
Abstract
Introduction
Rural and remote communities across Canada face significant challenges that urban areas do not, including barriers posed by inclement climate patterns, geographic remoteness, socioeconomic disparities, and more limited access to healthcare services, including appropriate and reliable paramedic care. 1 Taken together, these factors contribute to the worse health outcomes of rural residents.2,3
There has been an increasing focus on the development of new primary care services over recent decades. This has included a recent expansion of traditional paramedicine roles to include new and emerging integrated roles that can provide high acuity support across multiple community and healthcare settings.4–6 As highlighted by Tavares et al. (2025), these rapid transitions are giving rise to new roles that are augmenting interconnections between emergency and community services as a way of addressing complex healthcare challenges and better aligning with community needs. 7 One example of this is the role of the Advanced Care Paramedic (ACPs), which until recent years has been largely concentrated in urban settings with higher call volumes and greater requirement for the advanced skill set. 6 Their training provides ACPs with additional expertise in patient assessment and management, including cardiac monitoring, endotracheal intubation, and intravenous drug therapies.4–6 While great successes have been seen in high acuity situations, including documented reductions in emergency department (ED) utilisation,8,9 new modes of practice have emerged over recent years with ACPs taking on expanded roles within community settings.
Community paramedicine (CP) is well established across Canada and the world with increasing evidence to support its effectiveness in improving healthcare delivery.4–6 CP programs have evolved to be diverse and flexible, aiming to address health service delivery gaps and challenges. These roles are community-facing and expand beyond emergency care to include a broad range of preventative and primary care practices. The implementation of CP roles across Canada has prompted the Canadian Standards Association has developed a framework to guide program development. 10 In British Columbia (BC), a province in Western Canada, the CP program has recently expanded to include an ACP role specifically targeting rural and remote communities, coined the Rural Advanced Care Community Paramedic (RACCP).
The RACCP role builds upon the existing ACP and CP roles, providing a foundation for scheduled and emergent care for patients with higher acuity needs. RACCPs utilise their advanced skills and extended scope of practice to provide a broad range of care, with the aim of being responsive to community and patient needs. This role spans a diverse range of scheduled and unscheduled activities across diverse settings. For example, an RACCP may provide a range of scheduled community health assessments and care, including health assessment and monitoring, administration of medications, and provision of palliative care. In addition, unscheduled community care may be offered through informal drop-ins at a range of community settings, including safe injection sites. Finally, advanced emergency care is also offered, including deployment to life threatening pre-hospital emergencies or supporting urgent care needs within acute care settings, such as conducting endotracheal intubation in the emergency department (ED). Similar models have been successful in other jurisdictions, including Ontario (Canada), Australia, New Zealand, and the United States. 1 11–15 In Ontario, a recent initiative involving the implementation of community paramedic health evaluations led to a 24% reduction in traditional acute emergency medical service use, as well as significant reductions in ED visits and hospital admissions. 16 Furthermore, one recent study highlighted that there were high levels of community satisfaction associated with these expanded roles. 15
The evidence underpinning these expanded CP roles continues to develop and further research is needed to examine implementation and long-term impacts. 17 The overarching goal of this project is to examine the barriers and facilitators impacting the implementation and integration of the RACCP role in BC, a large Canadian province with approximately 18% of the total population dispersed across small and dispersed rural and remote communities. This work is guided by the question: does the implementation of RACCPs enhance healthcare access and delivery in five rural and remote communities in BC?
Methods
Qualitative approach and research paradigm
This research is guided by integrated knowledge translation (IKT), a collaborative approach to research that requires meaningful partnerships with knowledge users, including those most affected by an issue or those best positioned to influence change. 11 A qualitative descriptive design was adopted for this study, allowing for interpretive processes that remain close to the descriptions of the phenomenon in focus. 18 Grounded in a naturalistic and relativist approaches, qualitative description supports both deductive and inductive explorations of experiences as they occur within the natural context. 19
Researcher characteristics and reflexivity
Our research was co-produced with knowledge user partners from the British Columbia Emergency Health Services (BCEHS) and team members that included healthcare providers (a nurse and two emergency department physicians), health system decision-makers, researchers, and health research trainees. Collectively, team members contributed diverse perspectives related to paramedicine practice, healthcare delivery, and health research. The research team designed the study collaboratively and met regularly throughout the study. Each team member's feedback was considered as we progressed through the project and the Principal Investigator (PI; DB) guided the process, as an experienced qualitative researcher.
