
Abstract
Background
As ambulance services respond to a growing number of out-of-hospital deaths, supporting bereaved families is increasingly recognised as an important aspect of paramedic care. Actions from ambulance personnel can significantly shape family experiences, underscoring the need for compassionate, evidence-based care in the event of a death. However, currently, little is known about the needs and perspectives of families during these events, particularly from Indigenous and culturally diverse populations. This study explores the experience of Māori and non-Māori families from Aotearoa New Zealand who were present at a death where emergency ambulance services responded.
Methods
This qualitative study, underpinned by kaupapa Māori research principles, explored family experiences of emergency ambulance care in the context of a death. Participants were recruited through purposive volunteer sampling, with invitations shared via local and social media. Semi-structured interviews employed a collaborative storytelling approach, where researchers and families co-constructed digital narratives of their experiences. Data were analysed using Braun and Clarke's reflexive thematic analysis.
Results
We conducted 21 interviews with 23 bereaved family members. Families described having emotional, cultural and spiritual needs during out-of-hospital deaths. Four themes influenced the experiences of family. Making space for family highlighted the importance of meaningful presence and shared decision-making. Compassionate family care reflected the positive impact of compassionate actions. Communication, which was clear and timely, assisted family understanding. Finally, closure in crisis revealed how follow-up support is needed to help families process and accept death.
Conclusion
Care that centres empathy, shared decision making, clear communication and responsiveness to individual family needs can improve the experiences of bereaved families. Greater consideration of family needs during resuscitation and its termination is needed to challenge current care paradigms, which equate family presence with family support. Enhancing cultural and spiritual responsiveness offers an opportunity to provide more holistic and culturally safe bereavement care.
Background
In the face of an aging and co-morbid population, emergency ambulance services are attending increased numbers of out-of-hospital deaths.1,2 Paramedic care during these events has evolved over previous decades, with termination of unsuccessful resuscitation in the community becoming common. 3 Similarly, new models of paramedicine care mean that paramedics are attending palliative and end-of-life care scenarios where supporting death and dying within the community has become a care priority. 4
Most deaths attended by emergency ambulance will occur in the home, where family members are often present. 5 Experiencing the death of a family member is an emotional and challenging event, meaning that emergency ambulance services care must navigate the provision of clinical care, alongside attending to the emotional needs of grieving family members. Family grief experiences in out-of-hospital deaths are further complicated by the often sudden and unexpected nature of events, which has been associated with an increased risk of prolonged or complicated grief experiences.6,7 Literature from in-hospital and palliative care settings emphasises the importance of bereavement care in improving family grief experiences. 8 Providing quality bereavement care is important, as ambulance personnel's actions can directly impact bereaved families’ experiences and emotional recovery.9,10 However, the transferability of in-hospital bereavement care to emergency ambulance settings remains unclear, particularly given the limited training in grief support received by ambulance personnel. 11 Recent scholarship has called for greater understanding of how evidence-based bereavement care, which is culturally safe and person-centred, can be provided during out-of-hospital deaths.8,12,13 A challenge in examining previous literature on this topic is that much of the evidence focuses on the perspectives of ambulance personnel, leaving the voices of bereaved families largely unheard. 14 Lack of Indigenous and minoritised service user experiences within paramedicine research similarly challenge our understanding of what diverse families may need. 15
To improve paramedic care during death, dying, and bereavement, we must first gain a better understanding of families’ experiences, needs, and wishes during out-of-hospital deaths. This qualitative descriptive study aims to address this research gap by exploring the experiences of families in Aotearoa New Zealand who are present during an out-of-hospital death where the ambulance responds.
Methodology
Study setting
Aotearoa New Zealand has a population of over 5 million people, with Māori, the Indigenous people, comprising 20% of the population. 16 Māori face significant health inequities, including a higher incidence of out-of-hospital cardiac arrests and lower survival rates when compared to non-Māori. 17 Most of the total population (86%) resides within urban centres. 18 Large regions of rural and remote areas provide geographical barriers to healthcare delivery, which further perpetuates health inequities for Māori. 19 Ambulance care is delivered by two services operating under increasingly autonomous Anglo-American models. 20 Paramedics are registered healthcare professionals with bachelor-level qualifications. Other on scene responders within the ambulance workforce include volunteers, emergency medical technicians, and specialist paramedics. In this study, all dispatched emergency medical services personnel are referred to study as ambulance personnel.
