
Abstract
Background:
Deprescribing is a complex process requiring consideration of behavior change theory to improve implementation and uptake.
Aim:
The aim of this study was to describe the knowledge, attitudes, beliefs, and behaviors that influence deprescribing for primary healthcare providers (family physicians, nurse practitioners (NPs), and pharmacists) within Nova Scotia using the Theoretical Domains Framework version 2 (TDF(v2)) and the Behavior Change Wheel.
Methods:
Interviews and focus groups were completed with primary care providers (physicians, NPs, and pharmacists) in Nova Scotia, Canada. Coding was completed using the TDF(v2) to identify the key influencers. Subdomain themes were also identified for the main TDF(v2) domains and results were then linked to the Behavior Change Wheel—Capability, Opportunity, and Motivation components.
Results:
Participants identified key influencers for deprescribing including areas related to Opportunity, within TDF(v2) domain Social Influences, such as patients and other healthcare providers, as well as Physical barriers (TDF(v2) domain Environmental Context and Resources), such as lack of time and reimbursement.
Conclusion:
Our results suggest that a systematic approach to deprescribing in primary care should be supported by opportunities for patient and healthcare provider collaborations, as well as practice and system level enhancements to support sustainability of deprescribing practices.
Introduction
The use of potentially inappropriate medications (where the potential risk outweighs the potential benefit in the individual) and polypharmacy (taking five or more medications) has been associated with a number of negative health outcomes, including reduced quality of life, adverse drug reactions (ADRs), falls, non-adherence, hospitalization, and mortality.1 –7 In Canada, one in four community-dwelling older adults were prescribed 10 or more drug classes in 2016 8 with some evidence indicating that one in five prescriptions for older adults in primary healthcare are inappropriate. 9 A Canadian study from 2008 reported 12% of seniors taking five or more medications experienced an adverse effect that required medical attention compared with 5% of seniors taking only one or two medications. 10
With growing concern about the detrimental effects associated with potentially inappropriate use of medications worldwide, attention is shifting toward approaches to minimize harm, including “deprescribing.” 5 Deprescribing has been defined as the “planned and supervised process of dose reduction or stopping of medication(s) that may be causing harm or are no longer providing benefit” with the goal of reducing medication burden and harm, while maintaining or improving quality of life. 11 Studies examining deprescribing strategies have demonstrated reductions in medication use and associated costs.5,12 Some studies have also demonstrated clinical benefits, such as improved patient function and reductions in hospitalizations and mortality.5,12,13
Prescribing new medicines and renewing existing medications is a common practice for prescribers. When to consider ceasing medications is less clear. 14 The act of deprescribing is a complex behavior and therefore there is a need to understand the underlying context of the providers, patients, and systems.15,16 Conceptual frameworks of behavior change can be used to help design and evaluate complex behavior change interventions. 17 The Theoretical Domains Framework version 2 (TDF(v2)) is an integrative framework that consists of 14 domains not only to help determine the barriers and facilitators of implementing a change in behavior at an individual level but can also be used to understand behavior at the organizational or community level.18,19 A number of studies have used the TDF(v2) to understand influencers related to deprescribing, pharmacist prescribing, prescribing errors, and testing procedures.20 –23 The Behavior Change Wheel (BCW) by Michie et al. is a synthesis of frameworks of behavior change found in the literature. 19 At the core of the BCW is a model of behavior known as COM-B: standing for “capability,” “opportunity,” “motivation,” and “behavior.” This model recognizes that behavior is part of an interacting system involving these three main components. 19 Each domain of the TDF(v2) has been mapped to a COM-B component (Table 1).
TDF(v2) domains linked to COM-B components.
