
Abstract
Introduction:
The World Health Organization (WHO) Model List of Essential Medicines guides countries in selecting priority drugs to ensure equitable access to effective treatments. In regions such as Central America, with similar health and socioeconomic contexts, comparing national lists reveals patterns and opportunities for regional harmonization.
Methodology:
A cross-sectional comparative observational study was conducted using public secondary data from the official essential medicines lists of seven Central American countries: Belize, Costa Rica, El Salvador, Guatemala, Honduras, Nicaragua, and Panama. These lists were compared against the 2017 WHO Model List. Therapeutic classification was based on the Anatomical, Therapeutic, and Chemical Classification (ATC) system (level 2). Macroeconomic variables, including health expenditure per capita and gross domestic product (GDP) per capita, were analyzed for their relationship with list composition.
Results:
Panama had the most extensive NEML (570 drugs) and Nicaragua the shortest (271 drugs). Nicaragua showed the highest alignment with the WHO list, while Panama had the most exclusive drugs. A significant positive correlation was found between health expenditure per capita and NEML size (r = 0.77; p = 0.042), but not with alignment to the WHO list. The most represented therapeutic groups were antibacterials (31.2%) and antineoplastics (24.4%).
Conclusion:
Although Central American countries share regional similarities, their selection of essential medicines varies considerably. These differences reflect diverse public health priorities, institutional capacities, and economic conditions. The findings support the need for evidence-based, context-sensitive approaches and underscore the potential for regional cooperation in essential medicines policy.
Introduction
The World Health Organization (WHO) Model List of Essential Medicines is a policy document that aims to identify those medicines that offer the greatest benefit based on the needs of patients worldwide. It is a tool at the service of Member States to establish good practices and develop procedures for the selection of essential medicines at national level.1,2
The model list was first published in 1977, originally including 186 medicines considered indispensable to all health care systems and provided guidance on the selection of medicines for the national drug lists. 3 Since then, it has been updated every 2 years to incorporate new drugs, in response to the emergence of new diseases and the availability of recently approved treatments. As a result, the process of selecting medicines has become progressively more complex.1,4,5
Since 2007, the WHO has included a second list of medicines aimed at children, called the WHO Essential Medicines List for Children, which is also updated approximately every 2 years. 3 This study will only refer to the WHO Model List of Essential Medicines and not to the children’s Formulary of Essential Medicines.
Each country must carefully select the medicines that will be included in its official list, with the aim of ensuring sustainable and equitable access to treatments. For this reason, it is natural for drug lists to vary between countries, as each one responds to the specific needs of its population, excluding medicines from the model list and including exclusive medicines (which are not on the WHO model list). However, it is reasonable to expect that countries with similar characteristics (such as those with similar geographical proximity, income level, and epidemiological profile) will have comparable lists of medicines. 6
In Central America, national essential medicines lists play a key role as guides for public sector drug procurement, references for prescribing across different levels of care, and, in some cases, as criteria for reimbursement in public insurance systems. They are also used to set priorities for the availability of hospital and outpatient medicines. However, the degree of mandatory enforcement and the frequency of updates vary among countries, resulting in differences in their content and scope. These variations stem from institutional, regulatory, and technical factors that, in turn, shape the selection of medicines included.
This is why the comparison of lists of essential medicines among Central American countries is a methodologically viable initiative of high analytical value, given the shared regional context. This subregion is characterized by evident geographic proximity, epidemiological similarities, comparable health structures, and an intertwined socio-political history that has shaped health systems with common challenges and priorities. In addition, Central American populations have similar demographic profiles, population sizes, and ethnic compositions, which reinforces the relevance of contrasting their pharmaceutical policies. Although there are studies that have compared lists of essential medicines in other regions of the world, or that have focused their analysis on specific therapeutic groups, to date a comprehensive comparison of the complete lists in Central American countries has not been carried out. 6 Studying coincidences and divergences in the selection of essential medicines can provide useful evidence to promote regional harmonization, identify opportunities for improvement, and strengthen equitable access to critical therapies across the region. The objective of this study is to compare the lists of essential medicines of Central American countries, evaluating their alignment with the WHO model list and their relationship with macroeconomic variables.
