
Abstract
Introduction
Community paramedics provide care in a diverse range of settings that address the needs of the communities they serve. Recent developments have resulted in a call for guidance on the education requirements of community paramedics at a national level in Canada. To inform the development of such guidance, we sought to identify the various roles that community paramedics in Canada enact.
Methods
This was a three-phase study that combined (1) frameworks describing community paramedicine in Canada, (2) a review of community paramedicine literature focused within the Canadian setting, and (3) a review of data reported by a pan-Canadian working group. Elements identified at each phase were extracted and mapped to an existing role description for paramedics in Canada. Elements central or unique to community paramedic practice were iteratively identified and highlighted.
Results
Community paramedics perform multiple roles that span a broad continuum of the healthcare system. They deliver and support person-centred care through expanded assessment, diagnostic and therapeutic interventions (Clinician). They are situated in and engage with communities in designing programs to meet community needs (Professional). Through their trusted relationships with people receiving care and care partners, they engage in health promotion and education activities (Educator). They coordinate care and help patients navigate the care system (Health and Social Advocate). As members of interprofessional care teams (Team Member), they both accept referrals and refer within these teams, as well as support a range of disposition options. They continually assess and maintain their professional competence and personal wellbeing (Reflective Practitioner).
Discussion and conclusion
Community paramedics share common roles with other paramedics in Canada, but their enactment of these roles is contextually specific and involves elements that are unique or more prominent. The description of these roles in the community paramedic context will guide future developments in community paramedic education.
Introduction
Community paramedicine is a model of care whereby paramedics apply their knowledge and skills to provide immediate or scheduled primary, urgent and/or specialised healthcare often to medically complex and structurally vulnerable patient populations. They do so by focusing on improving equity in healthcare access across the continuum of care, providing care in place, wherever the patient happens to be. 1 Shannon et al. 2 furthered this description, offering an international consensus-derived definition that ‘a community paramedic provides person-centred care in a diverse range of settings that address the needs of the community. Their practice may include the provision of primary health care, health promotion, disease management, clinical assessment, and needs-based interventions. They should be integrated with interdisciplinary healthcare teams which aim to improve patient outcomes through education, advocacy, and health system navigation’. Integrating within interprofessional teams, providing health education, and helping with system navigation are emerging and evolving features of paramedic practice across many contexts, but are readily identifiable features of community paramedic practice in Canada.
One of the most pressing issues facing community paramedicine in Canada is the preparation of paramedics to undertake expanded and constantly evolving roles, due to a lack of appropriate education programs, shortcomings in regulatory structures, and poor integration within multidisciplinary teams. 3 Those who seek to practice as community paramedics require a combination of differing clinical experience from their traditional paramedic roles, supported by enhanced education and clinical support to successfully perform the functions of the position. This is supported by the recent release of the Paramedic Association of Canada's Career Framework for Paramedics. 4 For example, future advanced practice roles (Specialist Paramedic and Paramedic Practitioner) will have contextually specific advanced knowledge and skills in making complex clinical and treatment decisions. We argue that some community paramedics already operate in this advanced practice space despite lacking the preparation suggested by the framework. For example, it is recommended in the framework that paramedics in advanced practice roles hold a post-baccalaureate qualification in paramedic practice with expertise in a clinical speciality – in this case, in community and/or primary care. Advanced practice paramedics will possess the knowledge and skill to contribute to high-quality person-centred clinical care that goes beyond that of a traditional paramedic, which includes the ability to assess, conduct and interpret diagnostic tests, make diagnoses and provide interventions, and in the case of Paramedic Practitioners, independently prescribe medications. The use of expanded assessments, interventions, and alternative care pathways may carry greater uncertainty and therefore increased risk and responsibility. 5 Given that we know how inconsistent the current approach to community paramedic education is Chan et al., 6 we need to ensure that community paramedics are provided with additional support to prepare them to enact their roles, now and as they evolve further into advanced practice roles.
Unfortunately, unlike advanced practice roles in other health professions,7–9 community paramedic education across Canada is not delivered at an adequate level to consistently and safely produce specialist practitioners. Most community paramedic education programs, with only a handful of notable exceptions, are developed and delivered through employer-based (or in-service training) with highly variable duration, content, and award levels. 6 By virtue of such variability, an opportunity exists to develop pan-Canadian guidance on education requirements for advanced practice in community care, primary care, and public health. 6 In recent years, several documents have called for guidance related to the competencies and education of community paramedics and their evolving practice.1,10–13 To best inform the development of such guidance, an understanding of the foundational roles that community paramedics enact in this specialist context must first be identified and described.
Aim
We sought to identify both the various roles that community paramedics in Canada enact, and those that align with or support the ongoing evolution of this specialist context of paramedic practice.
