
Abstract
Introduction:
Higher levels of health literacy improve utilization of health information, medication adherence and outcomes. Few studies evaluate the utility of medicines information in hypertensive care in settings with low health literacy.
Aim:
To determine the level of health literacy and utility of medicines information leaflets (MILs) among hypertensive patients in public health care in Namibia.
Methods:
A hospital-based survey among hypertensive patients receiving care at a referral hospital in Namibia from the 8 June 2018 to 29 June 2018. Patient’s health literacy and utility of MIL were assessed using three literacy tools and a survey questionnaire. Quantitative data were analysed using descriptive statistics and qualitative thematic content analysis for factors associate with the utility of the MIL.
Results:
Of the 139 patients, 63% were female and the mean age was 45.7 (range: 19.0–84.0) years. Over 85.6% had of low literacy skills (Rapid Estimate of Literacy in Medicine (REALM) score <44, that is, unable to read simple health materials), 38.8% had positive Single Item Literacy Screener (SILS) scores (⩾2, require help to read medicines information) and 66.9% had inadequate skills for comprehension, appraisal and decision-making with regard to health information (Health Literacy Skills Instrument-Short Form (HLSI-SF) score <70%). The level of access to and utility of MIL were low, 32.4% and 34.6%, respectively. The main factors associated with poor utility of the MIL were low patient health literacy, lack of guidelines on the use of MIL and MIL written in non-native languages.
Conclusion:
Low rates of health literacy and utility of MIL were observed among hypertensive patients in Namibia. The integration of health literacy programmes, and MIL guidelines are needed to promote utility of medicine information and improve medication adherence.
Introduction
Inadequate literacy is a major barrier to access to public health care, particularly among patients in sub-Saharan Africa.1 –3 Current evidence suggests that limited literacy negatively impacts on a wide array of health outcomes, including childhood health, mental health and in patients with chronic diseases.4 –6 However, there are limited data on the impact of health literacy on the utility of medicine information among hypertensive patients in the sub-Saharan Africa where the burden of the disease is highest.7,8
Over half (9.4 million) of deaths due to cardiovascular diseases (CVDs) globally are linked to hypertension, the majority of which are among patients in low- and middle-income countries (LMICs) in the sub-Saharan Africa.9,10 With an estimated prevalence of 45%, Namibia has one of the highest burden of hypertension in sub-Saharan Africa.11 –13 This is a concern given the universal access to cost-free hypertensive care and medicines in Namibia. Nashilongo et al. 14 estimated that 58% of hypertensive patients in the suburbs of Windhoek do not adhere to their medication. These findings concur with the World Health Organization (WHO) estimates that over half of patients do not use their medication correctly.15,16 Moreover, adherence to antihypertensive medication is critical in the prevention of cardiovascular complications. 17
Several studies identified low health literacy rates among hypertensive patients as a major risk factor for sub-optimal utility of medicine information, medication adherence and blood pressure control.1,13,18,19 The WHO describes heath literacy as the ability to engage with health information and services.20 –22 This requires patients to access, comprehend, critique and use health information and services to make health-related decisions such as adhering to medicines prescribed. 20 A study across 14 sub-Saharan countries based on data from national demographic surveys estimated health literacy rates to range from 4% to 65.7%, with Namibia having the highest rate.6,23 This is helped by the fact that in 2015 the National Health Literacy Programme of Namibia estimated over 76% enrolment into adult literacy programmes. However, a study by Likando et al. challenges that adult literacy rarely translates into functional literacy to independently perform tasks such as improving medicine use based on the information contained in medicine leaflets.24 –26. Sub-optimal utility of medicines information is a public health concern in patients with chronic non-communicable diseases (NCDs) such as hypertension that require adequate levels of health literacy for medication adherence and self-care.19,27,28
The implementation of the United Nations Sustainable Development Goals (SDGs) in most countries in sub-Saharan Africa has enhanced access to universal health literacy programmes and the utility of medicines information.1,29,30 In Namibia, the National Human Rights Action Plan, Namibia patient’s charter and the Medicines and Related Substance Control Act provide a legal framework for patients to the right to access information on treatment and medicines information leaflets (MILs).31 –33 In this legal framework, all patients who receive health care are entitled to obtain MILs written in the official language that includes basic information on the medicine. For patients to effectively utilize MIL requires adequate level of health literacy, that is, the ability to read and comprehend medicines information with limited support and make decisions regarding to their health.34,35 Several studies give conflicting information on the utility of MIL in LMICs, some indicating low and others high utility.35 –38
Nevertheless, despites the relatively high adult literacy rates in Namibia, there are limited data on the health literacy levels (reading, comprehension and numeracy of health materials) and its impact on the utility of medicines information in public health care. Consequently, the study sought to address this by assessing the level of health literacy, access to, and utility of, MIL, among hypertensive patients and professionals at public health facilities in Namibia. The findings can be used to guide future policies for equitable access to medicines information at the point of care among public health facilities across Namibia as well as across sub-Saharan Africa.