Reflexive practices were encouraged throughout, allowing team members to recognise, discuss, and challenge their presuppositions, positions, and perspectives. How positionality intersected with the findings and analysis was actively explored through guided discussions. 20 One example of this was related to rural and remote healthcare, whereby team members often immediately focused on challenges, deficits, and disparities, despite good evidence of community agility, resilience, and strengths in the data. Likewise, for those leading the analysis (DB, AM, JF, KG), reflexive journaling and memoing was undertaken to interrogate and refine emerging analytical data.
Context and sampling strategy
This study was undertaken in British Columbia, Canada and was focused on five communities that were considered rural and/remote in nature by virtue of their population density and geographical distance from a larger metropolitan centre. Purposive and snowball sampling techniques were utilised to recruit our study sample. To be eligible, participants needed to be directly engaged in, or have experience of, healthcare delivery in one of the community sites, have engaged with BCEHS and/or an RACCP, or be an RACCP. All participants were required to provide informed consent. As each community had some unique features associated with the RACCP role, including operating practices, geography, infrastructure, and staffing, participant characteristics (e.g., types of roles) differed between sites.
A total of 36 interviews were conducted with 31 unique participants from five communities, of which most participants identified as male. Of these, 27 participants completed interviews during Phase One and nine participants during Phase Two. Five participants completed an interview in both Phases One and Two, allowing for the exploration of perspectives over time. Participants included health authority and emergency services staff, RACCPs, decision-makers, healthcare providers, and community knowledge users. Attempts were made to recruit a diverse sample; however, it was challenging to recruit physicians, community nurses, and community members. Nonetheless, we were able to recruit two nurses and an emergency department physician. Recruitment during Phase Two was delayed due to COVID-19 and was complicated by high levels of turnover and vacancy in RACCP roles. In addition, significant health human resource shortages across all healthcare disciplines and community sites were described, impacting the ability to recruit a diverse and larger sample of participants with direct experience of the RACCP role. Further, community sites varied with respect to the implementation timing, with some communities being early within the RACCP implementation, while others were 1 to 2 years into the implementation process. Thus, two communities had limited engagement due to delayed recruitment or deployment. To reflect this, data were coded for each phase, but themes were developed across both phases. Examples specific to each phase were delineated in the analytical descriptions as appropriate. Data saturation, or the point at which no new major themes emerged from the data, was achieved for this study.21,22
Ethical issues pertaining to human subject
This research was reviewed and received harmonized research ethics board approval (E2018.1005) with the University of Northern British Columbia Research Ethics Board as Board of Record. Prospective participants were provided with a comprehensive information sheet and consent form, along with opportunities to seek clarification and ask questions. Ongoing consent was prioritised, and participants were asked to reconfirm their verbal consent prior to any data collection. All data were de-identified, and efforts were made to promote the anonymity and confidentiality of the participants. Given that some participants hold prominent and one-of-a-kind roles within some communities, participants were made aware that confidentiality cannot be completely guaranteed. Where concerns of potential identification exist, participants were able to edit, remove, or keep any quotes or data. Access to data was restricted to the research leads and trained research associates and was stored on secure password-protected and encrypted servers.
Data collection methods, process, and analysis
Qualitative data were collected across two phases. Interview questions were developed in partnership with our BCEHS community partners to reflect the key functions of the RACCP role. Interviews were undertaken virtually, using a secure Zoom platform, and were digitally recorded and transcribed verbatim by a professional transcriptionist. Interviews ranged from 45 minutes to over 2 hours in duration. Phase One focused on the early implementation period (March 2019 and February 2020), and Phase Two interviews examining the integration of the RACCP role up to 2 years post-implementation (May–December of 2022). We worked with our partners to determine the best timing for data collection. We engaged participants from five rural and remote communities across BC.
Because data were gathered over two phases, it allowed us to conduct a comprehensive analysis of RACCP implementation over time.23–25 We utilised the theoretical domains framework (TDF), a framework that is grounded in over 120 different constructs and theories and organised into 14 domains, to categorise behavioural and organisational factors that influence implementation practices and outcomes. These domains include knowledge, skills, memory, attention and decision processes, behavioural regulation, social/professional role and identity, beliefs about capabilities, optimism, beliefs about consequences, intentions, goals, reinforcement, emotion, environmental context and resources, and social influences.25–27 The TDF was used to sensitise data collection and analysis, frame potential behaviour and implementation barriers, and explore facilitators of RACCP integration. 27
Analysis was guided by the Qualitative Descriptive approach and TDF. First, transcripts were each cleaned, read closely, and then coded inductively by four team members individually (DB, AM, JF, KG). Coding was iterative in nature, allowing for the emergence of meaningful phenomena and patterns. The team met to review emerging data, supporting the refinement of code groups into explanatory themes and to address inconsistencies or queries. Second, transcripts were also coded deductively according to the predetermined domains of the TDF (DB), with the aim of providing more specific insights relating to the barriers and facilitators of implementation and to frame potential recommendations. This analysis was discussed as a team and in keeping with the TDF approach,25–27 the most commonly coded domains were selected for discussion.
