
Abstract
Introduction
Background
Pain is a multidimensional experience that encapsulates a physiological, emotional and cognitive reaction in response to actual or potential tissue damage.1–4 The experience of pain is highly subjective, and is dependent on the individual's lived experience and tolerance of pain.3–5 The biopsychosocial model of health describes the understanding that in order to fully comprehend an individual's suffering, one must take into consideration the interactions between biological, psychological and sociocultural factors. 6 Due to sex potentially influencing each aspect of the biopsychosocial model, it is reasonable to assume that males and females may experience and express pain differently. Current literature indicates that females tend to disproportionally experience more severe, longer-lasting, recurrent and chronic pain, than their males counterparts.6–9 There is evidence that males tend to cope with their pain in a practical way through distraction and finding solutions to reduce pain, whereas females appear more likely to view pain as normal and surround themselves with support networks to help manage their pain.6,8,10–12 These differences may be the result of historical expectations of different genders roles, gender socialisation and dismissiveness or misunderstanding of gendered pain presentations.13,14 In specific relation to abdominal pain, compared to males of all ages, females younger than 17, experience more abdominal pain, and report poorer health outcomes overall. 15 While females present more frequently with gastrointestinal pain, males present more commonly with serious gastrointestinal complications.16–21 These research findings indicate sex has a significant impact on the perception and experience of abdominal pain, and therefore, support the hypothesis that pain has a gendered dimension.
In Australia, paramedicine refers to the provision of both emergency and non-emergency healthcare to the community in the out-of-hospital setting. 22 Paramedics are frequently contacted to alleviate pain in the community and as part of their patient assessment use a range of seemingly sex-neutral pain assessment and measurement techniques.23–25 These often do not consider the subjective nature of the pain experience, nor the biological, psychological or sociocultural influence that sex has on pain expression. 26 Whilst male and female paramedics rely on a patients symptoms and reporting of pain to inform analgesic decisions, ultimately, paramedics use their own subjective clinical judgement that is influenced by their experiences and scope of practice, to decide analgesic management. 27 This is done without consultation with medical personnel. Therefore, although it is expected that there is gender neutrality in relation to pain management, paramedics inform analgesic decisions based off patients’ response to objective clinical assessments, and the paramedic's subjective clinical judgement. Notwithstanding the engendered identity of patients and practitioners, unmet analgesic needs may undermine patient autonomy and the right to be pain free.
The aim of this study therefore was to determine the influence of patients’ sex on paramedic administration of analgesia, and specifically opioids, in cases of acute abdominal pain.
Methods
Study design
This study utilised a retrospective analytical cohort design using data from archived electronic medical records (MR) from one Australian jurisdictional ambulance service (JAS). This study is reported in adherence to the STROBE reporting guidelines for increasing transparency and quality in observational studies. 28
Setting
The setting was a large Australian ambulance service providing more than 1 million responses per year via the ‘000’ emergency system. 29 This service is the sole provider of emergency ambulance responses, servicing a population of 8.1 million people across metropolitan, regional, and remote areas. 30 The service provides a two-tiered road response, consisting of advanced life support paramedics, and specialist intensive/extended care paramedics. Paramedics in this JAS are predominantly degree-qualified, having completed 2-to-3-year Bachelor-level studies from universities approved by the Paramedicine Board of Australia. 31 Paramedics are permitted to engage in independent decision making without contemporaneous medical oversight whilst using clinical protocols to guide decisions and practice. All paramedics can administer oral, inhaled and parenteral analgesia including ibuprofen, methoxyflurane, morphine and fentanyl, whilst specialist paramedics additionally have a variety of options including local anaesthesia, regional anaesthesia and morphine/midazolam sedation. Whilst morphine could be administered via multiple parenteral routes, fentanyl could only be administered intranasally in this JAS during the period from which the data originated. Anti-spasmodic medication for abdominal complaints was not available in this system.
Population
The population comprised any individual between the ages of 16 and 65 with a complaint of abdominal pain who engaged with JAS paramedics anywhere in the state between July 2019 and June 2020. The ages of 16 to 65 were chosen as the analgesia protocols used by the JAS indicate the same dosage recommendations for these ages. Outside of this age range, the recommended dosage changes and in most cases decreases. Abdominal pain was chosen as the condition of interest as females more commonly present with it compared to males, and therefore understanding if disparities exist in a predominantly female condition is warranted.12,15,16,18 On the MR, it is mandatory for a paramedic to select one ‘chief protocol’ as the main treatment pathway for the patient, based on the patient's chief complaint. Paramedics may list subsequent protocols that were also adhered to. To increase sensitivity, cases were deemed to involve abdominal complaints if the paramedic-reported ‘chief protocol’ was ‘Abdominal Pain’ or ‘Gastroenteritis’. No steps were taken to limit the aetiology of the abdominal pain.
Bias
An annual block of dates was chosen to mitigate selection bias and enhance fair representation of the wider population, and subsequent generalisability. 32 More specifically, the dates covered the period before and during the coronavirus pandemic, as individual help-seeking behaviours and health service provider behaviours may have varied due to the pandemic and safety concerns. Moreover, by using a continuous year of data, one can be confident that the results are not due to seasonality, specific paramedics, or ambulance station culture, nor specific population characteristics.
Data source
Data were sourced from the routinely collected ambulance service dispatch and clinical record dataset, that are completed contemporaneously by paramedics for all patients. The MR comprises information including case details, dispatch and response times, patient details, presentation, paramedic-reported provisional diagnosis, clinical management and paramedic-reported outcomes. Whilst some of these dispatch-specific details are automatically generated, the majority, and specifically the clinical details, are completed manually by a paramedic immediately following completion of the case. Not all fields are mandatory on an MR, and therefore some data may be missing from record to record. All data provided were de-identified by the JAS prior to being shared with the research team.