Methods
Study design and population
The study consisted of two surveys, one among hypertensive patients and the other among health care professionals. The first survey assessed the levels of health literacy and utility of the MIL among hypertensive patients. This was conducted at Katutura Intermediate Hospital (KIH), a tertiary referral hospital from 8 June 2018 to 29 June 2018 using patient exit interviews. The hospital has annual turnover of 7000 patients on medication for NCDs including antihypertensive medication. A sample of 185 patients was estimated using Leslie Kish method.39,40 The study included only patients on antihypertensive treatment with at least one medication for a period of 3 months or more and gave written consent to participate. The study excluded patients who did not consent to participate, too sick to participate and/or unable to communicate due to language barrier (Figure 1).

Sample selection for inclusion of patients in the study.
Second, a survey was conducted among healthcare professionals (HCPs), that is, pharmacists, pharmacists-assistants and nurses, involved in dispensing antihypertensive medication, HCPs were interviewed using a semi-structured questionnaire to assess the factors associated with access to, and utility of, the MIL. The questionnaire assessed perceptions regarding the need, usefulness, availability, benefits and barriers to using the MIL.
Data collection procedure
Data on access to, and utility of, the MIL and associated factors were collected from hypertensive patients receiving care at the outpatient department of KIH. Patients were systematically (i.e. every third patient) recruited over the study period based on daily attendance registers. Patients were interviewed for access and utility of the MIL using a semi-structured questionnaire and health literacy using three tools. These were the Single Item Literacy Screener (SILS), Health Literacy Skills Instrument-Short Form (HLSI-SF) and Rapid Estimate of Literacy in Medicine (REALM) tools (see below). The three health literacy tools were subsequently assessed for comprehension, reading skills and numeracy skills. All the tools were piloted among 10 patients receiving antihypertensive care at the Intermediate hospital between 22 May 2018 and 24 May 2018 for suitability of the question items using semi-structured interviews. The face validity of the tools was subsequently established by the research team (S.M., D.K., E.H.) using 10 questionnaires for appropriateness of question items and standardized prior to the conducting interviews. Interviews to assess for health literacy and utility of the MIL were conducted in English. For some patients, the questionnaires on utility of the MIL were interpreted in Afrikaans and Oshiwambo, two widely spoken local languages in Namibia. Each interview lasted between 20 and 30 min per patient.
In addition, data were collected from the HCPs involved in the prescribing and dispensing of antihypertensive medication at the hospital. Data were collected using structured questionnaire interviewer-administered interviews that assessed for factors associated with the MIL and to promote access and utility of the MIL in antihypertensive care at the hospital. The study only included HCPs involved in hypertensive care and were on duty during the study interview.
Health literacy assessment tools
The level of health literacy among the hypertensive patients was assesses using three tools (REALM, SILS and HLSI-SF), which assess different dimensions of health literacy. The REALM assessed for the basic reading skills (literacy), the SILS assessed for the need for the support when reading health-related materials and the HLSI-SF assesses for comprehension and health seeking behaviours. A combination of three tools was used because no single tool comprehensively assess all the dimensions of health literacy.
First, the REALM tool assess the patient’s ability to read medicine information.41,42 The REALM tool consists of 66 health terms. The patient is scored with a point for the number of words that they read and pronounce with a maximum of 66 points. REALM scores 0–18 indicate that a patient is unable to read easy health information, 19–44 indicate that patients are only be able to read simple materials and a score above 44 indicates that the patient is able to read and understand health information. In this study, a REALM score of less than 44 was regarded as low literacy and unable to read or utilize information on the MIL.
Second, an SILS tool was used to assess the patient’s need for support in reading health-related materials. 43 Patients responded to a single question item ‘How often do you need to have someone help you when you read medicine information leaflets, or other written material from your doctor or pharmacy?’ The SILS is scored with 1 (never), 2 (rarely), 3 (sometimes), 4 (often) and 5 (always). Negative SILS score (⩽2) indicates that the patient never or rarely needs help when reading health-related materials, while a positive SILS score (>2) indicates that a patient experiences difficulty in reading health-related materials and requires support.
Third, a 10-item HLSI-SF assesses patient’s comprehension, numeracy, health information seeking, decision-making and navigation skills. 44 The HLSI-SF assessment requires patients to read a pre-designed MIL (print-prose), listen and correctly respond to recorded voices. The HLSI-SF is designed to measure patient’s ability to remembered and understand information they read on the print-prose, and find health information they need on printed documents. The tool also measures the ability to proficiently interpret figures and doing simple calculations according to the quantitative aspects of the print-prose, to remember and understand the information they heard or explain the health issue to an HCPs, ease to find the health information they needed and reason out concepts. Each correctly answered item on the HLSI-SF is scored one point and the incorrect zero. A percentage HLSI-SF score ⩾70% is considered as an adequate level of health literacy, >80% proficient, 70%–80% basic and <70% below basic.