Research design
Due to the absence of evidence exploring family experiences during out-of-hospital death in Aotearoa New Zealand, we recognised the importance of capturing a diverse range of family perspectives. Therefore, this study intentionally aimed to include Māori and non-Māori family experiences during an out-of-hospital death where ambulance services responded. To ensure research was culturally safe and responsive to the needs of Māori, this qualitative study was guided by Kaupapa Māori research principles and aligned with Te Ara Tika guidelines for ethical research with Māori. 21 Kaupapa Māori principles were applied across all participant interactions, reflecting our belief that all families would benefit from culturally safe research that upheld Māori principles. This research was situated within a constructivist epistemological stance, which acknowledges that the experiences of families and the researchers’ interpretations are shaped by social and cultural influences. 22
Researcher positionality
The research team included an interdisciplinary team of emergency nurse academics (ES and NA), a paramedic academic (BD), and social scientists (MG, TMM). Māori researchers include lead author ES, who is of Māori (Ngāpuhi) and Pākehā (New Zealand European) descent, and TMM (Ngāi Tai and Ngāti Pōrou). Co-authors NA and BD are of Pākehā descent, and author MG is of English and Welsh ancestry. Expert cultural guidance was provided by Kaumātua (respected elders) from the Te Ārai Kāhui (advisory group of Māori elders) of the Te Ārai Palliative Care and End-of-Life Research Group to ensure cultural safety of this study, the researchers and the participants. Including service users in this research was an important theoretical consideration.14,23 A service user with lived experience of out-of-hospital death contributed as an advisor and participant, offering family perspectives across all stages of the project.
Eligibility
Participants were eligible if they self-identified as ‘family’ and were present during an out-of-hospital death in Aotearoa New Zealand where ambulance services responded. We defined family following the kaupapa Māori definition of whānau, which considers family collectively and includes family members who are linked by kinship and social relationships. 24 All clinical scenarios, excluding forensic cases, were included. Instances where death did not occur in the community were excluded. No restrictions were imposed on the minimum or maximum time elapsed since the event, as evidence shows that it is unfeasible to set a standard timeframe that would reliably minimise research harm.25,26 Therefore, we adopted recommendations of volunteer self-selection that centred participant autonomy by allowing families to choose to participate at any point post-bereavement. 27
Recruitment methods
Recruitment used indirect convenience methods and was primarily conducted through electronic flyers shared on social media. Additional recruitment methods included snowballing and local media advertisements. This recruitment strategy was chosen due to limited access to family contact details and to minimise potential harm by avoiding unsolicited contact with bereaved family members who may not wish to participate. Flyers shared a fictional bereavement story which was informed by the service user advisor and authors’ previous research, clinical and lived experiences. The flyer was designed to resonate with potential participants and invite them to share their own stories. Flyers also outlined study details and noted that participants would receive a voucher to thank them for their time. Interested participants were instructed to contact the primary researcher, who provided further study information, screened for eligibility and arranged a time and location for an interview that was convenient for the participant. We estimated that 10–20 participants would be needed to achieve information power. 28 This was continuously evaluated through data collection and analysis. The decision to conclude recruitment was informed by initial reflexive thematic analysis (RTA) and discussion between researchers, which indicated that interviews yielded rich data sufficient to address the research objective.
Data generation
Data was generated through semi-structured interviews in two recruitment phases (April–June and August–December 2024). Participants had the option to take part in individual or family group interviews and were invited to include any supporters they would like to have present. Most interviews were conducted face-to-face, with the option of telephone and virtual interviews using Zoom also being available. All interviews were conducted by Māori author ES. Kaumātua from Te Ārai Kāhui were also available to provide additional cultural support for Māori whānau if required.
Interviews followed Kaupapa Māori principles, beginning with the opportunity to whanaungatanga (to establish relationships and connections). All families were offered the opportunity to karakia (pray, incantations) or engage in individual cultural or spiritual activities at the start and end of each interview. Kai (food) and a voucher were provided to manaaki (show generosity and hospitality) to participants.
