify pharmacies where masks could be accessed.53,55 Finally, medicine price variation and the erratic availability of medicines across Zimbabwean pharmacies, coupled with advertising regulations that encumbered pharmacies’ ability to broadcast details of their inventory to consumers, were associated with the persistence of the pharmacists’ WhatsApp group communities where availability information is routinely shared and price information is solicited. 67
Product sellers disclosing their inventory information
Medicine availability and price information interventions depend on the accessibility of medicine sellers’ inventory and price information. This can be through medicine sellers uploading their information to a government-run, publicly accessible and searchable website, for example, in Peru;43,44,57,59 using proprietary technology operated by medicine price comparison businesses, for example, in the United States; 56 linking pharmacy information systems to a central mainframe, for example, in Taiwan53,54,68,69 or as in Zimbabwe, having pharmacists participate on the WhatsApp communities of practice, responding to medicine availability and price queries posted there. 67
Information quality control
When pharmaceutical service providers are compelled to disclose information, there may be an incentive to report inaccurately. 67 Ways of safeguarding the quality of inventory and price information disclosed by medicine sellers are integral to any plan to provide reliable consumer information. In Peru, civil society monitors prices, availability and quality of medicines in communities.59,61 GoodRxTM56 reports that its proprietary technology checks and triangulates the price information that it provides. Finally, following Taiwanese citizens and residents’ reliance on crowdsourced social media mask availability information, the government began to supply real-time pharmacy mask inventory information, to facilitate access to information that’s more reliable. 53
Collaboration amongst multiple actors
Medicine price and availability information interventions are typically the result of collaborative actions, with different actor groups in a society taking up different roles. These roles include: advocacy and drawing attention to the need for an intervention, for example, citizens or bilateral development partners,43,44,53 approving, developing, funding and leading the intervention’s implementation, for example, governments, private for-profit entities, software developers,53–56 supplying the medicine and price information required to drive the interventions 67 or monitoring/verifying the information disclosed. 61
An enabling legal environment or governmental support
The interventions reviewed in this article owe their existence to permissive legal environments or government endorsement. In Peru, for instance, new legislation was promulgated to establish the Medicine Price Observatory 58 and mandated all medicine sellers to regularly submit their price information to the Medicines Price Observatory (MPO) Peru. 57 In the United States, the legal environment is considered liberal with respect to pharmaceutical advertising. 70 Interventions like GoodRxTM can be implemented there with minimal advertising-related legal impediments. The WhatsApp groups used by Zimbabwean pharmacists to indirectly communicate availability and price information to consumers operated with the implicit endorsement of medicine regulatory officers, some of whom were active members of these WhatsApp communities themselves. 67 The Taiwan face mask apps were developed following encouragement by the government, using real-time mask inventory information provided by the same government.53,54
Incentives
Incentives for both the consumers and providers of medicine availability and price information encourage the adoption of interventions that provide this information. For consumers, the prospect of accessing products quicker and more affordably, can be a powerful incentive for adoption. GoodRxTM incentivises consumers by offering them medicine discount coupons in addition to providing them with medicine prices and the pharmacy locations where these medicines are available. Although some pharmacies can lose revenue by dispensing medicines at discounted prices to bearers of GoodRxTM coupons, 64 and although there are concerns about the data protection policies of companies that supply discount coupons, 63 some pharmacists consider the potential increased traffic from coupon customers, a benefit. 64 Finally, participation on the Zimbabwean WhatsApp groups has several benefits for pharmacists. These benefits include: opportunities for socio-professional networking, opportunities to increase revenue by indirectly advertising their inventory and access to crowdsourced knowledge about a wide range of practice-related subjects. 67
A system that pools/crowdsources information
All medicines information interventions considered in this article rely on online systems of pooling medicines/product information. For instance, the Peruvian Ministry of Health manages a database (the MPO database) centrally. As already mentioned, Taiwan operates a single-payer National Health Insurance (NHI). The NHI-contracted pharmacies’ information systems are linked to the NHI mainframe. Therefore, the Taiwanese government superintends over a central online location where mask inventory information from NHI-contracted pharmacies updates in real time. This information is then provided to the public through apps and websites. GoodRxTM and similar tools in the United States consolidate availability and price information from multiple pharmacies and deliver it from a single digital platform. The Zimbabwean WhatsApp groups are convergence sites for hundreds of pharmacists. 67 They act as informal pooling digital locations where multiple pharmacists’ inventory information can be accessed.