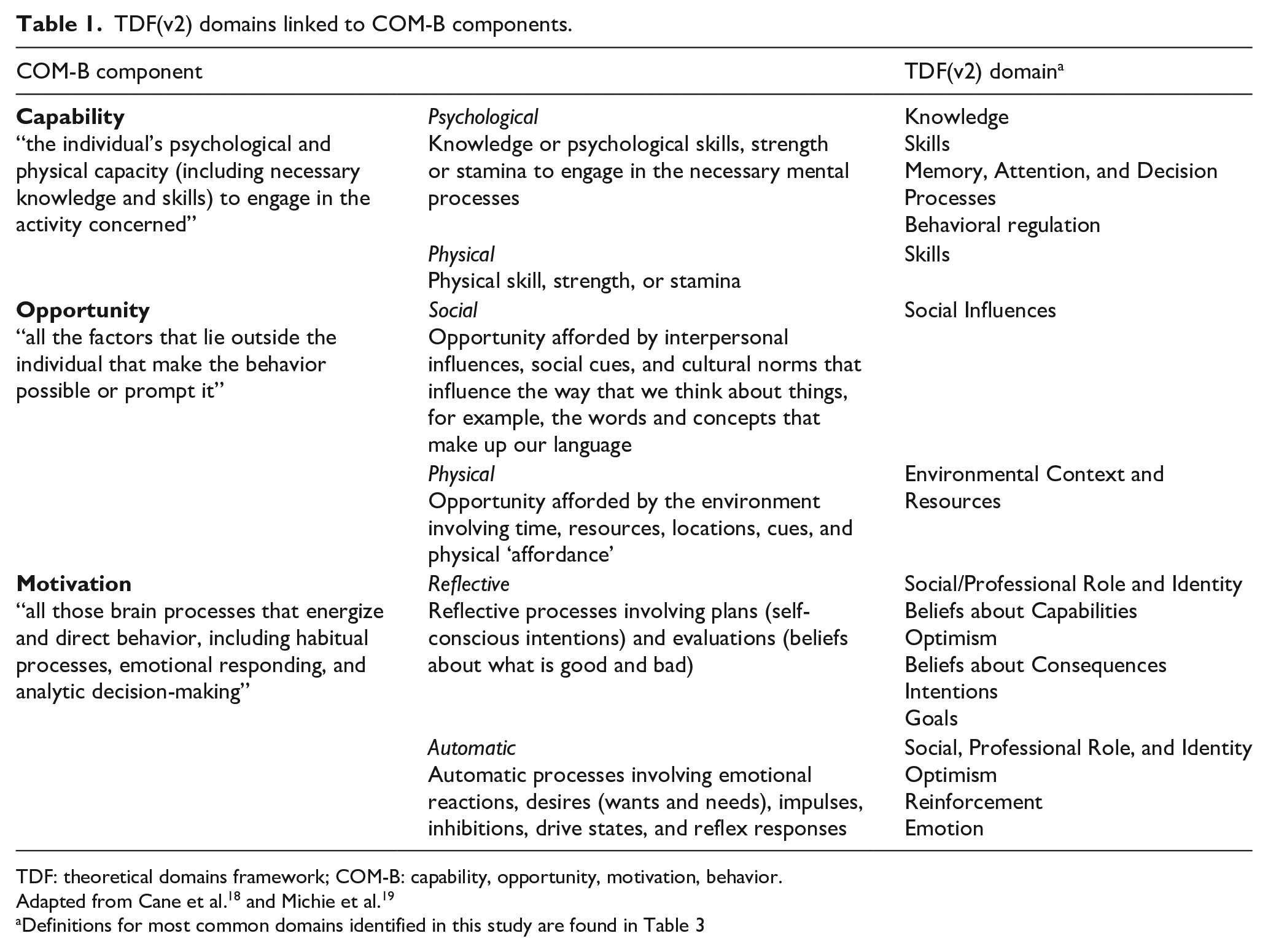
TDF: theoretical domains framework; COM-B: capability, opportunity, motivation, behavior.