Local epidemiological particularities may justify the inclusion of medicines not listed in the WHO Model List of Essential Medicines. Although the present study did not address specific high-prevalence diseases. It is acknowledged that such country-specific exceptions can significantly influence the composition of national essential medicines lists and should be considered in future research. Nevertheless, Central American countries share multiple geographic, epidemiological, demographic, and health system similarities, providing a methodologically sound basis for meaningful regional comparisons regarding the selection of essential medicines.
Materials and methods
Study design and context
A cross-sectional comparative observational study was carried out that analyzed the official lists of essential medicines of the seven Central American countries: Belize, Costa Rica, El Salvador, Guatemala, Honduras, Nicaragua, and Panama. The study was conducted between April and May 2025, using as a documentary basis the most recent versions available of each national list of essential medicines at the time of data collection.
No sample size calculation was performed, as the study included the complete universe of national essential medicines lists from the seven Central American countries, ensuring full regional coverage.
Data source and inclusion criteria
The official lists were obtained through government portals of the Ministries of Health, documents published in institutional repositories and international databases such as the WHO. Only documents identified as national lists of essential medicines in force were included, excluding other types of lists such as clinical guidelines, therapeutic protocols or commercial catalogs. No additional exclusion criteria were applied. All officially recognized national essential medicines lists were included regardless of their publication date, to ensure comprehensive regional coverage and representation.
Data processing and validation
Each drug was classified using its International Nonproprietary Name (INN). In cases where names did not follow standardized nomenclature or were in other languages, the WHO Anatomical, Therapeutic, and Chemical Classification (ATC) system was used to ensure uniformity. The classification level used was the second therapeutic level of the ATC system. No formal external validation of the classification algorithms was used, although manual peer review was applied to ensure accuracy in coding.
No formal external validation of the classification algorithms used for pairing with the ATC system was performed; however, manual peer review was applied to ensure consistency and accuracy in coding.
To minimize potential misclassification bias, all drug names were standardized using their International Nonproprietary Name (INN) and cross-verified with the WHO ATC classification system. Potential selection bias was reduced by including all officially recognized national essential medicines lists, regardless of their year of publication, ensuring comprehensive representation of each country.
Data access and management
The research team had full access to all the public documents analyzed. Data cleansing included the removal of duplicates, standardization of drug names, and homologation with ATC codes. The quality of the lists was assessed by verifying integrity, format, and correspondence with official sources.
Comparative analysis
The WHO Model List of Essential Medicines for 2017 was used as a reference, consisting of 414 medicines. The 2017 WHO Model List of Essential Medicines was selected as the reference because it was the most recent consolidated version available that corresponded with the latest national lists accessible at the time of data collection. Its use ensures a consistent basis for cross-country comparison, given that not all countries had adopted newer versions. The presence or absence of each of these drugs on the national lists was analyzed. In addition, the medicines included by each country that are not present in the model list were identified.
Variables and statistical analysis
The main variables analyzed included: total number of medicines per country, number and percentage of matches with the WHO list, and number of exclusive medicines per country. Likewise, macroeconomic variables such as the gross domestic product (GDP) per capita and health expenditure per capita of each country for the year 2018, extracted from the World Bank and the WHO, were collected. The year 2018 was selected because it was the most recent with complete and comparable macroeconomic data for all countries in the official sources at the time of the analysis, ensuring temporal consistency with the lists analyzed.
Descriptive statistics were calculated, and Pearson’s correlation coefficient was used to explore the relationship between health expenditure and the pharmaceutical indicators mentioned above. A value of p < 0.05 was considered as a threshold of statistical significance.
For each correlation coefficient, 95% confidence intervals were calculated using Fisher’s z transformation, applying the standard error formula and transforming the limits back to the r scale.
Summary of methodological process
The methodological flow followed for the selection, processing, and analysis of the national lists of essential medicines of the Central American countries is described below. This diagram summarizes the main stages, from obtaining the lists to generating results, including the sources of the data, the classification system used and the variables evaluated.
Ethical considerations
Because the study was based exclusively on publicly accessible secondary data and did not include individualized or identifiable information, it was not necessary to obtain approval from an ethics committee.