Access to digital information technology infrastructure and the Internet
Medicine availability and price information pooled from a large number of pharmacies can be dynamic and voluminous. Medicine availability and price information therefore lends itself to management by digital tools and transfer via the Internet. All the four interventions reviewed herein were Internet-based and could only be accessed via digital communication devices.
Discussion
Consumer ATM availability and price information is critical to facilitating patients’ timely access to affordable medicines. Through two scoping reviews, we sought to assess the extent to which this is recognised in extant ATM theory and discourse. We also sought to uncover factors that tend to be associated with the development and persistence of interventions that provide consumers with medicine price and availability information. Our analysis revealed that the role of information in the achievement of medicine access and PSS goals is universally recognised in ATM literature. However, consistent with our pre-study hypothesis, information in the context of ATM is mainly conceptualised as a resource that enables macro-level planning and monitoring by governments, or as a resource that organisations and practitioners involved in medicine management can use to make rational choices. The ATM and PSS frameworks and models turned up by our review do not adequately capture and engage with the role of information as a decision-making tool for individual medicine seekers. It could be argued that if medicine availability and affordability of medicines is ensured at the macro-level, it will necessarily be guaranteed at the micro-level thereby negating the need for consumers to have access to price and availability information. However, in reality, market and government failures at the macro-level undermine ATM at the micro-level.17,33 The resulting price variations and the uneven distribution of medicine stocks across pharmacies and drugstores in a health system then justify providing consumers with information that will help them with price comparisons and with locating pharmacies/drugstores that have particular medicines in stock.
It is concerning that access to price and availability information by consumers is overlooked in ATM theory. It is concerning because, as Table 2 shows, ATM frameworks are usually developed specifically for particular aims. 25 ATM frameworks signal global health priorities and influence decisions about where attention is focused. What is excluded from frameworks, therefore, risks exclusion from the implementation agenda. Indeed, the lack of any mention of medicine price and availability information for consumers in the vast majority of ATM and PSS frameworks coincides with the following observation from this article’s second scoping review: very few implementation cases exist of tools developed to assist consumers in timeously locating sources of affordable medicines and other medical devices typically found at pharmacies.
Despite the limited number of examples of medicine availability and price information tools aimed at individual consumers, they exhibit considerable diversity as far as types of actors that are driving the intervention implementation is concerned. In the United States, it is private corporations (exemplified by GoodRx) that are providing access to consumer price and availability information. In Peru, the MPO was established by the government, following processes brokered by the Medicines Transparency Alliance, a multi-stakeholder initiative. In Taiwan, it was the civil society of netizens that developed Mask-map apps with governmental support. In Zimbabwe, the WhatsApp groups used as a source of real-time price and availability information are products of action by healthcare professionals (pharmacists). This observation demonstrates that the under-provision of availability and price information to consumers is problematised from the perspectives of actors in diverse sectors. This bodes well for collaboration, 71 one of the factors consistent with the successful establishment of platforms that supply medicine availability and price information to consumers.
The simplistic visual representation of the factors associated with the provision of medicine availability and price information to consumers (Figure 4), should not be allowed to belie the complexity associated with getting all these eight factors to align. Achieving each of them can potentially require years of skilfully navigating socio-political landscapes while managing financial, human and information resources. For example:
The recognition of an access-related systemic problem requires people to problematise the crisis, possess agenda-setting power or at least have access to entities that have agenda-setting power. 72 Examples of such agenda-setting entities include, government, private sector businesses or civil society.