Methods
Study overview
This study involved a multi-phased, multiple-methods approach to identifying the roles enacted by community paramedics in Canada. We undertook a document analysis of existing frameworks, reviewed literature on community paramedicine, and integrated the insights from a national community paramedicine working group. This approach was considered by the research team to provide appropriate depth and scope of data, allowed for the use of multiple types of data, and, importantly, allowed for authentic and credible pan-Canadian perspectives to be considered (both in the data and within the research team) without burdensome logistics. 14 The multiple methods allowed for complimentary perspectives that were not duplicative, and built on the contributions of the included data. 15
To start, we define a ‘role’ using the definition from Tavares et al. 16 – it is more than simply what people do, or a list of competencies; it is their embodiment of their professional capabilities through their competencies. You may wish to think of roles as a conceptual framework by which you can group competencies towards the performance of specific professional activities. For example, providing care for a person experiencing homelessness requires enacting multiple competencies in clinical practice, communication, social determinants of health, reflection, and critical thinking skills, to name just a few. It is these combinations of competencies, when enacted, that inform these roles.
First, we performed an initial analysis of frameworks that individually described community paramedicine models of care. Next, we further expanded on these frameworks through analysis of findings from published community paramedic literature. Finally, we integrated the publicly available data reported by a pan-Canadian working group on paramedicine in primary care, public health, and community care settings. Given that this role document will be used to inform the development of a specialist competency framework for community paramedicine that builds upon the National Competency Framework for Paramedics (NCFP), we elected to not include the NCFP document itself in our analysis within this study.
We adapted the Framework Method 17 for the deductive content analysis of extracted data across the three phases against an existing role description. We approached this study from a pragmatism perspective,18,19 acknowledging that the aim of our research required broad ‘real-world’ data, that no singular data set could address it, and that we wanted to produce a practical and useful answer. We were aware of several existing projects (developed via diverse and mixed approaches) that described both the activities of community paramedics in complex healthcare systems, as well as features of community paramedicine programs that could help to explain the underlying mechanisms of enacting the community paramedic roles. Through multiple method approaches, these could be combined in a systematic and trustworthy manner to provide new insights, while harnessing the expertise of the group to provide additional insight with the final intent of producing useful (in the context of community paramedicine) knowledge. 20
Context
Within this study, context refers to the ‘context of practice’ of community paramedicine in Canada. We acknowledge that community paramedicine is delivered via numerous models across Canada and internationally. However, we suggest there are common traits and program features that support the enactment of various roles of the community paramedic. We aim to explore this using an existing national role description, Canadian frameworks that describe community paramedicine, and pan-Canadian data on community paramedicine practice.
Positionality and reflexivity
Our research team was composed of individuals with expertise in community paramedicine, public health, and primary care, which we defined as ‘practice, research, education, policy, and/or lived or living experience with the context’. Team members represented jurisdictions across Canada and were joined by colleagues with research expertise in community paramedicine from Australia. CL and AB led the data collection, analysis, and drafting of the initial roles framework. We did not have public or patient engagement within the team.
We acknowledge that having a research team of individuals who are invested in community paramedicine clinical practice, education, research, leadership and policy means that the team is somewhat introspective when it comes to the outcome of this work. Individually and as a group, we are all inherently shaped by such insider perspectives on the research topic. To provide balance to this insider perspective, we used multiple external data sources produced by others and a deductive analytical framework. We maintained open dialogue as a research team and engaged in several rounds of clarifying questions and revision of statements in the article.
Analytical framework
We used the ‘Canadian Paramedic Profile and Roles’ 21 as a working analytical framework to develop our community paramedic roles model by extracting roles, framing concepts, and cross-cutting themes (see Table 1). This model describes the roles that all paramedics enact in practice regardless of context, including clinician, team-member, health and social advocate, professional, reflective practitioner, and educator. 16 Three framing concepts emerged in this research: variable context of practice, embedded relationships, and a health and social continuum. In addition, four cross-cutting themes were developed: patient safety, compassion, adaptability, and communication. The cross-cutting themes were almost always present in what roles did emerge and thus were not considered unique roles in themselves. We applied the analytical framework to each of the frameworks identified in Phase 1. We were guided by the description of each of the roles to determine where to map elements from other frameworks, as outlined in Table 2. We use the term elements in this manuscript as a ‘catch-all’ phrase for the various individual items that may have been mapped from other frameworks. Given these documents were produced for different purposes, by different means, they contain a mixture of roles, dimensions, competencies, models, activities, units of work, descriptions and other terms. An element is thus an overarching concept of something that was extracted from a data source within the study that contributed a data point for analysis.
Summary of the elements extracted from the PAC Paramedic Profile to inform the analytical framework.

Role descriptor summaries to guide the mapping process.