Interviews were informed by pūrākau – a Māori storytelling method. 29 All interviews opened by inviting families to share their stories with us allowing for allowing for a culturally responsive approach to data generation, as storytelling has been identified as a transcultural communication method. 30 Follow-up questions were informed by an interview guide (see Supplemental File 1), developed by the research team based on a previous scoping review of family experiences. 10 The interview guide was tested in a pilot interview with the service user advisor, where minor refinements were made. This interview was included in the data analysis. All interviews were audio recorded with participant consent and transcribed by a transcriptionist or the interviewer. Transcribed interviews were de-identified by the author, with families being invited to select their own pseudonyms. Following this, collaborative story production methods were used to co-construct digital narratives of participants’ experiences. These stories were created by the interviewer from interview transcripts and returned to families, who were invited to make revisions. Collaborative story production was selected as it provides a more user-friendly form of member checking than verbatim transcript review. 31 It also aligns with Kaupapa Māori methodology by upholding storytelling as a traditional medium of knowledge transmission, while promoting participant engagement and data sovereignty through story co-construction.32,33
Analysis
Data were analysed inductively to identify themes across the dataset following Braun and Clarke's (2022) RTA. 34 This method aligned with the authors’ epistemological positioning by acknowledging the role of subjectivity in research and offered theoretical flexibility to incorporate kaupapa Māori concepts. The six steps of RTA were followed iteratively and concurrently with data collection, as demonstrated in Table 1. Steps 1–3 of RTA were completed by author ES with oversight from study authors NA and MG. All authors, including the service user advisor, were involved in developing and refining final themes. Reflexivity through author discussions was important for considering the positioning of Māori and non-Māori researchers. Tensions between coding experiences of Māori whānau using kaupapa Māori concepts were noted in early RTA stages, and after group discussions, this was managed by coding data from Māori whānau twice. In one analysis, data from Māori whānau were included in conjunction with all family data, and in a separate analysis, only Māori data were included to allow for a more in-depth analysis from a Kaupapa Māori lens. This study reports on the analysis of the combined family experiences, while a separate analysis of Māori whānau experiences has been completed.
Steps of reflexive thematic analysis.
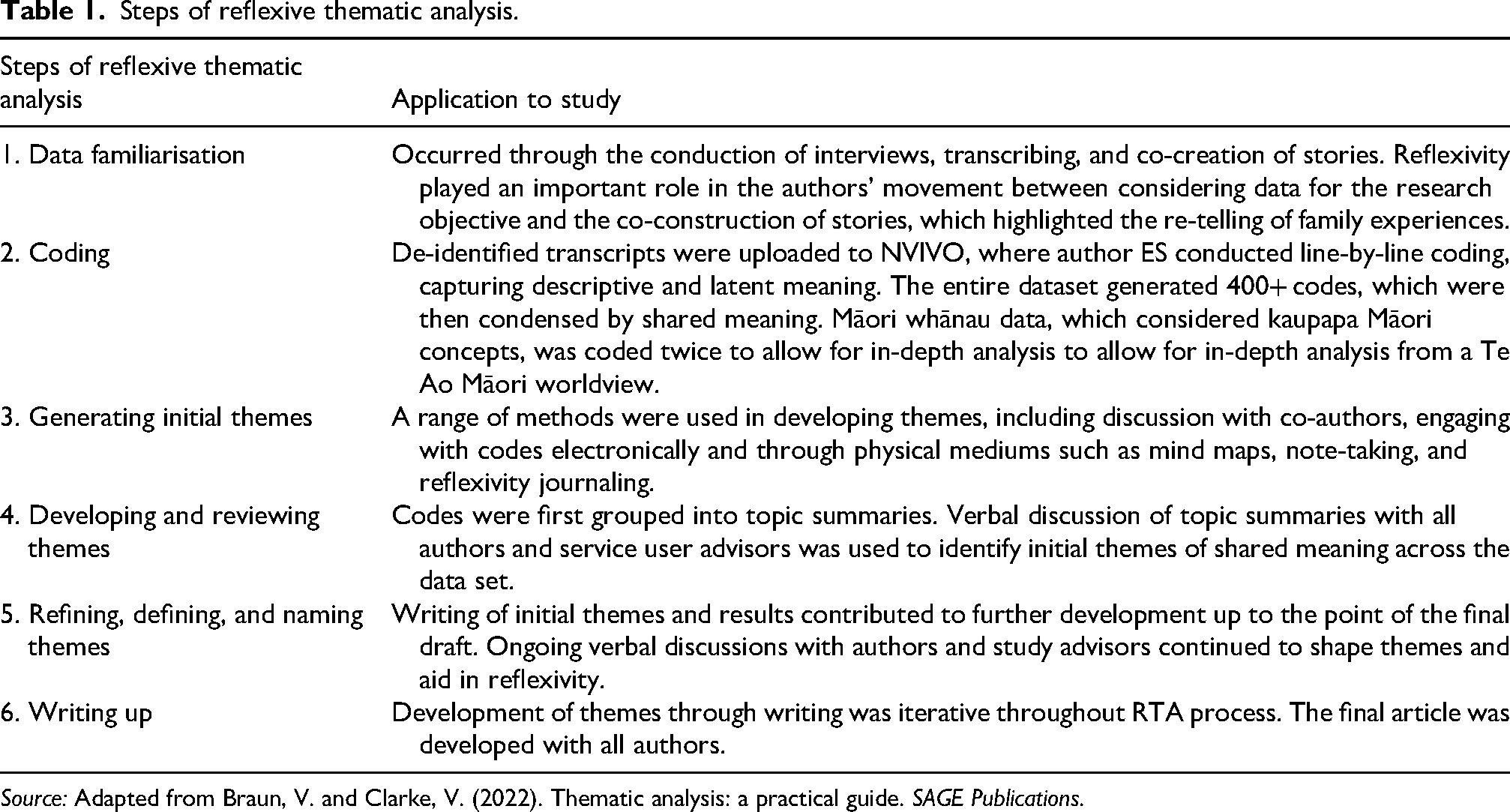
Source: Adapted from Braun, V. and Clarke, V. (2022). Thematic analysis: a practical guide. SAGE Publications.