The willingness of medicine sellers to disclose or avail their inventory information depends on how they perceive the costs and benefits of such disclosure. 67 Clarifying the incentives or demonstrating the benefits for medicine sellers is key.
Ways of safeguarding the quality of inventory and price information disclosed by medicine sellers are integral to any plan to provide reliable consumer information. However, the sheer volume of rapidly changing data reported by diverse sources can threaten the feasibility of effective information quality control plans. 73 This challenge can be managed by implementing risk-based verification models, where information from unreliable information suppliers is verified more rigorously than information from sources that are routinely reliable.
Coming up with the right incentives for pharmaceutical system actors to adopt certain innovations or behave in particular ways requires contextual and institutional analyses to understand the subjective perspectives of stakeholders. 33
Most governments regulate the flow of medicines information to consumers. On one hand, direct-to-consumer pharmaceutical advertising (DTCPA) laws can limit the ways in which medicine sellers can communicate details of their inventory and prices.16,70 On the other hand, legal coercion may facilitate the disclosure of inventory information by pharmaceutical service providers. An enabling legal environment or other governmental support is necessary to successfully deliver a medicines price and availability information tool. Yet, it may take years of lobbying to create. 74 It is however possible; in Zimbabwe for instance, courts of law were used to successfully lobby for the acceptance of a medicine price and availability information proposal. 75
Information pooling systems or centralised information systems may be at odds with the common new public management philosophy, which favour decentralised systems more. 76 However, decentralised systems need not prohibit the crowdsourcing activities that are necessary for running medicines information services.
Ensuring equitable access to digital information technology infrastructure and access to the Internet demands considerable financial investment and the political will to leverage technology for socioeconomic development. 77 Yet, this too can be achieved even by governments in low-income countries. 75
Finally, it is worth highlighting that the pursuit of the goal of providing consumers with medicine availability and price information may be associated with potential pitfalls that must be mitigated or guarded against. Here, we discuss three that are related to patient safety, social inequalities as well as information governance.
Patient safety
Tools that point consumers towards pharmacies that have particular medicines in stock, have the potential to drive patients towards pharmacies that dispense medicines of unverifiable quality. Even licenced pharmacies have been shown to stock substandard medicines.78–80
Social inequalities
Digital health interventions have the potential to bridge inequalities in health systems. For instance, telemedicine tools allow physically inaccessible patients to access medical care remotely.81,82 However, digital health interventions also have the potential to widen health inequalities, 83 especially in Africa’s developing countries. 84 National level of economic development and geographic location, level of education, poor computer skills, literacy skills, including health literacy, age, ability to pay for the technology, ethnicity, economic status all shape one’s engagement with digital health interventions.83,85,86 Likewise, digital tools that disseminate information about where particular medicines are available have both the potential to facilitate quicker access to affordable medicines for some patients, and the potential to widen pre-existing inequalities. For consumers to effectively use medicine price and availability tools, they would need to have access to the Internet and Internet-enabled devices. They would also need to be medically literate enough to be able to decode their own prescriptions or be assertive enough to demand that their healthcare providers clarify the contents of their written prescriptions. This means that demographic groups lacking medical literacy and/or Internet access can be excluded from potentially useful information services.
Information governance
The application of digital information management tools to healthcare-related processes raises data privacy and security concerns.87–89 For instance, data privacy and security concerns were raised about the selling of patient data to third parties by private sector firms like GoodRx, which run digital platforms to inform patients about the prices of medicines at different pharmacies in the United States. In addition to providing this obviously useful information to citizens, these firms then also offer discount coupons that citizens can redeem as they purchase medicines. It is in exchange of these coupons that these firms collect and store patients’ data. 64 On the WhatsApp groups used by Zimbabwean pharmacists, pictures of patients’ prescriptions were shared in order to find out the pharmacies that were able to dispense the medicines on the prescriptions. Although the WhatsApp group rules required that the patient name and other personal details be concealed before a prescription picture was posted onto the groups, some pharmacists neglected to do this. Social media, although convenient for social communication, is not secure enough for the transmission of health information. 90 In some jurisdictions, healthcare professionals have been investigated by regulators for inappropriately transmitting health information via social media. 91
Limitations
Consistent with the methodological framework for conducting scoping reviews, we did not discount reports based on a critical appraisal of quality. We included all documents turned up by our scoping review that reported on the intervention of interest. In coming up with the factors associated with the provision of medicines availability and price information to citizens, we then relied only on these reports, many of which were mostly positive and did not shed light on adoption or implementation challenges or the lack thereof. Moreover, only four interventions were identified through this scoping review. As similar interventions emerge and become reported in critical and balanced ways, the set of factors we advanced in this article will likely be modified. Second, we focused our review on content written in English or Spanish. It is possible that this might explain the low number of interventions discovered during the second scoping review.