Whilst it is understood that the mechanism of action of ketamine is that of a N-methyl-D-aspartate receptor antagonist, for the purpose of this research, ketamine was analysed in the same analytical category as an opioid due to its interaction on opioid receptors, and its use in conjunction with other opioids to provide pre-hospital analgesia.33–37
Regarding nomenclature for sex, the MR provides the following options for paramedics to choose from: male, female and indeterminate. For the purposes of this analysis and the study more broadly, it was deemed most appropriate to analyse males and females in terms of their biological sex. This is because the description of sex is based on the paramedic's binary assumption of male or female when completing medical records, not necessarily the patients’ self-identification. In the interest of criticality, this study did not intend to reify binary sex stereotyping. The terms of sex and gender were used interchangeably throughout, however for the sake of this research, will hold the same meaning of binary biological sex. Individuals that were classified as indeterminate were excluded from this analysis as outlined in the limitations.
Outcomes
The objective of this study was to determine if a patient's sex had any influence on patients receiving any type of pharmacological analgesia, or an opioid for management of abdominal pain. The primary outcomes of this study were two-fold: pharmacological analgesia provision (yes or no), as either a single agent or several combined, and opioid provision (yes or no). These outcomes were measured by analysing sex (male/female) as the defining variable, and by controlling for the possible confounders of patient sex, patient age and initial pain score. Other confounders identified in the literature, such as paramedic sex, paramedic clinical level, paramedic years of experience, patient race and socioeconomic status, were unable to be controlled for as they were not available in the provided dataset. The secondary outcomes were both descriptive investigations and association analyses of age, pain severity, and opioid dosage in the context of patient sex and analgesic and opioid administration decisions. It is of note that sex and age are both mandatory to complete on an MR, whereas pain score is not.
Statistical analysis
IBM SPSS Statistics 38 was the statistical analysis tool used for the analysis of the data. For all statistical testing, significance was determined at the p = .05 level. Descriptive statistics for all variables were calculated with significance testing conducted using independent sample t tests, Mann–Whitney U tests, and chi-square tests, dependent on the type of variable and its distribution. Data are described as mean with standard deviation (SD) or median with interquartile range (IQR), pending distribution. The chi-square (χ2) test for independence was used to assess significance of differences with the effect size statistic Phi (Φ) and Cramer's V (Φc) coefficient used to measure the strength of association. The coefficient was interpreted based on the effect sizes outlined by Pallant. 