Ethical considerations
Ethics approval was received by the Auckland Health and Research Ethics Committee (reference number AH27360) in April 2024.
Results
We conducted 21 individual and group interviews with 23 bereaved family members across Aotearoa New Zealand. Stories from families included instances of adult (n = 17) and paediatric (n = 3) death from a range of clinical scenarios including medical (n = 6), cardiac (n = 8), trauma (n = 2), suicide (n = 6) and three instances where the cause of death was unknown. Both urban (n = 15) and rural (n = 6) settings were included. Further demographic data is shown in Table 2. Four themes were generated that captured the experiences of families in out-of-hospital death where the ambulance responds: making space for family, compassionate family care, importance of communication, and closure in crisis.
Demographic data.
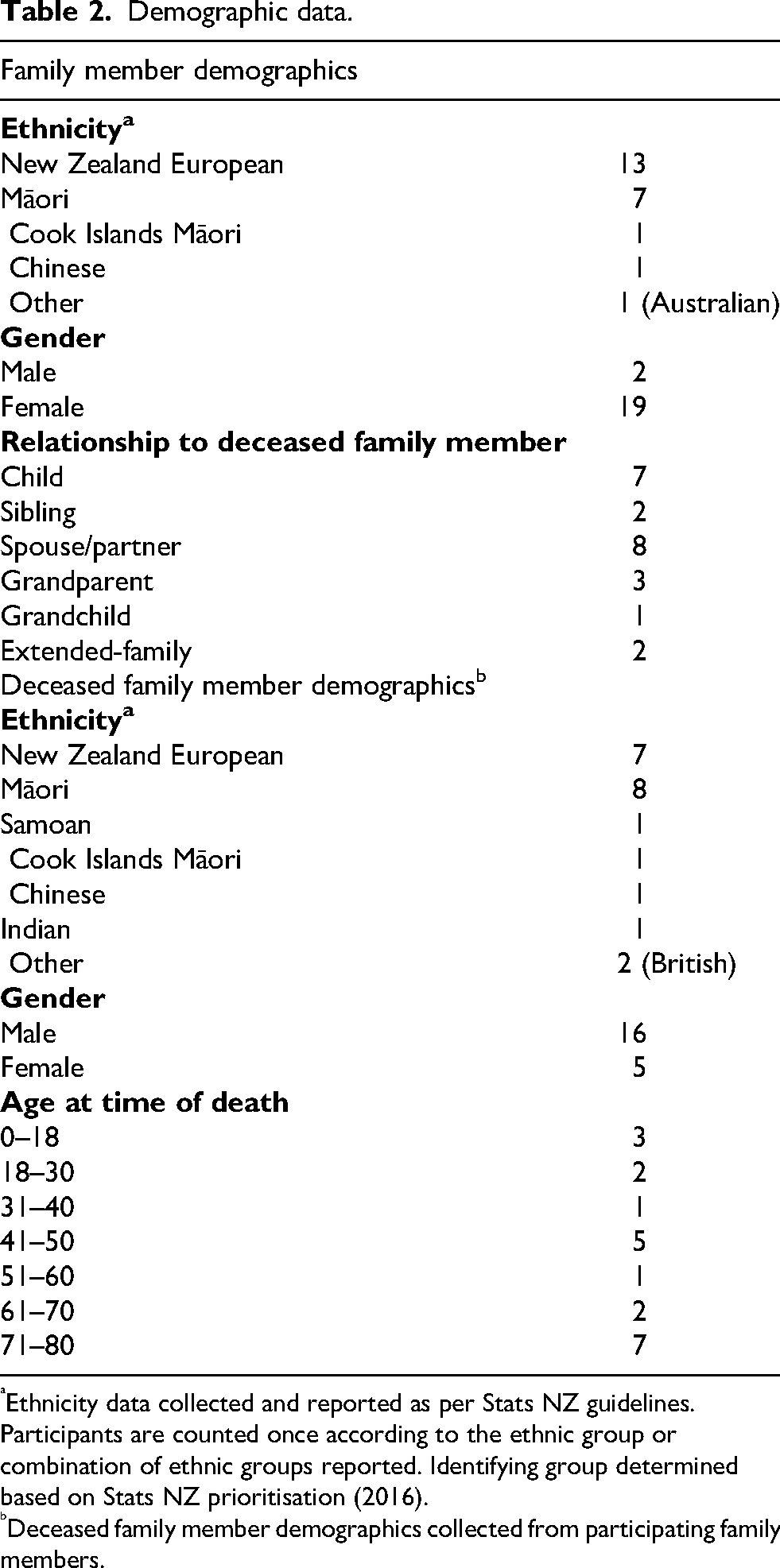
Ethnicity data collected and reported as per Stats NZ guidelines. Participants are counted once according to the ethnic group or combination of ethnic groups reported. Identifying group determined based on Stats NZ prioritisation (2016).