Techniques to enhance trustworthiness
To promote rigor and trustworthiness within our study, we considered factors of credibility, transferability, dependability, and confirmability. 28 For credibility, we established rapport with our participants and remained immersed in the data for a prolonged period, illustrated by participant quotes and the two-phase approach to our study over years. In addition, four members of the research team completed peer-checking of the results (e.g., codes and emerging themes) to mitigate individual biases. For transferability, we provided thick descriptions of the study and its results to enable the reader to understand the context and nuance within our study. In terms of clarity in sampling strategy, we were mindful of confidentiality but did provide details of our participants characteristics and roles. Dependability was established for our study by keeping an audit trail and detailed records of our study procedures, which allows us and others to trace our research activities. Confirmability was promoted within our study through peer debriefing in our research team which included diverse members. Furthermore, for those participants engaged in both Phase One and Phase Two of the study (n = 5), member checking with respect to key emerging insights was undertaken and helped informed the ongoing conduct of the Phase Two interviews. These discussions help validate our interpretations and minimise biases. Throughout the study, we engaged in reflexive practice.
Findings
Analysis of the study data gave rise to five central themes: (a) Evolution of the RACCP role, (b) RACCP scope and practice, (c) RACCPs in practice, (d) Resources and Supports, and (e) Evaluation and impact.
Evolution of the RACCP role
The RACCP role developed to address specific community needs. In Phase One, participants expressed strong support for the expanded scope of RACCP practice – encompassing blood work, prescribing and administering antibiotics, and conducting community-based assessments – emphasizing its critical, potentially life-saving impact. One participant (health system leader, female) noted it could mean the ‘difference between life and death’, while another (emergency services team member, male) explained: ‘It's just been so advantageous to have somebody with a higher level of skill, more tools in the toolbox, greater diagnostic capability, that's been like outstanding when we’ve had those opportunities’.
Addressing existing gaps in community-based healthcare and fostering more coordinated healthcare services were perceived to be key RACCP functions. Participants highlighted the opportunity for RACCPs to bolster and bridge existing services. Moreover, participants commented on the importance of the RACCP role in addressing the needs of underserved populations, including those requiring palliative care, harm reduction, and/or at-home treatment. For many, the ability to provide ‘proactive’ care in place was viewed as addressing gaps in care and offering a more acceptable pathway of care to those facing barriers. One participant (emergency department physician, male) commented: ‘I think it's going to be a potential for specific patient populations, such as struggles with mental health problems, and those who frequently make trips to the emergency department because of them not having good enough access to healthcare’.
RACCPs also contributed much needed advanced paramedic support within their communities. Participants explained that this additional level of support would streamline the delivery of urgent care within the clients’ home, enable safe patient transfers between facilities, aid in the management of advanced life support and trauma calls, and prevent unnecessary admissions to the ED or hospital. A participant (regional emergency services leader, male) reported: ‘It may also help with interfacility transfers and/or if the hospital is overwhelmed … We’re also now able to offer that advanced support in the field [and] pre-hospital 911 calls when we’re not engaged with community paramedicine’.
During Phase Two, participants expressed positivity about the RACCP role's contributions, both current and planned. They highlighted RACCPs’ involvement in diverse community and health activities, such as home visits, outreach to safe injection sites, complex patient transfers, and community health events. These evolving roles were seen as valuable for addressing unique and complex care gaps in the community. One participant (health system leader, female) expressed: ‘…because primary care access is so limited, having that advanced scope of skills really benefits these folks because that scope wasn’t just difficult to access before, it didn’t exist before in some of these communities, so it's really added something brand new that wasn’t there [before]’.
During both Phase One and Two interviews, participants identified beneficial outcomes seen in their community across all levels of healthcare, including impactful and ongoing improvements in chronic disease management, community outreach, coordinated care, mentorship, and health education. Further, direct benefits to populations that experience medical complexities were noted. Providing care in place was perceived as a major benefit, avoiding unnecessary transfer to the EDs and acute care settings. One participant (regional emergency services leader, male) commented: ‘We had a palliative care type situation where somebody was in quite a bit of pain and normally without that advanced care paramedic there we would’ve just had to transport this person… [the RACCP] was able to work in conjunction with another nurse that was there and by phone with doctor support and they were able to provide the pain relief that that patient needed without having to transport her’.