Definitions for most common domains identified in this study are found in Table 3
Currently, there is limited data on what may influence the knowledge, attitudes, beliefs, and behaviors (KABB) of primary healthcare providers regarding deprescribing in Canada with no studies published on the topic in the Canadian province of Nova Scotia. 24 This is an increasingly relevant issue due to the proportionately older population residing in this geographic area who are more likely to be taking a greater number of medications. 8 In primary healthcare in Nova Scotia, a variety of healthcare providers may be involved in medication management and deprescribing, most commonly family physicians, nurse practitioners (NPs), and pharmacists. In this system, family physicians may work in solo, group, or collaborative family practice teams (including family physicians, NPs, family practice nurses, and other healthcare professionals working together to provide comprehensive care for patients). NPs generally work in collaborative family practice teams, and pharmacists most often work in community pharmacy settings with a small number of pharmacists in collaborative practice teams. A few studies have previously investigated physician perspectives on deprescribing in different jurisdictions15,20,25 and that of physicians and either pharmacists or nurses;15,26,27 however, no previous studies have used the TDF(v2) to explore the perspectives of family physicians, NPs, and pharmacists in primary care in a single study.
A local contextual understanding of physicians’, NPs’, and pharmacists’ perceived influencers on their deprescribing behaviors will help inform the types of interventions to support deprescribing practices in primary healthcare. Therefore, this study aimed to describe the KABB that influence deprescribing for primary healthcare providers (family physicians, NPs, and pharmacists) within Nova Scotia using the TDF(v2) and COM-B models.
Methods
This research employed a qualitative design to explore healthcare providers’ (HCPs) KABB around deprescribing using one-on-one interviews 28 and focus groups. 29 The analysis was framed and guided by the TDF(v2) and BCW allowing for the systematic organization and identification of relevant data18,19 and findings. Our study included the following three steps.
1. Interview guide development
An interview guide that was used for both interviews and focus groups was developed through a review of the literature and team discussion.20,30,31 The guide was reviewed by three healthcare providers to assess quality, accuracy, and appropriateness of questions and was piloted with a mock focus group. (Additional details in Supplemental Appendix 1).
2. Collection of data using focus groups and semi-structured interviews
Sampling and participants
A purposive sampling method was employed to identify participants from the HCP groups—family physicians, NPs, and pharmacists. This sampling process allowed the selection of participants from both rural and urban settings who had direct experience with prescribing/deprescribing and could provide in-the-field insights. To be eligible, the individual must have met the following inclusion criteria: speak and understand English; be a primary healthcare provider working in Nova Scotia in a community setting, which may include a collaborative care team, community pharmacy, or university-affiliated community-based teaching unit; and have been employed in their current position for a minimum of 1 year. Potential participants for both one-on-one interviews and focus groups were identified by members of the research team and then further expanded by the snowballing technique 32 and by contacting stakeholders (e.g. professional associations). Those who expressed interest in the study were sent a formal email invitation with a copy of the consent form and participant information sheet.
Focus group and interview procedures
Three focus groups, one with each HCP group (involving three to four individuals), were conducted in person in Halifax, Nova Scotia. Nine one-on-one interviews were conducted by phone with HCPs from rural areas. Although data saturation was not assessed, it was expected that this number of participants would provide sufficient preliminary data to assist the research team in planning for larger studies on deprescribing. Participants reviewed and signed consent forms and provided verbal consent prior to the interview. Interviews and focus groups were led by a female Masters Student Research Assistant (HM) trained and experienced in conducting and analyzing qualitative interviews. The interviewer was in contact with participants via email and/or phone prior to the interviews and focus groups to establish a contact relationship. One-on-one interviews lasted between 30 and 60 minutes, and focus groups lasted between 60 and 90 minutes. All sessions were audio-recorded and transcribed verbatim by two research assistants (HM, ES).
3. Use of the TDF framework to identify key domains and generate subdomains or specific beliefs
To enhance trustworthiness of the findings, a four-stage analytic data approach was used:
Stage 1: Three team members (NKK, JEI, HM) independently reviewed one transcript and achieved consensus on the definitions and associated examples of each of the 14 domains of the TDF(v2). 18 Based on this initial review, a coding scheme was developed, and codes were clarified among the team members to ensure consistency.