Deceased family member demographics collected from participating family members.
Making space for families
During out-of-hospital resuscitation and death, families highlighted the importance of being present. However, having space to be present meant more than just physical proximity; it included having family identity recognised and their needs and decision-making abilities acknowledged.
Findings from this study highlighted the diversity of families in relationships, ethnicity, sexual orientation and cultural and spiritual beliefs. Recognising self-defined family identities was essential, as assumptions based on heteronormative family structures could diminish feelings of loss. This was particularly evident for Māori and Pacific whānau (families), who emphasised the importance of collective family identity. It was very common for multiple family members to be present and continue to arrive during resuscitation and after death. Family members felt supported by ambulance personnel when they were given space as a collective to be present and engage in cultural and spiritual beliefs.
Family presence was empowered when they were invited to stay during events and were provided with information and emotional support. High personnel numbers, sometimes upwards of 10 personnel across emergency services, acted as a barrier to family presence. Rarely were families discouraged from being present, though when this did occur, it negatively impacted family experience. Ambulance personnel's actions also influenced family perceptions of space after a death. Medicalisation of the scene and procedural elements, such as verification of death and police investigations, acted as barriers to family spending time with the deceased. This was improved through ambulance personnel encouraging family presence. Family were conscious of how their grieving actions would be perceived, particularly regarding cultural and spiritual needs. It was important that ambulance personnel normalised grief reactions and provided opportunity for beliefs to be acknowledged. Often, families did not expect specific cultural and spiritual support from ambulance personnel, but rather needed time and space to engage in their beliefs. It was essential that this space was given, as ambulance personnel's care of cultural and spiritual needs was otherwise limited. Deaths in public spaces were especially challenging, as privacy and dignity could be compromised. These factors impacted family comfort in spending time with the deceased family member, which sometimes affected their grieving actions. This is shown in the following extract from Chrissy, grieving the sudden loss of her dad. I was just crying, lying on him and crying. Then I came to realise that all these emergency services were watching. And it came to me, I've got to get up, I can’t hold them up. I felt pressured to get up. Not pressured by them, nobody was saying get up or anything like that. It was just knowing that the police and ambulance were there. Now I wish I had spent more time. Had he died at home, I wouldn't have felt pressured. If it had been anywhere else, I would have had more time. I could have lain there forever with him, and I feel ripped off knowing that I couldn't. (Chrissy, bereaved daughter)
Making space for shared decision-making also influenced families’ experience. Many family members wanted to be involved in decision-making and described how advocating for their family members’ wishes motivated them to stay during resuscitation. However, families reported poor information sharing during resuscitation and few opportunities to participate in decision-making. An exception was in palliative care scenarios, where families played a larger role in decision-making. This was not without its challenges, with some families commenting on the difficulties of advocating for the withholding of resuscitation and the legality of advance care directives. Four families highlighted that shared decision making could provide an opportunity to cease resuscitation efforts sooner or reduce unwanted transportation, as they felt resuscitation was unlikely to be successful. Involving family in termination decision-making provided an opportunity for family to gain a sense of control in an otherwise powerless situation. Stories from families involved in termination discussions suggested that empowering family decision-making could aid acceptance of termination by reframing the withdrawal of intervention as an intentional action to allow their family member to die peacefully. The [paramedics] said, ‘This is what we've tried to do, this is the decision that needs to be made, what do you want us to do from now?’ And they didn't rush either of them into saying something. They did it in such a way that was definitely calming and reassuring. My dad just said, ‘You know, if she hasn't got a life, then you know, there's no real point.’ I agreed with Dad; I knew even at that young age that that's not what she would have wanted. And so, they stopped. She pretty much slipped away at that moment. It was like we could let her go peacefully now. (Danielle, bereaved granddaughter)
Compassionate family care
Experiencing the death of a family member is emotionally challenging. Families’ experiences and their perception of emergency ambulance care were impacted by how personnel responded to their grief. Actions from emergency services that showed compassion were reported as supportive. Compassion could be shown through emotional gestures, such as empathising with family, addressing emotional needs, and practical actions, like organising funeral directors or offering food and drink. Once they realised that there was absolutely nothing they could do for [my brother], they did focus their attention on the rest of us. It couldn’t have been a better experience from the ambulance crew. My father kept on apologising to them, and they calmed him down and said, ‘Look, it doesn't matter if we’re here for the next four or five hours. We need to make sure everybody who was involved in this is okay.’ The female officer was lovely. She really took the time to calm Mum down, made her a cup of tea, and got her settled. (Jamie, bereaved brother) They got my mum out of the bathroom and they dressed her, put her in her nightie and put her in bed. It gave her dignity … They could have just put her on top of the bed in those [soiled] clothes couldn't they? But they dressed her and put her in bed like she was asleep. It was just the care they took with my mum, they were just so nice. (Julie, bereaved daughter)