Data analysis
The primary outcomes of the study were level of health literacy (reading, comprehension and numeracy) and utility of MIL among hypertensive patients. The secondary outcome was the factors associated with the utility of the MIL in hypertensive care. Quantitative data on health literacy, utility and access to MIL were entered in EpiData v3.1 software for management and exported to SPSS v23 software for descriptive analysis. The REALM assessment graded health literacy as adequate for a score of ⩾44, SILS ⩽ 2, that is, no need for assistance to read the MIL and 70% for HLSI-SF for comprehension, numeracy and decision-making. The factors associated with the utility of MIL were analysed qualitatively using content thematic analysis using manual colour coding to generate themes and subthemes. The level of access to MILs was estimated, respectively, by the proportion (%) of patients that ‘always’ received a MIL for their antihypertensive medication as required by the Medicines and Substance Act of Namibia. ‘Do you always receive the leaflets for your medication?’ The level of utility of MIL was determined by the proportion of patients (%) that self-reported that they have ever made reference to the MIL with regards to their antihypertensive medication. The HLSI-SF was assessed for construct validity in the Namibian population using factor analysis.
In addition, data from HCPs were qualitatively analysed using content analysis for themes on the factors associated with, and potential strategies, to improve access and utility of MIL in antihypertensive care at the health facility.
Ethics
The study was approved by Research and Ethics Committees of the Ministry of Health and Social Services and Katutura Intermediate Hospital (MoHSS042018). All respondents gave a written informed consent and confidentiality of data was maintained through anonymizing of questionnaires by use of codes rather than patient identifiers and all questionnaires secured at the University of Namibia.
Results
Characteristics of study populations
Of the 185 target sample, 139 hypertensive patients were recruited giving a response rate of 75.1% (n = 139/185). The majority of the patients were female (61.2%) and were not formally employed (63.3%). The average age was 45.7 years (range: 19.0–84.0), the majority not married (58.3%) and attained at least primary level education (54.7%, that is, grade 10). Of the 139 patients, 90.6% were on follow-up visits, 18% had diabetes mellitus and 5.8% HIV/AIDS (Figure 2). Of the 139 patients, the majority were prescribed hydrochlorothiazide/amiloride (74.8%, that is, co-amiloride®) or amlodipine (49.6%) for their hypertension. Low dose aspirin (14%) and metformin (14%) were the most prescribed co-medications (Figure 3).
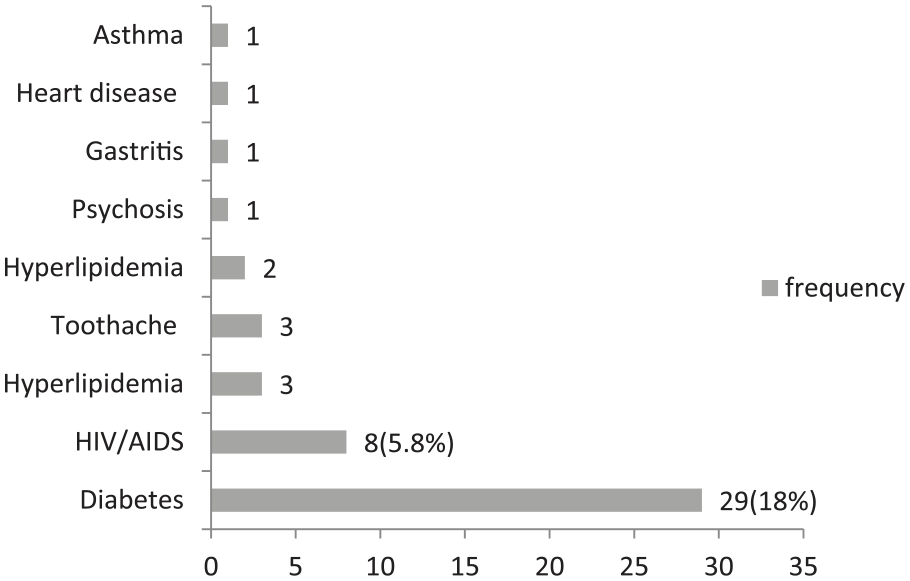
Co-morbidities among hypertensive patients at Intermediate hospital Katutura.