Stage 2: A larger team assisted in coding the transcripts (HM, NKK, JEI, RMM, AW, FB, SB, OK). One team member was designated as the primary coder for each transcript and read the transcript to identify pertinent sections from participant responses that were considered relevant to deprescribing and then assigned the most applicable TDF(v2) domain based on the coding scheme developed. Codes were also classified as barriers or facilitators to deprescribing. Another team member was designated as the second coder who reviewed for any additional codes, and this was followed by a third team member who reviewed the final coding. Any discrepancies were discussed and resolved. The involvement of multiple team members in the coding allowed the data to be analyzed from a variety of perspectives. Coded data were entered into NVivo 9 (QSR International Pty Ltd. NVivo qualitative data analysis Software, 2012) and analyzed to identify the key TDF(v2) domains that were most influential based on the highest frequency coded and the content of the responses. The TDF(v2) domains that represented the most prevalent domains for all HCP groups were identified.
Stage 3: Two team members (HM, RC) collaboratively analyzed the data within each of the top TDF(v2) domains from Stage 2 to develop themes that were identified as subdomains associated with behaviors related to deprescribing. A subdomain was defined as a group of responses which represented a similar topic (e.g. specific belief). Two additional team members (NKK, JEI) then reviewed the analysis and with the two initial reviewers came to consensus on subdomain themes.
Stage 4: TDF(v2) domains and subdomains were then organized according to the COM-B framework (as presented in Table 1) to improve usability for stakeholders and translation into practice.
The consolidated criteria for reporting qualitative research (COREQ-32) were used to report important aspects of the research team, study methods, context of the study, findings, analyses, and interpretations 33 (Supplemental Appendix 2).
Ethical approval was received from the Nova Scotia Health Authority Research Ethics Board (Approval No. 1022515).
Results
Participants
A total of 19 participants (14 female, 5 male)—six family physicians, seven NPs, six pharmacists—were recruited from urban and rural Nova Scotia practice settings (Table 2). The nine participants who completed one-on-one phone interviews practiced outside the urban center of Halifax, Nova Scotia, Canada. The 10 participants who completed focus groups all practiced in Halifax. No participants refused participation or dropped out after providing consent. More specific demographic data were not collected to protect anonymity given the small number of participants and relatively small size of the province.
Participant demographics.

Summary of findings within the analysis
Although all 14 domains of the TDF(v2) were coded in the data, the six that appeared to be most influential based on the frequency of codes and content of the responses for all participants were the following: (1) Social Influences, (2) Environmental Context and Resources, (3) Memory, Attention, and Decision Processes, (4) Social/Professional Role and Identity, (5) Intentions, and (6) Beliefs about Consequences. Within each TDF(v2) domain, subdomain themes were also identified. Table 3 presents the specific belief themes for each TDF(v2) domain related to the components of the COM-B model along with supporting quotes.
COM-B with associated TDF(v2) domains and rankings (by prevalence) linked to subdomains and sample quotes from primary care providers in Nova Scotia.

MD: family physician; NP: nurse practitioner; PhC: pharmacist; FG: focus group.
MD, NP, or PhC followed by a number indicates the interview identification number for a person from that professional group.
COM-B: Capability, Opportunity, Motivation, Behavior from the Behavior Change Wheel.
TDF(v2): Theoretical Domains Framework version 2 domains identified from the data.
Ranking: The rank order to the key TDF domains that appeared to be most influential based on the frequency of codes and content of the responses for all participants.
Subdomain: a group of responses within the TDF domain that were identified to have a similar belief.
Capability
Memory, Attention, and Decision Processes was the TDF(v2) domain related to
There were differences between the three HCP groups in what they emphasized in their deprescribing process. Family physicians described their decision process and triggers for initiating deprescribing. NPs tended to describe their process of discussing deprescribing with patients. Pharmacists tended to indicate how they identified opportunities for deprescribing and noted that they would need to collaborate with prescribers to initiate the deprescribing process.
Opportunity
Social Influences and Environmental Context and Resources were the most prominent TDF(v2) domains within
Related to Environmental Context and Resources, participants mentioned available deprescribing resources, such as Beers Criteria®, 34 Sleepwell, 35 and Deprescribing.org 36 that supported them in the deprescribing process. Participants also noted that there was a lack of tools for younger patients. Participants mentioned that having prompts built into electronic medical record systems, although not presently available, would help trigger them to deprescribe.