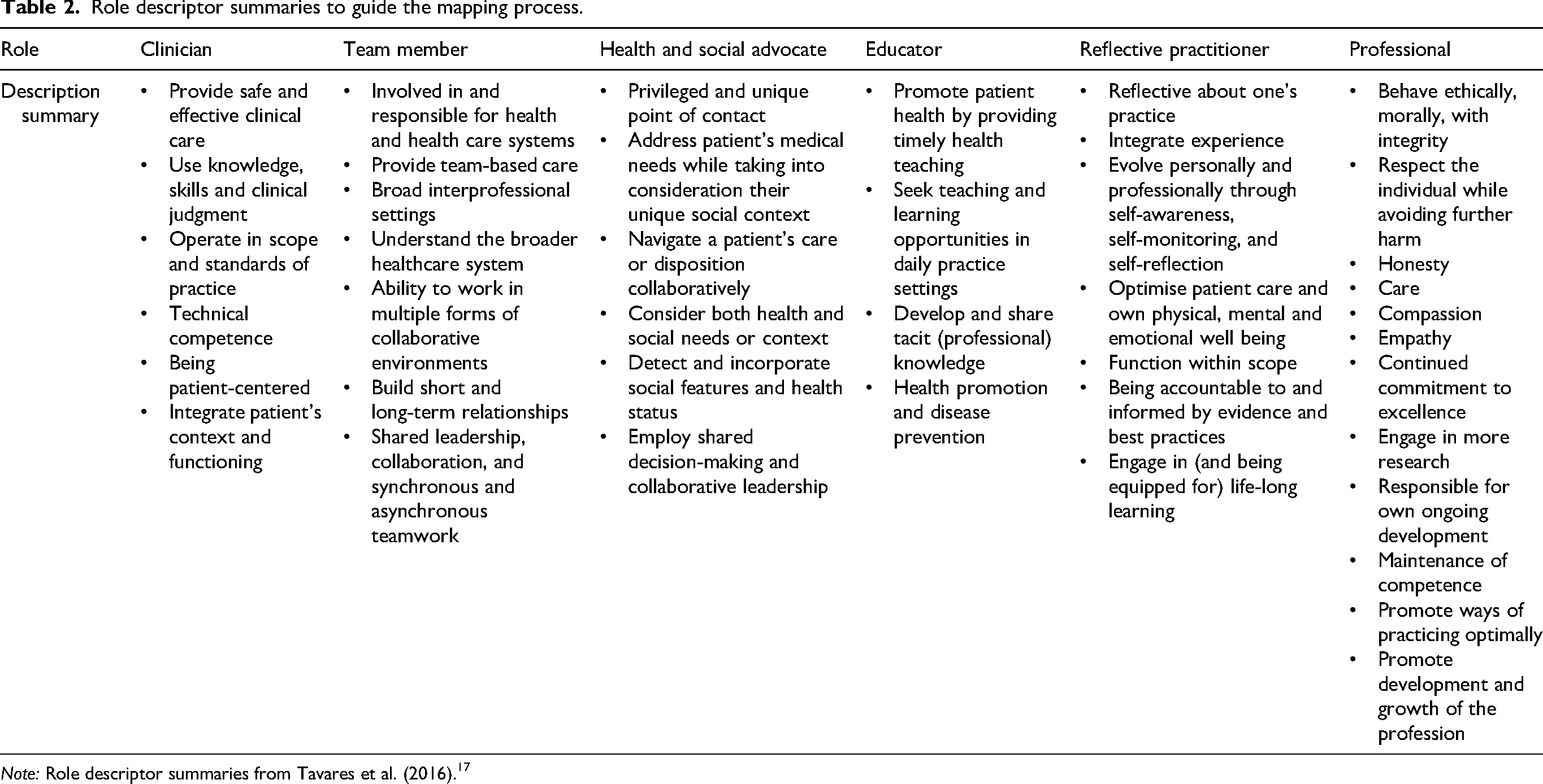
Note: Role descriptor summaries from Tavares et al. (2016). 17
Phase 1 data source – Existing frameworks
Our intent in Phase 1 was to explore existing frameworks that described community paramedicine in Canada. We searched for all existing community paramedicine frameworks in use in Canada by using existing literature review findings, frameworks identified by a national working group (details of this group's work are provided in phase 3), and combined these with the expertise of the research team. Additionally, several members of this research team sit on the national Community Paramedicine Technical Committee and are aware of context-specific developments of this nature. See Table 3 for details on each of these frameworks.
Phase 1 data results.