39 Univariate and multivariate logistic regression was conducted to test for relationships between the independent variables of patient sex, age and pain severity, and the outcome variables of both analgesic administration and opioid administration, and to control for potential confounding. The Hosmer-Lemeshow goodness-of-fit test was conducted to identify if the multivariate logistic model was suitable for the data. A backwards elimination model was also implemented to remove any statistically insignificant variables. Regression results are presented as unadjusted odds ratio (OR) and adjusted OR (aOR), with 95% confidence intervals (CIs).
Ethics approval
This study was approved by the Western Sydney University Human Research Ethics Committee with reference number H14835.
Results
Participants
During the study period, paramedics attended 26,417 (n) patients who met the inclusion criteria, with all descriptive statistics results listed in Table 1. Females made up 61.6% (n = 16,271) of the study population. The mean age of patients was 41 ± 14 where on average, male patients were found to be significantly older than their female counterparts (44 ± 13 vs 39 ± 14; p < .001).
Descriptive statistics of study population.
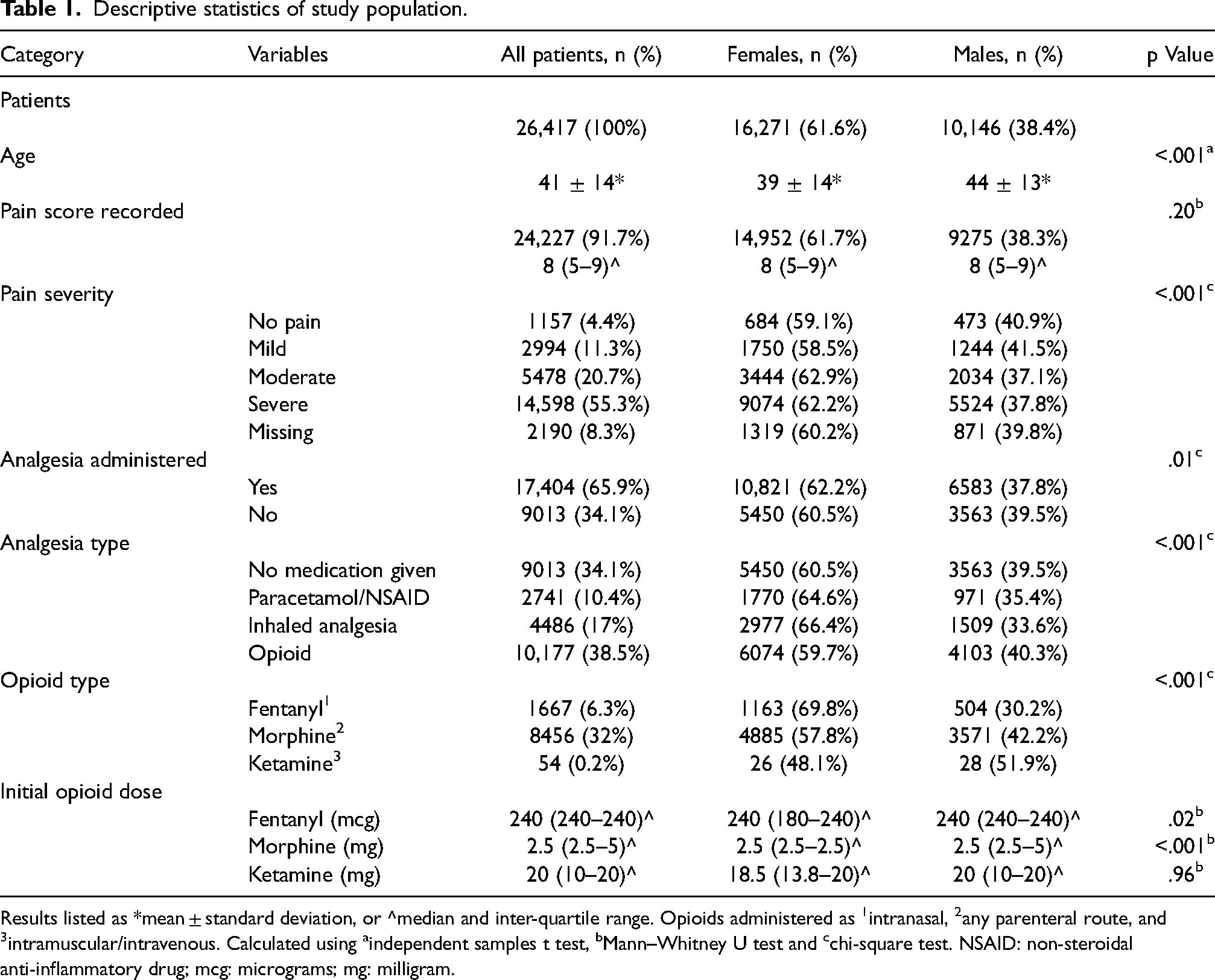
Results listed as *mean ± standard deviation, or ^median and inter-quartile range. Opioids administered as 1intranasal, 2any parenteral route, and 3intramuscular/intravenous. Calculated using aindependent samples t test, bMann–Whitney U test and cchi-square test. NSAID: non-steroidal anti-inflammatory drug; mcg: micrograms; mg: milligram.
Paramedics recorded a pain score in 91.7% (n = 24,227) of patient interactions with an initial median pain score of 8/10 (IQR: 5–9) across both sexes. Patients who received no analgesia had a lower median pain score compared to patients who received any type of analgesia (4 (IQR 2–6) vs 8 (IQR 7–10); p < .001). Patients who received an opioid or an inhaled analgesia had a higher pain score than those who received paracetamol/non-steroidal anti-inflammatory drug (8 (IQR: 8–10) vs (8 (IQR: 7–10); vs (5 (IQR: 4–7); p < .001). The distribution of pain scores and the associated analgesia given by sex is illustrated in Figure 1.
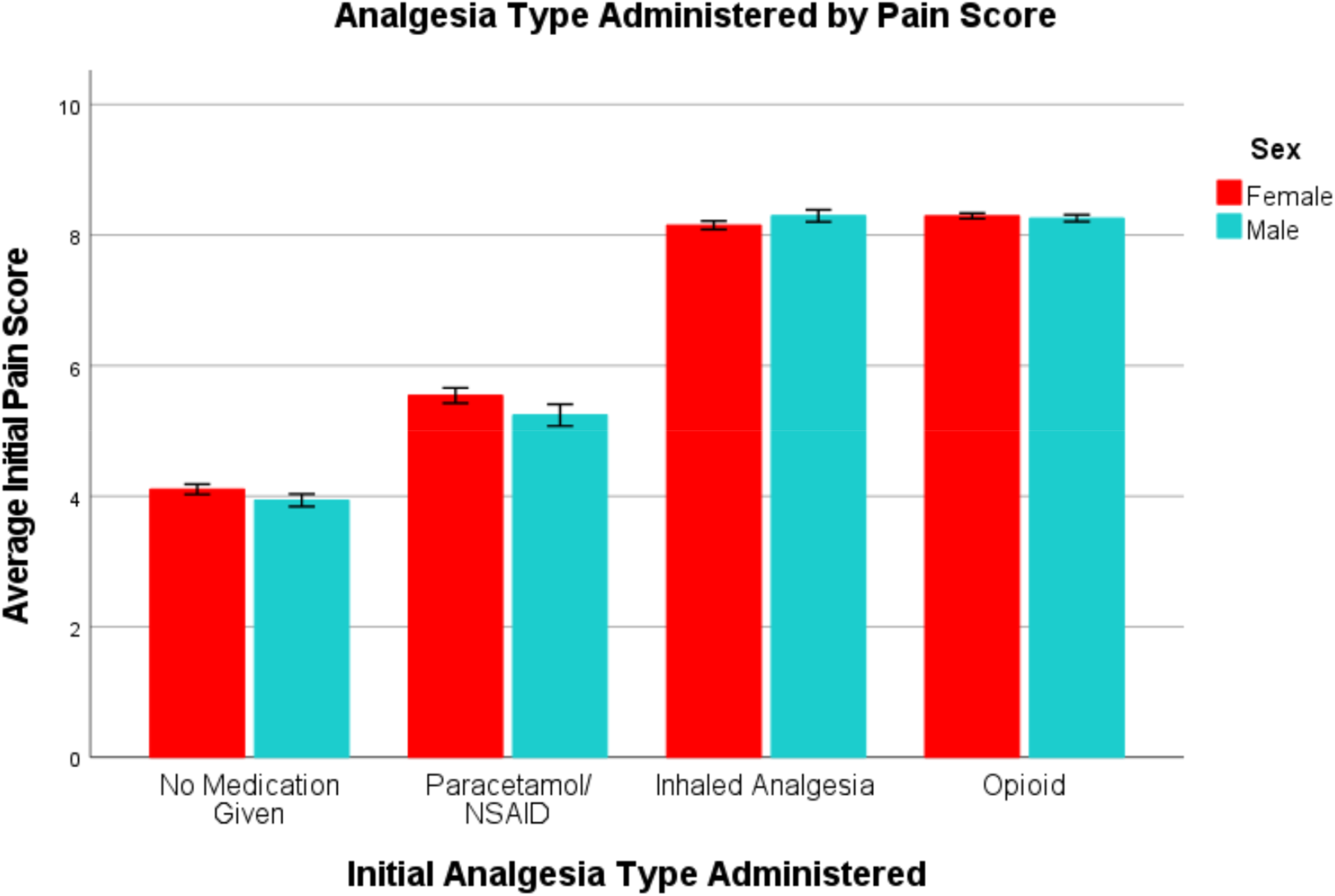
Analgesia type administered by pain score per sex with 95% confidence intervals.