Access to updated and accurate patient and medication information was also reported as an important component for deprescribing. Pharmacists noted that they did not have the same level of access to patient information as other HCPs and advocated for improvements in the system of communication with prescribers to better support deprescribing.
Some participants indicated that lack of adequate or optimized staffing was often a barrier to deprescribing. Lack of staff, for example, to keep medical records up-to-date was a barrier, optimal use of staff, for example, pharmacy technicians in the community pharmacy, or access to a pharmacist in a collaborative practice were seen as facilitators. Some family physicians who had previous exposure to the long-term care setting noted that there is a workflow for deprescribing in long-term care which is not present in the primary healthcare setting. These participants also felt that practice standards for routine (i.e. every 6 months) medication reviews in long-term care, if adopted in primary healthcare, could serve to facilitate deprescribing.
All participants mentioned a lack of time, including the limited patient visit time and the time required for reviewing medical records and monitoring and follow-up appointments, was a barrier. They indicated that they would deprescribe more often if they had the time. Reimbursement was an issue for pharmacists, who noted that there is no formal reimbursement method. This was reported as not an issue for NPs as they are salaried; however, some family physicians noted that remuneration dedicated to deprescribing would be an incentive.
Motivation
Social/Professional Role and Identity, Intentions, and Beliefs about Consequences were the most common TDF(v2) domains related to
Related to Intentions, participants described specific triggers or opportunities to deprescribe, and these were associated with the Memory, Attention, and Decision Process domain. The most common triggers or opportunities identified included patient factors, such as age (e.g. older adults), specific medication classes (e.g. proton pump inhibitors, benzodiazepines, antihypertensives, statins, antidepressants, antipsychotics, and opioids), polypharmacy, medication non-adherence, and changes in health status (e.g. experiencing adverse effects, falls, and recent hospital discharge). Participants reported that deprescribing was always on their minds and they actively looked for opportunities to deprescribe.
Related to Beliefs About Consequences, participants’ beliefs about the consequences of taking medications and belief that some medications may be inappropriate in certain situations were identified as a facilitator of the deprescribing process. Participants also expressed the need to always weigh the benefits of deprescribing (e.g. reduced pill burden, medication costs, adverse effects, and drug interactions) with the potential consequences of stopping the medication (e.g. withdrawal reactions and relapse of symptoms). They indicated this frequently added complexity to the deprescribing process and were associated with the Memory, Attention, and Decision Process domain.
Discussion
This study applied behavioral change theory, the TDF(v2) and BCW, to generate an understanding of the KABB that influence deprescribing for primary healthcare providers. The findings demonstrated that family physician, NP, and pharmacist participants have an awareness of and perceived inherent role in the deprescribing process, with the active intention to identify opportunities to deprescribe medications. Some participants felt that their deprescribing process could be more systematic and could be better supported by environmental factors, such as access to complete information, alerts/prompts, adequate time, and reimbursement. Participants also identified that social influences, such as collaborative relationships with patients and other healthcare providers, were key factors in supporting deprescribing practice.
Opportunities (physical and social) to perform deprescribing were identified as influential barriers and facilitators. Interestingly, these speak to influences that are external to healthcare providers and suggest the need for consideration of enablers and barriers not only at the individual level but also at a practice and system level to facilitate deprescribing. The need for policy and changes at the practice and system level is beginning to be described.37,38 A recently released National Strategic Action Plan in Australia on the quality of medicines in older adults recommends action items at an individual/public, healthcare professional, healthcare organization, and environment level. 39 Future strategies should consider the various levels that may influence deprescribing in practice.
The need for a systematic approach to deprescribing was identified as a means to facilitate inclusion in practice. A five-step patient-centered deprescribing process has been described 14 which can be initiated at any time in the patient’s care.5,14,40 Participants noted that the deprescribing process can be complex and time-consuming, involving communication with the patient and a plan for tapering and monitoring. Communication with patients using a shared decision-making approach has been suggested. 16 To initiate the deprescribing process, specific triggers (e.g. medications or patient status) are required to identify an opportunity to deprescribe. This approach could be reactive, in the case of a patient experiencing a potential adverse effect or being admitted to hospital, or proactive, in the case of a routine medication review or reassessment when refilling a medication. Studies have targeted specific patients (e.g. those with polypharmacy, older adults)41,42 or specific medications (e.g. benzodiazepines,43,44 proton pump inhibitors 45 to identify deprescribing opportunities. Clearly understanding and supporting these types of triggers will be important to consider when designing deprescribing interventions.