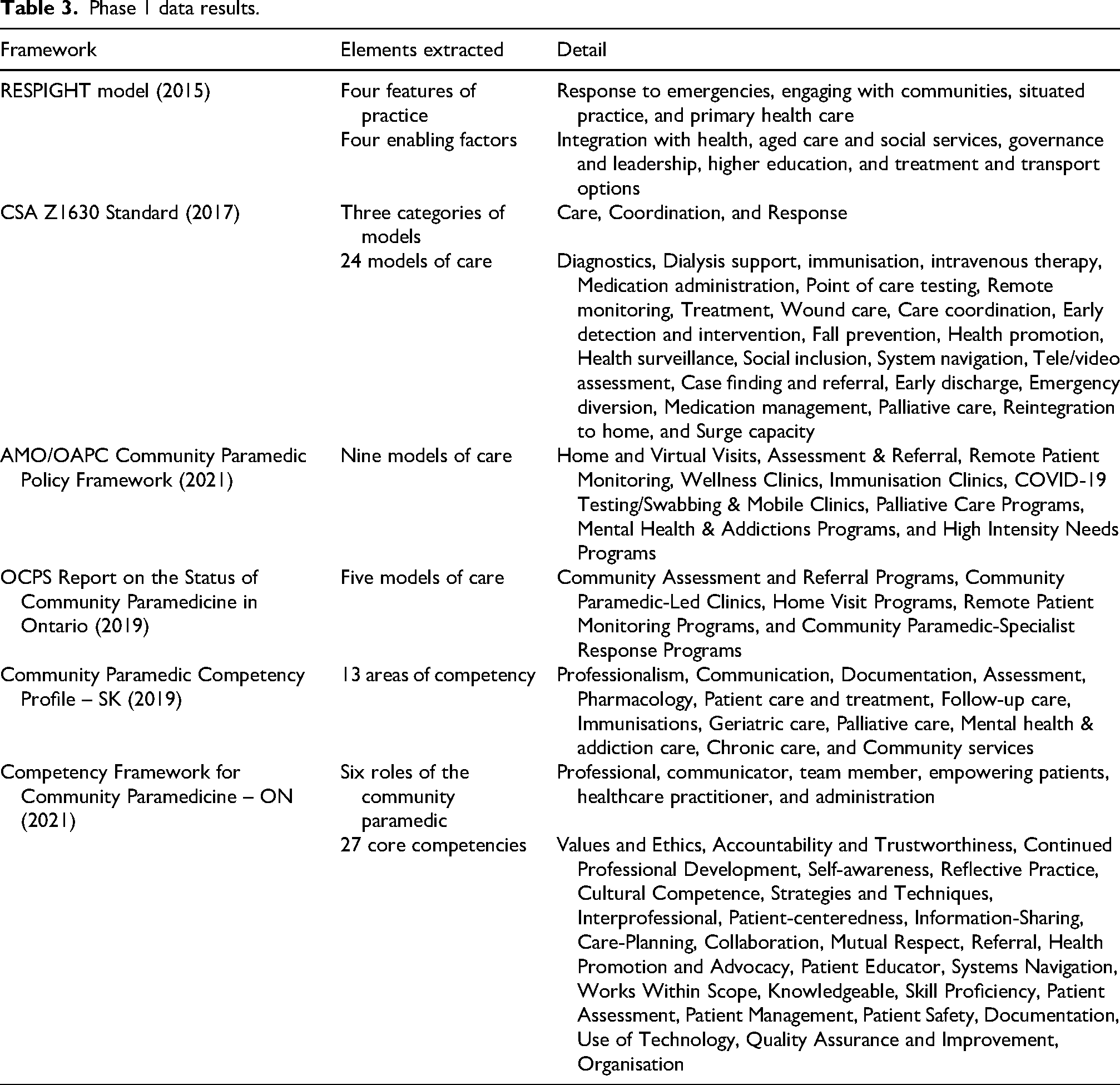
The RESPIGHT community paramedicine model of care 22 was developed in Ontario, Canada and provides a contextually specific description of community paramedicine as a model of care. It highlights the unique characteristics of community paramedicine that distinguish it from other related models of care, and includes response to emergencies, engaging with communities, situated practice, and primary health care. This model of care is facilitated by four enabling factors, which comprise integration with health, aged care and social services, 23 governance and leadership, higher education, and treatment and transport options. While the findings are not representative of all community paramedic programs, given the methods used, they are generalisable based on theory.
A pan-Canadian committee developed the Community Paramedicine Program Development standard in 2017. 1 Membership of this committee represented various sectors within community paramedicine, including service operators, community paramedics, educators, regulators, researchers, and others. The standard was developed using the CSA Group eight-stage development process, 24 which offered a defensible and rigorous project management solution. The standard describes 24 community paramedicine models of care under three organising categories – care, coordination, and response.
Two reports on community paramedicine, one from the Association of Municipalities of Ontario (AMO) and Ontario Association of Paramedic Chiefs (OAPC), 25 and one from the Ontario Community Paramedicine Secretariat (OCPS), 26 were also included. These outlined nine and five models of community paramedicine program delivery, respectively.
In addition, the ‘Community Paramedic Competency Profile’ from the Saskatchewan College of Paramedics was identified and included. 27 This profile outlines competencies of community paramedics across 13 areas.
Finally, we included the Competency Framework for Community Paramedicine in Ontario, based on an original framework developed by Middlesex-London Paramedic Service. 28 This document outlined six roles of a community paramedic, along with 27 core competencies.
Data extraction
We extracted each of the elements from these foundational frameworks into a spreadsheet. Two researchers (CL and AB) extracted elements individually and then compared findings. Any disagreement was resolved via discussion.
Phase 2 data source – Community paramedicine literature
Two researchers (CL and AB) began by intentionally focusing on literature related to community paramedicine in Canada. Our team had recently completed two reviews that identified community paramedicine literature, and we elected to use those reviews rather than complete a duplicative review. Both peer-reviewed and grey literature were included across the two reviews.
First, we used the findings of a recent Canadian paramedicine literature review to identify community paramedicine, public health, and primary care literature. 29 This was a restricted review focused on Canadian paramedicine literature published from 2011 to 2023 that used multiple databases and grey literature searches. In addition, Bolster et al. performed a manual review of Canadian Paramedicine magazine issues from 2014 to 2022.10,29
Second, while we initially focused on Canadian literature, we recognised that international works may have had an influence on or application to Canadian contexts. Consequently, we also opted to use a recently published restricted review of community paramedicine to provide additional insights from the international literature. 13
The full details of the included reviews, search strategies, and results are reported in their respective manuscripts, referenced above.