Results
The official lists of essential medicines analyzed in this study correspond to the seven countries of Central America: Belize, Costa Rica, El Salvador, Guatemala, Honduras, Nicaragua, and Panama. They were obtained from the international Global Essential Medicines database of the World Health Organization (WHO), 7 with the exception of the Panama and Guatemala schedules,8,9 which were located directly on the official websites of their respective Ministries of Health, as they were not available in that database. Only documents officially recognized as current national lists of essential medicines were included.
Comparison with the WHO model list
Nicaragua is the Central American country whose official list of essential medicines contains the fewest medicines included in the WHO Model List, with a total of 202 drugs. In contrast, El Salvador and Belize have the highest figures, with 253 drugs each (Table 1).
Composition of national essential medicines lists and main macroeconomic indicators in the seven Central American countries.

GDP: Gross Domestic Product; WHO: World Health Organization.
Exclusive essential medicines: Medicines considered essential by each of the countries that are not part of the WHO model list.
WHO Essential Medicines: Medicines that are part of the WHO Model List of Essential Medicines.
Difference: Corresponds to the difference between the number of medicines in each of the essential lists of each country with respect to the number of medicines present in the WHO model list.
Likewise, Nicaragua registers the lowest number of exclusive medicines by the WHO, with only 59, while Guatemala and Panama have considerably higher figures, with 227 and 337 medicines, respectively.
As shown in Figure 1, Nicaragua is the country that most adheres to the WHO Model List of Essential Medicines, suggesting greater alignment with international recommendations. At the opposite extreme, Panama includes a significant proportion of medicines that are not part of the list. Table 1 details these findings.
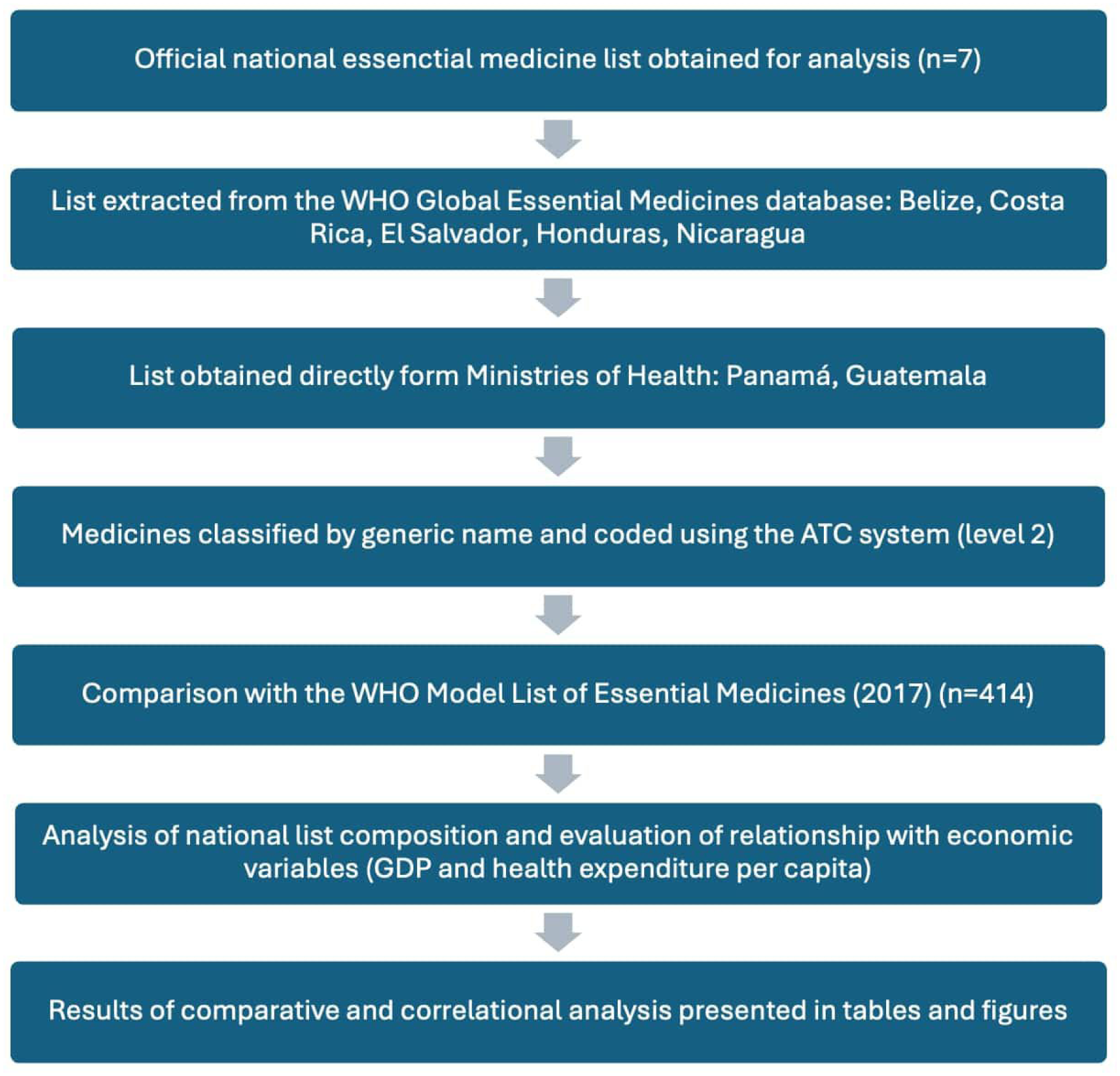
Flow chart of the process of obtaining, classifying, and analyzing the national lists of essential medicines of seven Central American countries.
None of the 7 countries includes all the medicines that the WHO considers essential medicines. Of the 414 WHO essential medicines used as references, 85 (20.53%) are present on the national lists of the seven countries analyzed and 191 (46.14%) are in at least six countries. In contrast, 39 drugs (9.42%) are present in only one country and 53 (12.80%) are not on the national lists of any of the countries in the region.
It is important to note that, of the 85 medicines shared by all Central American countries, 37 (43.53%) belong to the categories of medicines for the cardiovascular system, nervous system, or food tract and metabolism, according to the WHO ATC classification.