The role of patients, as a social influence, was found to be both a facilitator and barrier to the deprescribing process. The importance of patients and families as social influences was also reported by Ailabouni et al. 20 Barriers to deprescribing reported by patients identified by Reeve et al.5,14 included “Appropriateness” of the medication, the “Process” of deprescribing, including lack of physician time to support the procedure, “Influences” (family, HCPs, and friends), and “Fear” of return of symptoms and withdrawal. Despite clinicians reporting patients as a barrier to deprescribing, quantitative research has found that the vast majority of older adults are willing to have a medication deprescribed if their doctor said it was possible;46,47 however, the impact of recommendations by other HCPs, such as NPs or pharmacists, is less clear. Providing further support to the potential role of patients in facilitating deprescribing are two studies that specifically engaged and targeted patients as leaders in the deprescribing process with positive results.43,44
Collaboration and mechanisms to support collaboration (e.g. communication systems and electronic medical records) were felt to facilitate the deprescribing process. Access to support services has been identified as an enabler by general practitioners (GPs) in previous studies.15,25 Specifically, pharmacists were involved in performing medication reviews to identify deprescribing opportunities and to be a resource to support GPs’ decisions. In addition, access to specialists for decision support has been previously reported as an enabler but may also be understood as a barrier. Anderson et al. 15 reported that underdeveloped interprofessional relationships between healthcare providers (e.g. between GPs and pharmacists or GPs and specialists) hampered the deprescribing process, largely due to poor communication and insight into each other’s decision-making. Specialists have also been reported as influential in deprescribing decisions both for patients and prescribers.15,48 A comprehensive approach that includes more than one method to reduce inappropriate prescriptions and the combined efforts of multiple healthcare providers is needed to reduce polypharmacy and facilitate deprescribing. 49
Collaboration among healthcare providers in the deprescribing process including pharmacists and nurses to support physicians and NPs in tasks related to deprescribing was advocated by participants. From the literature, pharmacists have supported the deprescribing process by performing systematic medication reviews and providing recommendations to prescribers.42,50 –53 In these studies, pharmacists were either integrated into primary healthcare practices or were community-based pharmacists. A community pharmacist led intervention in which pharmacists sent patients an educational deprescribing brochure and a pharmaceutical opinion (which included why and how to deprescribe) to the physician resulted in less prescription renewals; 43% prescription renewals ceased for patients who received the educational intervention compared with 12% who received usual care. 43 The role of registered nurses and NPs in deprescribing in primary healthcare has not yet been well described. However, in a survey of community dwelling older people’s attitudes toward deprescribing, 42.6% expressed they would be comfortable having a nurse involved in stopping medications and follow-up. 47
Environmental context and resources was also a prominent domain for participants in this study and also been described in previous studies for GPs.20,25 Specifically, a lack of evidence-based guidelines, decision support systems, and data to quantify the benefits and harms of deprescribing were identified as potential barriers to deprescribing.15,20,25 In contrast, participants in this study indicated that the available guidelines (e.g. deprescribing.org) and tools (e.g. STOPP/Beers Criteria) were enablers to deprescribing in their practices. This speaks to the significant work done recently in Canada to develop and disseminate evidence-based tools to support clinician’s deprescribing practices. 54
Our study confirms findings from previous studies on the environmental context and resources concerns around lack of time, multiple competing demands, and insufficient reimbursement for deprescribing for physicians15,20,25,48,55 and expands on it, highlighting these may also be issues for pharmacists and NPs. In addition, a lack of complete and accurate medication information was also reported to hinder the deprescribing process, and the integration of electronic health records across the system of care is likely to help address this barrier. At the time of the study, a Drug Information System had been implemented in the province; however, only community pharmacies were required to use it and it did not include information (diagnoses, history) that may be required for deprescribing. Electronic health records are planned and may in the future support identified issues related to access to patient information.