During Phase Two, deep, lasting community connections were key indicators of success. RACCPs supported diverse patients and caregivers, particularly older adults and those with complex medical needs lacking strong support networks. As one RACCP (male) explained: ‘You’re making connections not just with the client but with their families, and some of them are quite extended and you start getting really involved in not just their medical care, but as in their overall care and finding out the advocacy for things and the things that challenge them and how to connect them to different parts of the medical system or the volunteer system, the community supports that are available to support them. And so, you really develop these different relationships rather than the emergency response where you were with them for, you know, an hour…’
RACCP scope and practice
During the interviews, participants described the ongoing evolution of the scope and practices of the RACCPs within the communities and how teams navigated complex policy and regulatory issues. Two sub-themes emerged from the analysis: (a) role clarity and (b) policy, regulation, and implementation challenges.
Role clarity
During both phases, participants from all knowledge user groups described the need for greater role clarity for RACCPs, both as a means of understanding the potential scope and contributions, but also as a way of promoting and supporting their broader integration into existing healthcare services. During the early implementation period, many of the participants commented that ‘a better definition around the scope of practice would be useful’ and that ‘short term, we need to get really clear on what our desired outcomes are for the ACPs’. Likewise, others recognised the need for more clarity and guidelines around the role, particularly for those new to the role and community.
The breadth of the role and ability to deliver healthcare across multiple settings was viewed as a novel and important component of the RACCP role. However, participants identified that greater role clarity was needed, particularly in relation to delineating responsibility for, and collaboratively delivering, inpatient and outpatient care. During Phase One, some participants raised concerns about potential overlaps in care or misdirection of resources, particularly where roles may overlap with existing community-based providers. Many of the participants recognised the potential for territorialism, as well as ‘pushback’ from other healthcare providers. One participant (health system leaders, male) explained: ‘The biggest challenges we currently face is the pushback from the existing health community who feel very protective of their turf and they seem overly worried about protecting their roles rather than sort of looking at the bigger picture, like who cares who delivers what to the patient as long as that patient is getting what they need and we keep them in their houses’.
While concerns about role overlap and territorialism emerged early in the implementation process, these faded as the RACCP became more established within the community and others became familiar with their role. While RACCPs were central to educating about, and promoting uptake of, this new role, other knowledge users were important in stewarding the integration of the role. One health system leader (health system leader, male) commented: ‘[It] was an issue for both sides at the beginning, had a meeting, made it clear they were there to partner and assist, not step on any toes’.
In sum, participants continued to be supportive of the RACCP role, recognising the importance of their engagement across diverse community and healthcare contexts. Despite this, there was a desire for greater role clarity, while preserving the flexibility to be responsive to community needs.
Policy, regulation, and implementation considerations
The introduction of the RACCP role gave rise to many policy, regulatory, and implementation considerations. During the early phase, participants identified that the lack of consistent or engrained operational policies and procedures made implementation difficult. Examples of these challenges included a lack of clarity around how to deploy RACCPs in emergency, high acuity, or trauma calls, as well as the absence of procedures for referral across the wider healthcare settings. Regarding the RACCP service, one leader (health system leader, female) explained: ‘It seemed like we were still siloed… I think that happens when you’re trying to introduce a new service’ while an RACCP (male) providing scheduled and unscheduled care commented ‘I’m trying to find a way to get notified whenever there's a helicopter coming in so I can be more involved in that. Just so they can start seeing some of the medicine that we do’. As a result, many of the RACCPs and providers were faced with the need to decipher processes within each of the communities and to integrate themselves within existing systems of care.
During the early interviews, regulatory concerns about the treatment and release of clients within the community context arose. In particular, the lack of formalised referral processes was seen as a barrier and contributed to concerns about potential disconnections in care. One participant (community organisation leader, male) explained: ‘One of his regular customers… fell and broke her foot on the ice, so [the RACCP] was the one who knew her best because he had seen her every week for weeks beforehand and yet he wasn’t supposed to be going to make a call on her unless a doctor referred him, which I thought was really a gap in the whole service’. ‘They were supposed to be sent on all red and purple calls and any calls that the crews requested them on and it took a long time for that to get down to the dispatch and the dispatch [to] be willing to send them. And now they are willing to send them on crew request, but it seems to be hit and miss if they remember there's an ACP in town …Dispatch used to have to be paramedics, not anymore, so not all dispatchers have medical or paramedic experience, which plays a big role in why the ACP is not being sent’.
The lack of engagement in high acuity calls was a factor that many participants identified as affecting long-term retention and engagement. A key concern was that RACCPs were being overlooked, placing them at risk of losing their high acuity skills. Of note, one participant (health systems leader, female) explained: ‘a lot of those skills our folks aren’t necessarily going to even be able to touch annually, and that can lead to a diminishment of job satisfaction, decrease in confidence in your skills’.