Analgesia was administered to 65.9% (n = 17,404) of patients, where the most administered analgesia type was opioids at 38.5% (n = 10,177). Morphine was the most administered analgesia at 32% (n = 8456) followed by methoxyflurane at 17% (n = 4486), where 27.6% (n = 6677) of patients who reported pain received no analgesia.
More than half the study population reported their pain as severe (55.3%; n = 14,598), where 58.8% (n = 8588) of them received an opioid. On average, females had greater variation in the initial dose of fentanyl, morphine and ketamine compared to their male counterparts.
Association testing
A statistically significant association was found between a patient's sex and the administration of analgesia (χ2(1, n = 26,417) = 7.32, p = .01, Φ = −0.02) and the administration of an opioid (χ2(1, n = 26,417) = 25.51, p < .001, Φ = 0.03). The strengths of these associations, as identified by Φ were however small and unlikely to have a clinical significance. Statistically significant associations between initial pain severity and analgesic administration (χ2(3, n = 26,417) = 8705.86, p < .001, Φc = −0.60) and opioid administration (χ2(3, n = 26,417) = 5386.64, p < .001, Φc = 0.47) were also identified, with these variables found to have a large effect size as noted by Φc. Chi-square tests and correlation coefficients are listed in Table 2.
Chi-square testing of outcome variables.
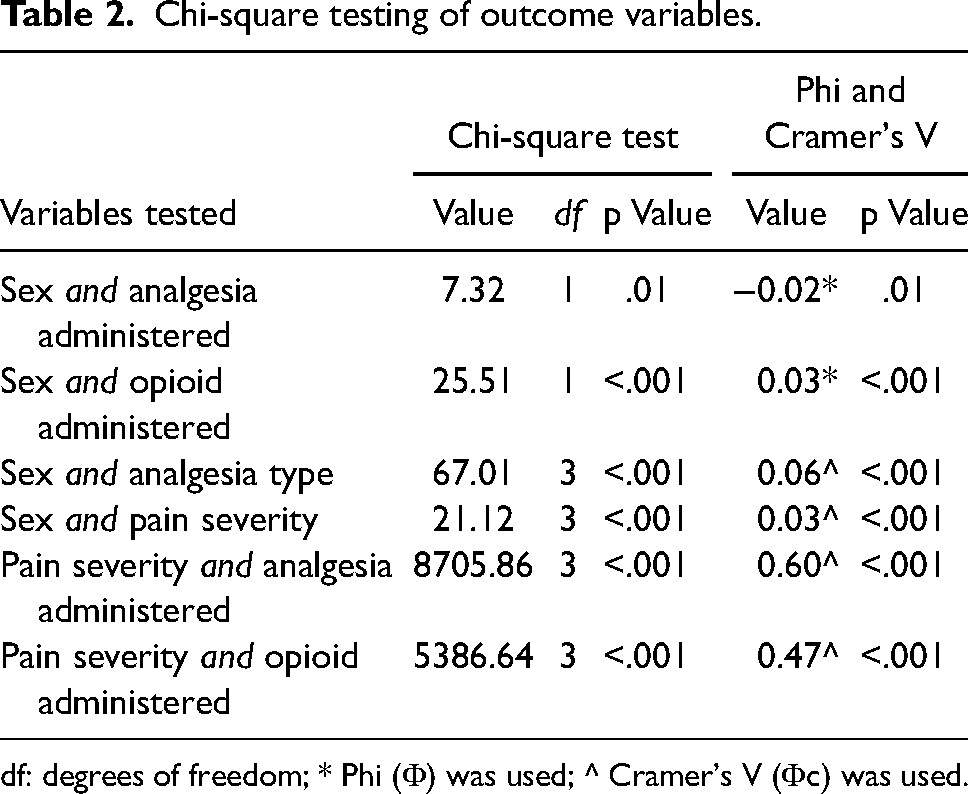
df: degrees of freedom; * Phi (Φ) was used; ^ Cramer's V (Φc) was used.
Univariate regression analysis
Analgesic administration
The unadjusted analysis found that females were more likely to be administered any type of analgesia than their male counterparts (OR 1.08; 95% CI 1.02–1.13; p = .01). Patients aged 25 to 54 had significantly greater odds of receiving analgesia than other ages. Patients who had reported severe pain were administered analgesia more often than those in any other pain group.
Opioid administration
The unadjusted analysis indicated that females were at lower odds of opioid administration compared to males (OR 0.88; 95% CI 0.83–0.92; p < .001). The analysis also indicated that the older the patient, the greater the odds of opioid administration. This trend does not continue however after the age of 59, indicating that patients between the ages of 60 and 65 are at lower odds to receive an opioid than those who are aged 55 to 59 (OR 2.08; 95% CI 1.81–2.39; p < .001 vs OR 2.16; 95% CI 1.88–2.49; p < .001). Patients reporting severe pain were at higher odds of being administered an opioid than those in any other pain group. Univariate regression results are outlined in Table 3.