A typical action in response to death was for ambulance personnel to acknowledge family grief through statements such as “I’m sorry for your loss.” However, the affirmation of loss alone did not aid in the family feeling more supported. When this statement was the only post-event support, it was reported to feel generic and impersonal as it failed to acknowledge the individual family members’ feelings and situational context: The [paramedics] said, ‘sorry for your loss,’ but it was a bit annoying. It felt a bit gross. I mean, they were trying to be kind, but, you know, it always feels weird when somebody says that because it feels insincere. (Ash, bereaved partner) It was quite clinical, at the point where all hope was lost. We still couldn’t get into the room with him because, of course, they were packing stuff up …. And they [the ambulance and fire personnel] were there talking about their weekend. You know, they're kind of just having a conversation with people they regularly see because there was nothing they could do and, look, if I were being critical, I'd say it was disrespectful. (Elaine, bereaved daughter-in-law)
Importance of communication
A key factor shaping family experiences was ambulance personnel communication. Overall, family received little communication during resuscitation. Use of medical jargon presented as a barrier to communication and negatively impacted family understanding. Families sometimes pretended to understand this jargon rather than seek clarity: The [paramedics] said, ‘he's in asystole’, and I went ‘oh yeah’ but did not know what that meant. Maybe if they'd said instead, he's died, or his heart's stopped beating, yeah, a bit more plain English for the layman. I might have understood it at another time, but [not] when you're in shock (Angela, bereaved spouse).
Family experience improved when there was deliberate communication during the resuscitation and post-termination. Having one ambulance personnel who was responsible for communicating with the family was described as helpful, as this provided a go-to person for families and reduced information overload, as demonstrated in the following extract from Aroha involving the death of her grandchild: There was one ambulance officer whose job was mainly to talk to me. And I think that was quite good that instead of them all coming up to me, because it's quite overwhelming having all of these people coming at you. They were really calm and, you know they were just explaining to me. I think they knew like how hysterical my daughter was. They weren't gonna be able to get through to her, so they were just explaining to me what they were doing. And then, you know I'd simplify it for my kids. (Aroha, bereaved grandmother)
Delivering the news that someone has died is one of the most crucial communications ambulance personnel will make. Most families described that the ambulance personnel delivered the news clearly and compassionately, which improved family experiences. They [paramedics] sat us down after they did their assessment, and I said, ‘You know, is she really …, is there anything there? And yeah, the ambulance people did a lovely job of just talking us through that. And kind of just saying this is what will happen now, and the police will be coming in. (Renee, bereaved sister) They just all suddenly stopped doing CPR. There was this beeping sound like beep, beep, beep, and I thought, oh, it's his heart, you know, his heart's going. Because they’d done a few [mimes shocks]. And I was like oh, they’ve got his heart going even though he was still lying there. But then everyone disappeared, and we were standing around thinking what's happened? Is he all right? Can we get in and be by him, you know? And then someone walked around, a young guy, and I’m not sure if he was an ambulance or a fireman, and he said, ‘Oh, are you family?’ And I said ‘Yes’, and he said, ‘Oh, I’m sorry, he's passed.’ And it's like, what? You know, we couldn’t believe it. Anyway, his koro [grandfather] let out this huge wail, and we were just all walking around in the rain, and we didn’t know what to do. (Winnie, bereaved grandmother)
Closure in crisis
Families often struggled to make meaning after the death of a family member. Actions of ambulance personnel and the chance to be present during resuscitation aided in the acceptance of events. Being present during resuscitation reassured families that every possible effort was made to save their family member, which positively influenced families’ perceptions of ambulance personnel. Despite the unsuccessful outcome, many families praised the clinical skills and dedication of the responders. Some families struggled to believe that their family member had died. Spending time with their deceased family member allowed them to come to terms with the reality of death and begin the grieving process: I was convinced that he was still alive. I guess I was in a state of mania, panic, shock, or something. Even when they explained to me that he was dead, I didn't believe them. The paramedics, they explained and they took me over there and just let me have a moment with him … something just wasn’t kicking into my brain that he was gone, until I touched him. So, seeing him like that, you know I didn't think it was real until I saw him in the ambulance … It was important for me to see him, just to know that it was real. (Kelly, bereaved partner) After the event, there is no post-care process for people dying. The oncologists didn't come over. The doctor didn't come over and explain what happened. We’re just left with burying my father in the ground. If there was some way that whānau had the option of speaking to the ambulance, or if somebody said to me now, do you want to read the ambulance report? I'd be all about it because there are so many voids in my head of those minutes when I don’t know what happened. I know for me it would make a huge difference if the emergency services that were involved gave me a rundown. If they presented a report back to us. Some whānau may say no; for example, I don’t know if my stepmum would be strong enough to read it. But I would read it for us and, you know, if any of my other whānau wanted to read it, my brother or sister, or my nephew's very close with my dad. That would give us some way of knowing what happened in those minutes. (Chrissy, bereaved daughter) It was a relief when the paramedic said ‘Mate he's been dead for a couple of hours at least. Nothing you would have done would have made a blind bit of difference.’ That was better because the thing is that I struggled for years afterwards about the fact that maybe if I did this. Maybe if I was quicker, maybe if I did this, maybe if I did this. But then I started to think, if the paramedic turned around and said there's nothing you could do. He's been dead for at least a couple of hours, that did make me feel better. (Jamie, bereaved brother)
Discussion
In this qualitative study, we identified four themes that influence the experiences of bereaved families during out-of-hospital deaths where ambulance services respond. Our findings highlight the significant role that ambulance personnel play in shaping family experience during death, dying, and bereavement. Family care varied across the timeline of events. During resuscitation, families described being treated as witnesses and were not commonly supported to be meaningfully present. In contrast, when resuscitation was withheld or terminated, family received higher levels of personnel support. These findings suggest that providing supportive care to families throughout all stages of emergency ambulance responses warrants greater attention. Inconsistencies in family support during resuscitation are mirrored in current ambulance care guidelines. While international and Australasian resuscitation councils endorse family presence during resuscitation35,36 few local and institutional policies guide ambulance personnel on how to support families effectively8,37 This lack of guidance is significant, as allowing presence is not the same as providing supportive family care.
Moving toward supportive care requires action to ensure families are not only present but recognised, included, and cared for throughout resuscitation and after death. Proactive engagement is needed to create space for family involvement, as the medicalisation of scenes can disempower families. This results in important emotional, cultural and spiritual needs being unspoken by families and unmet by ambulance personnel. Empowering family involvement must include recognising the systems and power structures represented by emergency services’ response. 38 This is especially critical when caring for Indigenous and ethnically minoritised populations, where cultural safety plays a vital role in supporting cultural and spiritual needs during end-of-life care. 39 Cultural safety is not limited to ethnicity alone; families’ needs are shaped by multiple intersecting factors such as religion, gender and sexual identities and spirituality.40,41 Findings from our study highlighted that families are highly diverse, with these factors influencing how they experience events, underscoring that a one-size-fits-all approach to family bereavement care is unlikely to be successful. 42 While this study considered family experiences broadly, it is important to acknowledge that Māori whānau may hold distinct cultural needs related to death and dying. Māori worldviews have been shown to be poorly understood in current paramedicine practice, 43 and focused research on Māori whānau experiences during out-of-hospital deaths will be essential to strengthen cultural safety and ensure that care reflects Māori values and aspirations. This reinforces the importance of individualised, person-centred assessments which consider holistic elements. 44
Family involvement during resuscitation can be improved by recognising collective family identities in line with Māori world views, and by increasing information sharing, which can promote family inclusion and facilitate shared decision making.45,46 Increasing shared decision-making with families presents an opportunity to reduce unwanted interventions and reframe termination of futile resuscitation as an act of care rather than a withdrawal of treatment.47,48 Earlier involvement of family in treatment decisions may also better prepare families for death and eliminate confusion that the patient has died. 49 Despite challenges such as the out-of-hospital setting, resourcing of emergency ambulance services, the nature of unexpected events, and legal complexities, involving family in decision-making remains central to end-of-life care.50,51 Inclusion of family in these discussions would better align with current practice recommendations, particularly as ambulance services increasingly respond to events where resuscitation is not wanted or warranted.2,52
Just as space must be actively created for family involvement, compassionate care doesn’t happen by default – it arises from empathetic interactions by ambulance personnel that recognise the emotional experiences of families. Understanding the distinctions between empathy and sympathy is central to the provision of compassionate care. Unlike sympathy, which is characterised by self-oriented expressions of pity for another's misfortune, 53 empathy involves understanding the feelings and perspectives of others and can lead to compassionate responses.54,55 In this study, empathetic responses were consistently described by families as comforting and memorable, whereas sympathetic actions were perceived as superficial and lacking connection. This reflects end-of-life literature, which shows that sympathy alone is typically viewed negatively by bereaved individuals. 56 These findings highlight the critical role of non-technical skills in emergency care – skills that remain challenging to teach and capture in policy, yet form the foundation of meaningful patient and family relationships.