Despite many challenges, some RACCPs were able to leverage existing interprofessional structures and practices to enhance their deployment and integration into community care. For example, RACCPs in northern BC communities were able to participate within existing community-based interprofessional primary healthcare team huddles, allowing for more effective collaboration and deployment. One RACCP (male) noted: ‘First and foremost, the easiest one was to join in on a meeting that was already established by the health authority. It's basically an interdisciplinary huddle … and there's people from across the various services and specialties that attend that from case managers, respiratory therapists, physiotherapists, myself, and what it does is it gives the opportunity to reduce some of the gaps that people are slipping through by all of us getting together in a room and saying hey I’m worried about so and so, are they followed, or who here can look after the specific need that we’ve identified has been a problem?’ ‘Unfortunately, what's going to end up happening is there's going to be a med error, there's going to be mistakes, someone is going to suffer, simply because of incomplete information… we really do need to have access to all the information that lends itself to those decisions and right now that's not in place’. ‘What I’ve done as a workaround… is phone calls and emails, trying to gather fragmented information which is not the best use of anybody's time really cause the information is already compiled somewhere, we just don’t have access’.
RACCPs in practice
The RACCPs role in responding to gaps in care was frequently discussed during the interviews. As RACCPs became engaged within communities, they worked to identify needs and deliver care across multiple settings. This included the provision of care to complex and underserved populations, including unhoused people, those with mental health concerns or substance use disorders, and seniors and clients receiving care in their home. In many cases, this enabled care to be delivered in place and avoided transfer to an acute care facility. Participants recognised that this was an excellent strategy for tailoring health promotion and services to the needs of the community. In this sense, there was the recognition that a one-size-fits-all plan for rural communities would likely not work. One RACCP (male) commented: ‘The latitude that we have in these roles to adapt to the communities is that little bit of preciousness that we have. That autonomy to just solve problems. Admin people, they have this saying that we solve problems you don’t even know you have. And that's kind of what this becomes, is that you’re solving problems that this health system doesn’t even really know that exist’. ‘While it's great for us to help out if the physicians feel they’re being overwhelmed and that we can come into an Emerg setting and lend a hand, we have to be cautious that we’re not band-aiding something that the health authority really needs to fund better’. ‘When COVID struck it kind of changed everything, my role became more, it was all telehealth and not doing visits which was really challenging for me personally to not see people. That was really challenging’.
Resources and supports
Participants frequently commented on the importance of resources and mentorship for RACCPs and the wider paramedicine community. Many recognised the value of ongoing mentorship as RACCPs adapted to their roles. They also highlighted the benefits of building a formal community of practice, though challenges like high turnover and limited communication about program changes often left connections informal. One participant (RACCP, male) noted the significance of these networks ‘There's not a lot of communication about what's happening with the program, or I don’t even get updates when people leave or someone comes in. The only way I find out is by word of mouth or someone calls me … how are we supposed to create a community if I don’t know if these people are still in it and then they disappear and then someone else comes in and then they disappear…’ ‘You don’t have your partner backing you up. As the RACCP role, it shouldn’t be as dangerous as going to what we go to as a crew, because the patients are supposedly been assessed by the doctor or in some cases the crews can sort of out forward, ya, this would be a good patient for the RACCP, but everybody has their vulnerabilities’. ‘hardening your heart to deal with these situations, it takes its toll on you … we [should] build this into the training earlier so that we start building the self-care and making it okay to have to deal with your feelings’. ‘He's got that great sort of bedside manner and instructional ability that not everybody has and it's great to have him there and be able to, like he's done some staff in-services for us and stuff. So it's nice to have that’.
Evaluation and impact
As previously described, RACCPs were perceived as making impactful contributions in their communities, bridging gaps in care, and working to address disparities among underserved communities. While participants recognised the importance of evaluation and its role in developing the RACCP program, there was not a collective sense of how the program was being evaluated, as there were no formal pathways for feedback. Furthermore, many participants reported that it is difficult to evaluate the positions, as many aspects are considered intangible or unique to each community. As one RACCP (male) commented: ‘The measuring is not by how many calls you do or how many skills you used. It's how many connections do you make in a day because it's the connections we have with each other or what measures for me that's the measure of success is the measure of connecting with the people which is a hard thing to find in a data point’. ‘To attract people and maintain and retain people they have to be interested in the work … When you take somebody who even if they’re not an adrenaline junkie that a good jolt three or four times a day and then you go to nothing for months and months and months. It's so different and so recruiting the correct people’.