Conclusion and recommendations
The role of information as an enabler of ATM is well-recognised. However, information is almost always conceptualised as a decision-making resource for governments, policymakers and organisations in their quest to ensure access to affordable medicines for whole populations and communities. In ATM discourse, information is less often cast as a decision-making aid for consumers as they seek to find out where to access specific medicines affordably. We recommend that more focused attention be directed at how medicine price and medicine availability information can empower individual medicine consumers to make sound purchasing decisions. Digital innovations that aim to directly or indirectly supply consumers with real-time information about where particular pharmacy products are in stock, as well as the price thereof, have begun to emerge. Their success however turns on governments, civil society, private sector and medicine sellers, working in concert to:
identify the value of transparency and information access at every level of the pharmaceutical system,
promote legal environments, information quality control protocols and incentive frameworks that are conducive for the equitable access to reliable consumer information and
build and sustain the requisite digital information management infrastructure.
Supplemental Material
sj-docx-1-map-10.1177_27550834221098598 – Supplemental material for Consumers’ access to information about medicine prices and availability as an enabler of last mile medicine access: A scoping review
Supplemental material, sj-docx-1-map-10.1177_27550834221098598 for Consumers’ access to information about medicine prices and availability as an enabler of last mile medicine access: A scoping review by Dudzai Mureyi, Shingai D Gwatidzo and Celia MJ Matyanga in Medicine Access @ Point of Care
Supplemental Material
sj-docx-2-map-10.1177_27550834221098598 – Supplemental material for Consumers’ access to information about medicine prices and availability as an enabler of last mile medicine access: A scoping review
Supplemental material, sj-docx-2-map-10.1177_27550834221098598 for Consumers’ access to information about medicine prices and availability as an enabler of last mile medicine access: A scoping review by Dudzai Mureyi, Shingai D Gwatidzo and Celia MJ Matyanga in Medicine Access @ Point of Care
Footnotes
Acknowledgements
The authors acknowledge the contribution of Claudia Pagliari, who helped identify the Taiwan mask intervention. Finally, the authors thank the anonymous reviewers whose feedback improved the quality of this article.
Author contribution(s)
Availability of data and materials
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The first author is a pharmacist currently researching and developing an intervention that aims to provide citizens with medicine availability and price information and has recently received funding from the Government of Zimbabwe to develop this intervention. The Government of Zimbabwe had no role in the design of this study and collection, analysis, and interpretation of data, in writing the article or the decision to publish. The remaining authors declare that they have no conflict of interest.
Ethical approval
This article reports the carrying out of two literature reviews. No animal or human studies were carried out. No secondary analysis of data collected from humans was carried out. Therefore ethics approval was not sought.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: While working on the research that resulted in this article, the first author received funding to cover doctoral tuition fees and expenses from the Beit Trust and the University of Edinburgh between 2016 and 2019. The funding bodies had no role in the design of the study and collection, analysis, and interpretation of data, in writing the article or the decision to publish.
Human rights
This article reports the carrying out of two literature reviews. No human studies were carried out. No secondary analysis of data collected from humans was carried out. Our work did not have human rights implications.
Informed consent
This article reports the carrying out of two literature reviews. No animal or human studies were carried out. No secondary analysis of data collected from humans was carried out. Therefore informed consent was not sought.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.