Data extraction
The extraction process for Phase 2 was informed by a series of elements. These included descriptions, models, expectations, roles, and attributes. In addition, we extracted data from included literature that described public health, palliative care, and other related community paramedic program models as suggested by the phase 1 results. We extracted each of the elements from these publications into the same spreadsheet. Two researchers (CL and AB) extracted elements individually and then compared findings. Any disagreement was resolved via discussion.
Phase 3 data source – Working group data
A working group dedicated to providing expertise on community care, primary care, and public health paramedicine submitted a report to the NCFP development group lead (AB) in October 2022 as part of the data collection process for developing the NCFP. This working group comprised 15 experts in community paramedicine, primary care, and public health with representation from Ontario, Saskatchewan, Manitoba, Alberta, Nova Scotia, Prince-Edward Island, and British Columbia. The group sought to describe and support with evidence what community paramedic units of work comprised nationally. They suggested competencies for community paramedics across eight categories. Several members of this working group are also members of the research team for this study (AH, RPS, BML, DK, BDA, LH, MSL, and SL). The report data is available on reasonable request.
Data extraction and analysis
The extraction process for Phase 3 was also informed by similar elements. These included descriptions, activities, and competencies. We extracted each of the elements from this data into a spreadsheet. Two researchers (CL and AB) extracted elements individually and then compared findings. Any disagreement was resolved via discussion.
Merging of findings
Two researchers (CL and AB) created an initial set of merged findings by cross-referencing and collapsing the mapped elements. This was achieved by seeking at least one occurrence of a mapped element to a role, cross-cutting theme, framing concept or enabling factor. Where we identified multiple mapped elements, we combined like terms and collapsed to higher-order terms (e.g., ‘referrals to community services’ was simplified to ‘referral’). This initial table of mapped and merged findings was brought to the research team.
The team agreed on unique or central elements to community paramedic practice through an iterative process of comparing the mapped results to the existing description of each role in the profile and highlighted elements that were more commonly described throughout the findings of this study (e.g., community based care, equity of access) or were unique to the mapped findings (e.g., social prescribing), to inform the final version of the merged findings. The team then reviewed the final version of the edited table and provided minor feedback on wording and placement of elements.
Trustworthiness and rigor
We enacted measures to improve the trustworthiness and rigour of our processes and outputs. 30 For example, we ensured a clear audit trail, capturing all documents, mapping exercises, and edits throughout multiple drafts. We ensured our team was composed of members of the profession with expertise in community paramedicine clinical practice, education, research, policy, and program development, with representation from across Canada. We used an analytical framework that describes the roles of all paramedics in Canada and used it to explore a context-specific implementation of the roles.