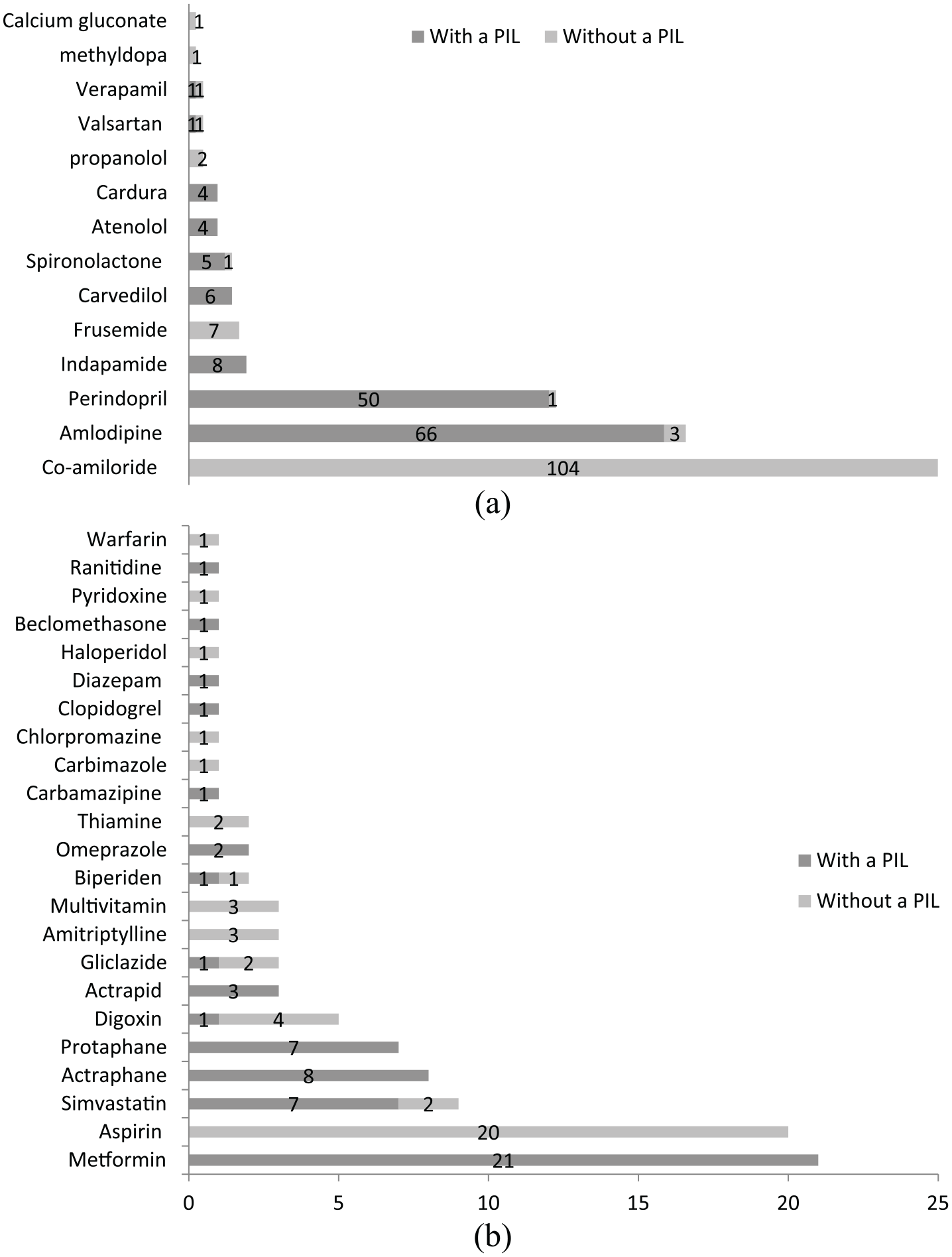
(a) Antihypertensives dispensed with medicine information leaflet. (b) Other chronic medication dispensed with or without a MIL.
Of the 14 HCPs recruited, 57.1% were females. The mean age and working experience of the HCPs was 34.1 ± 7.0 (range: 25.0–52.0) and 10.8 ± 7.3 (range: 2.0–30.0) years, respectively.
Health literacy among hypertensive patients
Of the 139 patients, 85.6% were unable to easily read medicine information (REALM score: 0–18) and 14.4% were only able to read simple materials (REALM score: 19–44) (Table 1). None of the patients were able to read complex health information such as MILs, that is, none had a REALM score ⩾44.
Patient access and use of MIL.