The importance of humanistic, person-centred care is well established in out-of-hospital and emergency settings,57,58 but application of this to clinical practice is not without challenges. Resourcing is commonly highlighted in paramedicine literature to be a barrier to family care, with both time and personnel availability being discussed as impacting care delivery.49,59 However, this research and international studies 60 show that it is common for high numbers of ambulance and other emergency services personnel to be present during out-of-hospital emergencies, which suggests that clinical resourcing may not be the only factor influencing family care. Previous research has shown that caring for the dying and bereaved can create dissonance on the perceived role of paramedics as ‘lifesavers’, affecting attitudes towards the role of paramedics in these events. 61 Furthermore, emotive work in fields where qualities like stoicism are ingrained can be challenging due to the high emotional labour demands.62,63 Although calls for improved recognition of family during out-of-hospital deaths have been made for decades,64,65 ambulance personnel continue to report inadequate preparation and systemic support in addressing the needs of patients and their families at the end of life.4,11,66 Multifaceted approaches will likely be required to improve family care, addressing personnel preparedness and organisational level guidance which recognises that responding to death and dying is an increasingly important part of emergency ambulance service responses.
Strengths and Limitations
A strength of this study was the broad inclusion criteria, capturing a wide range of scenarios and family experiences, reflecting the diverse events that ambulance services respond to. Use of Kaupapa Māori research methods also promoted culturally safe environments for Māori whānau to participate in this study. This research considered family experiences broadly; however, further research that explores the needs of Māori whānau and considers experiences through a Māori worldview is needed to inform culturally grounded policy and practice. Volunteer recruitment methods may have been influenced by self-selection bias. Experiences of bereaved male relatives were unexpectedly low, and more research may be needed to evidence their needs during these events.
Conclusion
This study reinforces the pivotal role of emergency ambulance personnel in supporting families during out-of-hospital deaths. Care that acknowledges family needs, communicates clearly, and demonstrates empathy is linked to more positive family experiences, underscoring the importance of humanistic skills in end-of-life care. While emotional support is frequently provided with compassion, greater attention to families’ cultural and spiritual needs is needed to ensure holistic bereavement support. Shifting organisational guidance from allowing family presence to providing active family support throughout resuscitation, death, and dying presents an opportunity to enhance the quality of care provided to families.
Supplemental Material
sj-docx-1-pam-10.1177_27536386251404049 - Supplemental material for Family experiences of out-of-hospital deaths where ambulance services respond in Aotearoa New Zealand
Supplemental material, sj-docx-1-pam-10.1177_27536386251404049 for Family experiences of out-of-hospital deaths where ambulance services respond in Aotearoa New Zealand by Eillish Satchell, Merryn Gott, Bridget Dicker, Tess Moeke-Maxwell and Natalie E Anderson in Paramedicine
Supplemental Material
sj-docx-2-pam-10.1177_27536386251404049 - Supplemental material for Family experiences of out-of-hospital deaths where ambulance services respond in Aotearoa New Zealand
Supplemental material, sj-docx-2-pam-10.1177_27536386251404049 for Family experiences of out-of-hospital deaths where ambulance services respond in Aotearoa New Zealand by Eillish Satchell, Merryn Gott, Bridget Dicker, Tess Moeke-Maxwell and Natalie E Anderson in Paramedicine
Footnotes
Acknowledgments
Authors would like to acknowledge Te Ārai Kāhui Kaumātua (advisory group of Māori elders) from Te Ārai Palliative Care and End-of-Life Research group for their guidance. We would also like to acknowledge the role of the service user advisor (who cannot be named due to their participation in the project) for their involvement across this study.
Ethical approval and informed consent statement
This study received ethical approval from the Auckland Health and Research Ethics Committee (approval AH27360) 15 March 2024. Written informed consent was obtained from all participants taking part in in-person interviews. Verbal consent was obtained for all participants taking part in online or telephone interviews.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Research Council of New Zealand (Grant No. 23/125/A).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analysed during the current study are not publicly available to maintain participant confidentiality in this sensitive research area. De-Identified aspects of the dataset are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.