Univariate regression of confounders influencing analgesic and opioid administration.
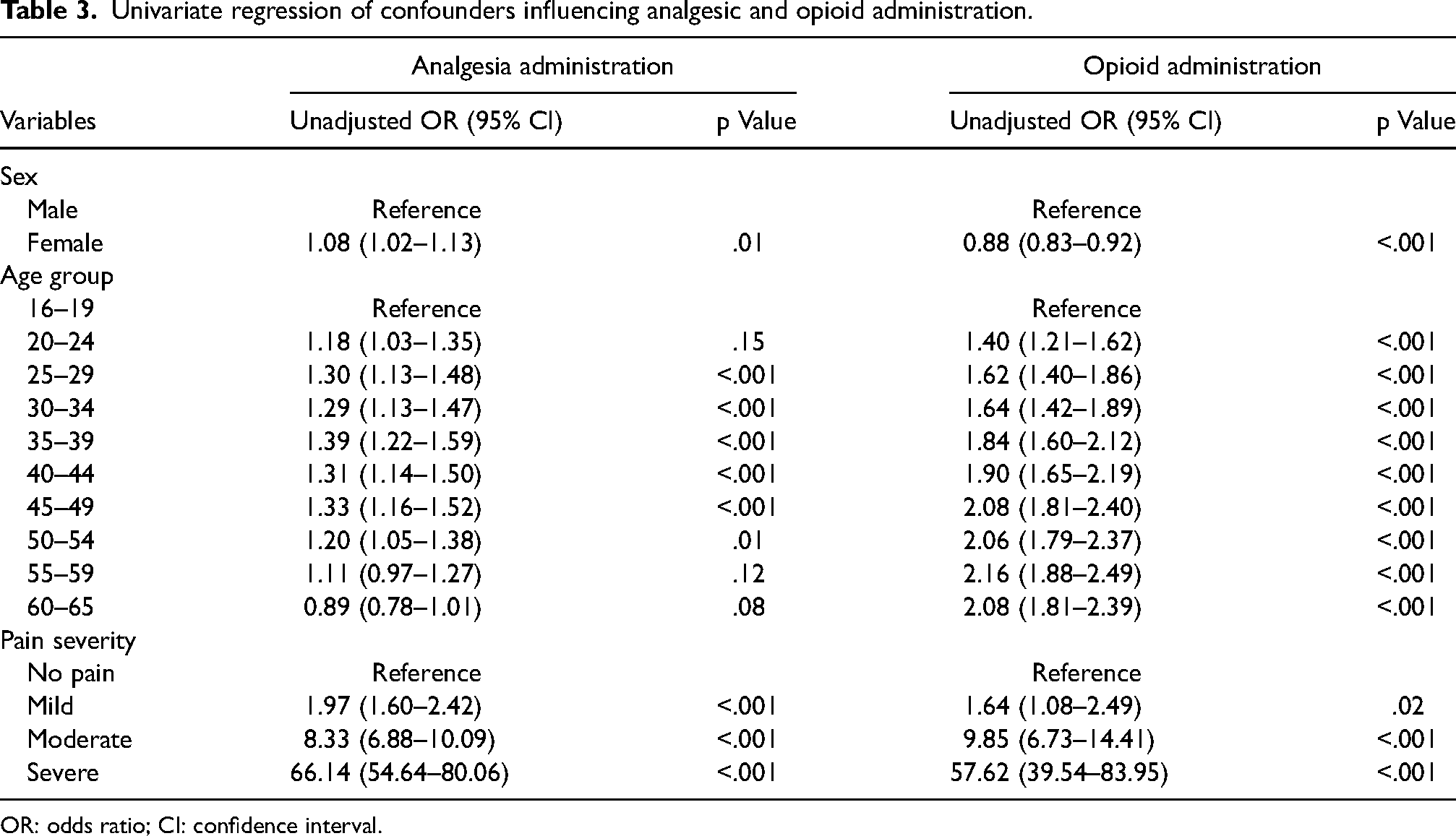
OR: odds ratio; CI: confidence interval.
Multivariate regression analysis
The regression was conducted as a complete case analysis where all variables tested for were found to be significant and therefore none were eliminated as part of backwards elimination. Interactions between variables were not analysed. The Hosmer-Lemeshow test indicated that the regression model was suitable for use in the analysis of analgesic administration (p = 0.50) and opioid administration (p = 0.37). Multivariate regression results are outlined in Table 4.
Multivariate regression of confounders influencing analgesic and opioid administration.