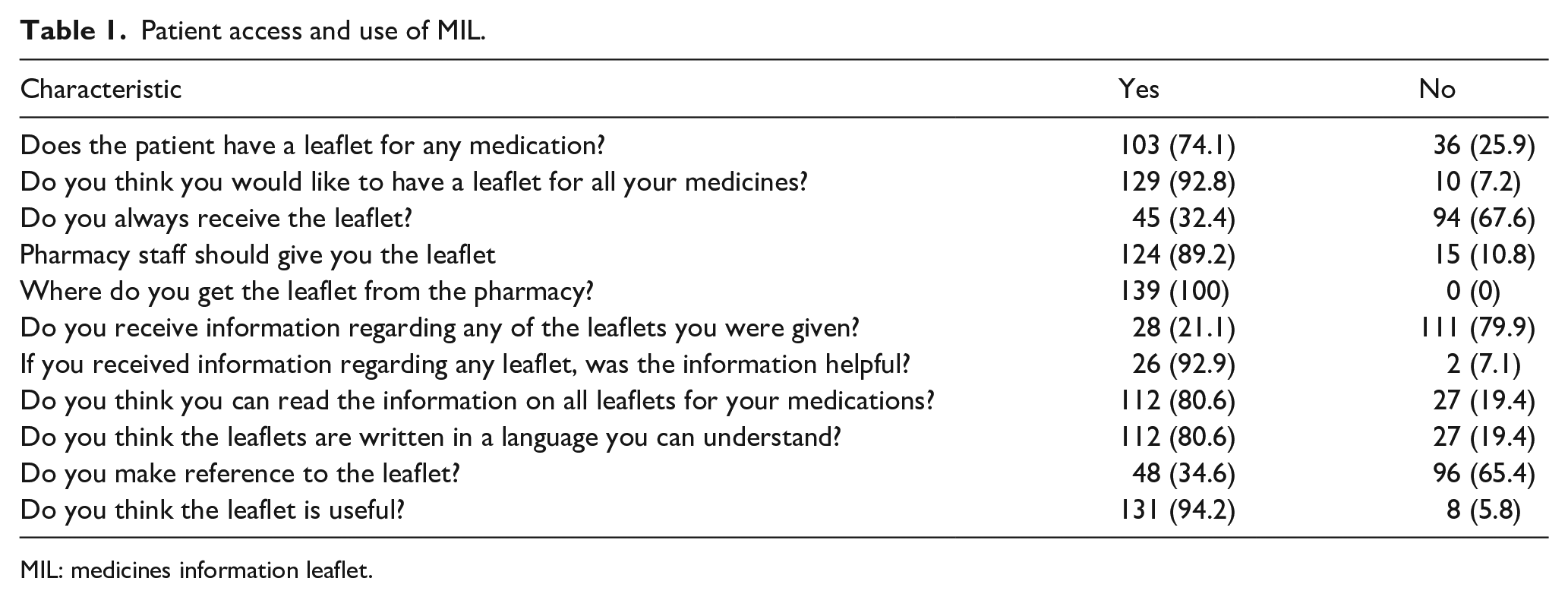
MIL: medicines information leaflet.
On the SILS assessment, 38.8% (n = 54/139) of the patients had positive scores (>2), that is, they have limited reading ability and they need support when reading medicine information. These patients experience difficulty in reading health-related materials and would require support (Table 1).
On average, patients had a health literacy level on HLSI-SF assessment of 58.5% ± 18.5% (range: 16.7%–100%). In addition, 66.9% of the patients had inadequate health literacy (HLSI-SF score <70%, Figure 4). That is, two-thirds of patients had limited ability to comprehend, communicate and make decisions regarding medicine information. In particular, 46% of the patients remembered and understood information they had read on the print-prose, 27.3% found health information they needed on printed documents and 42.4% proficiently interpreted figures and had performed simple calculations according to the print documentation. In addition, 47.5% of the patients remembered and had understood the information they heard or explained a health issue to an HCPs according to the oral domain and 25.2% easily found the health information they needed and reasoned out concepts according to the Internet domain (Table 1).

Health literacy level using the Health Literacy Skills Instrument-Short Form.
Access of MIL in hypertensive care
Of the 139 patients, 32.4% (n = 45) always receive a MIL for their antihypertensive medication at hospital (Table 2). The level of access of MILs for the antihypertensive medications was higher with amlodipine (44.5%) and perindopril (36%) compared to other medications. None of the patients received MILs for co-amiloride, the most used antihypertensive (Figure 3).
Patient study – qualitative analysis of patient access and use of MIL (n = 135).

MIL: medicines information leaflet.
This frequency or percentage was determined using a tally system to account for each option stated in a single quote, because within a single quote many options may have been stated.
Over 80% of the patients were aware of the right to access the MIL, but 74.1% had never requested for a leaflet. Most patients, 79.9% (n = 111/139), never received information on how and where to access, and instructions on the use of the MIL (Table 2).
Most HCPs had never received training on optimizing access to, and utility of, MIL (78.6%). HCPs were not aware of hospital-based policies/guideline to enhance the use of MILs (85.7%). However, 35.7% were aware of the national legal frameworks for the distribution of the MIL, 28.6% citing the Pharmacy Act. Of the 14 HCPs, 28.6% (n = 4) always dispensed antihypertensive medicines with an MIL. Most HCPs (64.3%) acknowledged the importance of MILs, that is, the MIL provides patients with more information on the medicines prescribed (57.2%), makes patients more knowledgeable and responsible (71.4%) and encourages patient involvement in treatment (28.6%) (Tables 3 and 4).