Ethical considerations
This study did not involve human research participants, and therefore, no ethics approval was required.
Results
Phase 1 findings
Table 3 outlines the elements extracted from the six frameworks included as Phase 1 data sources. These findings include various descriptions of community paramedicine models of care, areas of competency and core competencies, and proposed roles of community paramedics (that differ from the core roles profile).
Phase 2 findings
We identified 110 articles that were related to community paramedicine, harm reduction, Indigenous community care, mental health, rural practice, substance use, palliative care, public health, remote and isolated communities, and virtual care in the existing Canadian reviews. Proactive (i.e., scheduled care) and reactive (i.e., unscheduled care) models of community paramedicine were described, and described targeted approaches to reduce 911-initiated emergency calls, emergency department visits and hospital admissions.13,31,32 In addition, the creation of low-acuity pathways, outreach services, and social prescribing for community care of structurally marginalised populations were described in the literature.11,13,33,34 The captured studies reported the importance of the paramedic role in caring for people receiving palliative care,35–37 long-term care at home, 38 and primary care in the absence of appropriate access within the community.13,39,40 In addition, literature highlighted the ability of paramedic services to collaborate in the delivery of public health, including conducting mass testing, home visits, and immunisation clinics.41,42 Community paramedics also play a central role in the delivery of equitable health care access to incarcerated persons, people who use drugs, underserved minority populations, and remote and isolated communities – in particular, to remote Indigenous communities.11,43–47
Bowles et al. highlighted an additional four dimensions of paramedic practice that were mapped to the existing roles framework. 48 These were (1) Practitioner (who the practitioners are); (2) Practice settings (where they practice); (3) Care (what type of care they provide); and (4) Patient disposition (who/where they transition care of the patient to). Shannon et al. demonstrated a need to develop common approaches to education and the scope of role while maintaining flexibility in addressing community needs. They also observed a lack of standardisation in the implementation of governance and supervision models. 13
Phase 3 findings
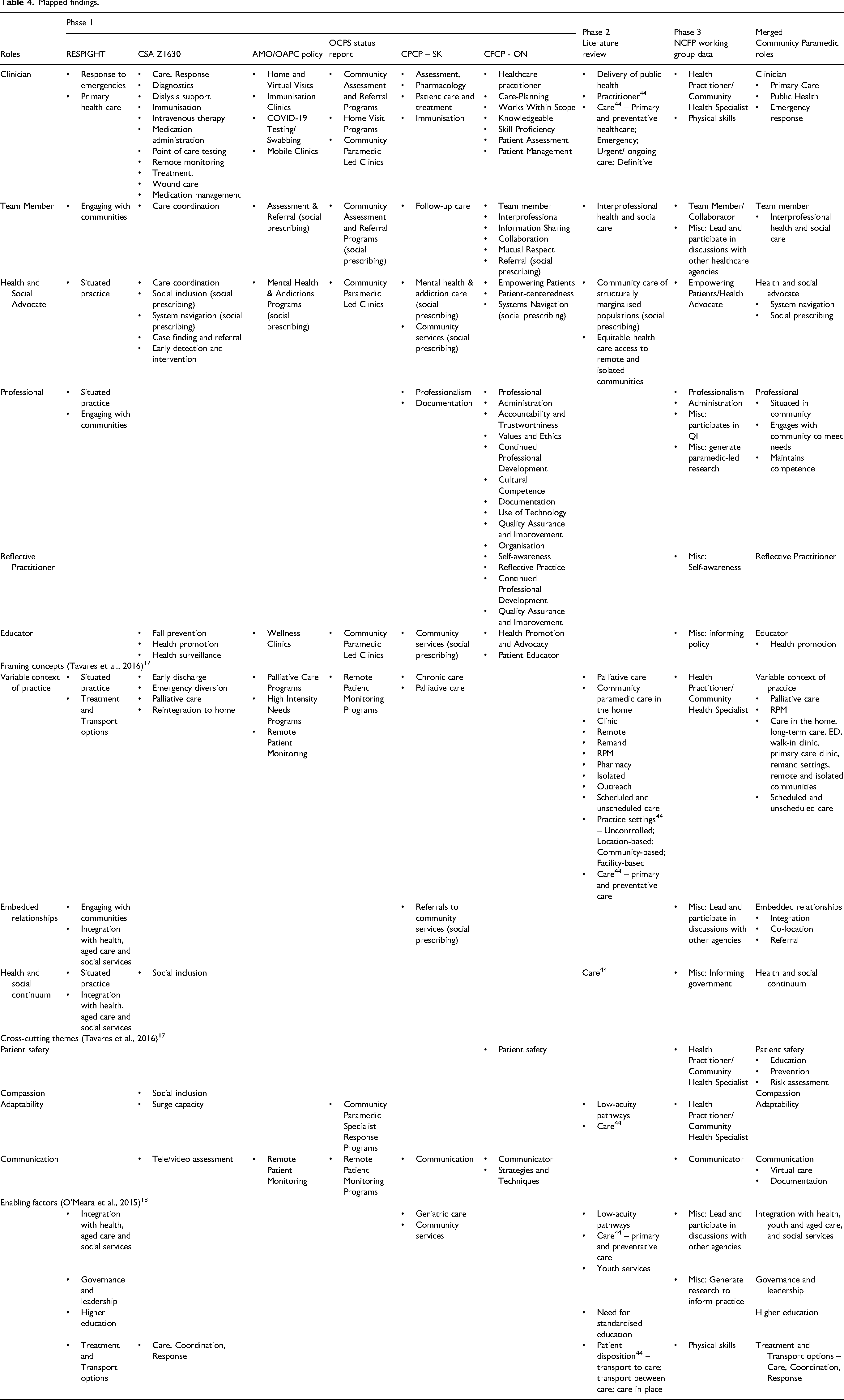
The NCFP working group reported a list of 128 competencies organised into eight categories: Professionalism, Communicator, Team Member/Collaborator, Empowering Patients/Health Advocate, Health Practitioner/Community Health Specialist, Physical skills, Administration, and Miscellaneous. The individual competency items from each category were mapped against the analytical framework. For simplicity, the mapped and merged findings (next section) only included the parent categories outlined in this paragraph, as outlined in Table 4.
Mapped findings.