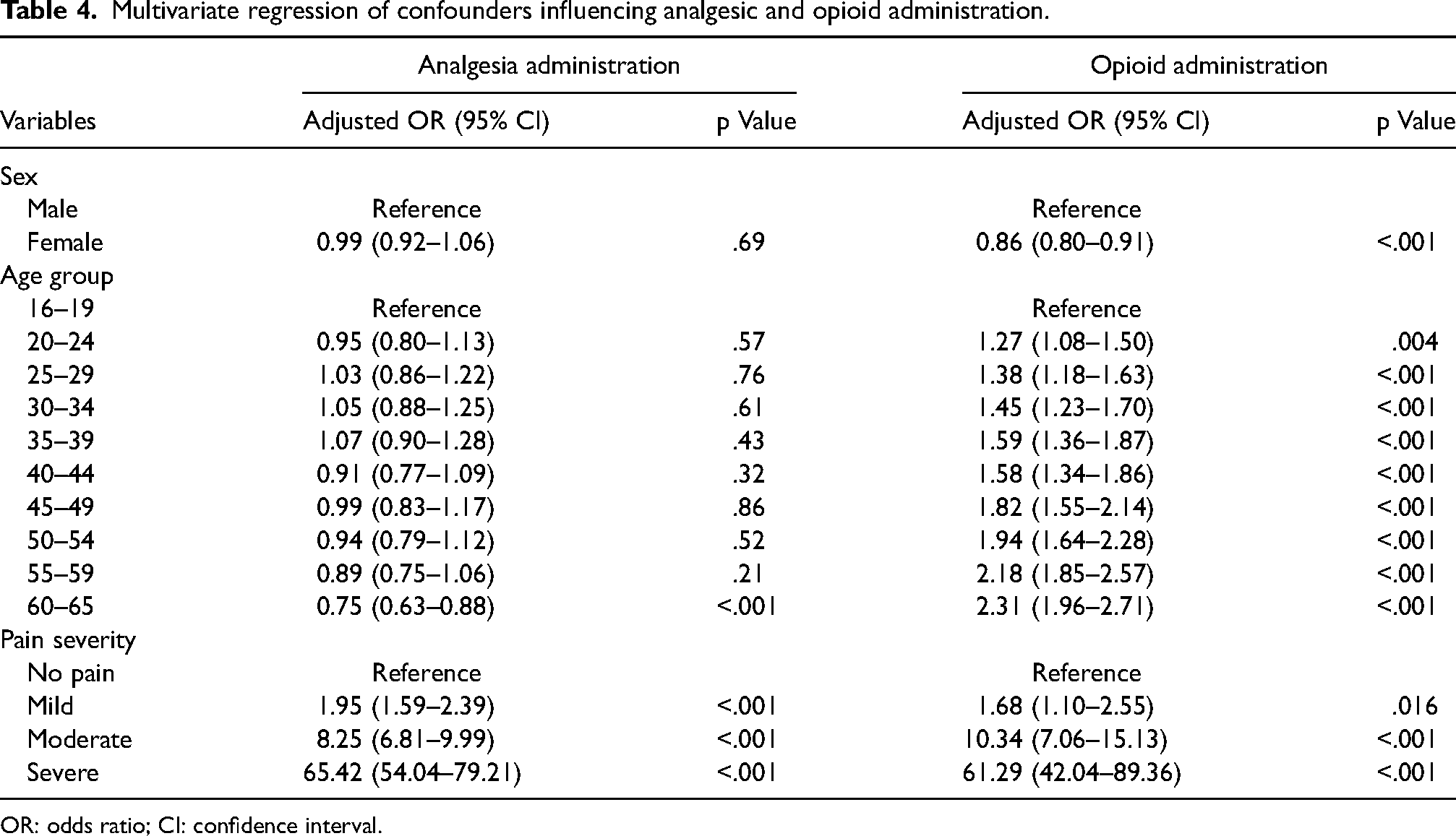
OR: odds ratio; CI: confidence interval.
Analgesic administration
After adjusting for confounders, the regression indicated there was no significant relationship between sex and analgesic administration (aOR 0.99; 95% CI 0.92–1.06; p = .69). Patients between the ages of 60 and 65 were found to be at lower odds of analgesic administration (aOR 0.75, 95% CI 0.63–0.88, p < .001). No other ages were found to be significant. Patients presenting with a higher pain severity had higher odds of receiving analgesia. Namely, patients with severe pain had greater odds of receiving analgesia than those with moderate, mild or no pain.
Opioid administration
After adjusting for confounders, the regression indicated that females were at lower odds of opioid administration than their male counterparts (aOR 0.86; 95% CI 0.80–0.91; p < .001). There was evidence that the odds of receiving analgesia increased with age. That is, patients between the ages of 60 and 65 were at greater odds of opioid administration than a patient in any of the other age group. Patients with a higher pain severity had greater odds of receiving an opioid. Specifically, patients with severe pain had an opioid administered more frequently than those with moderate, mild or no pain.
Discussion
The aim of this research was to attempt to identify if there was a difference in pharmacological analgesic management between females and males when they present with abdominal pain to an Australian ambulance service. This study evaluated 26,417 patients between the ages of 16 and 65 who presented to the JAS with a primary complaint of abdominal pain. Evaluation of the statistical data were conducted via deductive reasoning in correspondence with significance levels, as statistical significance does not necessarily correlate to clinical significance.40,41
After adjusting for confounders of age and pain severity, no significant difference between the sexes in overall analgesic administration was found. This finding is consistent with other studies that investigated paramedic management of pain and found that sex had no influence on analgesic administration.42–46 Two studies that investigated patients who presented to paramedics due to traumatic causes only, indicated that analgesic administration is not affected by a patient's sex and is instead based on the severity of pain described by the patient.43,45 Another study found that while patient sex did not influence analgesic administration, female paramedics were found to provide better analgesic administration noted by greater reduction in pain score. 46 Lord et al. 47 and Siriwardena et al. 44 alternatively found that the sex of the paramedic was not associated with analgesic administration. This present study's finding of no difference between the sexes in analgesic administration is indicative of equitable pharmacological management for abdominal pain by paramedics.
To qualify the above, this present study did find statistically significant differences in opioid administration between the sexes after controlling for age and pain severity. That is, females were found to be at lower odds of being treated for pain using an opioid than their male counterparts. This result is consistent with other studies investigating gender-biases in relation to pain management in the field of paramedicine.42,47–50 Three studies found that after conducting multivariable regression analyses, females received less opioids than males.42,47,50 It is of note that the studies by Lord et al.42,47 and Bendall et al. 48 that identified a sex-specific discrepancy in opioid administration were conducted on Australian JAS data. This may indicate that inequitable pain management practices and education on sex-specific presentations may not have changed significantly in Australia since the initial study in 2009 by Lord et al. 42 to this present study.