The economic investment in health of the seven Central American countries was analyzed with the aim of exploring how health spending and national economic power could influence the formation of their lists of essential medicines, particularly in terms of the degree of alignment with the WHO Model List and the inclusion of exclusive medicines. The data used correspond to the year 2018. Table 2 presents the breakdown of investment in health by country.
Five main therapeutic groups (CTA level 2) present in the combined lists of essential medicines of the Central American countries.

Figure 2 shows the relationship between the investment made by each Central American country in health and the number of essential medicines on their respective national lists. It stands out that those countries that direct more funds to health have more essential medicines on their national lists. Likewise, it is observed that countries such as El Salvador or Belize that invest less in health than Panama or Costa Rica, are more attached to the WHO’s model list of essential medicines as mentioned above.

Composition of the lists of essential medicines of the Central American countries.
The relationship between each country’s per capita health expenditure and three indicators derived from their national lists of essential medicines was assessed: the percentage of coincidence with the WHO model list, the total number of medicines included, and the percentage of exclusive medicines (those do not present on the WHO list). To do this, Pearson’s correlation coefficient was used, and the corresponding p values were calculated to determine statistical significance (Figure 3).

Relationship between investment in health by Central American countries and the number of essential medicines on their national lists.
It is important to clarify that no missing data were identified in the lists of drugs analyzed or in the macroeconomic variables used.
A positive and statistically significant correlation was observed between per capita health expenditure and the total number of essential medicines included in the national list (r = 0.77; 95% confidence interval (CI): 0.04–0.96; p = 0.042).
In contrast, no statistically significant relationship was found between per capita health expenditure and the percentage of agreement with the WHO list (r = –0.67; 95% CI: –0.95–0.17; p = 0.097), nor between health expenditure and the percentage of exclusive medicines (r = 0.67; 95% CI: –0.17–0.95; p = 0.097). Although these correlations were moderate, the results did not reach statistical significance, indicating that higher health spending does not necessarily translate into greater alignment with international standards, nor does it imply a clear trend toward the inclusion of medicines not contemplated by the WHO. This apparent disconnect can be explained by the influence of non-economic factors, such as national pharmaceutical governance, the level of technical independence of the committees that update the lists, or the influence of bilateral agreements, international cooperation programs and grants.