Patient study – health literacy as measured by the REALM, SILS and HLSI-SF.

REALM: Rapid Estimate of Literacy in Medicine; SILS: Single Item Literacy Screener; HLSI-SF: Health Literacy Skills Instrument-Short Form.
Themes generated from the qualitative analysis of healthcare worker suggested strategies to improve access and use of the MIL among patients (n = 14).
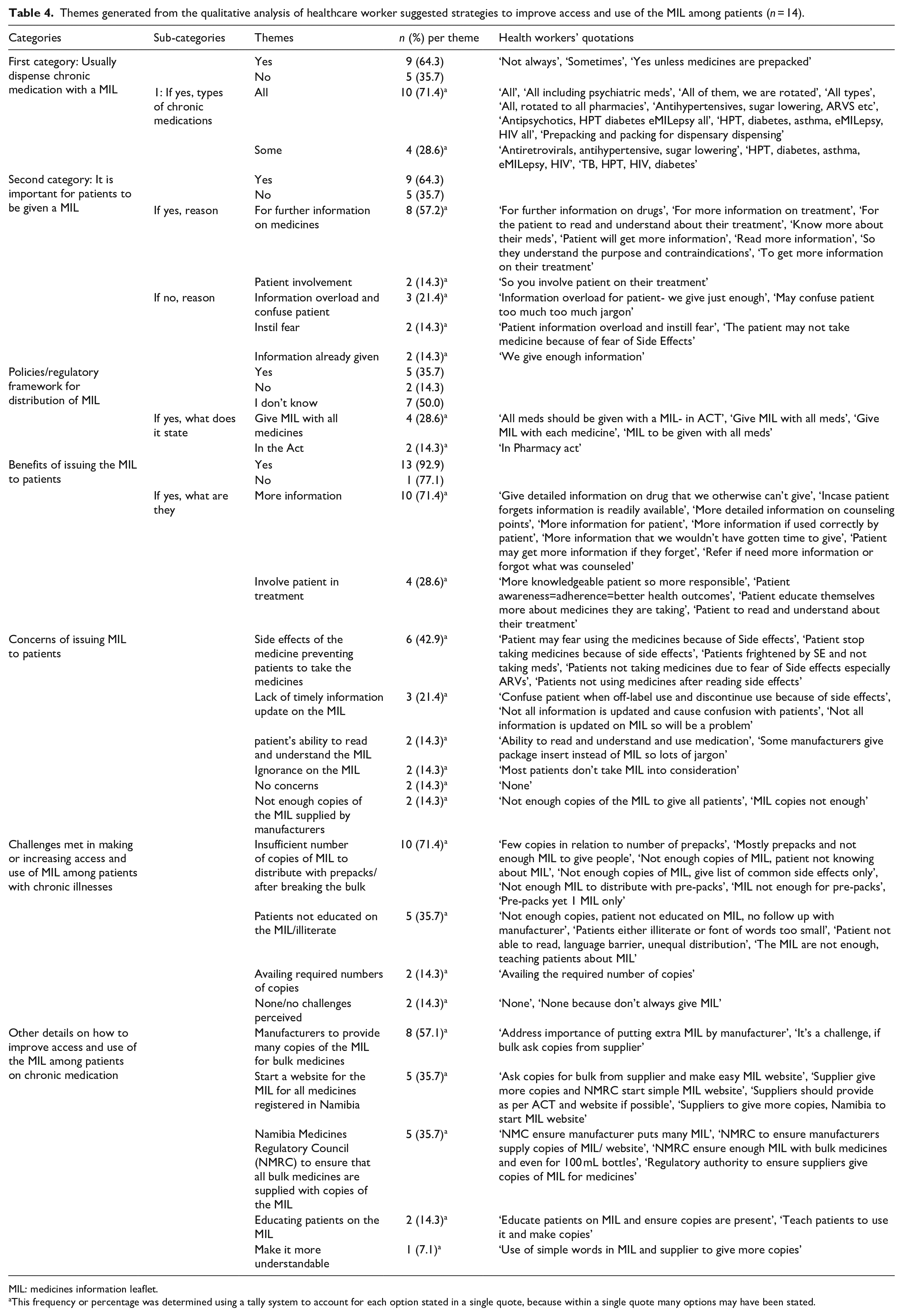
MIL: medicines information leaflet.
This frequency or percentage was determined using a tally system to account for each option stated in a single quote, because within a single quote many options may have been stated.