Discussion and recommendations
Emerging since the early 2000s, reframed paramedicine roles have included a new focus on preventative and upstream health initiatives, particularly in rural, remote, and underserved settings. 29 This study captures the integration of the RACCP role across five rural and remote communities in a western Canadian province, drawing on the insights of diverse professional and community-based knowledge users. Key insights and recommendations are now framed through the TDF, a theoretical approach to examining behavioural and implementation factors. 26 The most commonly coded domains are applied here to inform our recommendations (Table 1).
Key recommendations framed through the TDF domains based on findings regarding the implementation of RACCPs in BC
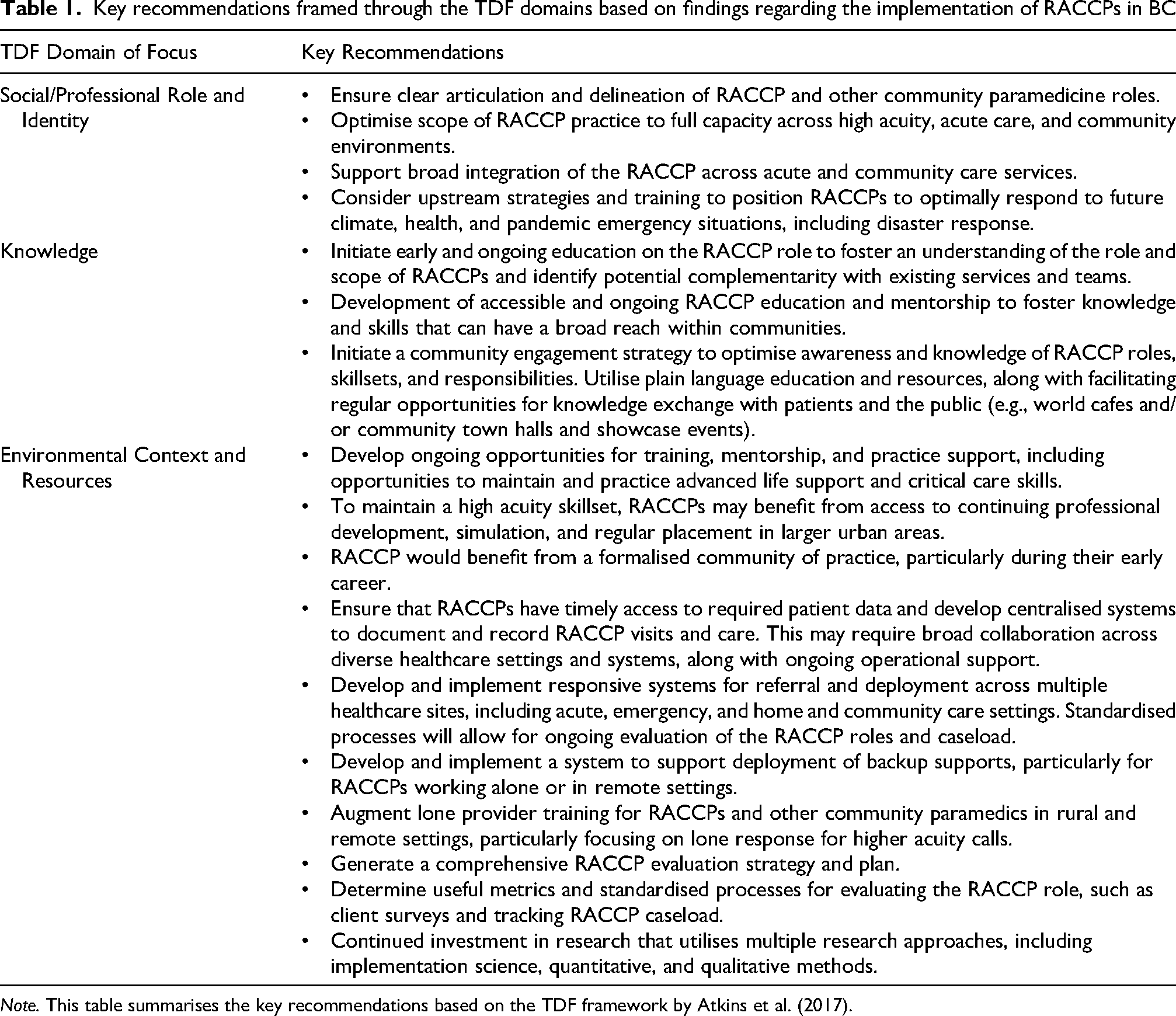
Note. This table summarises the key recommendations based on the TDF framework by Atkins et al. (2017).