Merged findings
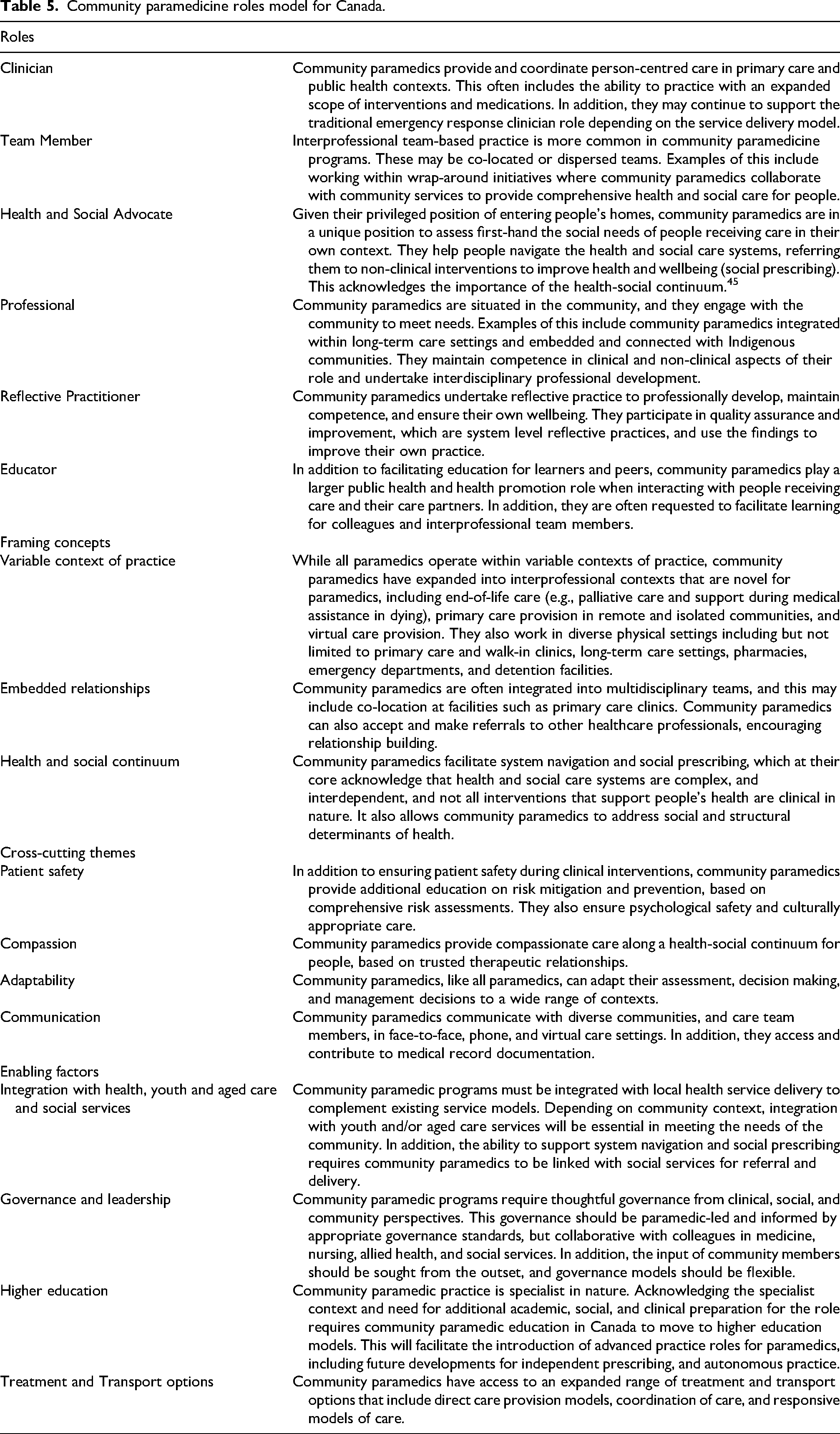
The merged findings offer an insight into a model of community paramedic practice, which is enacted through the previously described six roles of the paramedic (with unique or central elements to community paramedic practice highlighted in the merged results), three framing concepts, four cross-cutting themes, and four enabling factors. The mapping and merging exercise confirms the ability of the existing six roles to structure the context-specific roles that community paramedics enact. Further details on the community paramedicine roles model that resulted from the mapping exercise are provided in Table 5.
Community paramedicine roles model for Canada.
We offer a visual representation of this roles model in Figure 1. This model highlights the roles that community paramedics enact when practicing within their specialist context. Starting in the centre of the image, each role is present, and the italicised writing under each role highlights the central or unique elements that distinguish community paramedicine from traditional practice. Moving outwards, these roles are supported by cross-cutting themes and framing concepts identical to those described by Tavares et al. Importantly, moving to the outside of the image, community paramedicine is enabled by several factors highlighted by O’Meara et al., including clear governance and leadership, a need for higher education, integration within the broader system, and diverse treatment and transport options.

The roles of community paramedics in Canada. We combined an existing description of paramedic roles with multiple community paramedicine frameworks, literature findings, and working group data in Canada to structure our understanding of the roles of the community paramedic. Image used under a CC-BY 4.0 License.
Discussion
This study aimed to identify the context-specific enactment of the roles of community paramedics in Canada. Following a three-phase process that mapped existing frameworks, a comprehensive review of the literature, and an expert working group report, we identified the context-specific enactment of six roles. Our findings demonstrate that community paramedics provide emergency care, primary care, and public health (Clinician). They are situated in and engaged with communities in designing programs to meet community needs (Professional). They deliver and support direct patient care, often with an expanded clinical scope (Clinician). Using their trusted relationships with people receiving care and care partners, they engage in health promotion and education activities (Educator). Community Paramedics coordinate person-centred care, help people to navigate the health and social care system, and enact social prescribing solutions (Health and Social Advocate). As members of interprofessional care teams (Team Member), they both accept referrals from and refer within these teams, as well as support a range of disposition options for people receiving care. They also continually assess and maintain their professional competence and personal wellbeing (Reflective Practitioner).
Our findings support the utility of the existing roles description for paramedics 16 in describing and understanding the specific roles enacted by community paramedics, or more broadly, paramedics who practice within community and primary care settings. Enacting these roles is contextually specific and involves elements that are either unique or more prominent when compared to traditional paramedic practice. Two examples include practicing within interprofessional care teams, and social prescribing. Paramedics working within interprofessional care teams is a distinct difference from the emergency response context, where paramedics traditionally transfer care of patients directly to other care team members within hospitals or health centres.49–51 Evidence from the UK and Ireland demonstrates that assimilation of paramedics into primary care teams is complex and may present several challenges.52–54 As such, issues related to role conflict, communication ability, shared decision making, clinical governance and integration must be considered when embedding paramedics in care teams.53,55 Being embedded within a broader team context also requires paramedics to improve their understanding of collaborative practice and relationships with social and community service providers to help people receiving care to navigate the healthcare and social system.