The official lists of essential medicines of the seven Central American countries were analyzed. Each drug was classified using the ATC (Anatomical Therapeutic Chemical Classification System) at the level of the second therapeutic level, in order to identify the main national pharmacotherapeutic priorities and compare public health approaches between countries.
At the regional level, systemic antibacterials were the most represented with a total, with 31.2% of the total, reflecting the high regional priority toward the treatment of infectious diseases. It was followed by the group of antineoplastic agents (L01) with 24.4%, indicating a growing focus on access to cancer treatments. Other relevant groups included J05 (antivirals for systemic use, 10.5%), J07 (vaccines, 5.9%) and N05 (psycholeptics, 5.7%), which shows joint attention to infectious diseases, prevention through immunization and mental health. This distribution suggests a combination of priorities geared toward communicable disease control, cancer care, and strengthening essential clinical services. The summary of the main groups of medicines present in the essential drug lists of the region is presented in Table 3.
Main therapeutic groups (CTA level 2) in the lists of essential medicines of each Central American country according to quantity and percentage.

The therapeutic group J01 (antibacterials for systemic use) was the most represented in five of the seven countries: El Salvador (11.2%), Belize (10.9%), Nicaragua (10.8%), Guatemala (10.2%), Costa Rica (8.5%).
These findings reflect a marked regional priority toward infectious disease control, consistent with the prevalent epidemiological burden in the region and the importance of access to antibiotics in primary care.
On the other hand, the L01 group (antineoplastic agents) ranked first in the countries of Honduras (11.9%) and Panama (10.8%), suggesting a greater emphasis on access to cancer treatments in these health systems. In the rest of the countries, L01 was also positioned among the most frequent groups (Table 3), which shows a growing trend to include drugs for the treatment of cancer as part of national policies for essential medicines.
In addition to J01 and L01, three other therapeutic groups stood out among the five most represented at the regional level: J07 (vaccines), with a relatively high presence in countries such as El Salvador, Guatemala, and Panama, reflecting the priority given to immunization within public prevention policies. J05 (antivirals for systemic use), with relevant proportions especially in Belize, Guatemala, and Panama, probably in response to national programs for HIV, hepatitis, and other chronic viral infections. N05 (psycholeptics), which includes antipsychotics, anxiolytics, and sedatives, had significant representation in Costa Rica, Nicaragua, and Panama, suggesting a growing concern for mental health and behavior management in clinical settings.
These five groups reflect a regional vision that combines infectious disease response, cancer care, prevention through vaccines, treatment of chronic viral diseases, and addressing mental disorders. Differences between countries can be attributed to variations in disease burden, health system capacities, access to technology, and national policy priorities.
Discussion
Central America is a geographically compact region compared with other areas of the world, with a maximum distance of approximately 1,800 km between its northern and southern extremes, and a total area close to 523,000 km2. The countries that make it up also have important similarities in terms of population size, ethnic composition, and demographic profile. Despite this shared context, when comparing national lists of essential medicines, both between Central American countries and against the WHO model list, substantial differences are observed in the selection of drugs.
Figure 2 shows the proportion of essential medicines included in Central America’s national lists that match the WHO Model List of Essential Medicines, as well as the percentage of exclusive medicines that each country has considered essential but are not included in the model list. Looking at this figure, at first glance it could be interpreted that countries such as Nicaragua have a high adherence to the WHO list and, therefore, a better alignment with international recommendations. However, this does not reflect the absolute number of medicines included in each national list, which is essential for proper interpretation.
To this end, when observing Table 1, it is evident that Nicaragua is the country with the shortest list, while Panama presents the most extensive. Thus, although Nicaragua’s percentage of agreement with the WHO is high, this occurs on a significantly lower total basis, which relativizes its apparent alignment. On the other hand, countries such as Panama and Guatemala show lower percentages of agreement with the WHO, but this is largely due to the fact that they have incorporated a greater number of additional medicines considered essential according to their own national priorities.