In this study, participants expressed an overwhelming sense of optimism and hope for the RACCP role, noting the complex challenges that exist within their regions. As a novel community-based service, RACCP roles were seen to evolve organically to address gaps in care and respond to the unique needs of individual communities. A broad range of RACCP practices emerged, often entailing a mix of more ‘upstream’ community-based healthcare, alongside higher acuity care. While roles spanned many populations, it was typically centred on underserved populations, including older adults, patients requiring palliative care, populations who lived with housing insecurity, and substance use disorders. This broad and evolving role is reflected in the existing literature, including a study by Stirling and colleagues that highlighted how the expanded scope associated with these roles allowed providers to contribute directly to primary healthcare, while also increasing capacity for emergency response within their community. 11 These authors also noted the ability of these providers to increase the delivery of health promotion and illness prevention initiatives at the community level, a finding that was mirrored in our study. Overall, these roles provide an opportunity to reduce some of the healthcare barriers commonly faced by rural and remote residents. 30 Furthermore, the introduction of the RACCP role responds to current health system priorities, particularly with respect to increasing healthcare access in rural and remote BC and Canadian settings.31–33
Despite the excitement surrounding the RACCP program, knowledge and awareness of these roles across diverse knowledge user groups was limited, and many participants found it difficult to differentiate the RACCP from other community roles or understand their specific scope of practice. These concerns have been widely raised in the context of CP roles,34–37 with Shannon and colleagues highlighting a need for clear definitions of CP and more consistency with respect to educational preparation, scope of practice, and regulation. 35 Likewise, Rasku et al. have advocated for further research into the varied paramedicine roles in order to better understand the contributions of the distinct roles and the impacts of these roles upon key health system challenges. 29
While RACCPs reported feeling prepared for their role, they also recognised a lack of role clarity, along with the need to build relationships across the community and to shape their practice to reflect community needs. This lack of clarity persisted beyond the early implementation phase, highlighting the need for greater role clarity and further exploration of how the role integrates within existing emergency and community healthcare services. The lack of role clarity described here, along with other concerns related to varied terminology, have been widely reported, with other studies similarly recognising the developing nature of these roles, changing spaces of service provision, and changing client needs.33–41 To address this, emergency health services organisations may benefit from initiating early and ongoing education on the RACCP role and scope of practice, taking care to identify potential complementarity with existing services and flexibility to respond to gaps in care.
Along with professional knowledge users, the introduction of a community engagement strategy may similarly help to raise awareness and knowledge of RACCP roles and responsibilities at the community level. This may be achieved through the introduction of plain language resources, along with regular opportunities for knowledge exchange with patients and the public (e.g., world cafes and/or community town halls). Community-based knowledge translation approaches have been highlighted as a way to bridge the gap between health researchers and knowledge users.42–44 One example of town halls being used in Eastern Canada before integrating genomic medicine into the healthcare system. 43 Knowledge and awareness grew over the course of our study as the RACCP program was rolled out and had greater engagement within communities as well.
Data related to social and professional role and identity emerged strongly in the study. While there was support for this evolving role, challenges with integration into existing community services and policy and regulation were identified. RACCPs reported confusion and frustration when attempting to navigate what they could and couldn’t do as part of their role, particularly during the early implementation phases where there were limited scope of practice or regulatory guidelines available. Despite this, RACCPs valued the opportunity to craft and shape roles that best meet the needs of the community. Other knowledge users expressed similar feelings, contributing to uncertainty around their deployment and engagement. This lack of certainty also contributed to early concerns around territorialism and overlap with other community roles. However, concerns soon dissipated as RACCPs became more engaged within the healthcare teams. Similar challenges have been noted previously.33–36 Mulholland and colleagues highlighted the importance of positioning these advanced roles in areas of most need as a means of optimising their contributions and minimising overlap.29,39 To mitigate many of these challenges, greater clarity on core social and professional roles is needed, particularly for new providers entering these positions. RACCPs, along with healthcare and emergency services organisations, would benefit from greater collaboration to support implementation efforts. This would promote a more seamless integration of RACCPs into the interdisciplinary team and would help optimise the scope of RACCP practice. Finally, opportunities to extend RACCP roles were noted, including their optimal position to lead and support climate, health, and pandemic emergency situations, including disaster response.