Navigating health and social care systems is one example of the social prescribing interventions that community paramedics facilitate. 56 Although the nomenclature of social prescribing is not commonly used within the Canadian context, it provides a useful perspective that acknowledges the interdependency of the health-social continuum. By contrast to the United Kingdom, where social prescribing is performed by non-clinical staff based in primary care centres (and not commonly in the patient's own context),56,57 community paramedics can support a range of clinical and non-clinical interventions and referrals to holistically support the needs of people receiving care. Research into the role of community paramedicine programs in supporting health and social needs through social prescribing is underway, 3 and innovative care models are being developed and evaluated. 58
A significant barrier to the further development of community paramedicine in Canada at present is the absence of competency and education requirements to prepare professionals for this specialist contact of practice. While community paramedic programs should differ in their design based on community needs, the preparation of community paramedics must be based on an agreed-upon standard at provincial and/or federal levels. Chan et al. supported this need for formalised training and program frameworks in 2019, 6 yet to date there has been little development in this area in Canada compared to developments in other jurisdictions such as the Republic of Ireland and Australia, for example. While our study illustrates the new and diverse paradigms that community paramedics work within, the findings beg the question – are they adequately prepared for these roles?
An additional concern that our study highlights as an enabling factor, 22 but which requires further research and nuanced discussion, is the governance, leadership and infrastructure required to enable advanced practice in the specialist context of community paramedicine. In the absence of clear, coherent, profession-led governance of paramedicine across all jurisdictions, there is a risk that advanced practice positions are created without the critical infrastructure required to make them effective, safe, and accountable. 55 While our findings only begin to offer a structure by which to understand and explore advanced practice by paramedics, these essential governance issues must be addressed as equally necessary. As expectations related to governance and accountability of advanced practice are established, they may suggest changes to our understanding of the roles enacted by community paramedics.
Future directions for research to build on this work include identifying and exploring the competencies required to enact community paramedic practice and the required levels of advanced practice on a provincial and/or federal level in Canada. In addition, research to inform the education requirements to prepare community paramedics for their roles, and indeed the contextual enactment of those roles in diverse contexts across Canada, is also required. As we alluded to, the infrastructure, governance, and accountability of any such positions require careful consideration and exploration to ensure patient safety and service efficiency. Finally, we suggest that exploring the contexts that community paramedicine may expand into next in Canada would be a worthwhile endeavour to begin to prepare the system for future change and development.
Limitations
The very nature of community paramedicine programs means that how practice is enacted varies considerably across Canada, depending on context. However, we offer that the use of a pan-Canadian role description as the foundational analytical framework facilitates translation across such contexts. We did not perform any primary research in this study with community paramedics to understand these roles. Their perspectives, however, were captured within multiple documents that were included in and formed the data for this study (e.g., working group data, including literature that used interviews and focus groups with community paramedics). In addition, all members of the author team have expertise within community paramedicine, including clinical practice, research, education, policy, and leadership. What we offer here is a conceptual framework for understanding community paramedicine practice, that is, subject to change and influence as the meaning and foundation of community paramedicine itself evolves.
Conclusion
Community paramedics enact the same roles that are common for all paramedics in Canada. However, our study demonstrates that enacting these roles is contextually specific and involves elements that are either unique or more prominent when compared to traditional paramedic practice. Describing and understanding these roles in the community paramedicine context provides a foundation for future work to identify program delivery models, professional competencies, and guide education requirements.
Supplemental Material
sj-pdf-1-pam-10.1177_27536386261430036 - Supplemental material for Identifying the context-specific roles enacted by community paramedics in Canada
Supplemental material, sj-pdf-1-pam-10.1177_27536386261430036 for Identifying the context-specific roles enacted by community paramedics in Canada by Chelsea J. Lanos, Matthew S. Leyenaar, Liz Caperon, Brittany D’Angelo, Mathieu Grenier, Jessica Harrisson, JD Heffern, Laura Hirello, Amber Hultink, Danny Kustra, Bryan Laviolette, Shannon Leduc, Brent McLeod, Joanne Moss, Michael Nolan, Peter O’Meara, Brendan Shannon, Meagan Slack, Ryan P. Strum and Alan M. Batt in Paramedicine
Footnotes
Acknowledgements
We wish to acknowledge the input of all members of the NCFP working group on community care, primary care, and public health.
ORCID iDs
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by Ontario Health as part of the development of the Ontario Community Paramedicine Competency Framework (2024).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CL and AB were remunerated for their time on this project via contract. Alan Batt is a Deputy Editor of Paramedicine. He played no role in the editorial decision making process, which was conducted in adherence to the journal's peer review policy.
Data availability statement
Data for this study includes existing literature available in the public domain and data submitted by the NCFP working group. The literature sources used to contribute to our conclusions are outlined within the manuscript. The working group data can be provided on a reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.