The presence of sex-specific disparities in opioid administration is also well documented in emergency department settings. A recent study found that females presenting with abdominal pain had lower odds of analgesic and opioid administration than males with the same complaints. 19 Another study found no sex differences in opioid administration as a whole, however when investigating abdominal pain, identified that females were less likely to receive opioids. 51 Not dissimilar to this present study, Safdar et al. 20 and Chen et al. 52 found no differences in analgesic administration between the sexes, however when investigating opioid administration, males were found more likely to receive an opioid than females. Whilst these studies indicate a sex-specific disparity in opioid administration, the emergency department differs greatly to pre-hospital paramedic practice. These results do highlight however that if sex-specific disparities can be identified in different healthcare settings, then they are likely to exist in healthcare as a whole.
While it is not inherently clear what is driving this opioid-related disparity, one explanation may come from investigating the sociocultural aspect of the biopsychosocial model of health. Gender roles refers to the social beliefs surrounding masculinity and femininity, and encompasses generalisations about appropriate male and female behaviours. 12 Numerous studies have indicated that these gender roles can strongly influence and explain many of the sex-specific disparities observed in relation to pain.8,11,12,53–55 Other research found that males tend to have lower pain ratings, and a higher pain tolerance and threshold, whereas females express pain more frequently and in multiple sites, whilst accepting pain as a normal part of life.6,8,10,55 Moreover, it is indicated that in relation to pain, females report and seek medical advice more often than males do10,16,18–20,56 with a recent study conducted at a specialist pain clinic in Brazil indicating that twice as many females than males sought professional help. 17 It can be deduced that if an individual's environment shapes a person's responses, beliefs and actions, then the same can be said about an individual's response and management of pain. This understanding shines a light on the gender-biases that are most likely present in healthcare. It is worth noting that this study highlighted that males have higher odds of receiving an opioid, however when investigating analgesic administration in its entirety, no differences between the sexes were found. The findings of this study and those in the literature point to a flaw that may exist in pharmacological pain management. Through rational conjecture, it could be argued that if it is socially understood that males complain of pain less frequently, then when one does, their pain must be valid, and justifies stronger analgesia such as an opioid. Alternatively, it could be postulated that if females are socially perceived to have a lower threshold for pain, then one does not appreciate the severity of their pain and they are less deserving of receiving opioids. This social conditioning of patients and practitioners may be a driver of this sex-specific disparity found in this study in relation to opioid administration. The concern that emerges is for patient safety from possible over-administration on one hand or an unmet pain management need on the other, leading to inequitable pain management.
While there is much evidence to indicate that uni-dimensional pain assessment tools, such as the verbal numeric rating score (VNRS), is a valid, reliable, and sensitive tool for pain assessment, especially in the short term,57–61 there is also evidence to suggest that using this tool exclusively may not improve pain outcomes.62,26 A recommendation can therefore be made for paramedic education on multidimensional pain tools that encompass the different aspects of the biopsychosocial model to ensure management is best suited to the patient's individual pain experience as opposed to a single self-reported pain score number.58,62–64 While some of these multidimensional tools may not be practical due to time and setting constraints, embracing more diversity in pain measurement instrumentation may enhance and promote equity in care and allow a more tailored approach to treatment and better pain outcomes.62,64
Another finding in this study was that females presented more commonly with abdominal pain, with females comprising 61.6% (n = 16,271) of the patients, accounting for nearly two-thirds of the population: like that seen in the literature in various settings. In three different studies performed in various settings, females complaining of abdominal pain comprised of more than 60% of the included participants.16,19,20 These findings therefore indicate that this present study's sample population being made up of 61.6% females, is unlikely to be due to chance. When investigating the biological aspect of pain as per the biopsychosocial model, it has been reported that females have a lower pain threshold and tolerance, greater unpleasantness with pain, and more painful sensations both during and after stimuli removal.53,56,65–67 Existing research also indicates that females experience higher intensities and sensitivities for various modalities of pain such as heat, ischaemic and pressure pain.6,8,10,68 Males have thus been shown to demonstrate a higher threshold and tolerance for pain in comparison to their female counterparts overall.53,56,66,67 Moreover, females are found to present more frequently with gastrointestinal pain than males, with the female specific hormones of oestrogen and progesterone enhancing this presentation.21,54,69 It has been reported that two-thirds of irritable bowel syndrome diagnoses are in females, with females reporting more prominent gastrointestinal discomfort and somatic symptoms than males.12,16 It must also be noted that gynaecological presentations such as endometriosis, polycystic ovarian syndrome, and menstrual conditions, compound the female prevalence of abdominal pain in the population.70,71 These findings thus further indicate that sex has a significant impact on abdominal pain presentation and experience and may explain why this and other studies found females to present more frequently with abdominal pain than males. The implication is that gender inequity in pain management may be compounded in abdominal pain cases.
An essential recommendation of this research is to encourage more in-depth education on how the different sexes present with abdominal pain and why, whilst also highlighting metacognition and unconscious biases that may exist in practice. Enhancing paramedic decision making through tailored education, may hold benefit in improving pain management assessments and paramedic practices overall. 72 Further research using qualitative methods may also allow for a deeper understanding into paramedics’ decision making, and their behaviours and beliefs of analgesia and patient presentations.