Utility of MIL in hypertensive care
Of the 139 patients, 34.5% (n = 48) always refer to the MIL. Of the 28 patients who received information on the use of the MIL, 92.9% found it useful. Overall, most patients perceive the MIL as useful (94.2%, n = 131/139), easy to read and understand (80.6%) and prefer to access the MIL from pharmacy professionals (89.2%) (Table 2). Patients who are unable to read and understand the information on the MIL typically requested assistance from a peer or a family member. ‘Although I cannot read English, I give my daughter to read for me always when I get it’. Most patients (67.6%) prefer using the MIL to other sources of medicine information because it is easy to manage or keep (66.9%).
Patients identified the most useful information on the MIL as the indications for the medicine (27.5%), storage instructions (22.9%), description of the medicine prescribed (19.8%) and dosage instructions (18.3%). Most patients preferred to receive the MIL from outpatient pharmacies professionals (79.1%) compared to doctors (12.2%) or other HCPs.
The main reason patients read the MIL was insufficient information on their medication from either the doctor or the pharmacist. ‘They don’t give us enough information on the medicine even the disease, especially the doctors like now you are telling me these medicines are for blood pressure but the doctor didn’t tell me about it’. ‘The pharmacy tells us more information about the medicine than the doctors but when I read the MIL I get more information’. ‘The pharmacy people do not have time to really explain, they just say how to take the medicine’. Moreover, 58.3% (n = 81/139) stated that the information on the MIL sometimes conflicts with that given at the hospital, and this requires further consultation with a doctor or pharmacist.
Factors influencing the access and utility of MIL
Most patients (60.4%) were not satisfied with the quality and amount of medicine information they received especially from physicians. Patients reported limited access to the MIL at the hospital pharmacy and proposed that ‘manufacturers provide many copies of the MIL for all medicines’ (52.5%), ‘pharmacy staff make a deliberate effort to give each patient a MIL’ (22.3%), ‘educate the patients’ (14.4%) and ‘make the MIL more understandable’ (11.5%) (Table 3).
Some HCPs (35.7%) disregarded the importance of giving MIL to patients citing, information overload causing confusion among patients (21.4%), the side effects listed in the MIL would instil fear among patients resulting in medicine discontinuation (14.3%) and they had already given patients enough information (14.3%). The HCPs’ concerns on the distribution of MIL to patients included the following: (1) the side effects of the medicines would prevent patients from taking their medicines (28.6%), (2) lack of up-to-date and objective information on the MIL (21.4%), (3) patient’s inability to read and understand the MIL (14.3%), (4) patients’ ignorance on the MIL (14.3%) and (5) not enough copies of the MIL supplied by manufacturers (14.3%) (Table 3).
Strategies suggested by HCPs to improve access to, and utility of, the MIL included the following: (1) manufacturers provide many copies of the MIL for bulk medicines (57.1%), (2) development of a website/electronic platform where MILs for all medicines registered in Namibia can be accessed (35.7%), (3) the Namibia Medicines Regulatory Council (NMRC) to ensure that all bulk medicines are supplied with copies of the MIL (35.7%), (4) the need for patient education on the MIL (14.3%) and (5) the MIL to be made more understandable (7.1%) (Table 3).
Discussion
We believe this is the first study to assess the level of health literacy, and utility of MILs, among hypertensive patients at a public referral hospital in Namibia. This is important since inadequate health literacy, access and the utility of MILs were seen among hypertensive patients in Namibia. The inability of hypertensive patients to access and utilize medicine information is a major public health concern given the high public health burden of hypertension and non-adherence to antihypertensive medicines in Namibia.7,8
Our study found low health literacy rates among antihypertensive patients using the three different tools, REALM, SILS and HLSI-SF. Over 85% antihypertensive patients are unable to read simple health information (REALM: 0–18), 38.8% require support to read materials (SILS > 2) and 66.9% have limited ability to comprehend and make decisions regarding health information (HLSI-SF < 70%). This is a concern given that the utility of medicine information, adherence to hypertensive medication and blood pressure control require health literacy. 45 Our findings concur with several studies in sub-Saharan Africa that found low and varying rates of health literacy among patients on chronic medication and its impact on medication adherence and blood pressure control.19,23,28,46 Several studies advocate that hypertensive patients in low-literacy settings require repeated oral instructions and materials with illustrations in addition to written materials to comprehend and optimally use the information on the MIL, and we will be addressing this in future activities in Namibia.