Factors related to the Environmental Context and Resources emerged frequently in the analysis, including a need for mentorship, training, and formalised evaluation strategy. Participants recognised the benefits of early mentorship and support, particularly for those new in their positions or who have limited advanced paramedic experience. Likewise, training and support for other healthcare providers and community partners was recognised as a way of raising awareness of the RACCP role and ensuring smooth integration and teamwork. For example, the lack of an organised system for deployment and referral, particularly for high acuity calls, and a lack of access to healthcare records, meant that RACCPs were not fully optimised or able to respond to community needs most effectively. These factors limited engagement in some clinical areas and contributed to attrition or slow development of some skills. Difficulties related to the integration of CP roles are widely reported in contemporary literature. 28 35–38 Of note, Shannon and colleagues highlight the need to generate common understandings of roles and scope of practice, while preserving flexibility to respond to community needs. 40 Similarly, Spelten et al. warn that while there is potential to address health system challenges through these new and expanded roles, there is limited evidence of how these roles work within the context of integrated teams and their long-term impact. 38
For some RACCPs and other participants in this study, the failure to adequately support integration, along with lack of mentorship, training, and support, were seen as major contributing factors to ongoing recruitment and retention challenges. The challenges with turnover may signal a barrier and impact the sustainability of the program in the long-term. Moving forward, RACCPs may benefit from better established networks of formal and informal mentorship and oversight, allowing for more rapid knowledge exchange within the environmental context and greater resources to integrate their work. Similarly, greater standardisation with respect to orientation, regulation, and evaluation may be valued,
Beyond this, RACCPs were widely recognised as a vital community resource, particularly among paramedicine professionals and the community. RACCPs provide support for professional development, along with simulations and training for higher acuity cases. This was perceived as particularly valuable for emergency providers in rural communities, where there are fewer higher acuity calls and less access to training. Likewise, patients and community groups noted the importance of this role in providing on-the-ground support for populations who face barriers or are commonly underserved. RACCPs provide a holistic focus to care, having greater flexibility to organise and deliver care. Continued efforts to evaluate the unique and complementary impacts of RACCP practice, along with implementation and scalability factors, are needed and will contribute to a growing evidence base on CP. 41
Strengths and limitations
This study provides an in-depth exploration of the initiation, implementation, and integration of a newly evolving RACCP role in British Columbia, Canada. The longitudinal focus of the research, along with engagement of diverse knowledge user participants, created opportunities to explore barriers and facilitators over time, as well as gather examples of RACCP practice impacts. Despite many strengths, some limitations must be considered. First, the planned study timelines were impacted by COVID-19, and communities were studied at varied time points following implementation. Ongoing evaluation at regular time points would be valuable and will allow for longer term insights. Second, this study provides a qualitative exploration of RACCP implementation, as opposed to a distinct study of RACCP outcomes. Ongoing evaluation and research to capture practice outcomes is warranted, including quantitatively-derived data on the characteristics of patient visits and health system impacts, such as reductions in ED or hospital admissions. 35 The majority of our participants identified as male and future studies may choose to recruit a more diverse sample for additional insights. Moreover, studies may also attempt to recruit patients who have experience with RACCPs to gain further context as well.
Conclusion
Paramedicine practice has evolved considerably over recent decades and a new focus on community-based roles has emerged. The newly developed RACCP role in BC is one example of combining both primary care practice and advanced high acuity pre-hospital care. This study captures the integration of the RACCP role across five rural and remote communities in a western Canadian province, drawing on the insights of diverse professional and community-based knowledge users. The data from this study offers strong support for the RACCP role, noting the potential to address complex healthcare challenges within rural and remote communities. The RACCP role evolved to allow for care to be provided in place, preventing admissions to acute care and providing services to commonly underserved populations. While all participants were strongly positive about the RACCP role, a lack of role clarity, challenges in integrating within existing healthcare services, and policy/regulatory issues were seen as key barriers. Ongoing education, mentorship, and training are needed to best support the optimisation and integration of RACCP roles, along with comprehensive evaluation strategies to examine its impact.
Footnotes
Acknowledgements
First, this research was undertaken in rural and remote communities across British Columbia, Canada. In doing so, the authors wish to express our gratitude to be guests and visitors on the unceded, traditional territories of many Indigenous Peoples, whose ancestors have inhabited these lands for countless generations. Second, the authors thank our partners at British Columbia Emergency Health Services (BCEHS) for supporting this research and the Rural Coordination Centre of British Columbia who graciously funded this research. Finally, the authors would like to offer our sincere thanks to all of those that participated in this project, their passion, time, and wisdom were inspirational.
Ethical considerations
This research was approved by the BC harmonised research ethics board (#E2018.1005).
Consent to participate
Participants were provided with a comprehensive information sheet and consent form and were asked to provide written or verbal consent restricted to the research leads and trained research associates.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Rural Coordination Centre of British Columbia (RCCBC) Rural Research Grant to conduct this research.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.