A further finding from this research was that patients presenting with a higher pain severity were administered any type of analgesia, and opioids specifically, more frequently than those with lower severities after controlling for sex and age. That is, patients with severe pain had higher odds of receiving analgesia than those with moderate, mild or no pain. Association testing also found that pain severity had a strong statistically significant relationship with analgesic administration and opioid administration. This is demonstrative of ideal pain management where individuals are treated for their pain based on their own subjective scoring of pain severity.
The analysis also noted very small variation in opioid dosages between the sexes, with the only difference present in the IQR. This difference would hold no clinical significance. It is unsurprising these were similar however, as the protocols that the JAS paramedics operate in indicate an initial medication dosage that is not based on pain score or weight.
From these results, a recommendation can be made to make pain score a mandatory field to be completed by paramedics on an MR. An option of unable to rate pain and a free text component allowing paramedics to input other methods used to ascertain pain score would also be available. This would ensure that regardless of a patient's presentation, all patients were to be asked about the presence of pain, as a form of universal pain screening.
Another recommendation is that of analgesic prompts on an MR telling paramedics to consider analgesia for certain pain scores. For example, as used in this research, when a paramedic inputs a pain score between 7 and 10 indicating severe pain,57,73 the MR would provide a prompt asking the paramedic to consider an opioid medication. If a paramedic does not provide an opioid medication, it becomes mandatory to provide a reason for withholding analgesia. This visual prompt may influence paramedics to consider the type of analgesia they are administering and if it may be more appropriate to provide a different one. This may additionally assist in organisational changes as it would increase ease of auditing of pain management practices. This recommendation would mean that paramedics are more cognisant of tailoring pain management decisions directly to patients’ pain experiences, notwithstanding the nuance of sex.
This research has demonstrated that an opportunity exists for paramedics to recommit themselves as patient advocates in relation to equitable pain management and patient safety. Paramedics are not the gatekeepers of analgesia and should always aim to reduce a patient's pain efficiently and effectively where possible. Ambulance services and paramedicine programmes too have the responsibility of enabling such advocacy, in the interest of equitable pain praxis.
Limitations
Firstly, to undertake this research, retrospective data had to be used, and thus findings were limited by the quality of information provided on the MRs. For example, 8.3% (n = 2190) of initial pain scores were missing as it is not a mandatory field on the MR. Missing information therefore could not be accounted for. The VNRS was used to measure pain scores as part of the broader pain assessment which as previously stated, is not the most robust or reliable measure of pain. Authors were also limited in adjusting for confounders such as patient's weight, attitude towards analgesia, and current analgesia practices, as they could only control for those included in the dataset provided. The use of multiple regression modelling mitigated this somewhat.
Secondly, the free text narrative section of the MR that may have held valuable information surrounding alternative pain assessments or analgesic management decisions were not investigated due to the volume of data analysis exceeding the scope of this research.
Thirdly, a Glasgow Coma Scale (GCS) of <15 may result in a reduced ability to articulate a pain score and may prejudice analgesic administration, which may negatively impact accuracy of the data analysis. As it is not a mandatory field to complete in the MR, and as paramedics are trained to manage pain in the absence of pain scores, lowered GCS did not result in study exclusion and remains a limitation.
Fourthly, there is no ethically sound way to definitively ascertain a patient's sex and therefore engendered assumptions of a patient's sex may have been made by paramedics. The MRs do allow for a third option of indeterminate when selecting a gender, which in this dataset, four patients were classified as such. This small number did however mean that no analysis could be performed on this population as it fell below the threshold requirements of statistical analysis.
Finally, the analysis was based on a dichotomous result of yes or no for analgesic or opioid administration. No analysis was conducted on initial and overall analgesic dosages, and/or on the effectiveness of provided analgesia, which may have yielded a different conclusion. Moreover, interactions between variables such as sex and age were not conducted during analysis, however the authors do not believe this would have been clinically significant and changed the overall interpretation of the results.
Conclusion
This research study aimed to determine the influence of patients’ sex on paramedic administration of analgesia and specifically opioids in cases of acute abdominal pain presenting to an Australian JAS. Whilst analgesic administration in general is equitable between the sexes, females complaining of abdominal pain have lower odds of receiving opioids in comparison to males when treated pre-hospitally by a paramedic. The results reinforced the understanding that higher pain scores translated to better analgesic management. Four recommendations of multidimensional pain tools, mandatory pain score measurements, MR analgesic prompts, and further education were provided to assist in addressing gender-biases in paramedic pain management and enhance equity of care.
Footnotes
Acknowledgements
The authors would like to express their appreciation to Dr Paul Fahey, the Senior Lecturer for Biostatistics for the School of Health Sciences at WSU, for his wealth of knowledge and guidance in the statistical analysis component of this research.
Author Contributions
This research emanates from the Master of Research thesis by Sooaad Dahoud. The thesis was supervised by Dr Navindhra Naidoo and Associate Professor Paul Simpson. All authors contributed to and approved the manuscript with thesis reference of: Dahoud S. The Influence of Patient Sex on Paramedic Administration of Analgesia for Acute Abdominal Pain [thesis]. [Sydney (Au)]: Western Sydney University; 2023. All authors of this article therefore meet the requirements for authorship.
Data Availability
Due to the nature of the research, anonymity of the jurisdictional ambulance service, and the ethical considerations surrounding patient information and identifiably, supporting data is not available.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research and/or authorship of this article. In respect to publication, Paul Simpson is the Editor in Chief of Paramedicine and Navindhra Naidoo is an Associate Editor at Paramedicine. Neither played any role in the review process nor in the editorial decision making process. The paper underwent double-blinded review in adherence to the journal’s peer-review policy.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Correction (May 2024):
This article has been updated with University name in ‘Ethical Approval' section.