One strength of this study was that it used the validated TDF(v2) to identify influencers that were most relevant to the deprescribing process for participants. The qualitative data analyzed using TDF(v2) domains will inform the development of future interventions through the BCW ensuring a systematic and theory-driven process-based approach. Another strength of this study is the inclusion of a variety of healthcare providers from primary healthcare. Although barriers and facilitators to deprescribing have been reported previously for some professions (GPs and consultant pharmacists),15,20 they have not previously been reported for community pharmacists or NPs. This study has provided information on influencers on deprescribing using a behavior change lens grounded in the BCW. This provides a foundation for further study that can link the results to the intervention functions within the BCW and then to specific behavior change techniques.
There are several potential limitations to this study. Participants were identified due to their interest in deprescribing. Therefore, these participants were motivated and committed to deprescribing and our findings may not be transferable to other HCPs in primary care in Nova Scotia. However, the results may still help identify potential barriers and facilitators for HCPs who have not yet been able to engage in deprescribing practice more widely. An interprofessional focus group was not possible due to logistical issues (i.e. provider time), which may have prevented learning more about potential similarities and differences in beliefs of the different professional groups. To prioritize study findings, the team employed a method of identifying the most influential TDF(v2) domains based on the frequency of codes and content of the responses. This assumes that the most important factors were those discussed the most; however, the most common ones that are generally known/agreed upon may not be discussed as much and other less commonly discussed domains may also be relevant in some situations. Finally, this study was conducted in one Canadian province and findings may not be transferable to other provinces or countries due to differences in populations and healthcare systems. However, as many results are similar to findings in other jurisdictions, strength is added to the applicability of results outside Nova Scotia.
Conclusion
This study of family physicians, NPs, and pharmacists in the primary care setting in Nova Scotia, Canada identified many factors that influence their deprescribing. Deprescribing was felt to be part of the scope of practice of all participants but barriers often precluded implementation. Our results suggest that a systematic approach to deprescribing in primary care should be supported by opportunities for patient and healthcare provider collaborations, as well as practice and system level enhancements to support sustainability of deprescribing practices. This study provides foundational contextual information that may improve the development and implementation of sustainable deprescribing strategies in primary care.
Supplemental Material
Appendix_II_COREQ_Checklist – Supplemental material for Influencers on deprescribing practice of primary healthcare providers in Nova Scotia: An examination using behavior change frameworks
Supplemental material, Appendix_II_COREQ_Checklist for Influencers on deprescribing practice of primary healthcare providers in Nova Scotia: An examination using behavior change frameworks by Natalie Kennie-Kaulbach, Rachel Cormier, Olga Kits, Emily Reeve, Anne Marie Whelan, Ruth Martin-Misener, Fred Burge, Sarah Burgess and Jennifer E. Isenor in Medicine Access @ Point of Care
Supplemental Material
Appendix_I_Interview_and_Focus_Group_Guide – Supplemental material for Influencers on deprescribing practice of primary healthcare providers in Nova Scotia: An examination using behavior change frameworks
Supplemental material, Appendix_I_Interview_and_Focus_Group_Guide for Influencers on deprescribing practice of primary healthcare providers in Nova Scotia: An examination using behavior change frameworks by Natalie Kennie-Kaulbach, Rachel Cormier, Olga Kits, Emily Reeve, Anne Marie Whelan, Ruth Martin-Misener, Fred Burge, Sarah Burgess and Jennifer E. Isenor in Medicine Access @ Point of Care
Footnotes
Acknowledgements
The authors would like to thank Heather MacLean and Ellie Salsbury for their assistance in completing the interviews, transcriptions, and coding.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded through a Dalhousie University Faculty of Health Research Development Grant and grants from the Drug Evaluation Alliance of Nova Scotia (DEANS). The funders had no role in data collection, analysis, data interpretation or in writing or submission of the article.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.