This reflects how each country adapts the model list to its specific needs, considering its epidemiological profiles, public health priorities, health system capacities, and socioeconomic context. Therefore, beyond the proportion of coincidence, it is crucial to analyze what approach is adopted by each country in defining its lists and how this relates to their levels of health expenditure and GDP per capita, also reflected in Table 2.
Regarding the therapeutic approach of each of the national lists, the analysis of the therapeutic groups most represented in the lists of essential medicines of the Central American countries reveals consistent patterns, but also important differences that reflect the particular priorities of each health system. Overall, systemic antibacterials (J01 according to the second level ATC classification) were the most frequent group, with 31.18% of the total (Table 3), topping the list in five of the seven countries (Table 3). In countries such as Costa Rica, for example, although the mortality rate from communicable diseases has decreased (37.6 per 100,000 inhabitants in 2000 to 29.9 per 100,000 inhabitants in 2019), the use of antibiotics continues to be high and central in primary care, with amoxicillin among the most consumed drugs. 10 It is estimated that in this country, the 30 day mortality rate associated with community bacteremia due to Staphylococcus Aureus it is 40% in the adult population and 14.4% in children.11,12
In addition, the growing threat of multidrug-resistant bacteria has prompted the development of national action plans, such as the one implemented by Costa Rica (2018–2025), which emphasizes the surveillance, regulation, and rational use of antimicrobials. In this context, the widespread inclusion of antibacterials on essential lists responds to both immediate clinical needs and public health policies aimed at containing the spread of resistant infections and ensuring equitable access to effective treatments throughout the region.13,14
On the other hand, cancer-associated mortality represents a significant burden on Central American health systems; a possible explanation for why antineoplastic agents occupied the first place in the lists of Honduras and Panama (Table 3), and were among the main groups in the rest of the countries, demonstrating a growing effort to improve access to cancer treatments, in a context where cancer has gained relevance as one of the main causes of morbidity and mortality in Latin America.
The prominence of antineoplastic drugs in countries with lower health expenditures, such as Honduras, may seem contradictory, but it responds to a combination of factors. On one hand, cancer has emerged as a relevant cause of mortality in the region, which generates public and political pressure to guarantee access to treatments. 15 On the other hand, the inclusion of these medicines may reflect national strategies to improve basic cancer coverage, even when their effective availability is limited by budgetary barriers. In some cases, these countries could benefit from pooled procurement, volume purchasing or international grant mechanisms that facilitate the inclusion of high-cost therapies on official lists, without implying uniform implementation across the system. 16
According to data from the Pan American Health Organization (PAHO), in 2022 more than 1.4 million cancer deaths were registered in the region of the Americas, positioning cancer as the second leading cause of morbidity and mortality, after cardiovascular diseases. In Costa Rica, cancer represents the second leading cause of death with more than 6000 deaths annually, 17 with an invasive cancer incidence rate of 50.9 per 100,000 population with a significantly higher incidence in women than in men.18,19 In the rest of Central America, stomach cancer stands out as one of the leading causes of cancer death, with Guatemala having the highest mortality rate compared to the rest of the countries in the region, at 21.4 deaths per 100,000 inhabitants. Likewise, a sustained increase in breast cancer mortality rates has been observed in this country, as well as in El Salvador and Nicaragua, with estimated annual increases between 2.4% and 2.8%.20,21
Likewise, the prominent inclusion of vaccines in countries such as El Salvador, Guatemala and Panama highlights a commitment to primary prevention, associated with well-established immunization programs and the support of international organizations.22,23 In parallel, the group of antivirals for systemic use (J05) showed greater weight in Belize, Guatemala and Panama, related to the national response to HIV, hepatitis B/C and other viral infections with a chronic course or epidemic impact.
When analyzing the relationship between per capita health expenditure and the content of national lists of essential medicines in Central American countries, a positive and statistically significant correlation was identified between per capita health expenditure and the total number of medicines included in each list (r = 0.77; p = 0.042). This finding suggests that countries that invest more economic resources in their health systems tend to have more extensive lists of essential medicines, which could be related to a greater institutional capacity to evaluate, finance and guarantee access to a broader therapeutic spectrum. On the other hand, there was no statistically significant association between health expenditure and the percentage of agreement with the WHO Model List (r = –0.67; p = 0.097), nor with the percentage of exclusive medicines (r = 0.67; p = 0.097). Although the latter correlations were moderate, the absence of statistical significance indicates that higher health spending does not necessarily translate into greater adherence to international recommendations or a clear tendency to include additional drugs outside the framework established by the WHO. These findings highlight that, beyond economic investment, the composition of national lists is influenced by other factors such as local health priorities, policy decisions, pharmaceutical evaluation capacities, and regulatory or commercial agreements.