Second, the study found limited access to MIL at the hospital (32.4%). This is despite most patients being aware of their right to medicines information and the usefulness of MIL (Table 1). Moreover, access to MIL varied by the type antihypertensive medication. For example, none of the patients accessed MIL for hydrochlorothiazide/amiloride, the most prescribed antihypertensive. These findings are similar to another study which reported that very few patients receive MIL with their medications.47,48 Our study also found a low level of utility of the MIL among hypertensive patients in public health care (34.6%; Table 1), which is a concern given, as mentioned, the high prevalence of hypertension in Namibia. 8 The findings are comparable to a study conducted in Belgium which showed that MIL were infrequently read, that is, one out of every four patients. 49 The study in Belgium also reported that patients aged ⩾65 years always read the MIL while others never read the MIL, women read the MIL more often than men and the most frequently read parts of the MIL were on dosage and side effects. 49 Nevertheless, the majority of patients in our study acknowledge the importance of MIL in promoting medication adherence, health education, as a reference and complement limited or contradictory verbal information (i.e. appropriate use and storage) given at the hospital by various HCPs (Table 3). Our findings partly differ though from the study by Mottram and Reed that found that patients thought the section on storage conditions was of little importance. 50 In Namibia, patients argued that information on the storage conditions of medications was important because the weather varies widely throughout the year, which they believed may negatively impact on the efficacy of their medication. Encouragingly, several studies concur with our findings that access to appropriate, user-friendly medicine information that is easily read empowers patients regarding self-management and the safe use of medication for their NCDs.35,51 –53
Finally, the study also found that limited access to MIL in hypertensive care in Namibia was due to a number of logistical factors, that is, limited copies of MIL from manufacturers for bulk supplies; programmatic factors, that is, lack of guidelines/systems for the distribution of MIL at health facilities; and behavioural factors, that is, HCPs negative perception on MIL distribution to patients (Table 3). For instance, some HCPs believed that some patients may interrupt antihypertensive treatment if they become aware of serious adverse effects associated with their medication (Table 3). Our findings concur with those of Dixon-Woods et al. who reported that the use of MIL is greatly influenced by perceptions of individual patients, HCP’s role, the value of the leaflets, the quality of leaflets and the presence of appropriate topics that necessitate the use of the MIL. Similarly, Mottram and Reed 50 and Tong et al. 54 agree that the inclusion of information on adverse effects in the MIL impacts negativity on the use of medications among some patients. Similarly, the limited utility of MIL in this study was partly due to a low health literacy (28.1%) among the patients (Table 1); lack of awareness/education on the MIL, programmatic factors, that is, the pharmacy staff not making a deliberate effort to distribute the MIL and insufficient copies available; and beliefs, that is, patients believing they had already received enough information from pharmacy staff and doctors (Table 3). This was also seen in another study which showed that some patients believed they had received adequate information about the medicines from the HCPs and consequently did not read the MIL. 55 Mottram and Reed reported that some healthcare workers (HCWs) deemed some patients as not suitable to receive MILs, which is contrary to the right to this information. 50 Nonetheless, despite the inability to read the MIL, most patients in our study requested for universal access to MILs given that a family member or community peer would help read the MIL if needed particularly if written in common and understandable languages, that is, Afrikaans or English (Table 1).
In conclusion, health literacy, access to and utility of medicine information among hypertensive care are currently sub-optimal in Namibia. The main factors influencing access to, and utility of, patient information leaflets in hypertensive care in Namibia are first low health literacy levels, second non-availability of MIL at points of care, third lack of guidelines at points of care and finally negative beliefs among patients and HCPs. There is need for targeted interventions to integrate health literacy programmes in hypertensive care at public health facilities to enhance responsible self-care practices and outcomes among hypertensive patients in Namibia. In addition, there is need for policies to guide the effective implementation of systems to enhance access and utility of medicine information at points of care in the public health care. We will be following this up in future studies.
Limitations and strengths
The results of this study should be interpreted with limitations. First, this single-centre study adopted a cross-sectional design and the results may not be generalizable. Second, the study used a small sample size of hypertensive patients and may have under/overestimated the level of access to and utility of the MIL. Nevertheless, this is the first study in sub-Saharan Africa to assess health literacy, access to and utility of MIL among both patients and HCPs using three health literacy tools. The study also provided preliminary information on the factors influencing the utility of medicine information in hypertensive care. In addition, this is the first study to assess the role of health literacy on the utility of medicine information in a high hypertension burden country in sub-Saharan Africa. Consequently, we believe that the findings of this study provides preliminary evidence on the level of access and utility of MIL which can be used to guide future research to improve access to and utility of the MIL among hypertensive patients in public health settings in LMICs including sub-Saharan Africa as well as low-literacy settings.
Footnotes
Acknowledgements
The authors acknowledge all the patients and healthcare professionals for participating in the study; Helvi Naukosho for assisting with data collection; Liezel Bruwer for translating all patient-related information into Afrikaans; Rebecca Moltirie (Research Public Health Analyst, Centre for Communication Science); and Lauren McCormack (Vice President, Public Health Research Division) from RTI International for giving permission to use their health literacy tools (HLSI-SF) and related information used in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.