In addition to economic aspects, the composition of national lists also depends on the technical autonomy of the evaluation committees, the availability of cost-effectiveness studies, the priorities established in national health plans, and the type of international cooperation received, such as conditional donations or joint procurement mechanisms. These structural and political factors may explain divergences even among countries with similar financial capacity.24,25
A country’s list may contain a large number of essential medicines without incurring a higher cost if they are mostly generic or low-cost drugs. In contrast, the inclusion of high-cost drugs, such as antineoplastic drugs or immunomodulators, implies a much more significant investment, even if the total number of drugs is smaller.24,25
For this reason, countries with greater budgetary capacity, such as Costa Rica, can afford to integrate innovative and expensive treatments into their official list of essential medicines, which proportionally increases their health spending. By contrast, other countries, even if they include a larger number of medicines, may be limited to more economically accessible treatment options.
This contrast underscores the importance of assessing not only the size of the lists, but also their content and the financial context in which each country defines what it considers essential for its health system.
Conclusions
The comparative analysis of national essential medicines lists in the seven Central American countries reveals both similarities and notable differences, reflecting diverse public health priorities, institutional capacities, and policy contexts. While all countries use the WHO Model List as a reference, higher health expenditure per capita is associated with broader lists but not necessarily with greater alignment to WHO standards. The predominant therapeutic groups (antibacterials, antineoplastics, antivirals, vaccines, and psycholeptics) indicate shared regional priorities, and the case of Guatemala, with a longer list than Costa Rica despite the latter investing nearly three times more in health per capita, illustrates how differences in list composition, such as a greater proportion of generic low-cost medicines versus innovative high-cost drugs, can influence health expenditure independently of list size. These findings underscore the need to evaluate national lists considering both content and economic context, and to promote regional cooperation to harmonize selection criteria and strengthen equitable access to essential medicines.
Limitations of the study
This study has some limitations that should be considered when interpreting the findings. First, the 2017 version of the WHO Model List of Essential Medicines was used as a single reference, which may not reflect recent updates in therapeutic recommendations. Second, although the most recent official lists available were analyzed, the review mechanisms used by each country were not assessed, which could influence comparisons. In addition, the study focused on the presence or absence of drugs on official lists, without considering their actual availability, effective clinical use, or access in health systems. Finally, the correlation between macroeconomic variables and the content of the lists does not allow us to establish causal relationships, and there could be additional contextual factors (such as trade agreements or pharmaceutical market pressures) that were not included in the analysis.
In addition, the national lists of essential medicines used as a source of data were not created for research purposes, which could introduce classification biases, omissions or administrative changes not reflected in public documents. In addition, clinical or political variables that could influence drug selection were not measured in this study, representing a possible uncontrolled confounder.
Footnotes
Acknowledgements
The authors thank the health institutions of Central America that maintain their essential medicines lists publicly available, which enabled this regional comparative analysis.
ORCID iDs
Ethical considerations
The study used exclusively publicly accessible secondary data and did not involve identifiable individual information. As such, approval from an ethics committee was not require.
Consent to participate
Because no individual-level or identifiable data were collected or analyzed, obtaining informed consent from participants was not necessary.
Consent for publication
Not applicable.
Author’s Note
Kevin Cruz-Mora is now affiliated to Pharmacy Department, Hospital Clínica Bíblica, San José, Costa Rica.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All documents analyzed in this study are official, publicly accessible essential medicines lists and can be accessed online through the official portals referenced in the manuscript. No supplementary materials were generated. All the data generated are available in the body of the article.
Statement of generative AI in scientific writing
During the preparation of this work, the authors used ChatGPT (OpenAI) as a support tool for scientific writing. The content was reviewed and edited by the authors, who assume full responsibility for the final content of the article.